
Abstract
An extensive network of regulation of systemic inflammation makes development of a reproducible experimental model of sepsis a complex task. There is no single mouse model that can capture all clinical aspects of this complicated pathology. However, a combination of existing approaches can go a long way towards analysis of specific mechanisms of sepsis development and to the design of novel therapeutic approaches. This review describes the popular mouse models of sepsis and septic shock, as well as their limitations and development strategies.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
INTRODUCTION
According to current views, sepsis (from the ancient Greek σῆψις, rotting) is a life-threatening organ dysfunction that arises as a dysregulated response of the body to infection. Septic shock is a kind of sepsis where metabolic, cellular, and hemodynamic alterations substantially increase the likelihood of a fatal outcome [1]. Thirty million people annually develop septic complications and six million of them die according to the World Health Organization, and the ranges may be underestimated because disease registration is poor in low- and middle-income countries [2, 3]. Many new sepsis cases arise in developed countries. For example, every third death occurs in the presence of septic complications in US hospitals [4], and hospital infections are among the main causes of sepsis because their causative agents acquire resistance to antimicrobial therapy [5, 6]. Sepsis usually develops when barrier tissues are infected with pathogenic strains of Escherichia coli, Staphylococcus aureus, Klebsiella pneumoniae, Acinetobacter baumannii, Pseudomonas aeruginosa, and Streptococcus spp., but disruption of barrier tissue integrity by components of the normal microbiota may also induce sepsis [7–9]. The highest susceptibility to sepsis is characteristic of people older than 65 years of age, infants, immunocompromised patients, and patients with chronic disorders (autoimmune disorders, tumors, kidney diseases, lung diseases, etc.) [10].
Activation of innate immunity is a key event in the induction of sepsis and occurs as pathogen-associated molecular patterns (PAMPs) are recognized by pattern recognition receptors (PRRs), such as Toll-like receptors (TLRs), NOD- and RIG-like receptors, and scavenger receptors [11, 12]. Activation of these receptors leads to a systemic production of proinflammatory cytokines and chemokines. PRRs are capable of recognizing damage-associated molecular patterns (DAMPs), which are released from damaged host cells, thus leading to excessive activation of immunocytes and endotheliocytes. This imbalance leads to cytokine overproduction (cytokine storm) [13]. Sepsis has a biphasic nature, the vigorously developing proinflammatory phase is followed by a compensatory anti-inflammatory phase, which often leads to immunosuppression [14, 15]. An early hyperdynamic phase is characterized by a higher cardiac output (the blood volume that the heart pumps in a unit time) and a lower systemic vascular resistance; a subsequent hypodynamic phase is characterized by a decreased cardiac output and a lower systemic vascular resistance [8]. Sepsis is additionally accompanied by an increase in coagulation, a decrease in fibrinolysis, multiple organ failure, and other pathological alterations, thus making it a challenge to create a reproducible animal model [16].
EXPERIMENTAL MODELS OF SEPSIS AND THEIR COMPARATIVE CHARACTERISTICS
Three types of models are commonly used to induce experimental sepsis: injection of a toxic agent (lipopolysaccharide (LPS), CpG, zymosan, or another PRR ligand), injection of live pathogens (bacteria or intestinal contents; induction of pneumonia, meningitis, urosepsis, etc.), and impairment of barrier tissue integrity (intestinal perforation, wound sepsis models, etc.) [14]. The two first groups include mostly low-invasive nonsurgical models, while surgery is necessary to obtain a sepsis model of the third group. The most common experimental mouse models of induced sepsis are characterized in Table 1.
SEPSIS INDUCTION BY IMPAIRING THE INTEGRITY OF BARRIER TISSUES
In the most clinically relevant current models, polymicrobial peritonitis is mimicked by disrupting the gut integrity and thus allowing microbiota components to enter the peritoneal cavity [19].
Cecal ligation and puncture (CLP) reproduces the clinical picture of an intraperitoneal abscess and polymicrobial peritonitis in appendicitis or diverticulitis with tissue ischemia because an infection focus is present and bacteria gradually enter the peritoneal cavity [61]. The model additionally has other features of sepsis, such as activation of both proinflammatory and anti-inflammatory immune responses, early hyperdynamic and late hypodynamic phases, multiple organ dysfunction, hypothermia, metabolic alterations, DAMP production, and a similar kinetics of the cytokine response [60, 66, 68]. At the same time, an abscess often forms around the puncture site to prevent the release of cecal contents into the peritoneal cavity. Sepsis does therefore not progress to septic shock in some mice, and the acute inflammatory response becomes a chronic one, which may persist for several months [69, 73]. To model sepsis in patients with chronic kidney disease, folic acid is administered prior to CLP [75]. The CLP method does not require administration of toxins or live pathogens. Sample preparation is avoided, and diversity of the intestinal microbiota is thus preserved to a maximum extent as compared with intraperitoneal injection of gut contents to induce sepsis. The dynamics of sepsis development is possible to regulate by varying the length of the cecal region to be ligated, the needle size (18–25G), and the number of punctures (to a lesser extent), performing infusion therapy, administering antibiotics, or mimicking appendectomy by removing the necrotic cecal region via a second surgery [61]. It should be noted that the model is reproducible only when the experimental animal sample is large enough because the method is difficult to standardize because of the variation in surgery parameters, such as the type of anesthesia, the laparotomy technique, the cecal ligation length, the needle size, and the number of punctures and the dependence on the mouse genetic strain, gender, age, microbiota composition, and rearing conditions [20, 65, 72].
Colon ascendens stent peritonitis (CASP) reproduces the clinical picture of polymicrobial acute diffuse peritonitis and better mimics the pathophysiological alterations as compared with CLP, i.e., bacterial dissemination and systemic inflammation increase continuously together with cytokine production, multiple organ failure develops, while an abscess does not form to prevent the intestinal contents from entering the peritoneal cavity [76, 78]. With CASP, the dynamics of sepsis development is possible to regulate by varying the stent diameter (14–22G) or by removing the stent and suturing the intestinal perforation in a repeated surgery [77]. However, the model is more difficult to obtain as compared with CLP, the hemodynamic and metabolic changes in the model have not been characterized as completely, and the biphasic immune response in sepsis is not reproduced because the anti-inflammatory cytokine response arises almost at the same time as the proinflammatory response [71, 73]. The limitations common for both of the models are that newborn mice are impossible to use in experiments and that clinically relevant bacterial strains cannot be used to induce sepsis [71].
Cecal ligation and incision (CLI) has recently been developed and found to mimic more acute onset of sepsis as compared with that in the CLP model. However, CLI is not used broadly, and its metabolic, hemodynamic, and immunological responses have not been characterized in sufficient detail as of yet [79–81].
SEPSIS INDUCTION BY ADMINISTERING LIVE PATHOGENS
Administration of Gram-positive (Streptococcus pneumoniae and S. aureus) or Gram-negative (E. coli, Bаcteroides fragilis, K. pneumoniae, A. baumannii, and P. aeruginosa) bacteria provides a reproducible and low-invasive method to induce sepsis and is suitable for studying the mechanisms triggering the immune response to a particular pathogen without surgery [20, 22]. Depending on whether clinical isolates or laboratory strains are used, different bacteria differentially activate PRRs, for example, because they differ in LPS biological activity [21, 82, 83]. In general, the model poorly reflects the clinical picture of sepsis because there is no local infection focus where from bacteria spread continuously in a certain measure, but a single massive administration is used to achieve bacterial infection. In addition, the cytokine profile shows a faster kinetics, especially in early sepsis [30]. Only one bacterial strain is often used, while sepsis is usually polymicrobial [84]. On the other hand, use of pathogenic strains makes it possible to mimic hospital infections, which are often caused by monoinfections. The model partly reproduces the clinical picture of peritonitis in the case of intraperitoneal administration of bacteria or bloodstream infection through an intravascular catheter in the case of intravenous administration, and several PRRs are activated in contrast to single-toxin models. Alternative routes are possible for administering bacteria in the model: intravenous (i.v.), intraperitoneal (i.p.), subcutaneous (s.c.), etc. Depending on the pathogen administration site, the approach allows a modeling of meningococcemia [85] or, for example, urosepsis [86]. The dynamics of sepsis development is possible to regulate by varying the composition of the bacterial sample or using antibiotics [19]. Many bacteria die as a result of complement activation after their systemic administration, and the resulting rapid development of endotoxinemia causes early death of the host and limits the full development of sepsis [30, 87]. Lower amounts of bacteria should be administered to prevent endotoxinemia, and this is possible to achieve by using highly virulent strains or additional adjuvants (e.g., sterilized feces). Different mechanisms may underlie sepsis development depending on the bacterial strain; e.g., IFNγ promotes the survival in the case of P. aeruginosa and S. pneumoniae infections and decreases the survival in the case of S. aureus and E. coli infections [30, 88, 89]. The route of pathogen administration may also affect the pathogenesis mechanism; e.g, IL-10 exerts a protective effect in the case of intraperitoneal administration of bacteria and facilitates disease progression in the case of the induction of bacterial pneumonia [90, 91]. Bacterial may differentially infect different organisms; e.g., Salmonella typhimurium is more efficient in infecting mice compared with humans [92].

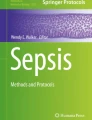
Development of acute hepatotoxicity after administration of LPS with D-GalN. UDP, uridine 5'-diphosphate; cyt C, cytochrome C; cas, caspases; ALT, alanine aminotransferase; AST, aspartate aminotransferase; DAMP, damage-associated molecular pattern.
Implantation of a bacteria-laden fibrin clot in the peritoneal cavity requires surgery under general anesthesia and results in a continuous release of bacteria, thus better mimicking the spread of pathogens from an infection focus as compared with systemic administration of bacteria [59]. Hemodynamic and metabolic alterations and the cytokine response kinetics reproduce the clinical picture of microbial peritonitis [58]. On the one hand, the model lasts several days (there is no early mortality due to endotoxinemia) and is therefore better suitable for studying monoinfections than systemic administration of bacteria; on the other hand, one bacterial strain is used, while sepsis usually has a polymicrobial component [84]. The method is suitable for studying early treatment with antibiotics during pathology development. The model is reproducible only when the bacteria-laden clot preparation and laparotomy techniques are standardized [93]. The sepsis development rate is possible to regulate by varying the fibrin clot density and selecting the necessary concentration of bacteria [22]. In addition, peritonitis progression is possible to terminate by removing the clot via a second surgery [20].
Intraperitoneal injection of a fecal solution or cecal slurry (CS). The models are simpler to obtain and provide a low-invasive means to induce polymicrobial sepsis, but require the sample to be prepared preliminarily and its bacterial composition to be standardized [52, 57, 94]. In contrast to classical sepsis, mass administration of intestinal contents may induce a strong immune response, which leads to early death or complete recovery [54]. The models poorly reproduce the hemodynamic and metabolic alterations in sepsis and display different profiles of relevant gene expression and cytokine production [56]. The dynamics of sepsis development is regulated by varying the amount of the intestinal contents administered, and microbiota diversity in the sample is lower than in the CLP and CASP models because certain bacteria (primarily anaerobes) die during sample preparation. Freezing the material to be administered partly solves the problem of sample standardization in different experiments, but causes death of certain sensitive strains [20]. Mice sometimes develop tolerance of their own microbiota, requiring the use of an additional adjuvant, such as barium sulfate [95].
Pneumonia-induced sepsis provides a clinically relevant model because airway infections often lead to secondary infection and subsequent acute respiratory distress syndrome, bacteremia, damage to the lungs, and multiple organ failure [20, 96, 97]. The model is relatively simple and reproducible and allows several alternative routes to administer bacteria, including intranasal (i.n.), intratracheal (i.t.), intrabronchial (i.b.), spraying, etc. (it should be noted that the i.t. and i.b. administration requires anesthesia, which may affect the development of the immune response) [50]. The model makes it possible to mimic community-acquired pneumonia by administering S. pneumoniae and S. pyogenes pathogenic strains or hospital-acquired pneumonia by administering P. aeruginosa, K. pneumoniae, S. aureus, and A. baumannii strains and even to reproduce the clinical picture of hospital infection in peritonitis when combined with the CLP or CASP model [14, 50]. An inverted response to therapy is often observed in this mouse model, i.e., inhibition of anti-inflammatory cytokines increases the survival, while inhibition of proinflammatory cytokines decreases the survival [43]. The sensitivity to different pathogens varies in the model. For example, large amounts of bacteria are necessary to inoculate in the lungs to induce P. aeruginosa pneumonia, and the disease develops within one day, rather than several days, thus poorly reflecting the clinical dynamics [44].
SEPSIS INDUCTION BY ADMINISTERING TOXINS
Low-invasive sepsis induction with toxic agents usually implies administration of PRR ligands, including zymosan, CpG, peptidoglycan, lipoteichoic acids, etc. [30]. Direct LPS toxicity (systemic administration of LPS) and acute hepatotoxicity (systemic administration of LPS in combination with D-GalN) models are the most common [93]. These controlled reproducible models greatly simplify the multistage clinical picture of sepsis development and rather reproduce certain features of endotoxemia or the acute phase of Gram-negative sepsis, such as lack of an infection focus, a hypodynamic stage developing without a preliminary hyperdynamic stage, lactic acidosis, short-time and abundant production of proinflammatory cytokines, increased expression of DAMPs (e.g., HMBG-1), and strong activation of innate immunity [19, 25, 30]. Toxin administration does not mimic the development of polymicrobial sepsis or the host-pathogen interactions because the immune system does not have to eliminate the pathogen [17]. At the same time, high LPS levels in the blood are observed in meningococcemia, bacteremia, and antibacterial therapy, rendering the models clinically significant [98]. Anti-inflammatory cytokines expressed upon activation of the TLR4 signaling pathway in the models are the main inductors of sepsis, and their production correlates with the severity of sepsis in the models as well as in patients [56, 99, 100]. The approaches are broadly used to study the TLR4 signaling pathways and to test blockers of inflammatory mediators (e.g., cytokines) in preclinical studies, but are rarely efficient in clinical studies. Several alternative routes (i.v., i.p., etc.) are available for toxin delivery into the body, and long-term continuous administration is possible because the LPS molecule is stable [22]. The immune response can be regulated by varying the LPS dose or using LPS preparations with different biological activities [21, 83]. It should be noted that LPS sensitivity greatly varies among species. For example, humans are several orders of magnitude more sensitive to LPS than mice [18].
Sensitization with D-GalN does not cause death in mice, but makes it possible to reduce the LPS amount necessary to induce sepsis by several orders of magnitude as compared with the direct LPS toxicity model [24]. The advantages of the LPS/D-GalN acute hepatotoxicity model are that the model is inexpensive, simple to obtain, and well reproducible and that experiments are easy to standardize. LPS/D-GalN administration activates TLR4 in liver resident macrophages (Kupffer cells) and subsequent production of proinflammatory cytokines, primarily TNF, thus inducing inflammation and liver failure; NF-κB inhibition in Kupffer cells decreases damage to the liver [25, 101–103]. Because D-GalN is metabolized exclusively in hepatocytes, its administration increases the liver sensitivity to TNF, and activation of the TNF-RI signaling pathway triggers apoptosis in hepatocytes [104–106]. Acute liver failure develops as a result and is associated with a substantial increase in the release of transaminases (ALT and AST), TNF, and interleukins into the blood, eventually leading to death [107, 108]. The kinases and transferases that convert glucose to UDP-glucose and galactose to UDP-galactose are involved in converting D-GalN to UDP-D-GalN as well, and uridine is consequently sequestered as a result of its incorporation in UDP-D-GalN when the D-GalN concentration is high enough. A transferase transfers the galactosyl moiety from UDP-galactose to a protein to produce galactosylated proteins and to restore the UTP pool, but is incapable of catalyzing the same reaction with UDP-D-GalN; UTP deficiency consequently develops in hepatocytes, and transcription is inhibited [23]. The inhibition of transcription stops the syntheses of antiapoptotic proteins (Bcl-2 and Bcl-xL) and activates the kinase cascade [25, 109]. LPS or TNF administered during this period lead to septic shock, while uridine administration protects mice from LPS/D-GalN toxicity [110]. Damaged hepatocytes produce DAMPs and alarmins, thus further stimulating macrophage activation [111].
It is of interest that a balance of proinflammatory and anti-inflammatory cytokines is distorted in Kupffer cells expressing transmembrane TNF (tmTNF); the distortion facilitates the development of inflammation, increases damage to the liver, and induces apoptosis through tmTNF and expression of the FasL proapoptotic factor [112]. TNF acts as an activator of neutrophils and monocytes; induces expression of the ICAM-1 and VCAM-1 adhesion molecules and selectins in endothelial cells and hepatocytes; and stimulates the production of the CXCL2, CXCL8, and CCL2 chemokines in hepatocytes, thus promoting neutrophil and monocyte migration into liver sinusoidal capillaries and then into liver parenchyma and increasing inflammation due to production of proinflammatory mediators [113–117]. The mechanism whereby hepatocyte apoptosis affects the induction of inflammation is still incompletely understood, but inhibition of their apoptosis is known to abolish migration of neutrophils into the liver and their activation [25]. Therapeutic administration of dopamine, cyclooxygenase inhibitors, and plant flavonoids (alpinetin, isovitexin, etc.) decreases the production of proinflammatory cytokines and improves the survival of mice in the model [118–122]. A general scheme of acute hepatotoxicity development induced with LPS/D-GalN is shown in Fig. 1.
EXPERIMENTAL MODELS OF SEPSIS: LIMITATIONS AND DEVELOPMENT STRATEGIES
Various agents (steroids, cytokine blockers, etc.) have been tested as medications to treat sepsis in several tens of clinical studies from the 1980s, but only few of them increased the survival in patients, while the majority of them were ineffective or even worsened the disease [19]. The examples of pharmacological agents that showed efficacy in treating experimental sepsis in animals, but were rejected in clinical studies (phases III and IV) in patients include selepressin (ClinicalTrials.gov Identifier: NCT02508649), anakinra (IL-1RA), TNF blockers (etanercept, CDP571, etc.), anti-endotoxin antibodies, TAK-242, tifacogin, TCV-309, lenercept, NO inhibitors, antithrombin, BB-882, BN 5021, alkaline phosphatases, drotrecogin alfa (activated), and methylprednisolone sodium succinate [19, 123]. It is clear that the circumstance is explained by a limited clinical relevance of preclinical mouse sepsis models, which fail to fully mimic the metabolic, hemodynamic, and immunological changes that occur in patients with sepsis or septic shock. Mice differ from humans in several immune properties that affect the pathogenesis of sepsis. Mice are several orders of magnitude more resistant to toxins (LPS and diphtheria toxin) than humans; have a lower total neutrophil fraction in the blood, a lower neutrophil enzymatic capacity, lower activity of the complement system, and a different set of pentraxins involved in the inflammatory process; and lack genes for important components of the immune system, such as IL-8, IL-37, TLR10, ICAM-3, etc. [72, 124, 125]. Combining several sepsis models, each of which is not universal when used alone, may provide for a better understanding of the molecular mechanisms of sepsis. The variation in the pathogenesis of many septic complications is another circumstance to consider, and etiological variations should be allowed for in a strategy of preclinical studies of therapeutic agents [126].
Laboratory mice reared in specific-pathogen-free (SPF) conditions usually have a rather immature immune system with a deficit of memory T cells [127], thus being better suitable for mimicking sepsis in human newborns, but not in adults. These mice may have limited diversity of the microbiota, which directly affects the immune system and the development of pathological conditions [128]. Moreover, persistent virus infections (for example, herpesviruses) are activated in humans, but not in SPF mice, with septic complications and may change the resistance to bacterial coinfections [72, 96, 97]. “Dirty” mice are possibly better suitable for mimicking human pathologies [129]. In addition, inbred mouse strains are used in the overwhelming majority of studies, while the human population is heterogeneous, pointing to the importance of studies in interstrain hybrid, outbred, and nonlinear mice.
Use of small animals in preclinical studies of sepsis makes it difficult to monitor the hemodynamics by invasive methods and to perform active maintenance therapy (artificial ventilation, infusion therapy, renal replacement therapy, parenteral nutrition, etc.). Concomitant antibacterial and vasopressor support is often ignored in experimental models of sepsis, while being always provided to human patients [44, 84, 130]. Use of larger animals (for example, non-anthropoid primates) to model sepsis will substantially increase the costs of studies, but will make invasive monitoring and maintenance therapy more efficient [131].
Healthy young mice (8–12 weeks) are commonly used in experiments, but old mice seem more expedient to use to study the pathogenesis of sepsis and means to treat it because elderly people are more susceptible to septic complications [132–135]. In addition, preclinical data are rather difficult to interpret because mice of one gender are often used, while sex hormones and sex-linked genes may affect the differential predisposition to sepsis [136].
Although mouse models do not always exactly mimic human inflammatory diseases [137], it is impossible to avoid experiments in mice because the species is well studied; similar gene expression profiles are observed in mice and humans during inflammation; there is an overlap in physiological, genetic, and biochemical features of mice and humans; and experiments with mice are inexpensive and simple to perform and involve minimal ethical problems [138–140]. Moreover, a vast panel of genetically modified mice with changes in immune system components is available and provides additional opportunities to investigate the molecular mechanisms involved in the pathogenesis of sepsis. Humanized mouse strains are important to use more broadly to experimentally model sepsis because the pathology development in humans is better reproduced in such models [134, 141–145]. However, it should be noted that immune system components are primarily subject to humanization, while the nervous system, the epithelium, the endothelium, and metabolic pathways important for the development of sepsis remain mouse [72, 146–149].
Apart from developing new models, it is important to standardize the existing experimental models of sepsis [150]. Standardization is necessary for a multiparametric system designed to evaluate the severity of septic condition in animal models [151]. Experimental models with different types of sepsis induction are important to combine in preclinical studies because data from a single model may lead to incorrect interpretation of the roles of factors involved in the pathogenesis of sepsis or the efficacy of therapies used. For examples, studies have shown that the TLR4 signaling pathway is essential for the development of polymicrobial sepsis and LPS- or LPS/D-GalN-induced toxicity [152–154], while other studies showed that TLR4 makes only a minor contribution to the pathogenesis of sepsis in the CLP and CASP models [155–157]. Another example is provided by the cytokine IL-12, which is involved in sepsis development in the CASP model [158], but plays no role in the CLP model [156].
A search for pharmacological agents to treat sepsis will certainly continue. It seems promising to investigate the blockers of the complement system (primarily C5b-9, C5a, and its receptors) [159, 160] and the immunological checkpoints (PD-1, CTLA-4, TIM-3, etc.) that affect the activation of innate and adaptive immune responses [161]. Another therapeutically interesting strategy is modulating the signaling pathways of the cytokines that regulate the pathogenesis of sepsis and septic shock: IFNγ, GM-CSF, MIF, IL-7, IL-8, IL-15, IL-17, IL-27, IL-33, etc. [162–166]. An important problem is to develop the pharmacological inhibitors for HMGB1 [167] and the microRNAs (miR-132, miR-146a, miR-150, miR-155, and miR-223) [168–170] that change in expression during sepsis development. The therapeutic properties are intensely studied for corticosteroids, β-blockers, thrombomodulin, and mesenchymal stem cells [16, 171–173]. Biotelemetry will help to better evaluate the physiological changes that occur in the body during sepsis development and to make experiments cheaper by reducing the sizes of test groups [64, 174].
REFERENCES
Singer M., Deutschman C.S., Seymour C.W., Shankar-Hari M., Annane D., Bauer M., Bellomo R., Bernard G.R., Chiche J.D., Coopersmith C.M., Hotchkiss R.S., Levy M.M., Marshall J.C., Martin G.S., Opal S.M., et al. 2016. The Third International Consensus definitions for sepsis and septic shock (Sepsis-3). J. Am. Med. Assoc. 315, 801‒810.
Reinhart K., Daniels R., Kissoon N., Machado F.R., Schachter R.D., Finfer S. 2017. Recognizing sepsis as a global health priority—a WHO resolution. N. Engl. J. Med. 377, 414‒417.
Fleischmann C., Scherag A., Adhikari N.K., Hartog C.S., Tsaganos T., Schlattmann P., Angus D.C., Reinhart K., International Forum of Acute Care. 2016. Assessment of global incidence and mortality of hospital-treated sepsis. Current estimates and limitations. Am. J. Respir. Crit. Care Med. 193, 259‒272.
Rhee C., Dantes R., Epstein L., Murphy D.J., Seymour C.W., Iwashyna T.J., Kadri S.S., Angus D.C., Danner R.L., Fiore A.E., Jernigan J.A., Martin G.S., Septimus E., Warren D.K., Karcz A., et al. 2017. Incidence and trends of sepsis in US hospitals using clinical vs. claims data, 2009‒2014. J. Am. Med. Assoc. 318, 1241‒1249.
Angus D.C., van der Poll T. 2013. Severe sepsis and septic shock. N. Engl. J. Med. 369, 840‒851.
Denstaedt S.J., Singer B.H., Standiford T.J. 2018. Sepsis and nosocomial infection: Patient characteristics, mechanisms, and modulation. Front. Immunol. 9, 2446.
Ramachandran G. 2014. Gram-positive and gram-negative bacterial toxins in sepsis: A brief review. Virulence. 5, 213‒218.
Chen P., Stanojcic M., Jeschke M.G. 2014. Differences between murine and human sepsis. Surg. Clin. North Am. 94, 1135‒1149.
Ranieri V.M., Thompson B.T., Barie P.S., Dhainaut J.F., Douglas I.S., Finfer S., Gardlund B., Marshall J.C., Rhodes A., Artigas A., Payen D., Tenhunen J., Al-Khalidi H.R., Thompson V., Janes J., et al. 2012. Drotrecogin alfa (activated) in adults with septic shock. N. Engl. J. Med. 366, 2055‒2064.
Gotts J.E., Matthay M.A. 2016. Sepsis: Pathophysiology and clinical management. Br. Med. J. 353, i1585.
Raymond S.L., Holden D.C., Mira J.C., Stortz J.A., Loftus T.J., Mohr A.M., Moldawer L.L., Moore F.A., Larson S.D., Efron P.A. 2017. Microbial recognition and danger signals in sepsis and trauma. Biochim. Biophys. Acta. Mol. Basis Dis. 1863, 2564‒2573.
Ozment T.R., Ha T., Breuel K.F., Ford T.R., Ferguson D.A., Kalbfleisch J., Schweitzer J.B., Kelley J.L., Li C., Williams D.L. 2012. Scavenger receptor class a plays a central role in mediating mortality and the development of the pro-inflammatory phenotype in polymicrobial sepsis. PLoS Pathog. 8, e1002967.
Rittirsch D., Flierl M.A., Ward P.A. 2008. Harmful molecular mechanisms in sepsis. Nat. Rev. Immunol. 8, 776‒787.
Kingsley S.M., Bhat B.V. 2016. Differential paradigms in animal models of sepsis. Curr. Infect. Dis. Rep. 18, 26.
Ward N.S., Casserly B., Ayala A. 2008. The compensatory anti-inflammatory response syndrome (CARS) in critically ill patients. Clin. Chest. Med. 29, 617‒625, viii.
Wannemuehler T.J., Manukyan M.C., Brewster B.D., Rouch J., Poynter J.A., Wang Y., Meldrum D.R. 2012. Advances in mesenchymal stem cell research in sepsis. J. Surg. Res. 173, 113‒126.
Copeland S., Warren H.S., Lowry S.F., Calvano S.E., Remick D., Inflammation, the Host Response to Injury I. 2005. Acute inflammatory response to endotoxin in mice and humans. Clin. Diagn. Lab. Immunol. 12, 60‒67.
Warren H.S., Fitting C., Hoff E., Adib-Conquy M., Beasley-Topliffe L., Tesini B., Liang X., Valentine C., Hellman J., Hayden D., Cavaillon J.M. 2010. Resilience to bacterial infection: Difference between species could be due to proteins in serum. J. Infect. Dis. 201, 223‒232.
Fink M.P. 2014. Animal models of sepsis. Virulence. 5, 143‒153.
Lewis A.J., Seymour C.W., Rosengart M.R. 2016. Current murine models of sepsis. Surg. Infect. (Larchmt). 17, 385‒393.
Korneev K.V., Kondakova A.N., Arbatsky N.P., Novototskaya-Vlasova K.A., Rivkina E.M., Anisimov A.P., Kruglov A.A., Kuprash D.V., Nedospasov S.A., Knirel Y.A., Drutskaya M.S. 2014. Distinct biological activity of lipopolysaccharides with different lipid A acylation status from mutant strains of Yersinia pestis and some members of genus Psychrobacter. Biochemistry (Moscow). 79, 1333‒1338.)
Poli-de-Figueiredo L.F., Garrido A.G., Nakagawa N., Sannomiya P. 2008. Experimental models of sepsis and their clinical relevance. Shock. 30 (Suppl. 1), 53‒59.
Silverstein R. 2004. D-galactosamine lethality model: Scope and limitations. J. Endotoxin. Res. 10, 147‒162.
Lehmann V., Freudenberg M.A., Galanos C. 1987. Lethal toxicity of lipopolysaccharide and tumor necrosis factor in normal and D-galactosamine-treated mice. J. Exp. Med. 165, 657‒663.
Maes M., Vinken M., Jaeschke H. 2016. Experimental models of hepatotoxicity related to acute liver failure. Toxicol. Appl. Pharmacol. 290, 86‒97.
van Zoelen M.A., Schouten M., de Vos A.F., Florquin S., Meijers J.C., Nawroth P.P., Bierhaus A., van der Poll T. 2009. The receptor for advanced glycation end products impairs host defense in pneumococcal pneumonia. J. Immunol. 182, 4349‒4356.
Achouiti A., de Vos A.F., de Beer R., Florquin S., van ‘t Veer C., van der Poll T. 2013. Limited role of the receptor for advanced glycation end products during Streptococcus pneumoniae bacteremia. J. Innate Immun. 5, 603‒612.
Achouiti A., van der Meer A.J., Florquin S., Yang H., Tracey K.J., van’t Veer C., de Vos A.F., van der Poll T. 2013. High-mobility group box 1 and the receptor for advanced glycation end products contribute to lung injury during Staphylococcus aureus pneumonia. Crit. Care. 17, R296.
Achouiti A., Van’t Veer C., de Vos A.F., van der Poll T. 2015. The receptor for advanced glycation end products promotes bacterial growth at distant body sites in Staphylococcus aureus skin infection. Microbes Infect. 17, 622‒627.
Buras J.A., Holzmann B., Sitkovsky M. 2005. Animal models of sepsis: Setting the stage. Nat. Rev. Drug Discov. 4, 854‒865.
van Zoelen M.A., Schmidt A.M., Florquin S., Meijers J.C., de Beer R., de Vos A.F., Nawroth P.P., Bierhaus A., van der Poll T. 2009. Receptor for advanced glycation end products facilitates host defense during Escherichia coli-induced abdominal sepsis in mice. J. Infect. Dis. 200, 765‒773.
Ramsgaard L., Englert J.M., Manni M.L., Milutinovic P.S., Gefter J., Tobolewski J., Crum L., Coudriet G.M., Piganelli J., Zamora R., Vodovotz Y., Enghild J.J., Oury T.D. 2011. Lack of the receptor for advanced glycation end-products attenuates E. coli pneumonia in mice. PLoS One. 6, e20132.
Tadie J.M., Bae H.B., Banerjee S., Zmijewski J.W., Abraham E. 2012. Differential activation of RAGE by HMGB1 modulates neutrophil-associated NADPH oxidase activity and bacterial killing. Am. J. Physiol. Cell. Physiol. 302, C249‒C256.
Achouiti A., de Vos A.F., van’t Veer C., Florquin S., Tanck M.W., Nawroth P.P., Bierhaus A., van der Poll T., van Zoelen M.A. 2016. Receptor for advanced glycation end products (RAGE) serves a protective role during Klebsiella pneumoniae-induced pneumonia. PLoS One. 11, e0141000.
Noto M.J., Becker K.W., Boyd K.L., Schmidt A.M., Skaar E.P. 2017. RAGE-mediated suppression of interleukin-10 results in enhanced mortality in a murine model of Acinetobacter baumannii sepsis. Infect. Immun. 85, e00954-16.
van Zoelen M.A., Achouiti A., Schmidt A.M., Yang H., Florquin S., Tracey K.J., van der Poll T. 2010. Ligands of the receptor for advanced glycation end products, including high-mobility group box 1, limit bacterial dissemination during Escherichia coli peritonitis. Crit. Care Med. 38, 1414‒1422.
Witteveen E., Wieske L., Manders E., Verhamme C., Ottenheijm C.A.C., Schultz M.J., van Schaik I.N., Horn J. 2019. Muscle weakness in a S. pneumoniae sepsis mouse model. Ann. Transl. Med. 7, 9.
Van Den Boogaard F.E., Brands X., Schultz M.J., Levi M., Roelofs J.J., Van’t Veer C., Van Der Poll T. 2011. Recombinant human tissue factor pathway inhibitor exerts anticoagulant, anti-inflammatory and antimicrobial effects in murine pneumococcal pneumonia. J. Thromb. Haemost. 9, 122‒132.
Schouten M., van’t Veer C., van den Boogaard F.E., Gerlitz B., Grinnell B.W., Roelofs J.J., Levi M., van der Poll T. 2010. Therapeutic recombinant murine activated protein C attenuates pulmonary coagulopathy and improves survival in murine pneumococcal pneumonia. J. Infect. Dis. 202, 1600‒1607.
Coopersmith C.M., Stromberg P.E., Dunne W.M., Davis C.G., Amiot D.M., 2nd, Buchman T.G., Karl I.E., Hotchkiss R.S. 2002. Inhibition of intestinal epithelial apoptosis and survival in a murine model of pneumonia-induced sepsis. J. Am. Med. Assoc. 287, 1716‒1721.
Coopersmith C.M., Amiot D.M. 2nd, Stromberg P.E., Dunne W.M., Davis C.G., Osborne D.F., Husain K.D., Turnbull I.R., Karl I.E., Hotchkiss R.S., Buchman T.G. 2003. Antibiotics improve survival and alter the inflammatory profile in a murine model of sepsis from Pseudomonas aeruginosa pneumonia. Shock. 19, 408‒414.
Muenzer J.T., Davis C.G., Dunne B.S., Unsinger J., Dunne W.M., Hotchkiss R.S. 2006. Pneumonia after cecal ligation and puncture: A clinically relevant “two-hit” model of sepsis. Shock. 26, 565‒570.
Knapp S., Schultz M.J., van der Poll T. 2005. Pneumonia models and innate immunity to respiratory bacterial pathogens. Shock. 24 (Suppl. 1), 12‒18.
van der Poll T. 2012. Preclinical sepsis models. Surg. Infect. (Larchmt). 13, 287‒292.
Chiavolini D., Pozzi G., Ricci S. 2008. Animal models of Streptococcus pneumoniae disease. Clin. Microbiol. Rev. 21, 666‒685.
Murakami K., Bjertnaes L.J., Schmalstieg F.C., McGuire R., Cox R.A., Hawkins H.K., Herndon D.N., Traber L.D., Traber D.L. 2002. A novel animal model of sepsis after acute lung injury in sheep. Crit. Care Med. 30, 2083‒2090.
Sordi R., Menezes-de-Lima O., Della-Justina A.M., Rezende E., Assreuy J. 2013. Pneumonia-induced sepsis in mice: Temporal study of inflammatory and cardiovascular parameters. Int. J. Exp. Pathol. 94, 144‒155.
Robertson C.M., Perrone E.E., McConnell K.W., Dunne W.M., Boody B., Brahmbhatt T., Diacovo M.J., Van Rooijen N., Hogue L.A., Cannon C.L., Buchman T.G., Hotchkiss R.S., Coopersmith C.M. 2008. Neutrophil depletion causes a fatal defect in murine pulmonary Staphylococcus aureus clearance. J. Surg. Res. 150, 278‒285.
Torres A., Rello J. 2010. Update in community-acquired and nosocomial pneumonia 2009. Am. J. Respir. Crit. Care Med. 181, 782‒787.
Müller-Redetzky H., Suttorp N., Witzenrath M. 2012. Experimental models of pneumonia-induced sepsis. Drug Discov. Today: Disease Models. 9, e23‒e32.
Sam A.D. 2nd, Sharma A.C., Law W.R., Ferguson J.L. 1997. Splanchnic vascular control during sepsis and endotoxemia. Front. Biosci. 2, e72‒e92.
Starr M.E., Steele A.M., Saito M., Hacker B.J., Evers B.M., Saito H. 2014. A new cecal slurry preparation protocol with improved long-term reproducibility for animal models of sepsis. PLoS One. 9, e115705.
Gentile L.F., Nacionales D.C., Lopez M.C., Vanzant E., Cuenca A., Cuenca A.G., Ungaro R., Szpila B.E., Larson S., Joseph A., Moore F.A., Leeuwenburgh C., Baker H.V., Moldawer L.L., Efron P.A. 2014. Protective immunity and defects in the neonatal and elderly immune response to sepsis. J. Immunol. 192, 3156‒3165.
Gentile L.F., Nacionales D.C., Lopez M.C., Vanzant E., Cuenca A., Szpila B.E., Cuenca A.G., Joseph A., Moore F.A., Leeuwenburgh C., Baker H.V., Moldawer L.L., Efron P.A. 2014. Host responses to sepsis vary in different low-lethality murine models. PLoS One. 9, e94404.
Brealey D., Karyampudi S., Jacques T.S., Novelli M., Stidwill R., Taylor V., Smolenski R.T., Singer M. 2004. Mitochondrial dysfunction in a long-term rodent model of sepsis and organ failure. Am. J. Physiol. Regul. Integr. Comp. Physiol. 286, R491‒R497.
Rittirsch D., Hoesel L.M., Ward P.A. 2007. The disconnect between animal models of sepsis and human sepsis. J. Leukoc. Biol. 81, 137‒143.
Bernardshaw S., Hetland G., Grinde B., Johnson E. 2006. An extract of the mushroom Agaricus blazei Murill protects against lethal septicemia in a mouse model of fecal peritonitis. Shock. 25, 420‒425.
Mathiak G., Szewczyk D., Abdullah F., Ovadia P., Feuerstein G., Rabinovici R. 2000. An improved clinically relevant sepsis model in the conscious rat. Crit. Care Med. 28, 1947‒1952.
Toky V., Sharma S., Arora B.B., Chhibber S. 2003. Establishment of a sepsis model following implantation of Klebsiella pneumoniae-infected fibrin clot into the peritoneal cavity of mice. Folia Microbiol. (Praha). 48, 665‒669.
Rittirsch D., Huber-Lang M.S., Flierl M.A., Ward P.A. 2009. Immunodesign of experimental sepsis by cecal ligation and puncture. Nat. Protoc. 4, 31‒36.
Mishra S.K., Choudhury S. 2018. Experimental protocol for cecal ligation and puncture model of polymicrobial sepsis and assessment of vascular functions in mice. Methods Mol. Biol. 1717, 161‒187.
Wichterman K.A., Baue A.E., Chaudry I.H. 1980. Sepsis and septic shock: A review of laboratory models and a proposal. J. Surg. Res. 29, 189‒201.
Herrmann I.K., Castellon M., Schwartz D.E., Hasler M., Urner M., Hu G., Minshall R.D., Beck-Schimmer B. 2013. Volatile anesthetics improve survival after cecal ligation and puncture. Anesthesiology. 119, 901‒906.
Lewis A.J., Yuan D., Zhang X., Angus D.C., Rosengart M.R., Seymour C.W. 2016. Use of biotelemetry to define physiology-based deterioration thresholds in a murine cecal ligation and puncture model of sepsis. Crit. Care Med. 44, e420‒e431.
Dejager L., Pinheiro I., Dejonckheere E., Libert C. 2011. Cecal ligation and puncture: The gold standard model for polymicrobial sepsis? Trends Microbiol. 19, 198‒208.
Tao W., Deyo D.J., Traber D.L., Johnston W.E., Sherwood E.R. 2004. Hemodynamic and cardiac contractile function during sepsis caused by cecal ligation and puncture in mice. Shock. 21, 31‒37.
Hubbard W.J., Choudhry M., Schwacha M.G., Kerby J.D., Rue L.W. 3rd, Bland K.I., Chaudry I.H. 2005. Cecal ligation and puncture. Shock. 24 (Suppl. 1), 52‒57.
Xiao H., Siddiqui J., Remick D.G. 2006. Mechanisms of mortality in early and late sepsis. Infect Immun. 74, 5227‒5235.
Nacionales D.C., Szpila B., Ungaro R., Lopez M.C., Zhang J., Gentile L.F., Cuenca A.L., Vanzant E., Mathias B., Jyot J., Westerveld D., Bihorac A., Joseph A., Mohr A., Duckworth L.V., et al. 2015. A detailed characterization of the dysfunctional immunity and abnormal myelopoiesis induced by severe shock and trauma in the aged. J. Immunol. 195, 2396‒2407.
Delano M.J., Scumpia P.O., Weinstein J.S., Coco D., Nagaraj S., Kelly-Scumpia K.M., O’Malley K.A., Wynn J.L., Antonenko S., Al-Quran S.Z., Swan R., Chung C.S., Atkinson M.A., Ramphal R., Gabrilovich D.I., et al. 2007. MyD88-dependent expansion of an immature GR-1+CD11b+ population induces T cell suppression and Th2 polarization in sepsis. J. Exp. Med. 204, 1463‒1474.
Maier S., Traeger T., Entleutner M., Westerholt A., Kleist B., Huser N., Holzmann B., Stier A., Pfeffer K., Heidecke C.D. 2004. Cecal ligation and puncture versus colon ascendens stent peritonitis: two distinct animal models for polymicrobial sepsis. Shock. 21, 505‒511.
Cavaillon J.M. 2018. New approaches to treat sepsis: Animal models “do not work” (review). Gen. Reanimatol. 14, 46–53.
Schabbauer G. 2012. Polymicrobial sepsis models: CLP versus CASP. Drug Discov. Today: Disease Models. 9, e17‒e21.
Nakagawa N.K., Jukemura J., Aikawa P., Nogueira R.A., Poli-de-Figueiredo L.F., Sannomiya P. 2007. In vivo observation of mesenteric leukocyte-endothelial interactions after cecal ligation/puncture and surgical sepsis source control. Clinics (Sao Paulo). 62, 321‒326.
Doi K., Leelahavanichkul A., Hu X., Sidransky K.L., Zhou H., Qin Y., Eisner C., Schnermann J., Yuen P.S., Star R.A. 2008. Pre-existing renal disease promotes sepsis-induced acute kidney injury and worsens outcome. Kidney Int. 74, 1017‒1025.
Traeger T., Koerner P., Kessler W., Cziupka K., Diedrich S., Busemann A., Heidecke C.D., Maier S. 2010. Colon ascendens stent peritonitis (CASP): A standardized model for polymicrobial abdominal sepsis. J. Vis. Exp. 46, e2299. https://doi.org/10.3791/2299
Zantl N., Uebe A., Neumann B., Wagner H., Siewert J.R., Holzmann B., Heidecke C.D., Pfeffer K. 1998. Essential role of gamma interferon in survival of colon ascendens stent peritonitis, a novel murine model of abdominal sepsis. Infect. Immun. 66, 2300‒2309.
Gomez H.G., Gonzalez S.M., Londono J.M., Hoyos N.A., Nino C.D., Leon A.L., Velilla P.A., Rugeles M.T., Jaimes F.A. 2014. Immunological characterization of compensatory anti-inflammatory response syndrome in patients with severe sepsis: A longitudinal study. Crit. Care Med. 42, 771‒780.
Scheiermann P., Hoegl S., Revermann M., Ahluwalia D., Zander J., Boost K.A., Nguyen T., Zwissler B., Muhl H., Hofstetter C. 2009. Cecal ligation and incision: An acute onset model of severe sepsis in rats. J. Surg. Res. 151, 132‒137.
Fink T., Heymann P., Taha-Melitz S., Taha A., Wolf B., Rensing H., Volk T., Mathes A.M. 2013. Dobutamine pretreatment improves survival, liver function, and hepatic microcirculation after polymicrobial sepsis in rat. Shock. 40, 129‒135.
Fink T., Glas M., Wolf A., Kleber A., Reus E., Wolff M., Kiefer D., Wolf B., Rensing H., Volk T., Mathes A.M. 2014. Melatonin receptors mediate improvements of survival in a model of polymicrobial sepsis. Crit. Care Med. 42, e22‒e31.
Korneev K.V., Arbatsky N.P., Molinaro A., Palmigiano A., Shaikhutdinova R.Z., Shneider M.M., Pier G.B., Kondakova A.N., Sviriaeva E.N., Sturiale L., Garozzo D., Kruglov A.A., Nedospasov S.A., Drutskaya M.S., Knirel Y.A., Kuprash D.V. 2015. Structural relationship of the lipid a acyl groups to activation of murine Toll-like receptor 4 by lipopolysaccharides from pathogenic strains of Burkholderia mallei, Acinetobacter baumannii, and Pseudomonas aeruginosa. Front. Immunol. 6, 595.
Korneev K.V., Kondakova A.N., Sviriaeva E.N., Mitkin N.A., Palmigiano A., Kruglov A.A., Telegin G.B., Drutskaya M.S., Sturiale L., Garozzo D., Nedospasov S.A., Knirel Y.A., Kuprash D.V. 2018. Hypoacylated LPS from foodborne pathogen Campylobacter jejuni induces moderate TLR4-mediated inflammatory response in murine macrophages. Front. Cell. Infect. Microbiol. 8, 58.
Stortz J.A., Raymond S.L., Mira J.C., Moldawer L.L., Mohr A.M., Efron P.A. 2017. Murine models of sepsis and trauma: can we bridge the Gap? ILAR J. 58, 90‒105.
Ribes S., Domenech A., Cabellos C., Tubau F., Linares J., Viladrich P.F., Gudiol F. 2003. Experimental meningitis due to a high-level cephalosporin-resistant strain of Streptococcus pneumoniae serotype 23F. Enferm. Infect. Microbiol. Clin. 21, 329‒333.
Svensson M., Yadav M., Holmqvist B., Lutay N., Svanborg C., Godaly G. 2011. Acute pyelonephritis and renal scarring are caused by dysfunctional innate immunity in mCxcr2 heterozygous mice. Kidney Int. 80, 1064‒1072.
Cross A.S., Opal S.M., Sadoff J.C., Gemski P. 1993. Choice of bacteria in animal models of sepsis. Infect. Immun. 61, 2741‒2747.
Sasaki S., Nishikawa S., Miura T., Mizuki M., Yamada K., Madarame H., Tagawa Y.I., Iwakura Y., Nakane A. 2000. Interleukin-4 and interleukin-10 are involved in host resistance to Staphylococcus aureus infection through regulation of gamma interferon. Infect. Immun. 68, 2424‒2430.
Rubins J.B., Pomeroy C. 1997. Role of gamma interferon in the pathogenesis of bacteremic pneumococcal pneumonia. Infect. Immun. 65, 2975‒2977.
van der Poll T., Marchant A., Keogh C.V., Goldman M., Lowry S.F. 1996. Interleukin-10 impairs host defense in murine pneumococcal pneumonia. J. Infect. Dis. 174, 994‒1000.
van der Poll T., Marchant A., Buurman W.A., Berman L., Keogh C.V., Lazarus D.D., Nguyen L., Goldman M., Moldawer L.L., Lowry S.F. 1995. Endogenous IL-10 protects mice from death during septic peritonitis. J. Immunol. 155, 5397‒5401.
Mittrucker H.W., Kaufmann S.H. 2000. Immune response to infection with Salmonella typhimurium in mice. J. Leukoc. Biol. 67, 457‒463.
Nemzek J.A., Hugunin K.M., Opp M.R. 2008. Modeling sepsis in the laboratory: Merging sound science with animal well-being. Comp. Med. 58, 120‒128.
Gonnert F.A., Recknagel P., Seidel M., Jbeily N., Dahlke K., Bockmeyer C.L., Winning J., Losche W., Claus R.A., Bauer M. 2011. Characteristics of clinical sepsis reflected in a reliable and reproducible rodent sepsis model. J. Surg. Res. 170, e123‒e134.
Ko J.J., Mann F.A. 2014. Barium peritonitis in small animals. J. Vet. Med. Sci. 76, 621‒628.
Sviryaeva E.N., Korneev K.V., Drutskaya M.S., Kuprash D.V. 2016. Mechanisms of changes in immune response during bacterial coinfections of the respiratory tract. Biochemistry (Moscow). 81 (11), 1340–1349.
Sviryaeva E.N., Korneev K.V., Drutskaya M.S., Nedospasov S.A., Kuprash D.V. 2016. Modeling of viral–bacterial coinfections at the molecular level using agonists of innate immunity receptors. Dokl. Biochem. Biophys. 471, 393–395.
Lepper P.M., Held T.K., Schneider E.M., Bolke E., Gerlach H., Trautmann M. 2002. Clinical implications of antibiotic-induced endotoxin release in septic shock. Intensive Care Med. 28, 824‒833.
Ben Ari Z., Avlas O., Pappo O., Zilbermints V., Cheporko Y., Bachmetov L., Zemel R., Shainberg A., Sharon E., Grief F., Hochhauser E. 2012. Reduced hepatic injury in Toll-like receptor 4-deficient mice following D-galactosamine/lipopolysaccharide-induced fulminant hepatic failure. Cell Physiol. Biochem. 29, 41‒50.
Kuzmich N.N., Sivak K.V., Chubarev V.N., Porozov Y.B., Savateeva-Lyubimova T.N., Peri F. 2017. TLR4 signaling pathway modulators as potential therapeutics in inflammation and sepsis. Vaccines (Basel). 5, 34.
Wheeler M.D., Kono H., Yin M., Nakagami M., Uesugi T., Arteel G.E., Gabele E., Rusyn I., Yamashina S., Froh M., Adachi Y., Iimuro Y., Bradford B.U., Smutney O.M., Connor H.D., et al. 2001. The role of Kupffer cell oxidant production in early ethanol-induced liver disease. Free Radic. Biol. Med. 31, 1544‒1549.
Lu J.W., Wang H., Yan-Li J., Zhang C., Ning H., Li X.Y., Zhang H., Duan Z.H., Zhao L., Wei W., Xu D.X. 2008. Differential effects of pyrrolidine dithiocarbamate on TNF-alpha-mediated liver injury in two different models of fulminant hepatitis. J. Hepatol. 48, 442‒452.
Hoffmann F., Sass G., Zillies J., Zahler S., Tiegs G., Hartkorn A., Fuchs S., Wagner J., Winter G., Coester C., Gerbes A.L., Vollmar A.M. 2009. A novel technique for selective NF-kappaB inhibition in Kupffer cells: Contrary effects in fulminant hepatitis and ischaemia-reperfusion. Gut. 58, 1670‒1678.
Decker K., Keppler D. 1974. Galactosamine hepatitis: Key role of the nucleotide deficiency period in the pathogenesis of cell injury and cell death. Rev. Physiol. Biochem. Pharmacol. 71, 77‒106.
Leist M., Gantner F., Bohlinger I., Tiegs G., Germann P.G., Wendel A. 1995. Tumor necrosis factor-induced hepatocyte apoptosis precedes liver failure in experimental murine shock models. Am. J. Pathol. 146, 1220‒1234.
Zhou B.R., Gumenscheimer M., Freudenberg M., Galanos C. 2003. A striking correlation between lethal activity and apoptotic DNA fragmentation of liver in response of D-galactosamine-sensitized mice to a non-lethal amount of lipopolysaccharide. Acta Pharmacol. Sin. 24, 193‒198.
Mignon A., Rouquet N., Fabre M., Martin S., Pages J.C., Dhainaut J.F., Kahn A., Briand P., Joulin V. 1999. LPS challenge in D-galactosamine-sensitized mice accounts for caspase-dependent fulminant hepatitis, not for septic shock. Am. J. Respir. Crit. Care Med. 159, 1308‒1315.
Kawaguchi K., Kikuchi S., Hasegawa H., Maruyama H., Morita H., Kumazawa Y. 1999. Suppression of lipopolysaccharide-induced tumor necrosis factor-release and liver injury in mice by naringin. Eur. J. Pharmacol. 368, 245‒250.
Nakama T., Hirono S., Moriuchi A., Hasuike S., Nagata K., Hori T., Ido A., Hayashi K., Tsubouchi H. 2001. Etoposide prevents apoptosis in mouse liver with D-galactosamine/lipopolysaccharide-induced fulminant hepatic failure resulting in reduction of lethality. Hepatology. 33, 1441‒1450.
Silverstein R., Norimatsu M., Morrison D.C. 1997. Fundamental differences during Gram-positive versus Gram-negative sepsis become apparent during bacterial challenge of D-galactosamine-treated mice. J. Endotoxin Res. 4, 173‒181.
Tsutsui H., Imamura M., Fujimoto J., Nakanishi K. 2010. The TLR4/TRIF-mediated activation of NLRP3 inflammasome underlies endotoxin-induced liver injury in mice. Gastroenterol. Res. Pract. 2010, 641865.
Yang P., Zhou W., Li C., Zhang M., Jiang Y., Jiang R., Ba H., Li C., Wang J., Yin B., Gong F., Li Z. 2016. Kupffer-cell-expressed transmembrane TNF-alpha is a major contributor to lipopolysaccharide and D-galactosamine-induced liver injury. Cell Tissue Res. 363, 371‒383.
Lawson J.A., Burns A.R., Farhood A., Lynn Bajt M., Collins R.G., Smith C.W., Jaeschke H. 2000. Pathophysiologic importance of E- and L-selectin for neutrophil-induced liver injury during endotoxemia in mice. Hepatology. 32, 990‒998.
Bajt M.L., Farhood A., Jaeschke H. 2001. Effects of CXC chemokines on neutrophil activation and sequestration in hepatic vasculature. Am. J. Physiol. Gastrointest. Liver Physiol. 281, G1188‒G1195.
Dorman R.B., Gujral J.S., Bajt M.L., Farhood A., Jaeschke H. 2005. Generation and functional significance of CXC chemokines for neutrophil-induced liver injury during endotoxemia. Am. J. Physiol. Gastrointest Liver Physiol. 288, G880‒886.
Jaeschke H. 2006. Mechanisms of liver injury: 2. Mechanisms of neutrophil-induced liver cell injury during hepatic ischemia-reperfusion and other acute inflammatory conditions. Am. J. Physiol. Gastrointest Liver Physiol. 290, G1083‒1088.
Zimmermann H.W., Trautwein C., Tacke F. 2012. Functional role of monocytes and macrophages for the inflammatory response in acute liver injury. Front. Physiol. 3, 56.
Liong E.C., Xiao J., Lau T.Y., Nanji A.A., Tipoe G.L. 2012. Cyclooxygenase inhibitors protect D-galactosamine/lipopolysaccharide induced acute hepatic injury in experimental mice model. Food Chem. Toxicol. 50, 861‒866.
Zhou H., Tang L., Yang Y., Lin L., Dai J., Ge P., Ai Q., Jiang R., Zhang L. 2018. Dopamine alleviated acute liver injury induced by lipopolysaccharide/D-galactosamine in mice. Int. Immunopharmacol. 61, 249‒255.
Wang Y.Y., Diao B.Z., Zhong L.H., Lu B.L., Cheng Y., Yu L., Zhu L.Y. 2018. Maslinic acid protects against lipopolysaccharide/D-galactosamine-induced acute liver injury in mice. Microb. Pathog. 119, 49‒53.
Hu J.J., Wang H., Pan C.W., Lin M.X. 2018. Isovitexin alleviates liver injury induced by lipopolysaccharide/D-galactosamine by activating Nrf2 and inhibiting NF-kappaB activation. Microb. Pathog. 119, 86‒92.
Liu T.G., Sha K.H., Zhang L.G., Liu X.X., Yang F., Cheng J.Y. 2019. Protective effects of alpinetin on lipopolysaccharide/D-galactosamine-induced liver injury through inhibiting inflammatory and oxidative responses. Microb. Pathog. 126, 239‒244.
Pickkers P., Mehta R.L., Murray P.T., Joannidis M., Molitoris B.A., Kellum J.A., Bachler M., Hoste E.A.J., Hoiting O., Krell K., Ostermann M., Rozendaal W., Valkonen M., Brealey D., Beishuizen A., et al. 2018. Effect of human recombinant alkaline phosphatase on 7-day creatinine clearance in patients with sepsis-associated acute kidney injury: A randomized clinical trial. J. Am. Med. Assoc. 320, 1998‒2009.
Ong G.L., Mattes M.J. 1989. Mouse strains with typical mammalian levels of complement activity. J. Immunol. Methods. 125, 147‒158.
Ratelade J., Verkman A.S. 2014. Inhibitor(s) of the classical complement pathway in mouse serum limit the utility of mice as experimental models of neuromyelitis optica. Mol. Immunol. 62, 104‒113.
Lewis A.J., Rosengart M.R. 2018. Bench-to-bedside: A translational perspective on murine models of sepsis. Surg. Infect. (Larchmt). 19, 137‒141.
Beura L.K., Hamilton S.E., Bi K., Schenkel J.M., Odumade O.A., Casey K.A., Thompson E.A., Fraser K.A., Rosato P.C., Filali-Mouhim A., Sekaly R.P., Jenkins M.K., Vezys V., Haining W.N., Jameson S.C., Masopust D. 2016. Normalizing the environment recapitulates adult human immune traits in laboratory mice. Nature. 532, 512‒516.
Turner P.V. 2018. The role of the gut microbiota on animal model reproducibility. Animal. Model Exp. Med. 1, 109‒115.
Masopust D., Sivula C.P., Jameson S.C. 2017. Of mice, dirty mice, and men: Using mice to understand human immunology. J. Immunol. 199, 383‒388.
Seboxa T., Amogne W., Abebe W., Tsegaye T., Azazh A., Hailu W., Fufa K., Grude N., Henriksen T.H. 2015. High mortality from blood stream infection in Addis Ababa, Ethiopia, is due to antimicrobial resistance. PLoS One. 10, e0144944.
Chen L., Welty-Wolf K.E., Kraft B.D. 2019. Nonhuman primate species as models of human bacterial sepsis. Lab. Anim. (New York). 48, 57‒65.
Saito H., Sherwood E.R., Varma T.K., Evers B.M. 2003. Effects of aging on mortality, hypothermia, and cytokine induction in mice with endotoxemia or sepsis. Mech. Ageing Dev. 124, 1047‒1058.
Howell G.M., Gomez H., Collage R.D., Loughran P., Zhang X., Escobar D.A., Billiar T.R., Zuckerbraun B.S., Rosengart M.R. 2013. Augmenting autophagy to treat acute kidney injury during endotoxemia in mice. PLoS One. 8, e69520.
Ernst W., Zimara N., Hanses F., Mannel D.N., Seelbach-Gobel B., Wege A.K. 2013. Humanized mice, a new model to study the influence of drug treatment on neonatal sepsis. Infect. Immun. 81, 1520‒1531.
Turnbull I.R., Clark A.T., Stromberg P.E., Dixon D.J., Woolsey C.A., Davis C.G., Hotchkiss R.S., Buchman T.G., Coopersmith C.M. 2009. Effects of aging on the immunopathologic response to sepsis. Crit. Care Med. 37, 1018‒1023.
Mege J.L., Bretelle F., Leone M. 2018. Sex and bacterial infectious diseases. New Microbes New Infect. 26, S100‒S103.
Seok J., Warren H.S., Cuenca A.G., Mindrinos M.N., Baker H.V., Xu W., Richards D.R., McDonald-Smith G.P., Gao H., Hennessy L., Finnerty C.C., Lopez C.M., Honari S., Moore E.E., Minei J.P., et al. 2013. Genomic responses in mouse models poorly mimic human inflammatory diseases. Proc. Natl. Acad. Sci. U. S. A. 110, 3507‒3512.
Osuchowski M.F., Remick D.G., Lederer J.A., Lang C.H., Aasen A.O., Aibiki M., Azevedo L.C., Bahrami S., Boros M., Cooney R., Cuzzocrea S., Jiang Y., Junger W.G., Hirasawa H., Hotchkiss R.S., et al. 2014. Abandon the mouse research ship? Not just yet! Shock. 41, 463‒475.
Takao K., Miyakawa T. 2015. Genomic responses in mouse models greatly mimic human inflammatory diseases. Proc. Natl. Acad. Sci. U. S. A. 112, 1167‒1172.
Efron P.A., Mohr A.M., Moore F.A., Moldawer L.L. 2015. The future of murine sepsis and trauma research models. J. Leukoc. Biol. 98, 945‒952.
Laudanski K., Lapko N., Zawadka M., Zhou B.X., Danet-Desnoyers G., Worthen G.S. 2017. The clinical and immunological performance of 28 days survival model of cecal ligation and puncture in humanized mice. PLoS One. 12, e0180377.
Parker D. 2017. Humanized mouse models of Staphylococcus aureus infection. Front Immunol. 8, 512.
Schlieckau F., Schulz D., Fill Malfertheiner S., Entleutner K., Seelbach-Goebel B., Ernst W. 2018. A novel model to study neonatal Escherichia coli sepsis and the effect of treatment on the human immune system using humanized mice. Am. J. Reprod. Immunol. 80, e12859.
Lapko N., Zawadka M., Polosak J., Worthen G.S., Danet-Desnoyers G., Puzianowska-Kuznicka M., Laudanski K. 2017. Long-term monocyte dysfunction after sepsis in humanized mice is related to persisted activation of macrophage-colony stimulation factor (M-CSF) and demethylation of PU.1, and it can be reversed by blocking M-CSF in vitro or by transplanting naive autologous stem cells in vivo. Front. Immunol. 8, 401.
Unsinger J., McDonough J.S., Shultz L.D., Ferguson T.A., Hotchkiss R.S. 2009. Sepsis-induced human lymphocyte apoptosis and cytokine production in “humanized” mice. J. Leukoc. Biol. 86, 219‒227.
Laudanski K., Stentz M., DiMeglio M., Furey W., Steinberg T., Patel A. 2018. Potential pitfalls of the humanized mice in modeling sepsis. Int. J. Inflam. 2018, 6563454.
Deutschman C.S., Tracey K.J. 2014. Sepsis: Current dogma and new perspectives. Immunity. 40, 463‒475.
Melican K., Michea Veloso P., Martin T., Bruneval P., Dumenil G. 2013. Adhesion of Neisseria meningitidis to dermal vessels leads to local vascular damage and purpura in a humanized mouse model. PLoS Pathog. 9, e1003139.
Rongvaux A., Willinger T., Martinek J., Strowig T., Gearty S.V., Teichmann L.L., Saito Y., Marches F., Halene S., Palucka A.K., Manz M.G., Flavell R.A. 2014. Development and function of human innate immune cells in a humanized mouse model. Nat. Biotechnol. 32, 364‒372.
Osuchowski M.F., Thiemermann C., Remick D.G. 2017. Sepsis-3 on the block: What does it mean for preclinical sepsis modeling? Shock. 47, 658‒660.
Shrum B., Anantha R.V., Xu S.X., Donnelly M., Haeryfar S.M., McCormick J.K., Mele T. 2014. A robust scoring system to evaluate sepsis severity in an animal model. BMC Res. Notes. 7, 233.
Poltorak A., He X., Smirnova I., Liu M.Y., Van Huffel C., Du X., Birdwell D., Alejos E., Silva M., Galanos C., Freudenberg M., Ricciardi-Castagnoli P., Layton B., Beutler B. 1998. Defective LPS signaling in C3H/HeJ and C57BL/10ScCr mice: Mutations in Tlr4 gene. Science. 282, 2085‒2088.
Daubeuf B., Mathison J., Spiller S., Hugues S., Herren S., Ferlin W., Kosco-Vilbois M., Wagner H., Kirschning C.J., Ulevitch R., Elson G. 2007. TLR4/ MD-2 monoclonal antibody therapy affords protection in experimental models of septic shock. J. Immunol. 179, 6107‒6114.
Cao C., Chai Y., Shou S., Wang J., Huang Y., Ma T. 2018. Toll-like receptor 4 deficiency increases resistance in sepsis-induced immune dysfunction. Int. Immunopharmacol. 54, 169‒176.
Weighardt H., Kaiser-Moore S., Vabulas R.M., Kirschning C.J., Wagner H., Holzmann B. 2002. Cutting edge: Myeloid differentiation factor 88 deficiency improves resistance against sepsis caused by polymicrobial infection. J. Immunol. 169, 2823‒2827.
Echtenacher B., Freudenberg M.A., Jack R.S., Mannel D.N. 2001. Differences in innate defense mechanisms in endotoxemia and polymicrobial septic peritonitis. Infect. Immun. 69, 7271‒7276.
Feterowski C., Emmanuilidis K., Miethke T., Gerauer K., Rump M., Ulm K., Holzmann B., Weighardt H. 2003. Effects of functional Toll-like receptor-4 mutations on the immune response to human and experimental sepsis. Immunology. 109, 426‒431.
Entleutner M., Traeger T., Westerholt A., Holzmann B., Stier A., Pfeffer K., Maier S., Heidecke C.D. 2006. Impact of interleukin-12, oxidative burst, and iNOS on the survival of murine fecal peritonitis. Int. J. Colorectal Dis. 21, 64‒70.
Napier B.A., Brubaker S.W., Sweeney T.E., Monette P., Rothmeier G.H., Gertsvolf N.A., Puschnik A., Carette J.E., Khatri P., Monack D.M. 2016. Complement pathway amplifies caspase-11-dependent cell death and endotoxin-induced sepsis severity. J. Exp. Med. 213, 2365‒2382.
Ward P.A., Fattahi F. 2019. New strategies for treatment of infectious sepsis. J. Leukoc. Biol. https://doi.org/10.1002/JLB.4MJR1118-425R
Patil N.K., Guo Y., Luan L., Sherwood E.R. 2017. Targeting immune cell checkpoints during sepsis. Int. J. Mol. Sci. 18, E2413.
Shin J., Jin M. 2017. Potential immunotherapeutics for immunosuppression in sepsis. Biomol. Ther. (Seoul). 25, 569‒577.
Brown K.A., Brown G.A., Lewis S.M., Beale R., Treacher D.F. 2016. Targeting cytokines as a treatment for patients with sepsis: A lost cause or a strategy still worthy of pursuit? Int. Immunopharmacol. 36, 291‒299.
Guo Y., Luan L., Patil N.K., Wang J., Bohannon J.K., Rabacal W., Fensterheim B.A., Hernandez A., Sherwood E.R. 2017. IL-15 enables septic shock by maintaining NK cell integrity and function. J. Immunol. 198, 1320‒1333.
Alves-Filho J.C., Sonego F., Souto F.O., Freitas A., Verri W.A., Jr., Auxiliadora-Martins M., Basile-Filho A., McKenzie A.N., Xu D., Cunha F.Q., Liew F.Y. 2010. Interleukin-33 attenuates sepsis by enhancing neutrophil influx to the site of infection. Nat. Med. 16, 708‒712.
Limongi D., D’Agostini C., Ciotti M. 2016. New sepsis biomarkers. Asian Pacific J. Trop. Biomed. 6, 516‒519.
Ueno T., Ikeda T., Yokoyama T., Kihara Y., Konno O., Nakamura Y., Iwamoto H., Shimizu T., McGrath M.M., Chandraker A. 2016. Reduction in circulating level of HMGB-1 following continuous renal replacement therapy in sepsis. Cytokine. 83, 206‒209.
Nahid M.A., Satoh M., Chan E.K. 2011. Mechanistic role of microRNA-146a in endotoxin-induced differential cross-regulation of TLR signaling. J. Immunol. 186, 1723‒1734.
Wang J.F., Yu M.L., Yu G., Bian J.J., Deng X.M., Wan X.J., Zhu K.M. 2010. Serum miR-146a and miR-223 as potential new biomarkers for sepsis. Biochem. Biophys. Res. Commun. 394, 184‒188.
Pop-Began V., Paunescu V., Grigorean V., Pop-Began D., Popescu C. 2014. Molecular mechanisms in the pathogenesis of sepsis. J. Med. Life. 7 (2), 38‒41.
Heming N., Lamothe L., Ambrosi X., Annane D. 2016. Emerging drugs for the treatment of sepsis. Expert Opin. Emerg. Drugs. 21, 27‒37.
McIntyre L.A., Stewart D.J., Mei S.H.J., Courtman D., Watpool I., Granton J., Marshall J., Dos Santos C., Walley K.R., Winston B.W., Schlosser K., Fergusson D.A., Canadian Critical Care Trials G., Canadian Critical Care Translational Biology G. 2018. Cellular immunotherapy for septic shock. A phase I clinical trial. Am. J. Respir. Crit. Care Med. 197, 337‒347.
Krasnodembskaya A., Samarani G., Song Y., Zhuo H., Su X., Lee J.W., Gupta N., Petrini M., Matthay M.A. 2012. Human mesenchymal stem cells reduce mortality and bacteremia in Gram-negative sepsis in mice in part by enhancing the phagocytic activity of blood monocytes. Am. J. Physiol. Lung Cell Mol. Physiol. 302, L1003‒L1013.
Lewis A., Zuckerbraun B., Griepentrog J., Zhang X., Rosengart M. 2017. Reducing animal use with a biotelemetry-enhanced murine model of sepsis. Sci. Rep. 7, 6622.
ACKNOWLEDGMENTS
I am grateful to D.V. Kuprash for careful reading of the manuscript and helpful advice.
Funding
This work was supported by the Program of fundamental research for state academies for 2013–2020 (research topic no. 01201363823).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The authors declare that they have no conflict of interest. This article does not contain any studies involving animals or human participants performed by any of the authors.
Additional information
Translated by T. Tkacheva
Abbreviations: LPS, lipopolysaccharide; D-GalN, D-galactosamine; PRR, pattern recognition receptor; DAMP, damage-associated molecular pattern; CLP, cecal ligation and puncture; CASP, colon ascendens stent peritonitis.
Rights and permissions
About this article

Cite this article
Korneev, K.V. Mouse Models of Sepsis and Septic Shock. Mol Biol 53, 704–717 (2019). https://doi.org/10.1134/S0026893319050108
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1134/S0026893319050108