
Abstract
Insomnia and the inability to sleep affect people’s health and well-being. However, its systematic estimates of prevalence and distribution in the general population in China are still lacking. A population-based cluster sampling survey was conducted in the rural and urban areas of Hunan, China. Subjects (n = 26,851) were sampled from the general population, with a follow-up using the Pittsburgh Sleep Quality Index (PSQI) for interview to assess quality of sleep and Insomnia (PSQI score >5). While the overall prevalence of insomnia was 26.6%, and little difference was found between males (26.3%) and females (27.0%); the mean PSQI score was 4.26 (±2.67), and significant higher in females (4.32 ± 2.70) than males (4.21 ± 2.64, p = 0.003). Individuals in the rural areas tended to report a higher PSQI score (4.45 ± 2.81) than urban residents did (4.18 ± 2.60) (p < 0.001) and the estimates of prevalence of insomnia was 29.4% in the rural areas, significant higher than 25.5% in the urban areas (p < 0.001). Multiple logistic regression analysis showed that female gender, older age, higher level of education, being unmarried, living in the rural area, cigarette smoking and alcohol drinking were associated with insomnia. Our study may provide important information for general and mental health research.
Similar content being viewed by others


Introduction
Sleep is an important physiological process that affects health and well-being and the experience of proper sleep varies across individuals. Sleep quality is a measure of the feeling that a person would have of being energetic, active, and ready for a new day. It includes quantitative aspects such as sleep duration, sleep latency, and number of arousals, as well as qualitative aspects such as the depth and feeling of restfulness upon awakening1. While the direct benefits of high-quality sleep are not well quantified across populations, it is understood that sleep loss or insomnia is a serious public concern that may affect quality of life and well-being2. Epidemiological surveys indicate that about 15% to 35% of adult individuals have frequent sleep disturbances, including difficulty falling asleep or maintaining sleep1.
Poor sleep quality may have serious health and personal consequences. It can lead to impairment or poor performance during daytime school or work, increase risk for motor vehicle or occupational accidents, exacerbate medical and psychiatric conditions, and result in diminished quality of life3. Frequent difficulties initiating sleep have been associated with higher mortality among men but not women4. Thus, sleep disturbances affect a wide range of aspects of health and well-being.
The measurement and assessment of sleep disturbances is particularly important with respect to study of sleep and its related effects. Proper sleep may not be completely assessed by a single dimension such as duration, but have to be considered as a multi-dimensional construct. Such measurement considerations can influence both prevalence estimates and examining the association of sleep disturbances with health outcomes. The most widely used standardized measure is the Pittsburgh Sleep Quality Index (PSQI), which is designed to differentiate between “good” sleepers and “poor” sleepers and to identify subgroups of poor sleepers1. As such, it permits a comprehensive assessment of sleep.
There has been lack of consistency in the studies of gender differences in sleep quality. Buysse et al. found an association of female gender with high PSQI scores in a community-dwelling adults sample5. A recent school-based study with 7,507 children and adolescents showed higher prevalence of insomnia symptoms in girls than boys6, indicating that a gender difference may extend across the life course. However, Buysse and colleagues previously found no significant gender differences in PSQI among healthy young and elderly subjects7. When it comes to clinical patients, there was a significant difference in mean PSQI scores between male and female patients in the last week of study and in the pre-illness period8. However, men may consider their quality of sleep better than women9. Nevertheless, considering a line of evidence on morphologic differences between males and females in circadian clock genes, respiratory control, the action of sex hormones, stress responses on sleep mechanisms, and social patterning of behaviors that affect sleep, the difference in sleep quality between genders is likely real3,10.
Quality of sleep may vary substantially by gender and residential location. A great attention has been paid to social, demographic, and societal influences on sleep11,12,13. Previous research identified that neighborhood environments may influence sleep-related outcomes14. An examination of residential status is particularly important in China as the residential registration system (hukou) has restricted the mobility of residents over the past decades. Residential location was indicated as an important factor associated with sleep quality in the rural and urban areas near Beijing and Shanghai15 and in the United States16. However, a robust population-based estimates of sleep disturbances and insomnia are scarce in the general populations of mainland China; and little had been known about the differences in sleep quality by gender and residential location.
The main purpose of this study is to evaluate differences in sleep quality and insomnia by gender and residential location. We also tried to assess association of factors such as age, marital status, educational level, cigarette smoking and alcohol drinking with rate of insomnia (with PSQI > 5) in the general population sample. Our primary hypotheses were: (1) the mean PSQI scores and the prevalence of insomnia will be higher for women, and (2) poor sleep quality and prevalence of insomnia will be higher in urban areas given the increased exposure to noise and light pollution as well as the more intense pace of life in such locales.
Results
Participant demographic characteristics
Among the total 26,851 participants, 26,766 participants (14,215 men and 12,551 women) were included in demographic analysis. The mean age was 38.1 (±16.05) years old, with 42.8 (±17.53) in the rural residents, which was significantly older than 36.0 (±14.85) in the urban residents (p < 0.001). Compared with female participants, males tended to have a higher level of education, Body Mass Index (BMI), personal income, as well as were more likely to be employed, married, urban residents, and overwhelmingly more likely to smoke cigarettes and drink alcohol (Table 1).
Sleep quality and poor sleeping
After the exclusion of individuals with missing information on demographics and PSQI, 25,827 participants were included in the final analysis of sleep quality and poor sleeping. Analysis of the PSQI score estimated that the mean sleep latency (defined as the amount of time it takes to fall asleep after lights off) was 21.05 (±19.33) minutes (20.48 ± 19.99 in males and 21.05.8 ± 18.57 in females); the mean of total sleep time was 454.75 (±77.30) minutes (451.61 ± 78.38 in males and 458.39 ± 75.94 in females). Detailed statistics of PSQI components and total score in the overall sample and by gender are presented in Table 2.
Female participants tended to have higher scores than males in multiple PSQI component scores. We observed significant difference in PSQI components of subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, and sleep disturbance between men and women (p < 0.0001). However, there were no significant gender differences in other two PSQI components - need for sleep medications (p = 0.437) and daytime dysfunction (p = 0.220). While females had a higher PSQI total score than males (p = 0.003), there was no significant difference (p = 0.232) when it came to the rate of poor sleepers between males (26.3%) and females (27.0%). It is noteworthy that the lowest PSQI component score was found with “a need for sleep medications” in overall participants (0.11 ± 0.38), with less than 10% of participants reporting a need for sleep medications during the past month before the time of survey (6.9% reported less than once a week, 1.4% reported once or twice a week and 0.4% reported ≥3 times a week (Table 2).
PSQI total score and prevalence of insomnia by gender and region
Considering that there was a significant difference in PSQI total score between males and females, we performed a stratification analysis by region, as urban residence is highly heterogeneous in the size of city, which may have different implications for the sleep quality (Table 3). Overall, there was a significant difference in PSQI total score between the rural and urban areas (4.45 ± 2.81 vs 4.18 ± 2.60, p < 0.01). However, when examining the urban sample alone, we found that the difference in PSQI total score between men and women were less or not significant in individuals who lived in small town (p = 0.059), county city (p = 0.048), prefecture city (p = 0.0894), all of which were small to medium size city; but we still observed a significant gender difference in people who lived in Changsha, the largest metropolitan and the capital city of Hunan (p = 0.02).
Similar stratification analysis of prevalence of insomnia was performed and showed no significant differences in insomania by gender and by region (p > 0.11). However, we found a significant difference (p < 0.001) in prevalence of insomnia between urban (25.5%) and rural areas (29.4%). Individuals who lived in the rural areas had a high likelihood of poor sleeping (Table 4).
Factors associated with increased likelihood of sleep problems or insomnia
Based on descriptive analysis and previous literature, we examined the association of factors such as age, gender, marital status, level of education, rural and urban residence, cigarette smoking and alcohol drinking, with poor sleeping. Based on simple linear regression analysis, we found that all seven factors were associated with PSQI total score (sleep quality) (see Table 5). Further with multiple logistic regression analysis, we confirmed that more likelihood of insomnia was associated with female gender (OR = 1.367, P < 0.001), rural residence (OR = 1.115, p = 0.002), older age (OR = 1.026, p < 0.001), higher level of education (OR = 1.02, p < 0.001), unmarried status such as divorced, separated or widowed status (OR = 1.587, p < 0.001), cigarette smoking (OR = 1.468, P < 0.001) and alcohol drinking (OR = 1.265, p < 0.001) (Table 6). The effect size for some of these factors were not trival.
Discussion
In this study, we provide the first estimates of sleep quality and insomnia by gender and residence and examination of associated factors in a large sample of the general population in mainland China. While reporting a similar rate of insomnia, women tended to have a poorer sleep as measured by PSQI total score; We also found a significant difference in poorer sleep quality and higher prevalence of insomnia in rural than urban residents, but inconsistent with other studies; and multiple regression analysis also showed a number of demographic variables are also associated with sleep quality.
Overall, insomnia is a common health problem in the general population of central China. According to our estimates, more than one fourth of individuals had insomnia during the past month at the time of survey. These findings are similar, with some variation due to study populations, to the prevalence of sleep problems found in epidemiological studies conducted in other parts of China. Previous studies showed that an overall point estimate of the prevalence of insomnia (PSQI score > 5) was 39.4% in the general population of Hong Kong17,18, and reported a 32.9% of insomnia among the elderly Chinese in Shandong19; Community- or population-based cross-sectional surveys also reported that the prevalence of poor sleep (PSQI score > 5) in older adults was 20.67% in Guangdong20, and 26.36% in adults aged 20 and above in the rural areas of Liaoning21. A Japanese nationwide survey in general population reported the overall prevalence of insomnia was 32.7%22; and A German study of community sample (aged 18–80 years) estimated that 36% of the general population had bad sleep quality (PSQI > 5)23. Our estimate of prevalence appears lower than those previous studies. While population structure may contribute to this difference, ethnicity13, socioeconomic status, and even geographic locations11 may affect sleep quality and insomnia. These are all warranted to have a further investigation of the determinants of sleep quality and insomnia.
There was a significant difference in sleep quality but not prevalence of insomnia between men and women. Consistently with previous studies3, our study indicates that women had poorer sleep quality than men. However, we found no significant difference in the overall prevalence of insomnia between men and women; this appears contradictory to other previous reports22,24. For example, the prevalence of having sleep problems were 26.4% in men and 31.1% in women in the general Japanese adult population25, and 9.5% in men and 14.3% in women in another sample from northern Japan26. Defined by PSQI > 5, another urban population-based sample in Iran showed 27% in men versus 35% in women27. The absence of a gender difference in the prevalence of insomnia in the central China merits a further investigation.
It was a little surprise to see a significant difference in poorer sleep quality and higher prevalence of insomnia in rural than urban residents. We had anticipated that the greater noise and light pollution as well as more fast-paced urban life may have diminished the likelihood of quality sleep. This finding is also contradictory to other studies. A cross-sectional survey conducted in older adults in the urban and rural areas of Beijing and Shanghai reported that, despite lower socio-economic status and poor medical insurance coverage, rural residents were more likely to report better sleep quality than urban residents15. Yet, a study of middle age people in Beijing found that while overall there was no significant difference between rural and urban residents in any type of insomnia, more rural (21.1%) than urban(14.9%) residents reported the highest rate of at least one type of insomnia (overall 17.1%)28.
There may be multiple explanations to the higher prevalence of insomnia in the rural areas that may deserve some attentions. In the rural areas of China, high demands for physical work often leads to musculoskeletal pain or illness that may affect sleep quality among rural workers29. We may also consider that the higher level of insomnia in the rural areas may be influenced by the massive rural-to-urban migration occurring in China. Rural migrants may suffer more from stressful events that may result from finding a job and decent place to live or more commutes between home and work place. The current study showed that rural participants was older than the urban participants, which may be due to the rural to urban migration of younger people30, leaving relatively older adults who may suffer from stress from separation with their migrant daughters and sons and in general may have more sleep problems as brain aging. Besides older age, limited access to quality health services may result in a higher prevalence of insomnia in rural areas31; and availability and quality of health services were different between urban and rural areas of China32,33. Future investigations should consider which social and institutional factors related to migration may cause the difference in insomnia in the general population between rural and urban locations.
Our multiple logistic regression model also showed that female gender, older age, high level of education, unmarried status, living in the rural areas, and cigarette smoking and alcohol drinking were associated with higher odds of insomnia. Those demographic variables have been established elsewhere in the literature. A telephone survey among the Hong Kong Chinese population also showed a higher prevalence of insomnia in females34. The gender differences in insomnia were confirmed by a meta-analysis35. Clinical and pre-clinical studies suggest that biological sex and sex steroids influence sleep behavior and sleep disorders10,36. A line of research has shown that insomnia was significantly associated with older age22,24,37,38; and marital status and level of education were associated with insomnia28. However, Xiang et al showed that low level of education (illiteracy and primary school) was significantly associated with insomnia28. One of the possible reasons we found different results may be due to the ever-increasing occupational stress among well-educated people in China.
Cigarette smoking and alcohol use were associated with sleep problems. Our previous studies showed frequently sleep problems among drug users39,40. The current study did find that cigarette smokers and alcohol drinkers had higher odds for poor quality of sleep, which also was consistent with other previous studies41,42,43. As use of substance in China is highly gendered, more so than in other regions of the world, it remains important to further examine the role of such substance use behaviors in the gender and regional differences described above. It remains interesting that men use substances much more so than women use, yet do not seem proportionally affected in their overall prevalence of insomnia. Further explication of the complex underlying mechanisms between insomnia and age, levels of education, marital status, and residential regions is needed.
This study has a number of strengths, including the large sample size, the high rate of participation, the use of well-established instruments to examine sleep problems, and the questionnaire-based door-to-door interview. However, there were some limitations. First, although this is a randomly selected sample of community-dwelling participants, we did not use a multistage, stratified sampling method to select a provincially representative sample of the general population. That may limit the generalizability of this study. Second, in the present study, sleep quality and insomnia were assessed using a retrospective, self-reported approach using PSQI, which may be subject to some reporting errors; participants with insomnia may be more likely to overestimate their sleep latency and underestimate their sleep duration. Although objective measures (i.e., physiologic measurements such as electroencephalography) are desirable, they have, however, not been regularly incorporated into such a large epidemiologic study of the general population. Thus, self-reports and interview-based measures remain the most widely used measures in community surveys44. Third, we were not able to distinguish between primary and secondary insomnia and to classify insomnia into DSM-5 subtypes, such as primary insomnia, insomnia related to a mental disorder, for example, substance-induced insomnia are very common39,40. In addition, because the analysis is cross-sectional, we are unable to make inferences of causal relationships for the factors identified, such as that between substance use and sleep quality. For example, insomnia is an important indicator of perceived physical and mental health status22. However, the focal point of gender within our study permits some assurance with respect to the directionality of such a causal pathway.
In conclusion, the present study, based on the PSQI, showed a high prevalence of insomnia in the general population of central China. Females reported poorer sleep quality than males, and rural participants reported poorer sleep quality and higher prevalence of insomnia than urban participants did. Older age, high levels of education, unmarried status, cigarette smoking and alcohol drinking were also associated with insomnia. Further studies using longitudinal designs are warranted to examine the community-level, psychosocial, and biologic factors of insomnia. Within the public health system, further attention has to be given to sleep quality and insomnia.
Methods
Design
A cross-sectional survey design was used to explore sleep quality. We used a community-based method to select a sample of persons 12 years of age or older in the general population from Hunan Province, a province located in the south-central region of China, with a population of 65.68 million (according to The Sixth National Population Census of the People’s Republic of China in 2010). Hunan has 14 prefecture-level regions, which are subdivided into 122 county-level administration divisions (including 34 districts, 16 county-level cities, 65 counties, and 7 autonomous counties).
Study Participants
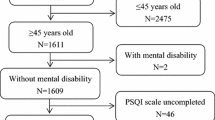
In this population-based cross-sectional survey, participants were recruited from September 2012 to October 2012 in Hunan province. We used a community-based method to select participants from all divisions (13 prefecture level cities and 1 autonomous prefecture) of Hunan province, including 93 urban street districts (31 capital cities, 23 prefecture level cities, 23 county level cities, 16 small towns) and 42 rural villages were randomly selected, which yielded 135 sites in total. In each prefecture level city or autonomous prefecture, at least 1 prefecture level city, 1 county level city, 1 small town and 1 rural village has been randomly selected. Only a person aged 12 years or older and living in their current residence for 5 years or longer were selected from each household without replacement. 27,300 people were randomly selected from the selected sites and invited to participate in the study; 26,851 persons completed the study (details showed in Fig. 1). The overall response rate was 98.4% (449 participants refused to respond, including 228 men and 221 women; 243 lived in urban areas and 206 lived in rural areas). After the exclusion of missing demographic and PSIQ information, 25,827 participants were included in the final analysis. The ages of the participants ranged from 12 to 99 years, with an average age of 38.1 ± 16.05 years.

Flowchart of the sampling procedure in the Hunan province, China for sleeping quality study.
The protocol was approved by the university ethics committee (The Second Xiangya Hospital of Central South University Review Board, No. S101, 2011) and the studies were carried out in accordance with the Declaration of Helsinki. Subjects were fully informed about the survey. All study participants gave verbal informed consent. Eligible subjects were 12 years of age or older who could fully understand the survey.
Procedure
At each selected site, participants from door to door were invited to fill out the survey if they consented to participate. Every household member aged 12 or more years was encouraged to participate by a face-to-face interview. As part of the consent process, participants were provided with a detailed explanation of the objectives of the study and study expectations. Participants were advised of their ability to withdraw from the study at any point. Issues of confidentiality and anonymity were discussed. Verbal informed consent was obtained. Participants were encouraged to answer the questionnaire independently and as soon as possible. Those who were unable to recognize 1,500–2,000 Chinese characters were defined as illiterate. In such cases, the staff would read and explain each question, and helped illiterate participants to write down the answer if necessary.
Assessment measures
In this face-to-face survey, each participant was asked to answer a self-reported battery of questionnaires that consisted of socio-demographic and sleep-related information. The demographic section gathered information on age, gender, marital status, employment status, and years of education, height, weight, personal income, cigarette smoking, and alcohol drinking. The Pittsburgh Sleep Quality Index (PSQI)1 was used to assess sleep. The PSQI is a validated, self-administered questionnaire used that measures sleep quality and disturbances over a one-month time interval. It is a seven-item questionnaire with each item rated from 0 to 3 (sleep duration, sleep efficiency, sleep latency, sleep disturbance, daytime dysfunction, frequency of sleep medications, and subjective sleep quality) with scores ranging between 0 and 21 points; higher scores indicates a lower quality of sleep. A PSQI global score greater than 5 indicates ‘poor sleep’ with a sensitivity of 89.6–98.7% and specificity of 84.4–86.5% and was used to define symptoms of insomnia in this study1,45. The questionnaire is easy to handle and can be completed within 5 minutes. The Chinese version of PSQI has been extensively used in patients and general populations with good reliability and validity39,46.
Statistical analysis
Statistical analysis was performed using SPSS (Version 16, SPSS Inc., Chicago, IL, USA). To address missing data, incomplete questionnaires missing the variables of interest were excluded. Descriptive statistics were examined on demographic characteristics and pooled responses, including the mean, standard deviation for continuous variables, and percentage for categorical variables. Between-group comparisons were performed using χ2 (Chi-square) for categorical variables and the Wilcoxon rank sum test (Mann-Whitney U-test) (as the data are not perfect normal distributions) for continuous measures. The subjects were classified into two groups by sleep quality: good if PSQI score ≤ 5; poor sleepers or insomnia if PSQI score > 5. Simple linear regression analysis was used to examine the association between continuous variables (PSQI total score) and each of the associated factors (age, gender, marital status, levels of education, rural or urban residence, with or without cigarette smoking, and with or without alcohol drinking). Then, multiple logistic regression analysis was performed to obtain the odds ratios between the associated factors and poor sleep. A power analysis was also performed, and the odds ratios (OR) and 95% confidence intervals (CI) of the predictors were derived. A p-value threshold of 0.05 was set to determine statistical significance.
Additional Information
How to cite this article: Tang, J. et al. Gender and Regional Differences in Sleep Quality and Insomnia: A General Population-based Study in Hunan Province of China. Sci. Rep. 7, 43690; doi: 10.1038/srep43690 (2017).
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
Buysse, D. J., Reynolds, C. F., Monk, T. H., Berman, S. R. & Kupfer, D. J. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry research 28, 193–213 (1989).
Hayashino, Y. et al. Association between number of comorbid conditions, depression, and sleep quality using the Pittsburgh Sleep Quality Index: results from a population-based survey. Sleep medicine 11, 366–371 (2010).
Mollayeva, T. et al. The Pittsburgh sleep quality index as a screening tool for sleep dysfunction in clinical and non-clinical samples: A systematic review and meta-analysis. Sleep medicine reviews 25, 52–73 (2016).
Lallukka, T. et al. Insomnia symptoms and mortality: a register‐linked study among women and men from Finland, Norway and Lithuania. Journal of sleep research 25, 96–103 (2016).
Buysse, D. J. et al. Relationships between the Pittsburgh Sleep Quality Index (PSQI), Epworth Sleepiness Scale (ESS), and clinical/polysomnographic measures in a community sample. J Clin Sleep Med 4, 563–571 (2008).
Zhang, J. et al. Emergence of Sex Differences in Insomnia Symptoms in Adolescents: A Large-Scale School-Based Study. Sleep 39 1563–1570 (2016).
Buysse, D. J. et al. Quantification of subjective sleep quality in healthy elderly men and women using the Pittsburgh Sleep Quality Index (PSQI). Sleep 14, 331–8 (1991).
Doğan, O., Ertekin, Ş. & Doğan, S. Sleep quality in hospitalized patients. Journal of clinical nursing 14, 107–113 (2005).
Tribl, G. et al. Sleeping habits in the Austrian population. Sleep medicine 3, 21–28 (2002).
Mong, J. A. & Cusmano, D. M. Sex differences in sleep: impact of biological sex and sex steroids. Phil. Trans. R. Soc. B 371, 20150110 (2016).
Grandner, M. A. et al. Geographic distribution of insufficient sleep across the United States: a county-level hotspot analysis. Sleep health 1, 158–165 (2015).
Grandner, M. A., Patel, N. P., Gehrman, P. R., Perlis, M. L. & Pack, A. I. Problems associated with short sleep: bridging the gap between laboratory and epidemiological studies. Sleep medicine reviews 14, 239–247 (2010).
Grandner, M. A. et al. Who gets the best sleep? Ethnic and socioeconomic factors related to sleep complaints. Sleep medicine 11, 470–478 (2010).
Hale, L. & Do, D. P. Racial differences in self-reports of sleep duration in a population-based study. Sleep 30, 1096–103 (2007).
Haseli-Mashhadi, N. et al. Sleep quality in middle-aged and elderly Chinese: distribution, associated factors and associations with cardio-metabolic risk factors. BMC Public Health 9, 130 (2009).
Grandner, M. A., Jackson, N. J., Pigeon, W. R., Gooneratne, N. S. & Patel, N. P. State and regional prevalence of sleep disturbance and daytime fatigue. Journal of clinical sleep medicine 8, 77 (2012).
Wong, W. S. & Fielding, R. Prevalence of insomnia among Chinese adults in Hong Kong: a population‐based study. Journal of Sleep Research 20, 117–126 (2011).
Abdullah, A. S., Qiming, F., Pun, V., Stillman, F. A. & Samet, J. M. A review of tobacco smoking and smoking cessation practices among physicians in China: 1987–2010. Tobacco control 22, 9–14 (2013).
Liu, X. & Liu, L. Sleep habits and insomnia in a sample of elderly persons in China. Sleep 28, 1579–87 (2005).
Zhang, H.-S. et al. A community-based cross-sectional study of sleep quality in middle-aged and older adults. Quality of Life Research, 1–11 (2016).
Liu, R.-Q. et al. Poor sleep quality associated with high risk of hypertension and elevated blood pressure in China: results from a large population-based study. Hypertension Research 39, 54–59 (2016).
Furihata, R. et al. The association between sleep problems and perceived health status: a Japanese nationwide general population survey. Sleep medicine 13, 831–837 (2012).
Hinz, A. et al. Sleep quality in the general population: psychometric properties of the pittsburgh sleep quality index, derived from a german community sample of 9284 people. Sleep Medicine, doi: 10.1016/j.sleep.2016.03.008 (2016).
Breslau, N., Roth, T., Rosenthal, L. & Andreski, P. Sleep disturbance and psychiatric disorders: a longitudinal epidemiological study of young adults. Biological psychiatry 39, 411–418 (1996).
Minowa, M., Uchiyama, M. & Okawa, M. Subjective sleep quality and sleep problems in the general Japanese adult population. Psychiatry and Clinical Neurosciences 55, 213–215 (2001).
Okubo, N. et al. Relationship between self-reported sleep quality and metabolic syndrome in general population. BMC public health 14, 562 (2014).
Alimohamad Asghari, M., Mohammad Farhadi, M., Seyed Kamran Kamrava, M., Babak Ghalehbaghi, M. & Marzieh Nojomi, M. Subjective sleep quality in urban population. Archives of Iranian medicine 15, 95 (2012).
Xiang, Y.-T. et al. The prevalence of insomnia, its sociodemographic and clinical correlates, and treatment in rural and urban regions of Beijing, China: a general population-based survey. Sleep 31, 1655 (2008).
Moreno, C. R., Lowden, A., Vasconcelos, S. & Marqueze, E. C. Musculoskeletal pain and insomnia among workers with different occupations and working hours. Chronobiology international 33, 749–753 (2016).
Zhao, Y. Leaving the countryside: rural-to-urban migration decisions in China. The American Economic Review 89, 281–286 (1999).
Zhang, H.-S. et al. Sleep quality and health service utilization in Chinese general population: A cross-sectional study in Dongguan, China. Sleep Medicine 27-28, 9–14 (2016).
Hou, J. & Ke, Y. Addressing the Shortage of Health Professionals in Rural China: Issues and Progress: Comment on’Have Health Human Resources Become More Equal between Rural and Urban Areas after the New Reform?’. Int J Health Policy Manag 4, 327–328 (2015).
Astell-Burt, T. et al. Health reform and mortality in China: multilevel time-series analysis of regional and socioeconomic inequities in a sample of 73 million. Scientific reports 5, 15038 (2015).
Li, R., Wing, Y., Ho, S. & Fong, S. Gender differences in insomnia—a study in the Hong Kong Chinese population. Journal of Psychosomatic Research 53, 601–609 (2002).
Zhang, B. & Wing, Y. K. Sex differences in insomnia: a meta-analysis. Sleep 29, 85–93 (2006).
Krishnan, V. & Collop, N. A. Gender differences in sleep disorders. Current opinion in pulmonary medicine 12, 383–389 (2006).
Liu, X. & Liu, L. Sleep habits and insomnia in a sample of elderly persons in China. Sleep-new york then westchester 28, 1579 (2005).
Morphy, H., Dunn, K. M., Lewis, M., Boardman, H. F. & Croft, P. R. Epidemiology of insomnia: a longitudinal study in a UK population. Sleep 30, 274–80 (2007).
Tang, J. et al. Sleeping problems in Chinese illicit drug dependent subjects. BMC psychiatry 15, 28 (2015).
Liao, Y. et al. Sleeping problems among Chinese heroin-dependent individuals. The American journal of drug and alcohol abuse 37, 179–183 (2011).
Lexcen, F. J. & Hicks, R. A. Does cigarette smoking increase sleep problems? Perceptual and motor skills 77, 16–18 (1993).
Strine, T. W. & Chapman, D. P. Associations of frequent sleep insufficiency with health-related quality of life and health behaviors. Sleep medicine 6, 23–27 (2005).
Kaneita, Y. et al. Insomnia among Japanese adolescents: a nationwide representative survey. Sleep 29, 1543 (2006).
Roberts, R. E., Shema, S. J., Kaplan, G. A. & Strawbridge, W. J. Sleep complaints and depression in an aging cohort: A prospective perspective. Am J Psychiatry 157, 81–8 (2000).
Backhaus, J., Junghanns, K., Broocks, A., Riemann, D. & Hohagen, F. Test–retest reliability and validity of the Pittsburgh Sleep Quality Index in primary insomnia. Journal of psychosomatic research 53, 737–740 (2002).
Tsai, P.-S. et al. Psychometric evaluation of the Chinese version of the Pittsburgh Sleep Quality Index (CPSQI) in primary insomnia and control subjects. Quality of Life Research 14, 1943–1952 (2005).
Acknowledgements
The study was supported by the Natural Science Foundation of China (Grant No. 81371480 to J.T., 81671325 to Y.L. and 81471361 to X.C.), the National Key Basic Research and Development Program (973) (Grant No. 2012CB517904 to X.C.). The authors would like to acknowledge all the participants. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
J.T. and Y.L. designed the project. X.C. supervises J.T. and Y.L.’s work and provided guidance in the conception and design of the project. Y.L., J.T., L.X., C.Q., C.P., W.H. and T.L. collected the data. Y.L., F.Z. and Y.X. analyzed the data. J.T. and Y.L. wrote the first manuscript. B.K., F.Z. and Y.X. commented on and revised the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Tang, J., Liao, Y., Kelly, B. et al. Gender and Regional Differences in Sleep Quality and Insomnia: A General Population-based Study in Hunan Province of China. Sci Rep 7, 43690 (2017). https://doi.org/10.1038/srep43690
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep43690
- Springer Nature Limited
This article is cited by
-
Comparative insomnia prevalence between geriatrics lived in urban and rural areas: a multicenter nationwide study analysis
BMC Public Health (2024)
-
The association between energy-adjusted dietary inflammatory index and physical activity with sleep quality: a cross-sectional study
BMC Nutrition (2024)
-
Prevalence and predictors of insomnia and its treatment-seeking among older adults in India
Journal of Activity, Sedentary and Sleep Behaviors (2024)
-
Shorter self-reported sleep duration is associated with worse virtual spatial navigation performance in men
Scientific Reports (2024)
-
Associations between masturbation frequency, anxiety, and sleep disturbances during the COVID-19 era
International Journal of Impotence Research (2024)