
Abstract
Chronic Obstructive Pulmonary Disease (COPD) is a global health concern. Mind–body exercises like Tai Chi and Yoga are suggested as non-pharmacological interventions for COPD management. This meta-analysis evaluates mind–body exercises' impact on lung function and exercise capacity in stable COPD patients, aiming to assess their effectiveness in rehabilitation. A systematic search across various databases identified relevant randomized controlled trials until April 2024. Primary outcomes included lung function tests (FEV1, FVC, FEV1/FVC, FEV1%) and Six-Minute Walk Test (6MWT) results. The Standardized Mean Difference (SMD) measured intervention effects. Fifteen studies with 1047 participants were analyzed. Mind–body exercises significantly improved FEV1 (SMD = 0.87), FEV1/FVC (SMD = 0.19), FEV1% (SMD = 0.43), and 6MWT (SMD = 1.21) compared to standard care. Sensitivity and subgroup analyses confirmed result stability despite some heterogeneity.In conclusion, Mind–body exercises enhance lung function and exercise capacity in stable COPD patients. Integrating them into comprehensive rehabilitation programs is advisable. Further research should explore the specific impacts of different exercise types and intensities.
Similar content being viewed by others

Explore related subjects
Find the latest articles, discoveries, and news in related topics.Introduction
Chronic Obstructive Pulmonary Disease (COPD) is recognized globally as a major public health concern, not only due to its high prevalence and mortality rates but also because of its severe impact on the daily life quality of patients. Characterized by persistent airway restriction and limited airflow, patients with COPD often experience progressive symptoms such as breathing difficulties, limited activity, and acute exacerbations, which further deteriorate their quality of life. The primary objectives in the management of COPD are to alleviate symptoms, decelerate lung function decline, maintain or enhance exercise capacity and life quality, thus minimizing disability and maximizing benefits for the patients. Therefore, identifying effective intervention strategies is of paramount importance.
Although pharmacological treatments play a critical role in controlling symptoms and reducing acute episodes, non-pharmacological treatments, especially rehabilitative exercise, are equally vital for improving lung function and exercise capabilities of the patients. Previous studies have shown that high-intensity aerobic or resistance exercises could benefit the rehabilitation of COPD patients1. However, other studies suggest that high-intensity exercises may not be suitable for COPD patients2. Given that most COPD patients are middle-aged to elderly and experience respiratory distress, it is advisable to choose exercises that are slow, gentle, and of low intensity. Mind–body exercises have garnered widespread attention as a holistic treatment method due to their gentle nature, rhythmic breathing adjustments, and ease of learning. Defined by the National Institutes of Health and the National Center for Complementary and Integrative Health as an alternative and complementary medicine3, mind–body exercises represent a multimodal exercise category that encompasses features of aerobic and resistance activities4,5. This includes traditional Chinese exercises such as Tai Chi, Wuqinxi (Five-Animal Exercises), Yi Jinjing, Baduanjin as well as Indian practices like Yoga and meditation6. These exercises not only involve physical activity but also incorporate breathing techniques and psychological relaxation elements, characterized by focused, relaxed, meditative, and gentle physical movements7 and are adaptable to various environments (e.g., home, office)8. They aim to enhance the overall health status of COPD patients. However, despite preliminary evidence supporting the benefits of mind–body exercises, reports in the scientific literature regarding their effects are inconsistent9,10. Moreover, studies on the rehabilitation effectiveness for stable COPD patients often have small sample sizes and vary in design11,12. Due to differences in intervention programs (Tai Chi, Qigong, Yoga), duration, frequency, and duration of interventions, the specific impacts of mind–body exercises on lung function and exercise capacity in COPD patients remain unclear. In light of these considerations, the present study aims to systematically evaluate the existing literature on the effects of mind–body exercises on the rehabilitation outcomes in stable COPD patients through a meta-analysis. This is intended to provide robust scientific evidence, support evidence-based clinical treatment and rehabilitation, and further facilitate an understanding and improvement of treatment strategies for this disease.
Methods
This study has been registered on the PROSPERO platform with the registration ID CRD42024547593.
Literature search strategy
The literature search strategy for this study was meticulously developed in accordance with the PRISMA guidelines13 and based on the principles of evidence-based medicine defined by the PICOS criteria. The search strategy involved stringent criteria for retrieving, including, screening, and excluding studies. For Chinese databases such as CNKI, WFDSP, and VIP, a Boolean logic search was conducted with Chinese keywords ("Pulmonary Disease, Chronic Obstructive" or "COPD" or "Chronic Obstructive Lung Disease") and ("Mind and body exercise" or "physical and mental exercise" or "Yoga" or "Mediation" or "Tai Chi" or "Baduanjin" or "Qigong" or "Yijinjing" or "Wuqinxi"). For international databases including Elsevier ScienceDirect, Web of Science, PubMed, ProQuest, Scopus, and The Cochrane Library, English keywords were used in a Boolean search: ("Pulmonary Disease, Chronic Obstructive" or "Chronic Obstructive Lung Disease" or "Chronic Obstructive Pulmonary Diseases" or "COAD" or "COPD" or "Chronic Obstructive Airway Disease" or "Chronic Obstructive Pulmonary Disease" or "Airflow Obstruction, Chronic" or "Chronic Airflow Obstructions") and ("Mind and body exercise" or "Mind and body Therapy" or "Mind–body exercise" or "Yoga" or "Meditation" or "Taichi" or "Baduanjin" or "Qigong" or "Yijinjing" or "Wuqinxi"). The search formulas were adapted to the specific features of each database. Additionally, manual searches of references from included studies and relevant reviews were conducted to ensure the completeness of the literature retrieved. The search was limited to documents published in Chinese and English, with Chinese sources restricted to core journals. The search timeframe spanned from the inception of each database until April 2024. Searches for unpublished academic literature were not conducted. An example of the search conducted in PubMed is presented in Box 1
Inclusion and exclusion criteria
Inclusion criteria
Studies included in this review must meet the following criteria: ① Only randomized controlled trials (RCTs) are included; ② Participants diagnosed with Chronic Obstructive Pulmonary Disease (COPD); ③ Interventions for the experimental group include any form of mind–body exercises such as Yoga, Meditation, Tai Chi, Qigong including Baduanjin, Liuzijue, and Yijinjing, whereas control group interventions involve standard care and treatment for COPD patients or unstructured physical activities; ④ Outcome measures include lung function (FEV1, FVC, FEV1/FVC ratio, FEV1%) and exercise capacity (6MWT).
Exclusion criteria
Exclusion criteria are as follows: ① Duplicated publications; ② Non-RCT studies; ③ Animal studies; ④ Descriptive and survey studies, reviews, and conference proceedings; ⑤ Non-Chinese or English publications; ⑥ Studies where results are not presented in the form of (x ± s) or where data extraction is not feasible; ⑦ Studies with additional interventions during the intervention period; ⑧ Incomplete data description or data that cannot be converted; ⑨ Chinese publications not from core journals; ⑩ Patients in an acute exacerbation phase or interventions lasting less than four weeks.
Literature screening and data extraction
Two researchers independently conducted the literature search using Endnote 21 software to collate the collected documents and eliminate duplicates. The titles and abstracts were then independently screened. Full texts were read in detail according to the inclusion and exclusion criteria for further selection. The results of the selections were cross-checked between the two researchers; if discrepancies occurred, a third researcher was consulted to discuss and reach a consensus. Data extraction from the final included studies was conducted using a pre-designed data extraction form, which included the following: ① basic information of the studies (title, first author, year of publication, etc.); ② characteristics and information of the subjects (sample size, age, etc.); ③ details of the interventions and controls (type, duration, frequency, etc.); ④ quality of the studies; ⑤ outcome measures and main findings.
Assessment of risk of bias in included studies
The risk of bias in the included studies was assessed independently by two researchers using the Cochrane Collaboration's tool for assessing risk of bias (version 5.1 of the Cochrane Handbook)14. The assessment covered seven domains: sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, completeness of outcome data, selective reporting, and other sources of bias. Each domain was rated as high risk, unclear, or low risk. Disagreements were resolved through discussion. If inconsistencies persisted, a resolution was sought through discussion with another researcher.
Statistical analysis
The statistical analyses were conducted using RevMan 5.4 software for traditional meta-analysis and assessment of literature quality. Since different tools were used across studies for the same outcomes, standardized mean differences (SMD) and 95% confidence intervals were used as effect size measures, with baseline significance set at α = 0.05. The SMD is a measure that expresses the difference between two group means in terms of their pooled standard deviation, allowing for the comparison of effects across different scales. Heterogeneity among studies was assessed using I2 and P-values. If I2 ≤ 50% and P > 0.10, homogeneity was assumed, and a fixed-effect model was used for analysis; if I2 > 50% and P ≤ 0.10, indicating heterogeneity, a random-effects model was applied, supplemented by subgroup and sensitivity analyses to explore the sources of heterogeneity. Sensitivity testing and publication bias analysis were performed using Stata-MP 17 software from the Computing Resource Center, USA.
Results
Literature search and screening
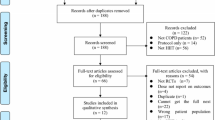
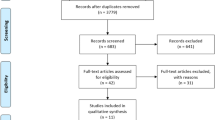
A preliminary search yielded 2161 documents. After a rigorous screening process, 15 studies were finally included. The screening process and results are detailed in Fig. 1.

Flow of study selection.
Characteristics of the included studies and assessment of methodological quality
The final inclusion comprised 15 studies, with a total of 1047 participants (Table 1). The observation periods ranged from 8 to 52 weeks, with intervention frequencies of 2 to 7 times per week, and each session lasted between 30 to 60 min. All included studies were randomized controlled trials. Thirteen of the studies reported specific randomization methods: three studies used random number tables15,16,17, five utilized computer-generated random methods18,19,20,21,22, one study employed cluster randomization23, and two applied block randomization24,25. Two studies utilized random methods such as drawing lots or tossing coins for randomization. Due to the nature of the exercise therapies and the requirement for informed consent, none of the trials were double-blinded. Nine studies16,18,21,22,23,24,25,26,27 implemented single-blinding. The assessment of the quality of the studies is depicted in Figs. 2 and 3.

Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Meta-analysis results
Lung function outcomes
The effects of mind–body exercises on lung function in COPD patients included Forced Expiratory Volume in One Second (FEV1), Forced Vital Capacity (FVC), the ratio of FEV1 to FVC (FEV1/FVC), and the percentage of FEV1 as predicted (FEV1%).
In this study, nine articles17,18,20,22,23,24,26,27,28 involving a total of 671 patients compared the maximum exhalation indicators (FEV1) between two groups of COPD patients. Significant heterogeneity was observed among the studies (df = 8, P < 0.00001, I2 = 92%), necessitating the use of a random-effects model for analysis. The results indicated that mind–body exercise interventions significantly improved FEV1 in COPD patients (SMD = 0.87, 95%CI [0.26, 1.48], P = 0.005), demonstrating that mind–body exercises can enhance FEV1, as shown in Fig. 4.

Effects of Mind–body Exercise on FVE1.
Six studies17,18,20,22,24,26, totaling 504 individuals (254 in the experimental group and 250 in the control group), assessed FVC. A meta-analysis of these six studies showed considerable heterogeneity (I2 = 91%, P < 0.00001). Following sensitivity analysis, which involved removing data with significant bias from studies by Chan et al.22 and Thokchom et al.20, the heterogeneity significantly decreased (I2 = 6%, P = 0.36). The results revealed no statistically significant differences between the two groups in terms of FVC levels (SMD = 0.08, 95% CI[− 0.14, 0.29], P = 0.49), suggesting that mind–body exercises had a similar impact on FVC levels as the control interventions, as depicted in Fig. 5.

Effects of Mind–body Exercise on FVC.
Seven articles18,20,21,23,24,27,29 including a sample of 539 participants (269 in the experimental group, 270 in the control group) assessed the FEV1/FVC. The analysis found statistically significant effects of mind–body exercises on COPD interventions (P = 0.001) with a narrow confidence interval (SMD = 0.45, 95%CI [0.02, 0.88]) and high heterogeneity (I2 = 81%, P < 0.0001). After excluding data with significant bias from Thokchom20, the heterogeneity became negligible (I2 = 48%, P = 0.09), and the intervention effect remained statistically significant (SMD = 0.19, 95%CI [0.01, 0.37], P = 0.04), indicating that mind–body exercises can improve the FEV1/FVC in COPD patients, as shown in Fig. 6.

Effects of Mind–body Exercise on FEV1/FVC.
Seven studies16,17,21,23,27,28,29 that included FEV1% involved a total of 394 COPD patients (195 in the experimental group and 199 in the control group). A meta-analysis using a fixed-effects model showed low heterogeneity (I2 = 33%, P = 0.18). The results demonstrated that mind–body exercise interventions had a statistically significant effect on FEV1% (SMD = 0.43, 95%CI [0.23, 0.63], P < 0.0001), indicating a significant improvement in the FEV1% index for COPD patients following the intervention, as illustrated in Fig. 7.

Effects of Mind–body Exercise on FEV1%
Exercise capacity outcomes
Twelve studies15,16,17,18,19,20,21,22,23,25,26,27 analyzed the impact of mind–body exercises on the Six-Minute Walk Test (6MWT) in patients with COPD, involving a total of 728 participants (370 in the experimental group and 358 in the control group). A meta-analysis of these studies indicated considerable heterogeneity (I2 = 86%, P < 0.00001). The heterogeneity remained largely unchanged after sequentially excluding individual studies, necessitating the use of a random-effects model for the combined analysis. The results demonstrated a statistically significant difference between the two groups in terms of the 6MWT levels (SMD = 1.21, 95%CI [0.77, 1.66], P < 0.00001). This suggests that mind–body exercises can significantly improve the 6MWT performance in COPD patients, as shown in Fig. 8.

Effects of Mind–body Exercise on 6MWT.
Subgroup analysis
In order to understand the impact of intervention duration, frequency, and session length on pulmonary function and exercise capacity, subgroup analyses were conducted. The results of the subgroup analysis for lung function are presented in Table 2, and the results for the impact on the 6MWT are shown in Table 3.
Intervention duration
For lung function outcomes, given the heterogeneity observed in FEV1, a subgroup analysis was conducted to further explore the sources of heterogeneity. Among the nine studies included for the FEV1 indicator, four studies18,20,23,28 with an intervention duration between 12 and 24 weeks showed a pooled effect size of SMD = 1.92 (95%CI [0.38, 3.46], P = 0.01). Four studies22,24,26,27 exceeding 24 weeks showed a pooled effect size of SMD = 0.47 (95%CI [− 0.19, 1.13], P = 0.16), and one study17 shorter than 12 weeks had an SMD of − 0.36 (95%CI [− 0.97, 0.26], P = 0.26). Interventions lasting < 12 weeks and ≥ 24 weeks did not show a statistically significant difference in their impact on FEV1 (P > 0.05). However, interventions exceeding 12 weeks demonstrated statistically significant improvements in FEV1 compared to other durations (P < 0.05).
In the 12 studies analyzing the 6MWT, five studies15,18,19,20,23 with intervention durations ≥ 12 weeks and < 24 weeks showed a pooled effect size of SMD = 1.32 (95%CI [0.76, 1.87], P < 0.00001); six studies16,21,22,23,25,26,27 with durations over 24 weeks had a pooled effect size of SMD = 1.32 (95%CI [0.63, 2.01], P = 0.0002). Both intervention durations showed statistically significant differences in exercise capacity compared to control groups. The effect size for interventions ≥ 12 weeks was higher than those < 12 weeks (SMD = -0.02), suggesting that mind–body exercise interventions of more than 12 weeks have a greater impact on the 6MWT in COPD patients.
Intervention frequency
Among the nine studies included for the FEV1 indicator, studies with a frequency of more than three times per week18,20,23,24,27 showed a pooled effect size of SMD = 1.63 (95%CI [0.46, 2.79], P = 0.005). Studies with a frequency of three times per week17,26 showed a combined effect size of SMD = − 0.1 (95%CI [0.57, 0.37], P = 0.006), and studies with less than three times per week15,18,20,21,22,23,27,28 showed a combined effect size of SMD = 0.35 (95%CI [0.05, 0.66], P = 0.02). Significant statistical differences were observed in the impact on exercise capacity across all three frequencies (P < 0.05), with the highest effect observed in groups exercising more than three times per week, suggesting that this frequency has the greatest impact on lung function in COPD patients.
For the 12 studies included for the 6MWT, six studies15,18,20,21,23,27 with a frequency of more than three times per week showed a combined effect size of SMD = 1.65 (95%CI [0.87, 2.44], P < 0.0001). Four studies (16,17,25,26 with a frequency of three times per week had a combined effect size of SMD = 0.86 (95%CI [0.34, 1.38], P = 0.001), and two studies19,22 with a frequency of less than three times per week had a combined effect size of SMD = 0.59 (95%CI [0.26, 0.92], P = 0.0004). Significant statistical differences were observed in the impact on exercise capacity across all frequencies (P < 0.01), indicating that the improvement in 6MWT is ranked as follows based on frequency: more than three times per week > three times per week > less than three times per week.
Intervention time
In the nine studies considering the FEV1 index, one26 did not specify the time of each mind–body exercise intervention and was thus excluded from the subgroup analysis. Two studies17,24 with each session lasting 30 min or less showed a pooled effect size of SMD = − 0.12 (95%CI [− 0.38, 0.13], P = 0.35), which was not statistically significant (P > 0.05). Six studies18,20,22,23,27,28 where each session exceeded 30 min showed a pooled effect size of SMD = 1.46 (95%CI [0.57, 2.35], P = 0.001), indicating a statistically significant difference (P < 0.05). Therefore, it is inferred that mind–body exercise interventions longer than 30 min per session have the greatest impact on lung function in COPD patients.
In the 12 studies assessing the 6MWT, one study26 did not report the time of each mind–body exercise intervention and was not included in the subgroup analysis. Ten studies with session exceeding 30 min showed a pooled effect size of SMD = 1.34 (95%CI [0.85, 1.83], P < 0.00001), which was statistically significant. One study with a session duration of 30 min showed a combined effect size of SMD = − 0.02 (95%CI [− 0.64, 0.60], P = 0.96), which was not statistically significant, but the comparison between groups was statistically significant. Thus, it is presumed that mind–body exercise interventions lasting more than 30 min per session have the greatest impact on exercise capacity in COPD patients.
Intervention type
In the 12 studies assessing the 6MWT and conducting a subgroup analysis of intervention types, Tai Chi, Qigong, Baduanjin, Liuzijue and Yijinjing which are collectively recognized as “Health Qigong” in China, were combined into one group and compared with a yoga group. The health qigong group15,16,17,18,19,21,22,23,25,26,27showed a combined effect size of SMD = 1.10, while the yoga group 20(SMD = 2.67) demonstrated a significantly greater effect, which may be due to the large variance resulting from only one study being included in the yoga group. Thus, this significant difference should be interpreted with caution.
Publication bias analysis
For this study, funnel plots were drawn for the indices FEV1 and 6MWT to analyze their symmetry and assess the presence of publication bias, as shown in Figs. 9 and 10. The distribution of data points in the funnel plot is asymmetric, suggesting the presence of some degree of publication bias in the included literature. The asymmetry in the Funnel plot indicates that studies with non-significant results may be less likely to be published, potentially leading to an overestimation of the intervention effects. Additionally, the variability in sample sizes across the included studies may contribute to the observed heterogeneity. Studies with smaller sample sizes are more susceptible to random errors and may not accurately capture the true effect of mind–body exercises on COPD outcomes. The studies included in this analysis vary greatly in terms of intervention duration, ranging from a minimum of 8 weeks to a maximum of 52 weeks, and baseline information across studies could differ significantly, potentially introducing bias.

Funnel Plot (FEV1).

Funnel Plot (6MWT).
Discussion
Impact of mind–body exercises on lung function and exercise capacity
This study analyzes the impact of mind–body exercises on the rehabilitation of patients with stable Chronic Obstructive Pulmonary Disease (COPD), particularly on lung function and exercise capacity. Lung function in COPD patients is characterized by a decline assessed as reduced expiratory airflow, necessitating lung ventilation function tests measuring FEV1, FEV1%, FEV1/FVC, and FVC30. These indices are often used as outcomes in COPD patient studies due to their reproducibility, ease of measurement, and relevance31. The meta-analysis indicates that mind–body exercises have a moderate effect on lung function, significantly enhancing FEV1 (SMD = 0.87, 95% CI [0.26, 1.48], P = 0.005) and FEV1% (SMD = 0.43, 95% CI [0.23, 0.63], P < 0.0001), and showing improvement in FEV/FVC, though the effect on FVC was not significant (SMD = 0.08, 95% CI [− 0.14, 0.29], P = 0.49), suggesting a trend towards improvement following the intervention. Overall, mind–body exercises can enhance lung function in COPD patients. Subgroup analyses reveal that conducting exercises for more than 12 weeks, more than three times per week, and for over 30 min each session is most beneficial for lung function improvement.
COPD patients often experience restricted airflow and progressive pulmonary hyperinflation, leading to abnormal thoracoabdominal respiratory movements and reduced respiratory muscle function, skeletal muscle dysfunction, and atrophy32. Consequently, COPD patients typically exhibit significantly reduced exercise capacity, making this a defining feature of the disease. Clinically, the Six-Minute Walk Test (6MWT) is a primary method for assessing exercise capacity, with improvements in 6MWT scores indicating enhanced physical capability. The overall results of this meta-analysis show that mind–body exercises significantly improve exercise capacity in COPD patients (SMD = 1.21, 95%CI [0.77, 1.66], P < 0.00001), consistent with findings from other studies such as those by Meng et al.33. Extensive research demonstrates the effects of Tai Chi and similar exercises on physical capability. Yan et al.34 found that Tai Chi not only improves lung function and reduces symptoms of dyspnea in COPD patients but also enhances their exercise capacity. Subgroup analysis indicates that interventions of more than 12 weeks, with frequencies over three times per week, and sessions lasting longer than 30 min each, exhibit the most significant statistical differences in exercise capability, suggesting that longer durations and higher frequencies of such exercises are most effective.
The improvement in lung function among COPD patients might be due to the integration of traditional breathing exercises such as diaphragmatic breathing and pursed-lip breathing with physical movements in practices like Tai Chi and Yoga35. These exercises involve deep, slow abdominal breathing predominantly through diaphragmatic movement, with breathing guided by mindfulness36. For instance, Tai Chi emphasizes the harmony of 'mind, breath, and form,' coordinating internal energy with breathing for enhanced movement efficiency 37,38. Yoga offers various breathing techniques and specialized practices that enhance respiratory efforts, like abdominal breathing, bellows breath (Bhastrika), yoga postures, breath retention (Kumbhaka), alternating nostril breathing (Nadi Shodhana), or unilateral nostril breathing (Surya Bhedana)39. Under the regulation of the higher respiratory centers, the coordination of muscle contraction and respiratory cycles enhances respiratory muscle training, increasing endurance and thus pulmonary capacity. The potential mechanism may involve dilating spastic arterioles to prevent collapse of the bronchioles, improving oxygen diffusion in the lungs, elevating alveolar oxygen partial pressure, and subsequently increasing both tidal volume and residual volume, improving clinical symptoms and signs40,41,42.
Exploring the mechanisms by which mind–body exercises impact exercise capacity, it is hypothesized that the necessity for shifting the center of gravity, adjusting posture, and performing slow movements under controlled breathing might be one contributing factor. For example, Tai Chi stresses "taking the waist as the axis," requiring a variety of balanced postures typically performed in a semi-squat position, facilitating spine-led movements that fully engage joints such as the shoulders, elbows, wrists, hips, knees, and ankles, beneficial for strengthening muscular endurance43. In Baduanjin's " Holding Up the Sky with Both Hands to Regulate the Sanjiao. " practitioners stand straight and lift their hands upward, shifting their center of gravity upwards. In " Using Both Hands Skillfully like the Hero of the Legend of the Codor Heroes.," practitioners step to the left or right while adjusting their breathing and posture to stretch the muscles and enhance physical health44. Wuqinxi involve mimicking animal movements and expressions through body stretching, bending, and rotation to exercise muscles and joints45. Similarly, Yoga incorporates various postures aimed at enhancing flexibility and balance through stretching and extending the body. These activities involve stretching different muscles and mobilizing joints, thus improving exercise capacity in COPD patients. Additionally, during mind–body practices, participants are required to maintain focus and avoid distractions, engaging the nervous system to facilitate rapid excitation transfer, resulting in highly excitable muscle fibers and an increased number of active muscle fibers, further enhancing exercise capacity function46,47.
Comparison with previously published meta-analyses
Although the results of this study align with most of the existing literature8,48, the effect sizes noted in some key indicators are more significant here. This might be due to our meta-analysis including the latest studies and employing stricter inclusion criteria and statistical methods, which help reduce bias and enhance the accuracy of results. Notably, our study introduces a granular subgroup analysis that dissects the impact of various durations, frequencies, and session lengths of mind–body interventions on lung function and exercise capacity—a dimension not extensively explored in prior meta-analyses. By encompassing a broader spectrum of mind–body exercises and considering the heterogeneity of intervention strategies, our research offers a significant extension and complement to the existing body of literature.
Limitations
This systematic review has certain limitations. Firstly, three of the fifteen included studies were assessed as being of low quality. Hence, low methodological quality could affect the strength of the evidence. Secondly, the range in sample sizes, from a minimum of 30 to a maximum of 198 participants, may introduce greater bias. Thirdly, the methodological quality of the included studies varied. The unknown allocation concealment in several studies raises the possibility of selection bias, which may have influenced the assignment of patients to the intervention group, and this is a limitation that must be considered when interpreting the results. Fourth, the types and durations of interventions varied significantly among the studies, increasing the heterogeneity of the results. Lastly, the studies included were primarily focused on stable COPD, with benefits during acute exacerbations yet to be explored, which may be a focus for future research. Given these limitations, our results should be interpreted with caution.
Future research directions
In light of the findings and limitations of the current study, such as the small number of reports and the variability in study design, it is essential that future research adopts a more standardized approach. Firstly, large-scale, multi-center, randomized controlled trials should be conducted to validate the long-term effects and safety of mind–body exercises on lung function and exercise capacity in COPD patients. Secondly, a three-arm comparison study involving yoga, tai chi, and a no-exercise control group could offer a comprehensive understanding of the comparative benefits of these interventions. Future empirical studies may focus on combined interventions, such as different types of exercises combined with pharmacological treatments, to develop optimal synergistic treatment strategies for specific outcomes. Theoretical research should delve into classifying and grading the mechanisms by which mind–body exercises impact COPD, explaining the common or unique mechanisms behind each phenomenon, aiming to provide objective and comprehensive theoretical bases for COPD patients.
Conclusion
This meta-analysis underscores the potential value of mind–body exercises in improving lung function and exercise capacity in patients with stable COPD. In the absence of adverse events, clinicians might consider incorporating this training modality into the frontline rehabilitation plans for COPD patients. Overall, despite some limitations, mind–body exercises have demonstrated significant roles as non-pharmacological treatment options in the comprehensive management of COPD patients. Future research needs to further explore the optimal implementation of these interventions to maximize their benefits for patient health.
Data availability
All data generated or analysed during this study are available to readers upon request to the author YT-Z.
References
Butcher, S. J. & Jones, R. L. The impact of exercise training intensity on change in physiological function in patients with chronic obstructive pulmonary disease. Sports Med. 36, 307–325 (2006).
Nici, L. et al. American thoracic society/European respiratory society statement on pulmonary rehabilitation. Am. J. Resp. Crit. Care Med. 173, 1390–1413 (2006).
Complementary, N. C. f. & Health, I. Complementary, alternative, or integrative health: What’s in a name? Maryland (2018).
Zou, L., Loprinzi, P. D., Yeung, A. S., Zeng, N. & Huang, T. The beneficial effects of mind-body exercises for people with mild cognitive impairment: A systematic review with meta-analysis. Arch. Phys. Med. Rehabil. 100, 1556–1573 (2019).
Wang, J., Meng, J. & Guo, Z. Z. Systematic review on the impact of mind-body exercises on sleep quality. Chin. J. Rehabil. Theory Pract. 29, 205–213 (2023).
Li, Z., Liu, S., Wang, L. & Smith, L. Mind–body exercise for anxiety and depression in copd patients: A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 17, 22 (2020).
Li, H. et al. A RCT reticulated meta-analysis of six MBE therapies affecting college students' negative psychology. Iscience (2023).
Wang, K., Liu, S., Kong, Z., Zhang, Y. & Liu, J. Mind-body exercise (Wuqinxi) for patients with chronic obstructive pulmonary disease: A systematic review and meta-analysis of randomized controlled trials. Int. J. Environ. Res. Public Health 16, 72 (2019).
Norweg, A. M. et al. Mind-body intervention for dysfunctional breathing in chronic obstructive pulmonary disease: Feasibility study and lessons learned. J. Integr. Comp. Med. 29, 156–168 (2023).
Papp, M. E., Henriques, M., Biguet, G., Wändell, P. E. & Nygren-Bonnier, M. Experiences of hatha yogic exercises among patients with obstructive pulmonary diseases: A qualitative study. J. Bodywork Movem. Ther. 22, 896–903 (2018).
Yeh, G. Y. et al. Tai chi mind-body exercise in patients with COPD: Study protocol for a randomized controlled trial. Trials 15, 1–13 (2014).
Malik, S. et al. Exercise capacity in patients with chronic obstructive pulmonary disease treated with tele-yoga versus tele-pulmonary rehabilitation: A pilot validation study. Cureus 14 (2022).
Liberati, A. et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. Ann. Internal Med. 151, W65–W94 (2009).
Liu, M., Wu, H. & Wei, M. Systematic Review, Meta-Analysis Design and Implementation Methods. (2011).
Du, S. T. et al. The impact of Tai Chi exercise on the BODE index and SGRQ scores in patients with chronic obstructive pulmonary disease. Chin. J. Sports Med. 32, 403–407. https://doi.org/10.1603/j.1000-6710.2013.05.007 (2013).
Zhu, S. et al. A modified 6-form Tai Chi for patients with COPD. Comp. Ther. Med. 39, 36–42. https://doi.org/10.1016/j.ctim.2018.05.007 (2018).
Pan, Y. et al. Evaluation of the therapeutic effect of 24-form simplified Tai Chi in the pulmonary rehabilitation of patients with stable chronic obstructive pulmonary disease. Chin. J. Rehabil. Med. 33, 681–686 (2018).
Jiang, L. et al. Effects of pulmonary-based Qigong exercise in stable patients with chronic obstructive pulmonary disease: A randomized controlled trial. BMC Comp. Med. Ther. 23, 418. https://doi.org/10.1186/s12906-023-04238-8 (2023).
Liu, X. et al. Effects of water-based Liuzijue exercise on peak exercise capacity, functional exercise capacity, and quality of life in people with COPD. Clin. Resp. J. 15, 956–966. https://doi.org/10.1111/crj.13399 (2021).
Thokchom, S. K., Gulati, K., Ray, A. & Menon, B. K. Effects of yogic intervention on pulmonary functions and health status in patients of COPD and the possible mechanisms. Comp. Ther. Clin. Pract. 33, 20–26. https://doi.org/10.1016/j.ctcp.2018.07.008 (2018).
Li, P. et al. Effects of long-term home-based Liuzijue exercise combined with clinical guidance in elderly patients with chronic obstructive pulmonary disease. Clin. Interventions Aging 13, 1391–1399. https://doi.org/10.2147/CIA.S169671 (2018).
Chan, A. W. K., Lee, A., Suen, L. K. P. & Tam, W. W. S. Tai chi Qigong improves lung functions and activity tolerance in COPD clients: A single blind, randomized controlled trial. Comp. Ther. Med. 19, 3–11. https://doi.org/10.1016/j.ctim.2010.12.007 (2011).
Wang, L., Wu, K., Chen, X. & Liu, Q. The effects of Tai Chi on lung function, exercise capacity and health related quality of life for patients with chronic obstructive pulmonary disease: A pilot study. Heart Lung Circ. 28, 1206–1212. https://doi.org/10.1016/j.hlc.2018.05.204 (2019).
Luo, C., Jiang, H., Li, H. & Chi, X. Effects of Tai Chi on patients with moderate to severe COPD in stable phase. Medicine 102, e33503. https://doi.org/10.1097/md.0000000000033503 (2023).
Liu, X.-D. et al. Therapeutic effects of Qigong in patients with COPD: A randomized controlled trial. Hong Kong J. Occup. Ther. 22, 38–46. https://doi.org/10.1016/j.hkjot.2012.06.002 (2012).
Kantatong, T., Panpanich, R., Deesomchok, A., Sungkarat, S. & Siviroj, P. Effects of the tai chi qigong programme on functional capacity, and lung function in chronic obstructive pulmonary disease patients: A ramdomised controlled trial. J. Trad. Comp. Med. 10, 354–359. https://doi.org/10.1016/j.jtcme.2019.03.008 (2020).
Zhang, M., Xv, G., Luo, C., Meng, D. & Ji, Y. Qigong Yi Jinjing promotes pulmonary function, physical activity, quality of life and emotion regulation self-efficacy in patients with chronic obstructive pulmonary disease: A pilot study. J. Altern. Comp. Med. 22, 810–817. https://doi.org/10.1089/acm.2015.0224 (2016).
Yudhawati, R. & Mariani Rasjid, H. S. Effect of yoga on FEV1, 6-minute walk distance (6-MWD) and quality of life in patients with COPD group B. Adv. Resp. Med. 87, 261–268. https://doi.org/10.5603/ARM.2019.0047 (2019).
Yang, D. L., Wu, J. H. & Han, Z. J. Evaluation of the therapeutic effect of fitness Qigong Baduanjin in pulmonary rehabilitation of patients with stable chronic obstructive pulmonary disease. Chin. Gen. Pract. 20, 356–358 (2017).
Zhou, M. J. & Zheng, J. P. Clinical practical methods, indicators, and significance of pulmonary function testing. Chin. J. Pract. Internal Med. 32, 575–577 (2012).
Donohue, J. F. Minimal clinically important differences in COPD lung function. COPD J. Chronic Obstruct. Pulmonary Dis. 2, 111–124 (2005).
Bonnevie, T. et al. The six-minute stepper test is related to muscle strength but cannot substitute for the one repetition maximum to prescribe strength training in patients with COPD. Int. J. Chronic Obstructive Pulmonary Dis., 767–774 (2019).
Ding, M., Zhang, W., Li, K. & Chen, X. Effectiveness of t’ai chi and qigong on chronic obstructive pulmonary disease: A systematic review and meta-analysis. J. Altern. Comp. Med. 20, 79–86 (2014).
Yan, J.-H., Guo, Y.-Z., Yao, H.-M. & Pan, L. Effects of Tai Chi in patients with chronic obstructive pulmonary disease: Preliminary evidence. PloS one 8, e61806 (2013).
Yang, X. et al. The effects of a customized yoga breathing exercise on pulmonary rehabilitation and depression in COPD patients. J. Nurs. Sci. 30, 18–21 (2015).
Zou, L. et al. Effects of mind–body movements on balance function in stroke survivors: A meta-analysis of randomized controlled trials. Int. J. Environ. Res. Public Health 15, 1292 (2018).
Xu, W. J. & Li, Y. K. Interpretations of Tai Chi Theory and Methods. J. Beijing Sport Univ. 34, 1–4 (2011).
Li, J., Hong, Y. & Chan, K. Tai chi: Physiological characteristics and beneficial effects on health. Br. J. Sports Med. 35, 148–156 (2001).
Brown, R. P. & Gerbarg, P. L. Yoga breathing, meditation, and longevity. Ann. New York Acad. Sci. 1172, 54–62 (2009).
Cleutjens, F. A. et al. The impact of cognitive impairment on efficacy of pulmonary rehabilitation in patients with COPD. J. Am. Med. Directors Assoc. 18, 420–426 (2017).
Engel, R. M., Gonski, P., Beath, K. & Vemulpad, S. Medium term effects of including manual therapy in a pulmonary rehabilitation program for chronic obstructive pulmonary disease (COPD): A randomized controlled pilot trial. J. Manual Manipul. Ther. 24, 80–89 (2016).
Schroff, P. et al. Pulmonary rehabilitation improves outcomes in chronic obstructive pulmonary disease independent of disease burden. Ann. Am. Thoracic Soc. 14, 26–32 (2017).
Zhang, L. L., Ke, D. D., Wu, W. & Lu, D. J. The effects of Tai Chi on physical fitness and health in humans. Chin. J. Gerontol. 37, 2309–2312 (2017).
Zou, L. et al. A review study on the beneficial effects of Baduanjin. J. Altern. Comp. Med. 24, 324–335 (2018).
Guo, Y. et al. Beneficial effects of qigong wuqinxi in the improvement of health condition, prevention, and treatment of chronic diseases: Evidence from a systematic review. Evid.-Based Comp. Altern. Med. 2018 (2018).
Pelegrino, N. R. G. et al. Influence of lean body mass on cardiopulmonary repercussions during the six-minute walk test in patients with COPD. Jornal Brasileiro de Pneumologia 35, 20–26 (2009).
Celli, B. R. et al. The body-mass index, airflow obstruction, dyspnea, and exercise capacity index in chronic obstructive pulmonary disease. New England J. Med. 350, 1005–1012 (2004).
Wu, L.-L. et al. Effectiveness of meditative movement on COPD: A systematic review and meta-analysis. Int. J. Chronic Obstructive Pulmonary Dis., 1239–1250 (2018).
Author information
Authors and Affiliations
Contributions
Y.T.-Z. designed the study and was responsible for the literature search and screening process, data extraction, and statistical analysis. Y.T.-Z. also drafted the initial manuscript and made substantial revisions to the entire text. Z.H.-D. contributed to the study design and data extraction, provided technical support for the data analysis, and made significant modifications and corrections to the initial draft to ensure data accuracy and the soundness of the analysis. Z.H.-Z. conducted the literature search and screening process, assisted with data extraction and organization, and contributed to the writing and revision of the manuscript, particularly in the methods and results sections. F.-Z. provided the conceptual framework and overall guidance for the study, supervised all stages of the research, ensured the project proceeded as planned. F.-Z. also provided the necessary data and supplementary information as required.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zhu, Y., Zhang, Z., Du, Z. et al. Mind–body exercise for patients with stable COPD on lung function and exercise capacity: a systematic review and meta-analysis of RCTs. Sci Rep 14, 18300 (2024). https://doi.org/10.1038/s41598-024-69394-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-69394-4
- Springer Nature Limited