
Abstract
Population aging is a global phenomenon due to declining birth rates and increased life expectancy. This demographic shift poses a challenge to society, requiring adaptation of policies, economies, and healthcare systems to safeguard the well-being of older individuals. Health inequalities, influenced by social determinants such as education, economic status, and place of residence, impact this population group, with notable differences between men and women. Several studies have demonstrated that social determinants of health (SDH) affect the quality of life (QoL) of older individuals, especially women. In general, women report lower quality of life indicators, lower educational levels, and poorer health compared to men. This study aims to examine how social determinants of health can influence the quality of life of the population aged 50 or older in different European countries, from a sex perspective, through a longitudinal approach. The main SDHs associated with poorer QoL were female sex advanced age, economic hardship, educational level, and geographic location within Europe. Depression in women and men in Southern Europe was associated with a decrease in QoL scores.
Similar content being viewed by others

Introduction
Population aging is a global phenomenon that is transforming the demographic structure due to declining birth rates and increasing life expectancy (United Nations, 2019), (National Institute of Statistics, 2020). According to the World Health Organization (WHO), it is expected that by 2050, 22% of the global population will be over 60 years old, compared to 12% in 2015 (World Health Organization., 2011). This shift represents a considerable challenge for society (United Nations, 2021). To protect the well-being of older people and promote healthy and fulfilling aging, countries must adapt their policies, economies, social structures, and healthcare systems (Serdà Ferrer, 2014), (Palomino Moral et al., 2014), as inaction can lead to significant problems of health inequalities. Therefore, it is important to address health inequalities that affect this population group, especially between men and women, which may be influenced by social determinants of health (SDHs), such as age, educational level, economic status, immigrant status, and place of residence, both internationally and within each country (Phelan et al., 2010), (Arcaya et al., 2015a).
In 2008, the Commission on Social Determinants of Health defined SDHs as a set of personal, social, economic, and environmental factors that influence the health status of individuals and populations, becoming the most widely used model in SDHs research (World Health Organization, 1998), (World Health Organization, 2008). These determinants have an impact on opportunities for good health and highlight the existence of sex-based health inequalities (Salgado-de Snyder, Wong, 2007) based on power, prestige, and access to resources (Marmot, 2007). Recent studies have demonstrated a direct relationship between SDHs and quality of life (QoL) among individuals with fewer economic resources (García Ramírez et al., (2017), those who are older, and women (Mejía Reyes, 2021). These determinants influence the QoL of older people, which is a multidimensional construct essential for social well-being and satisfaction of basic needs. QoL encompasses both objective and subjective aspects of the individual, and the WHO defines it as “an individual’s perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards, and concerns,” which is widely accepted by most authors (World Health Organization, 1996).
Several studies have been conducted on how objective health aspects influence the QoL of older individuals in Europe, such as multimorbidity (Fernández et al., 2020), chronic diseases (Sexton et al., 2015), limitations in activities of daily living, and the presence of depression, all of which have a significantly negative impact on their QoL. Structural SDHs like economic status, lack of material resources (Zaninotto et al., 2009), sex, and educational level also influence the QoL of this population group, especially in women. Women generally report poorer QoL indicators, lower levels of education, and poorer health compared to men (Ahrenfeldt & Möller, 2021).
Recently, the influence of family trajectories on perceived QoL in old age has been studied in Spain using the Spanish cohort of the Survey of Health, Ageing, and Retirement in Europe (SHARE) in waves 3 (2009) and 7 (2017), and it was found that subjective aspects such as social relationships and life as a couple affect the QoL of men and women differently, whereby men with stable partners and offspring perceived a better QoL compared to women in similar conditions (Fernández-Carro & Gumà, 2022).
Although previous studies on SDHs and their influence on QoL have been conducted, to our knowledge, no specific research has been conducted out among individuals aged 50 years and older from different European regions with a differentiated focus on men and women, to analyze how SDHs can affect the evolution of their QoL.
Hypothesis: SDHs, such as age, educational level, economic status, immigrant status, and place of residence, will influence the evolution of the Quality of Life (QoL) of individuals over 50 years old, and there will be differences based on sex and the European region where they reside.
Objective: To analyze how SDH, such as age, educational level, economic status, immigrant status and place of residence, influence QoL in individuals over 50 years of age in several European countries, according to sex and the European region where they reside in a longitudinal study.
Materials and methods
This was a population-based, analytical, and prospective cohort study that used data collected in the fifth, sixth, and seventh waves of the SHARE study conducted in 2013, 2015, and 2017, respectively (Malter, Börsch-Supan, 2015).
The SHARE study has standardized fieldwork procedures, minimizing country-specific artefacts that could interfere with cross-country comparisons. SHARE is a multinational survey that involves differences in sampling resources between countries. Consequently, sample frames are chosen according to the best available resources in each country to achieve total probabilistic sampling. (Börsch-Supan et al., 2013). It is a longitudinal study at the European level that provides primary data. (Börsch-Supan A, 2005).
The information was obtained through computer-assisted personal interviewing (CAPI) with an approximate duration of 90 minutes conducted in the home of each participant and uniformly for all participants (Börsch-Supan et al., 2013). The data are available to the scientific community free of charge at www.share-project.org after registration.
Participants
In the fifth wave of the SHARE study conducted in 2013, a total of 59,421 individuals from 13 selected European countries were surveyed, including Germany, Austria, Belgium, Denmark, Slovenia, Spain, Estonia, France, Italy, Luxembourg, Sweden, Switzerland, and the Czech Republic. The selection criteria for this study required participants to be 50 years or older, reside regularly in one of the 13 European countries analyzed in the fifth wave, agree to participate in this study, and have participated in the three consecutive waves under study. Of the respondents, 11,493 met these inclusion criteria. The remaining participants did not participate in the consecutive waves or in any of them due to dropout or death (Bergmann et al., 2019) Fig. 1.

Total respondents Wave 5, participants, non-participants in some of the following waves (6 and 7) object of study and total sample studied.
A comparative analysis was conducted between the participants in the study and non-participants from Wave 5 of recruitment, resulting in a sample of female participants lower than that of non-participants (54.3% vs. 56.5%), with a younger mean age 64.2 (SD 9.8) vs. 67.0 (SD 10.2) and higher CASP-12 scores 38.3 (SD 6.3) vs. 37.6 (SD 6.3) as the most relevant data.
To address these significant differences, probably because the analyzed sample of participants was younger than that of nonparticipants, a random selection of nonparticipants was performed. A copy of the method used can be downloaded from a repository on GitHub (Vila 2024). First, two separate datasets were created: one with participants and another with non-participants. An algorithm was implemented that, in a loop, iterated through all the records in the participant dataset. For each participant, the following steps were taken: a participant was selected, non-participants with the same sex and age (±2 years) were preselected, and one of them was randomly chosen, forming a “pair.” This pair was added to a third dataset called “pair” and removed from their original datasets (participant or non-participant). This process was repeated for each participant, ultimately generating a “pair” dataset containing participant identifiers, non-participant pairs, and pair identifiers. This “pair” dataset was merged with the original dataset to obtain CASP values. Thus, among non-participants of the same age, sex, and European region, CASP-12 scores were very similar 38.3 (SD 6.29) vs. 38.2 (SD 6.19).
Therefore, it could be assumed that participants in the three consecutive waves of the study are representative of a slightly younger fraction with a slightly lower percentage of women in all European regions compared to those who participated in Wave 5. The complete data are shown in the Supplementary Material, Table S1.
The countries were grouped according to the four regional clusters defined in a 2013 report by the European Commission, which corresponds to different models of social welfare: Northern Europe, with a social democratic regime (Denmark and Sweden, n = 2747); Continental Europe, with a corporatist regime (Austria, Germany, Belgium, France, Luxembourg, and Switzerland, n = 4443); Southern Europe, with a southern European regime (Spain and Italy, n = 2,770); and Eastern Europe, with a post-socialist regime (Slovenia, Estonia, and the Czech Republic, n = 1,533) (Abdallah et al., 2013).
Study variables
Outcome variable
This study assessed participants’ QoL using the control, autonomy, satisfaction, and self-realization (CASP-12) scale (Wiggins et al., 2008), a specific and validated tool consisting of four subscales with three items each: control, autonomy, satisfaction, and self-realization. Each item is rated on a Likert scale from 1 (never) to 4 (often). The total score ranges between 12 and 48 points, with a higher score indicating better QoL. Scores below 35 indicate low QoL, 35 to 37 indicate moderate QoL, 38 to 39 indicate high QoL, and 39 to 48 indicate very high QoL. The multidimensional model for the CASP-12, it has potential for use as a multidimensional tool for assessing quality of life in older people. This scale has a Cronbach’s alpha coefficient of 0.84 (Hyde et al., 2003), (Pérez-Rojo et al., 2018).
Explanatory variables
This study was based on the 2008 WHO SDH model “Commission on Social Determinants of Health” that addresses health inequalities, and by consensus of the authors and based on literature we used the following determinants: sex, age group, educational level, economic level, autochthonous or emigrant and place of residence. Our focus is primarily on the individual level (Arcaya et al., 2015b).
Data on SDHs were collected through questions related to age range, it has been grouped by interest groups, the age range 50–64 years (active in the workforce), 65–74 years (recently retired senior), 75–84 years (older adult) and over 85 years (older persons of more advanced age), educational level, according to the International Standard Classification of Education (ISCED), the original seven categories of ISCED were reorganized to enhance analysis into the following groups: low educational level (corresponding to ISCED 0–2, basic or lower secondary education), medium educational level (ISCED 3–4, upper secondary education), and high educational level (ISCED 5–6, tertiary education). (United Nations Educational Scientific and Cultural Organization, 1997), (United Nations Educational Scientific and Cultural Organization, 2011), economic level, the SHARE study determines the economic level using the variable “making ends meet” with the options: 1. Very easily, 2. Quite easily, 3. With difficulties, 4. With many difficulties. For the analysis in this study, it has been dichotomized into 1. No difficulty 2. Difficulty. Additionally, the variable Received external financial help is used with options: 1. Yes, 2. No. Origin of the person (native or immigrant). Place of residence (the variable “residential area” is a self-reported variable in the SHARE study, classified as: 1. A big city; 2. The suburbs or outskirts of a big city; 3. A large town; 4.A small town; 5. A rural area or village). For the analysis in this study, the variables 1, 2, and 3 have been grouped into category 1: urban, and the variables 4 and 5 have been grouped into category 2: rural (European Commission, 2010), and European region (north, continental, south, and east).
Covariates
Sociodemographic variables included data on marital status (married, divorced, single, widowed), employment status (retired, employed, unemployed, disabled, homemaking), for this study has been dichotomized into (Present worker: yes or no), family composition (living alone, living with a partner, living with 3 or more people), number of children (no children, 1 to 2, 3 or more), and number of grandchildren (no grandchildren, 1 to 4, 5 or more).
Clinical variables, Self-perceived health (excellent/very good, good, fair, poor), number of chronic diseases (none, 1–2, 3 or more), and mobility difficulties (without difficulty, with difficulty) were evaluated. Physical activity, in the SHARE study, it was analyzed as an ordinal scale with vigorous physical activity categorized as: 1. More than once a week 2. Once a week 3. From one to three times a month 4. Almost never or never. For this study, variables 1 and 2 were grouped into category 1: active, and variables 3 and 4 were grouped into category 2: inactive (Paxton et al., 2010), (Reitlo et al., 2018), was also assessed. The EURO-D scale with 12 items, a specific and validated tool in a previous trans-European study on the prevalence of depression, EURODEP, for measuring the presence of depressive symptoms in older adults in European countries, was used with a maximum score of 12 (very depressed) and a minimum of 0 (not depressed), and a cutoff point of 4 indicated the presence of depression. This scale has a Cronbach’s alpha coefficient between 0.62 and 0.78 (Castro‐Costa et al., 2008), (Prince et al., 1999). Additionally, body mass index (the BMI variable is classified into standard categories determined by the World Health Organization (1995): “Underweight” (<18.5), “Normal weight” (18.5–24.9), “Overweight” (25–29.9), and “Obesity” (>30) (World Health Organization, 1995), (Collins et al., 2016), daily tobacco consumption (according to the SHARE survey, individuals are classified into: present smokers or non-smokers/ex-smoker, and alcohol consumption (does not drink or consumes alcohol less than 1–2 times a month, between 1 and 4 days a week, almost every day) were collected.
Statistical analysis
SHARE is a general-purpose survey used for both inferring about finite populations and inferring about data generation processes defined by models. The units of analysis include both individuals and households and provides calibrated design weights. To minimize potential selection bias across different countries, SHARE calculates calibrated weights to use weighted statistical samples that enable inference.
Please refer to the SHARE Sampling Procedures and Calibrated Design Weights for more details. (Börsch-Supan A, 2005).
Descriptive statistics was reported with mean and standard deviation for numerical variables while absolute frequencies and relative percentages were used for categorical variables. Chi-square and the Student-t test were used in the univariate analysis. Univariate results were stratified by European region and sex (male-female). The linearity effect of numerical variables on QoL was assessed. A skewed distribution was observed in the number of children and grandchildren and therefore both variables were grouped into categories, according to what was suggested by means of smoothing spline regression. Furthermore, multicollinearity among predictor variables was assessed by means of the Generalized Variance-Inflation Factor (gVIF). The maximum gVIF of 1.22 was found, indicating no multicollinearity issues.
To analyze the direct effect of Sex on QoL, crude and multivariate models were performed using linear mixed-effects models with the lmer function from the lme4 package in R software (Bates et al., 2015). All models included participant Identifier as random intercept. Only Sex was added to get the crude model. To get estimates of the direct effect of Sex for specific age groups or regions, instead of stratifying (i.e., sub-setting), at the crude model the Wave, the European Region, and the Age Groups were included. This model was named ‘adjusted’ and then, by changing as appropriate the reference category, the estimates of the direct sex-effect was obtained for each age group or for each region. The statistical Sex*Region and the Sex*Age Group interaction was also tested. Estimates of differences on QoL of some relevant determinants of health stratified by sex, were obtained including one of each health determinant as explanatory QoL.
The data were analyzed with the SPSS-25 program (Statistical Package for the Social Sciences, IBM Corp. Armonk, NY, USA) and with R version 4.3.0, a language and environment for statistical computing from the Foundation for Statistical Computing, Vienna, Austria. A significant difference was considered when the p-value was less than 0.05.
Results
Participant characteristics at the follow-up starting moment (wave 5 of the SHARE study) according to European region and Sex
In the fifth wave baseline, differences were observed between men and women when analyzing the SDHs of all participants. The average age for women was 63.3 (SD 10.2) years, while for men, it was 64.4 (SD 9.4) years. The most represented age group was the 50–64 age group, encompassing 54.4% of women and 50.0% of men (p < 0.001). Regarding education, 37.0% of women had a low education level compared to 32.9% of men (p < 0.001). Economic difficulty was observed in 30.5% of women and 26.7% of men (p < 0.001). Additionally, over 90% of respondents of both sexes were native to the country where the interview took place.
When analyzing the sociodemographic and clinical variables, notable differences were found between men and women. Regarding marital status, most participants of both sexes were married, but there was a higher proportion of widows (13.4%) than widowers (4.5%) (p < 0.001), as well as a higher proportion of women living alone than men (19.4% vs. 12.6%) (p < 0.001). Self-perceived health was significantly lower among women (p = 0.034). Although participants of both sexes had few mobility difficulties, they were more common among women (p < 0.001). Physical inactivity was more frequent among women (49.8%) than among men (42.4%) (p < 0.001). Additionally, tobacco and alcohol consumption were significantly higher among men than among women (p < 0,001). Regarding depression (EURO-D), a significant difference was observed between women (30.3%) and men (17.5%) (p < 0.001).
Significant differences were observed in terms of sex and European region. Regarding SDHs, the southern region had an older population of people of both sexes, with 6% of women over 85 years of age. In contrast, the continental and northern regions had the lowest proportions of this age group, at 2.3% and 2.4%, respectively (p < 0.001). In terms of educational level, the southern region showed the highest percentage of women with a low education level, 76.3% of the respondents, while in the northern region, this proportion was 23.7% (p < 0.001). In relation to economic difficulty in making ends meet, the eastern and southern regions had the highest percentages, especially among women, with 50.8% and 46.1%, respectively, compared to 13.4% in the northern region and 23.7% in the continental region (p < 0.001). In terms of nativity, the continental region had a proportion of 16% of respondents of both sexes who were not native to the country of residence, while in the southern region, this percentage was 4.8% (p < 0.001).
For complete data, refer to Table 1.
Relationship between QoL and SDHs and covariates differentiated by sex, region, in wave 5 and consecutive waves 6 and 7
In the fifth wave, a lower QoL score was observed in the southern region of Europe for both sexes, with the most significant differences observed between women in the southern region and women in the northern region, 35.0 (SD 6.55) vs. 40.7 (SD 5.17) (p < 0.001), respectively. This trend also persisted in subsequent waves (6 and 7). In all European regions, men obtained higher QoL scores than women, although the sex difference was smaller in the northern region of Europe in all waves (p < 0.001). Furthermore, the score decreased with age for both sexes and in all European regions and consecutive waves (p < 0.001).
Regarding educational level, women in the southern region of Europe with a low level of education obtained the lowest QoL score, 34.3 (SD 6.62), compared to men, 35.6 (SD 6.32) (p < 0.001), and this trend persisted during the follow-up. The variable that showed the greatest significant sex differences in QoL scores in all European regions and consecutive waves was economic difficulty, which was notably lower in the southern region and among women, score 32.7(SD 6.44) vs score 34.2(SD 6.28) the men (p < 0.001). Additionally, in all waves, both native men and women obtained a better score than immigrants, except in the southern region of Europe. In the fifth wave, both male and female respondents from all European regions who lived with a partner obtained a higher QoL score than those who lived alone. The score was always higher for men living with a partner, except in the northern region. The difference was significantly greater between women and men in the southern region, 35.0 (SD 6.68) vs 36.2 (SD 6.28) respectively (p = 0.03).
Self-perceived health was a variable with large differences in QoL scores between regions; women in the southern region obtained lower scores in quality of life related to dismal self-perceived health compared to women in the northern region, 27.8 (SD 5.78) vs. 32.8 (SD 7.08) (p < 0.001), respectively.
Regarding lifestyle, no significant differences in QoL scores related to smoking habits were found between regions or sexes, except in the Southern European region, where male nonsmokers obtained a significantly higher QoL score than female nonsmokers 36.2 (SD 6.12) vs 34.9 (SD 6.41) (p < 0.001). Regarding alcohol consumption, individuals of both sexes who consumed alcohol moderately (1–4 days/week) obtained the highest scores in all regions. Women who consumed alcohol daily in the Eastern European region scored higher, 39.6 (SD 5.71), compared to non-consumers 36.7 (SD 6.34) (p < 0.001) and compared to men, 38.6 (SD 6.19) (p < 0.001). The presence of depression showed a significant decrease in QoL score in both women and men in all regions, with the lowest score among respondents from Eastern and Southern Europe relative to the other regions. For complete data, refer to Table 2. For more details on consecutive waves 6 and 7 see Supplementary Material. Tables S2 and S3.
Differences in QoL in some relevant health determinants in Wave 5 and consecutive waves (6 and 7)
Over the four years of longitudinal follow-up, starting from the reference Wave 5, both sexes experienced a significant decrease in QoL score (β Wave-7, Women = −0.430, 95% CI: −0.580; −0.280/Men = −0.293, 95% CI: −0.455; −0.132). The between sex comparison of these slopes did not reach statistical significance (p-value = 0.225). (see Table 3)
In both sexes the QoL worsened with age, with the highest decrease observed in the older group (β-Women = −4.311, 95% CI: −4.826; −3.797/Men = −2.890, 95% CI: −3.446–2.2334) with statistically significant differences between sexes (p-value < 0.001).
Participants of both sexes with medium and high level of education achieved a better QoL score than those with a low level of education during follow-up. These differences were significantly greater among women than among men (p-value: Medium = 0.034, High = 0.033) showing that educational level had a greater influence on QoL among women than among men over time.
During the follow-up, women and men without economic difficulty achieved a better QoL scores (β-Women = 3.447, 95% CI:3.249; 3.646/Men = 3.265, 95% CI: 3.046; 2.334). The between sex comparison of these slopes did not reach statistical significance (p-value = 0.100).
Conversely, needing external financial assistance significantly showed a worsening of QoL, with marginally statistical differences among sexes (p-value 0.079).
Living in a rural area or in a suburb of major city showed a significant protective factor in QoL evolution for women, although this effect was not observed in men. Nevertheless, women vs men comparison did not achieve statistically significance.
Differences in QoL scores were observed among interviewees of both sexes according to their region of residence, where Continental and especially North region achieved better scores in both sexes. And what is more, in the North region women presented significant better scores than men (p-value = 0.002). For complete data, refer to Table 3.
Differences in quality of life by sex according to regions and age groups
A multivariate model was performed to determine the differences in quality of life by sex according to the regions and age groups. In the crude model, only sex plus the participant’s identifier was introduced as an explanatory variable as a random intercept (p < 0.001); subsequently, an adjusted model was performed, with the variables of the crude model, plus the wave, the European region and the age groups (p < 0.001).
In the “all ages” model, as an adjusted model, eliminating the age groups and adding the sex-region interaction, modifying the reference category as appropriate, no significant differences were observed between men and women in the Northern region (p = 0.385), but significant differences were observed in the rest of the regions (p < 0.001).
The “age-specific” models were like the corresponding all-age models but adding the “age group” and modifying the reference category “age group as appropriate, and significant differences were found between men and women as age increased (p < 0.001).
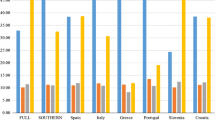
A statistically significant interaction was observed when adding in the fitted model the interaction “sex-European region” (p value = 0.0378), as well as the interaction “sex-age group” (p value < 0.001). For complete data, refer to Table 4 and Fig. 2.

Sex QoL differences with 95% confidence interval according to regions and age groups.
Discussion
SDHs have played a crucial role in understanding health disparities, and their origin goes beyond mere biological influences. This approach has proven to be highly valuable in formulating public health policies that address entrenched health inequities. To organize and comprehend the complexity of these determinants, various models have been proposed, such as that of Dahlgren and Whitehead, which categorizes SDHs into three fundamental levels: the micro level, encompassing individual characteristics; the meso level, focusing on the environment where diverse individuals interact; and the macro level, situated in a broader context, including public policies, sociocultural characteristics, and other general factors (Dahlgren, 1991). Also, the model of Social Determinants of Health proposed by the World Health Organization (WHO), which is the one we have used in our research. This model distinguishes three interrelated levels of functioning: the individual level, encompassing biological factors, individual behaviors, and access to health services; the meso or intermediate level, which includes social networks and support, the physical environment, as well as culture and values; and the macro level, incorporating socio-economic determinants, policies, and health systems, as well as social inequalities. This framework provides a robust foundation for analyzing the diverse factors that can impact health at both individual and community levels. (Hernández et al., 2017).
The relationship between these levels is complex and bidirectional, as macro-level factors can influence at the individual level, such as in access to healthcare, while individual behaviors can have cumulative effects on the health of an entire community. Therefore, understanding this interrelation and interconnectedness is essential for designing meaningful and effective interventions that address the SDHs in all their dimensions. (De La Guardia Gutiérrez et al., 2020).
This study investigated SDHs and QoL among people aged 50 years and older in 13 European countries, encompassed in four European regions, from a differentiated perspective between men and women in a longitudinal study and brings new comparative data to the existing literature to help understand and address health inequalities. The results revealed significant differences in the evolution of QoL between regions in Europe and between men and women during follow-up.
Consistent with the findings of previous research using the SHARE cohort (Cantarero-Prieto et al., 2018), our findings support evidence that women experienced a significant decline in their QoL compared to men over time, more significantly in the Southern European region.
Our findings suggest that not facing economic difficulties has a protective effect on the evolution of QoL. This statement is supported by a study by Niedzwiedz et al. in 2014 (Niedzwiedz et al., 2014), which demonstrated a significant association between lifelong socioeconomic position and life satisfaction in early old age and revealed differences in this association between countries with different welfare systems. In our study, economic hardships were also related to lower QoL scores, especially in Southern and Eastern European countries during the follow-up period, and this effect was more evident among women. This finding is consistent with that of previous research, such as that of Conde-Sala et al. in 2017 (Conde-Sala et al., 2017), suggesting that QoL is related to social welfare regimes. These regimes are more limited in Eastern and Southern European countries compared to Nordic and continental countries and have a protective effect on the evolution of QoL, especially among women (Ayala et al., 2021). We also found that being native to the country where the interview took place was a protective factor in the evolution of quality of life for women, in line with previous studies that found that migrant women experience triple discrimination based on ethnicity, sex, and class (Lirola, 2016) that have significant implications for their QoL (González-Castro & Ubillos, 2011), which is not the case for men.
In this study, we observed that lower levels of education were correlated with worse QoL, especially in Southern European countries and among women. These results are consistent with those of other studies, such as that by Rivas et al. (Rivas et al., 2011), which found an association between lower education levels and worse perceived QoL. The southern region had a higher prevalence of depression among the older people, which was directly related to lower QoL, in line with the findings of a meta-analysis conducted by Zhao et al. in 2012 (Zhao et al., 2012).
No significant differences were found regarding place of residence, except among women, for whom living in a rural area had a protective effect on the evolution of QoL compared to living in a large city. These results differ from those of previous research, such as that of Lenehan et al. (Lenehan et al., 2020) in 2020, in which their meta-analysis showed that older adults living in rural areas had significantly lower health related QoL than those living in urban areas.
Regarding lifestyle, differences were observed in tobacco consumption between men and women in all European regions and waves, with a higher prevalence among men. These findings have been shown in previous studies conducted with the SHARE cohort and data from the European Health Survey (Corominas Barnadas et al., 2017). In our study, we found that moderate alcohol consumption was associated with higher QoL scores, especially in the Southern and Eastern European regions. This could be explained by factors such as geographic location, alcohol availability, and social norms that normalize alcohol consumption, especially among men (Bosque-Prous et al., 2015). Physical activity was lower among women during the follow-up period and was directly related to a decrease in QoL scores, in line with a recent study that provided strong evidence that regular physical activity has a positive impact on the QoL of older adults (Marquez, 2020).
Among the strengths of this study, it is worth noting that a representative sample of 13 European countries was used, and the respondents participated in three consecutive waves, allowing for an understanding of their individual aging trajectories with a sex perspective. Additionally, the use of a multidisciplinary database provided a broad and cross-sectional view of the respondents. Finally, it is important to mention that grouping by European regions allowed for the identification of differences between them, as well as the association between SDHs and sex-based differences.
However, this study also has some limitations that should be considered when interpreting the results. Case loss between each wave and the selection of only those respondents who participated in all three consecutive waves may limit the external validity of this study. Random selection was made from the non-participants, matching for sex, age (±2 years), and European region. CASP values were then compared. Thus, among non-participants of the same age, sex, and European region, CASP-12 scores were very similar. Therefore, it could be assumed that participants in the three consecutive waves of the study are representative of a fraction of all European regions compared to those who participated in Wave 5.
Another limitation would be assessing alcohol consumption. The specific guidelines for moderate and excessive alcohol consumption can vary among European countries and local public health recommendations. Some European countries have adopted general guidelines recommended by the WHO.
The ethnicity or race of the respondent is not determined; only whether they are from the country of the interview is considered, it would be interesting to know their country of origin, as being an immigrant from a developed or underdeveloped country can make a difference.
Another limitation is that the SHARE study determines the economic level with the variable “making ends meet” and with the variable “received external financial aid” and this may generate a bias in the results since it is not quantifiable and may vary over time.
To improve this comparative and longitudinal study, many other variables related to the social determinants of health could have been added, such as: percentile of household income, economic benefits, family histories, childhood health, family support, participation in social activities, satisfaction, and access to services in the neighborhood where they live, computer literacy, among others. Further research is needed to identify and reduce health inequalities between regions in Europe. For example, countries in the Northern region show lower levels of inequality compared to countries in the Southern region (Jessoula, 2022).
To achieve this goal requires practical and specific measures to address existing disparities, such as the one proposed by Marmot in his report, with a focus on the social determinants of health, there is a proposal for the development and implementation of interventions that address these factors, such as affordable housing programs, education, and employment opportunities (Marmot, 2017).
Other proposals include improving the living conditions of the population, addressing the unequal distribution of power, money and resources, health education, intersectoral collaboration and promoting sex equity (Solar, Irwin 2010).
It is therefore crucial to implement social welfare policies that include greater investment in education, social benefits to reduce poverty and government support for older adults in general and women, especially in countries with less beneficial welfare systems. This financial investment in support would translate into lower future investment in the healthcare system and help to reduce the significant differences observed between countries and regions in Europe, as well as between the sexes.
Conclusions
This analysis allowed the identification of sex inequalities in the QoL of individuals over 50 years of age in Europe, as well as the determinants that influence them.
During the follow-up period, women had lower QoL scores than men. Irrespectively of the age, North region showed lower differences in QoL between male and female, while in the South region was the one with higher differences.
The main SDHs associated with lower quality of life scores, considering the sex perspective during the follow-up period, were older age, differences in quality of life between men and women increasing linearly with age in all regions, economic difficulties (more evident in the southern and eastern regions of Europe and among women), educational level, lower among women and in the southern region, and geographic location within Europe.
Furthermore, a higher prevalence of depression was found among women and men in the southern region of Europe, which was also associated with a decrease in QoL scores.
Physical activity in the female population was lower throughout the follow-up period, which was directly related to a decrease in QoL scores.
Data availability
This research utilizes data from waves SHARE 5, 6, and 7 (https://doi.org/10.6103/SHARE.w5.700, https://doi.org/10.6103/SHARE.w6.700, https://doi.org/10.6103/SHARE.w7.700). www.share-project.org. GitHub repository, https://github.com/JoanVilaDomenech/Matching/.
References
Abdallah, S, Stoll L, & FF Eiffe (2013) Third European Quality of Life Survey - Quality of Life in Europe: Subjective Well-being. Luxembourg: Publications Office of the European Union. In Publications Office of the European Union. https://www.eurofound.europa.eu/en/publications/2013/quality-life-europe-subjective-well-being
Ahrenfeldt LJ, Möller S (2021) The reciprocal relationship between socioeconomic status and health and the influence of sex: A European SHARE-analysis based on structural equation modeling. Int J Environ Res Public Health 18(9):5045. https://doi.org/10.3390/ijerph18095045
Arcaya MC, Arcaya AL, Subramanian SV (2015a) Inequalities in health: definitions, concepts, and theories. Glob Health Action 8(1):27106. https://doi.org/10.3402/gha.v8.27106
Arcaya MC, Arcaya AL, Subramanian SV (2015b) Inequalities in health: definitions, concepts, and theories. Glob Health Action 8(1):27106. https://doi.org/10.3402/gha.v8.27106
Ayala A, Rodríguez-Blázquez C, Calderón-Larrañaga A, Beridze G, Teixeira L, Araújo L, Rojo-Pérez F, Fernández-Mayoralas G, Rodríguez-Rodríguez V, Quirós-González V, Zorrilla-Muñoz V, Agulló-Tomás MS, Ribeiro O, Forjaz MJ (2021) Influence of active and healthy ageing on quality-of-life changes: insights from the comparison of three European Countries. Int J Environ Res Public Health 18(8):4152. https://doi.org/10.3390/ijerph18084152
Bates, D, Mächler, M, Bolker, B, & Walker, S (2015). Fitting linear mixed-effects models using lme4. J Stat Softw, 67(1). https://doi.org/10.18637/jss.v067.i01
Bergmann, M, K. T., de LG, & S. A. (2019). Survey Participation in the Survey of Health, Ageing and Retirement in Europe (SHARE), Wave 1–7. https://share-eric.eu/fileadmin/user_upload/SHARE_Working_Paper/WP_Series_41_2019_Bergmann_et_al.pdf
Börsch-Supan A, Brandt M, Hunkler C, Kneip T, Korbmacher J, Malter F, Schaan B, Stuck S, Zuber S (2013) Data resource profile: The Survey of Health, Ageing and Retirement in Europe (SHARE). Int J Epidemiol 42(4):992–1001. https://doi.org/10.1093/ije/dyt088
Börsch-Supan A, JH (2005). The Survey on Health, Ageing and Retirement in Europe – Methodology. In The Survey on Health, Ageing and Retirement in Europe – Methodology. Mannheim, Germany: Mannheim Research Institute for the Economics of Ageing (MEA). https://share-eric.eu/fileadmin/user_upload/Methodology_Volumes/Methodology_2005.pdf
Bosque-Prous M, Espelt A, Borrell C, Bartroli M, Guitart AM, Villalbí JR, Brugal MT (2015) Gender differences in hazardous drinking among middle-aged in Europe: the role of social context and women’s empowerment. Eur J Public Health 25(4):698–705. https://doi.org/10.1093/eurpub/cku234
Cantarero-Prieto D, Pascual-Sáez M, Blázquez-Fernández C (2018) What is happening with quality of life among the oldest people in Southern European countries? An Empirical approach based on the SHARE Data. Soc Indic Res 140(3):1195–1209. https://doi.org/10.1007/s11205-017-1828-5
Castro‐Costa E, Dewey M, Stewart R, Banerjee S, Huppert F, Mendonca‐Lima C, Bula C, Reisches F, Wancata J, Ritchie K, Tsolaki M, Mateos R, Prince M (2008) Ascertaining late‐life depressive symptoms in Europe: an evaluation of the survey version of the EURO‐D scale in 10 nations. The SHARE project. Int J Methods Psychiatr Res 17(1):12–29. https://doi.org/10.1002/mpr.236
Collins KH, Sharif B, Sanmartin C, Reimer RA, Herzog W, Chin R, Marshall DA (2016) Association of body mass index (BMI) and percent body fat among BMI-defined non-obese middle-aged individuals: Insights from a population-based Canadian sample. Can J Public Health 107(6):520–525. https://www.jstor.org/stable/90006523
Conde-Sala JL, Portellano-Ortiz C, Calvó-Perxas L, Garre-Olmo J (2017) Quality of life in people aged 65+ in Europe: associated factors and models of social welfare—analysis of data from the SHARE project (Wave 5). Qual Life Res 26(4):1059–1070. https://doi.org/10.1007/s11136-016-1436-x
Corominas Barnadas JM, López-Pousa S, Vilalta-Franch J, Calvó-Perxas L, Juvinyà Canal D, Garre-Olmo J (2017) Estudio MESGI50: descripción de una cohorte sobre la madurez y el envejecimiento satisfactorio. Gac Sanit 31(6):511–517. https://doi.org/10.1016/j.gaceta.2016.07.017
De La Guardia Gutiérrez, Alberto Mario, Ledezma Ruvalcaba (2020) Health and its determinants, health promotion, and health education. J Negat No Posit Results 5(1):81–90. https://scielo.isciii.es/scielo.php?script=sci_abstract&pid=S2529-850X2020000100081
European Commission. (2010). Eurostat Regional Yearbook 2010. Eurostat Statistical Books No. KS-HA-10-001-EN. Luxembourg: European Commission. (KS-HA-10-001-15). https://ec.europa.eu/eurostat/web/products-statistical-books/-/ks-ha-10-001-15
Fernández I, Sentandreu-Mañó T, Tomas JM (2020) Impacto del estatus de fragilidad sobre la salud y calidad de vida en personas mayores españolas. Atención Primaria 52(10):731–737. https://doi.org/10.1016/j.aprim.2019.11.006
Fernández-Carro C, Gumà J (2022) Influyen las trayectorias familiares en la calidad de vida percibida en la vejez? Rev Española de Sociolía 31(2):a109. https://doi.org/10.22325/fes/res.2022.109
García Ramírez JA, Consuelo Vélez Álvarez(2017) Social determinants of health and quality of life in the adult population of Manizales, ColombiaRev Cubana Salud Publica43(2):191–203 http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S0864-34662017000200006&lng=es&tlng=es
González-Castro JL, Ubillos S (2011) Determinants of psychological distress among migrants from Ecuador and Romania in a Spanish City. Int J Soc Psychiatry 57(1):30–44. https://doi.org/10.1177/0020764009347336
Hernández LJ, Ocampo J, Ríos D, Calderón C (2017) El modelo de la OMS como orientador en la salud pública a partir de los determinantes sociales. Rev de Salud Pública 19(3):393–395. https://doi.org/10.15446/rsap.v19n3.68470
Hyde M, Wiggins RD, Higgs P, Blane DB (2003) A measure of quality of life in early old age: The theory, development, and properties of a need’s satisfaction model (CASP-19). Aging Ment Health 7(3):186–194. https://doi.org/10.1080/1360786031000101157
Lenehan, ME, OM, & L-WP. (2020). Health-related quality of life among older adults in rural compared to urban areas: a systematic review and meta-analysis of comparative studies. Int J Environ Res Public Health, 17(9)
Lirola MM (2016) An exploration of the representation of immigrant women in a sample from the Spanish press. Gend Quest 2(1):84–97. https://doi.org/10.25159/2412-8457/1566
Malter, F and Börsch-Supan, A (2015). SHARE Wave 5: Innovations & Methodology. https://share-eric.eu/fileadmin/user_upload/Methodology_Volumes/Method_vol5_31March2015.pdf
Marmot M (2007) Achieving health equity: from root causes to fair outcomes. Lancet 370(9593):1153–1163. https://doi.org/10.1016/S0140-6736(07)61385-3
Marmot M (2017) The Health Gap: The Challenge of an Unequal World: the argument. Int J Epidemiol 46(4):1312–1318. https://doi.org/10.1093/ije/dyx163
Mejía Reyes ÁF (2021) Determinantes sociales y su impacto sobre la salud de los trabajadores centroamericanos durante la última década. Población y Desarro - Argonautas y Caminantes 17:81–90. https://doi.org/10.5377/pdac.v17i2.12745
National Institute of Statistics. (2020). National Institute of Statistics. (2020). Life Expectancy. In: Men and Women in Spain. https://www.ine.es/ss/Satellite?L=0&c=INEPublicacion_C&cid=1259924822888&p=1254735110672&pagename=ProductosYServicios%2FPYSLayout¶m1=PYSDetalleGratuitas
Niedzwiedz CL, Katikireddi SV, Pell JP, Mitchell R (2014) The association between life course socioeconomic position and life satisfaction in different welfare states: European comparative study of individuals in early old age. Age Ageing 43(3):431–436. https://doi.org/10.1093/ageing/afu004
Palomino Moral PA, Grande Gascón ML, Linares Abad M (2014) La salud y sus determinantes sociales. Desigualdades y exclusión en la sociedad del siglo XXI. Rev Int Soc 72(Extra_1):45–70. https://doi.org/10.3989/ris.2013.02.16
Paxton RJ, Motl RW, Aylward A, Nigg CR (2010) Physical activity and quality of life—the complementary influence of self-efficacy for physical activity and mental health difficulties. Int J Behav Med 17(4):255–263. https://doi.org/10.1007/s12529-010-9086-9
Pérez-Rojo G, Martín N, Noriega C, López J (2018) Psychometric properties of the CASP-12 in a Spanish older community dwelling sample. Aging Ment Health 22(5):700–708. https://doi.org/10.1080/13607863.2017.1292208
Phelan JC, Link BG, Tehranifar P (2010) Social conditions as fundamental causes of health inequalities: theory, evidence, and policy implications. J Health Soc Behav 51(1_suppl):S28–S40. https://doi.org/10.1177/0022146510383498
Prince MJ, Reischies F, Beekman ATF, Fuhrer R, Jonker C, Kivela S-L, Lawlor BA, Lobo A, Magnusson H, Fichter M, Van Oyen H, Roelands M, Skoog I, Turrina C, Copeland JRM (1999) Development of the EURO–D scale – a European Union initiative to compare symptoms of depression in 14 European centers. Br J Psychiatry 174(4):330–338. https://doi.org/10.1192/bjp.174.4.330
Reitlo LS, Sandbakk SB, Viken H, Aspvik NP, Ingebrigtsen JE, Tan X, Wisløff U, Stensvold D (2018) Exercise patterns in older adults instructed to follow moderate- or high-intensity exercise protocol – the generation 100 study. BMC Geriatr 18(1):208. https://doi.org/10.1186/s12877-018-0900-6
Rivas M, Nuevo R, Ayuso-Mateos JL (2011) Depresión subclínica en España: prevalencia e impacto sobre la salud. Rev de Psiquiatría y Salud Ment 4(3):144–149. https://doi.org/10.1016/j.rpsm.2011.05.005
Salgado-de Snyder V, Wong R (2007) Gender and poverty: determinants of health in old age. Salud Pública de México 49(4):515–521. https://www.researchgate.net/publication/6114839_Gender_and_poverty_health_determinants_in_old_age
Serdà Ferrer B-C (2014) Quality of life and gerontology: description of a research line. Eur J Investig Health, Psychol Educ 4(3):301–308. https://doi.org/10.3390/ejihpe4030028
Sexton E, King-Kallimanis BL, Layte R, Hickey A (2015) CASP-19 special section: how does chronic disease status affect CASP quality of life at older ages? Examining the WHO ICF disability domains as mediators of this relationship. Aging Ment Health 19(7):622–633. https://doi.org/10.1080/13607863.2014.955457
Solar, O, & Irwin A (2010). A conceptual framework for action on the social determinants of health. Social determinants of health discussion paper 2. https://www.who.int/publications/i/item/9789241500852
United Nations. (2019). United Nations. Departament of Economic and Social Affairs. Popiulation division. World Population Prospect: Highlights. https://population.un.org/wpp/Publications/Files/WPP2019Highlights.pdf
United Nations. (2021). United Nations. Population Fund. (2021). Aging in the 21st Century: A Celebration and a Challenge. https://www.unfpa.org/sites/default/files/pub-pdf/Ageing%20Report%20Executive%20Summary%20SPANISH%20Final_0.pdf
United Nations Educational Scientific and Cultural Organization. (1997). International Standard Classification of Education: ISCED 1997. http://uis.unesco.org/sites/default/files/documents/international-standard-classification-of-education-1997-en_0.pdf
United Nations Educational Scientific and Cultural Organization. (2011). International Standard Classification of Education: ISCED 2011. http://uis.unesco.org/sites/default/files/documents/international-standard-classification-of-education-isced-2011-en.pdf
Vila. J (2024). Matching function, GitHub repository. https://github.com/JoanVilaDomenech/Matching/
Wiggins RD, Netuveli G, Hyde M, Higgs P, Blane D (2008) The evaluation of a self-enumerated scale of Quality of Life (CASP-19) in the context of research on ageing: a combination of exploratory and confirmatory approaches. Soc Indic Res 89(1):61–77. https://doi.org/10.1007/s11205-007-9220-5
World Health Organization (1995) Physical status: The use and interpretation of anthropometry. World Health Organ Tech Rep Ser 854:1–452. https://europepmc.org/article/MED/8594834
World Health Organization. (1996). World Health Organization. (1996). Quality of Life Group. What Quality of Life? Foro Mund Salud. https://iris.who.int/handle/10665/55264
World Health Organization. (1998). World Health Organization. (1998). Health Promotion: Glossary. https://apps.who.int/iris/handle/10665/67246
World Health Organization. (2008). Commission on Social Determinants of Health. (2008). Closing the Gap in a Generation: Health Equity Through Action on the Social Determinants of Health: Executive Summary of the Final Report. https://apps.who.int/iris/handle/10665/69830
World Health Organization. (2011). World Health Organization. (2021). Aging and Health. https://www.who.int/es/news-room/fact-sheets/detail/ageing-and-health
Zaninotto P, Falaschetti E, Sacker A (2009) Age trajectories of quality of life among older adults: results from the English Longitudinal Study of Ageing. Qual Life Res 18(10):1301–1309. https://doi.org/10.1007/s11136-009-9543-6
Zhao K-X, Huang C-Q, Xiao Q, Gao Y, Liu Q-X, Wang Z-R, Li Y-H, Xie Y-Z (2012) Age and risk for depression among the elderly: a meta-analysis of the published literature. CNS Spectr 17(3):142–154. https://doi.org/10.1017/S1092852912000533
Acknowledgements
This research utilizes data from waves SHARE 5, 6, and 7 (https://doi.org/10.6103/SHARE.w5.700, https://doi.org/10.6103/SHARE.w6.700, https://doi.org/10.6103/SHARE.w7.700). For methodological details, please refer to Börsch-Supan et al. (2013). https://doi.org/10.1093/ije/dyt088.
Funding
The data collection of SHARE has been primarily funded by the European Commission through the 5th Framework Programme (QLK6-CT-2001-00360), 6th Framework Programme (SHARE-I3: RII-CT-2006-062193, COMPARE: CIT5-CT-2005-028857, SHARELIFE: CIT4-CT-2006-028812), and 7th Framework Programme (SHARE-PREP: N°211909, SHARE-LEAP: N°227822, SHARE M4: N°261982). Additional funding is acknowledged from the German Ministry of Education and Research, the Max Planck Society for the Advancement of Science, the U.S. National Institute on Aging (U01_AG09740-13S2, P01_AG005842, P01_AG08291, P30_AG12815, R21_AG025169, Y1-AG-4553-01, IAG_BSR06-11, OGHA_04-064, HHSN271201300071C), and various national funding sources (see www.share-project.org).
Author information
Authors and Affiliations
Contributions
All authors contributed to the conception and design of the study. Material preparation, data collection, and data analysis were performed by [R L-O], [C B-F], and [J G-O]. The first draft of the manuscript was written by [R L-O] and all authors commented on earlier versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The author declares no competing interests.
Consent to publish
This study does not contain individual participant data.
Ethics approval
The Ethics Committee of the Max Planck Society for the Advancement of Science has thoroughly reviewed the materials of the SHARE project, including wave 5 and its follow-up waves (waves 6 and 7). The committee certifies that the research project, its procedures, and the measures to ensure the confidentiality and privacy of data and information provided to participants comply with international ethical standards in accordance with the Declaration of Helsinki and the International Ethical Guidelines for Biomedical Research Involving Human Subjects.
Informed consent
Informed consent was obtained from all individual participants included in the study during the interview.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Llorens-Ortega, R., Bertran-Noguer, C., Juvinyà-Canals, D. et al. Influence of social determinants of health in the evolution of the quality of life of older adults in Europe: A comparative analysis between men and women. Humanit Soc Sci Commun 11, 401 (2024). https://doi.org/10.1057/s41599-024-02899-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1057/s41599-024-02899-5
- Springer Nature Limited
This article is cited by
-
Pharmacotherapy for Coronary Artery Disease and Acute Coronary Syndrome in the Aging Population
Current Atherosclerosis Reports (2024)