
Abstract
It remains unclear whether and how maternal exposure to biomass fuel influences infant anthropometry or body proportionality at birth, which are linked to their survival, physical growth, and neurodevelopment. Therefore, this study seeks to explore the association between household-level exposure to biomass cooking fuels and infant size and body proportionality at birth among women in rural Bangladesh. A total of 909 women were derived from the Pregnancy Weight Gain study, which was conducted in Matlab, a rural area of Bangladesh. Infant’s weight (g), length (cm), head circumference (cm), small for gestational age (SGAW), short for gestational age (SGAL), low head circumference for gestational age (SGAHC), ponderal index, and cephalization index at birth were the outcomes studied. Of the women, 721 (79.3%) were dependent on biomass fuel. Compared to infants born to mothers who used gas for cooking, those born to biomass users had lower weight (β − 94.3, CI − 155.9, − 32.6), length (β − 0.36, 95% CI − 0.68, − 0.04), head circumference (β − 0.24, CI − 0.47, − 0.02) and higher cephalization index (β 0.03, CI 0.01, 0.05) at birth. Maternal biomass exposure is more likely to lead to symmetric SGA, although there is evidence for some brain-sparing effects.
Similar content being viewed by others


Explore related subjects
Find the latest articles, discoveries, and news in related topics.Introduction
Infants who are born small for gestational age (SGA)—frequently due to fetal growth restriction (FGR)—are inevitably at greater risk of childhood mortality and morbidity. In addition to that, they are more likely to experience poor linear growth, neurodevelopmental delay, and a higher incidence of non-communicable diseases in adulthood, which ultimately lead to reduced human capital1,2,3,4. An estimated 23.3 million infants were born small for gestational age (SGA) in low- and middle-income countries (LMICs) in 20125. Bangladesh ranked fourth for the total burden of SGA births, with a prevalence of 30.5%5. Any conditions that impede the transplacental transfer of oxygen and nutrients may hinder fetal growth and eventually cause SGA6. In addition to poor maternal nutrition, adolescent pregnancy, inadequate gestational weight gain7, infections during pregnancy, and pregnancy-induced hypertension5,6,7,8, certain environmental factors such as maternal smoking and air pollution have been found to negatively influence infant size at birth9.
Around 2.4 billion people worldwide rely on biomass fuels such as wood, charcoal, crop leftovers, or animal dung as their principal source of domestic energy for cooking, including more than half of households in developing nations and up to 95% in low-income countries10,11,12. In Bangladesh, overall, 82% of the households and 95% of the households in rural areas cook using biomass fuels13. The low-efficiency biomass fuels are generally burnt in traditional, poorly enclosed and ventilated stoves, which results in incomplete combustion of the fuels and emission of several air pollutants such as particulate matter, carbon monoxide, and polycyclic aromatic hydrocarbons14,15. The women in the households, especially those involved in cooking, are predominantly exposed to noxious biomass smoke16. As reproductive-aged women are the main cooks in their households, there is an increasing interest in exploring how this exposure affects the health of pregnant women and the growing fetus. Studies have linked reduced birth weight with maternal exposure to household air pollution resulting from inefficient combustion of biomass cooking fuels17,18,19. A recent systematic review has evaluated the available evidence from nineteen published studies of the impact of burning solid fuels (biomass or coal) on pregnancy outcomes. The pooled estimates reveal that household solid fuel combustion results in an 86.43 g (95% CI 55, 117) reduction in birth weight and a 35% increase in the risk of low birth weight (LBW)20.
The FGR can lead to the birth of an infant who is small in terms of weight, length, head circumference, or any combination of those. It is generally believed that factors such as chronic undernutrition21,22,23 (stunting), smoking24,25, and long-term exposure to toxic substances26,27,28, including biomass fuel, which are present even before conception, affect weight, length, and head circumference proportionately. Conversely, a late pregnancy insult as maternal vascular disorders such as pregnancy-induced hypertension supposedly reduces birth weight but spare length and the brain (head circumference)27,28,29. In LMICs, symmetric SGAs are more common30.
Most studies examining the effect of biomass fuel exposure have focused only on birth weight, either as a continuous measure or as LBW (< 2500 g)17,18,19. Previous research has established an association between maternal biomass fuel exposure and preterm birth6,9,20,31. However, it remains unclear whether and how maternal exposure to biomass fuel influences infant length, head circumference, size, or body proportionality at birth, particularly in full-term infants, which are linked to their survival, physical growth, and neurodevelopment. Furthermore, birth weight, as a standalone fetal growth indicator, has several well-known limitations32,33. To address this issue and advance the understanding, our study investigated the effects of household-level maternal exposure to biomass cooking fuels on size and body proportionality at birth among full-term infants in rural Bangladesh.
Methods
Study setting
The study took place in Matlab, a rural area of Bangladesh. In Matlab, the International Centre for Diarrhoeal Disease Research, Bangladesh (icddr,b) maintains a Health and Demographic Surveillance System (HDSS) that covers a population of 230,000 along with the central health facility, Matlab Hospital. Demographic information from people residing in the surveillance area is collected through quarterly home visits. Trained Community Health Research Workers collect data on Tablet Computers through in-person interviews34. The HDSS also conducts household socioeconomic censuses at a certain interval (usually every 10 years). In 2014, a socioeconomic census was conducted to update the socioeconomic status of households within the HDSS. A structured questionnaire was used to collect the data35.
Children under 5 years and reproductive-aged (15 to 49 years) women from the icddr,b service area receive free-of-cost care from the hospital. Maternal care services provided include vaginal delivery and antenatal and postnatal care. Referrals are made if cesarean delivery is required. The setting has been described in detail elsewhere36.
Data for this study were derived from the Pregnancy Weight Gain study, which evaluated the status of gestational weight gain and its determinants among women in Matlab. The methodology of the study has been published elsewhere37. The study included 1883 pregnant women admitted to Matlab Hospital’s labor ward between 2012 and 2014. These women had singleton live births at term, and they sought routine antenatal care from the same facility in the second trimester. All anthropometric measurements were taken following standard procedures at Matlab Hospital. The date of the last menstrual period (LMP) was considered for the estimation of gestational age, and it was confirmed by a pregnancy ultrasound at the first antenatal visit.
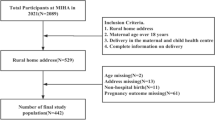
This study analyzed a sub-sample of 909 women who gave live birth to singleton infants by normal vaginal delivery at 37 completed to 42 weeks of gestation and were dependent on either gas or biomass as a cooking fuel at the household level. Those with missing information on infant weight, length, or head circumference at birth (n = 723 in cesarean delivery and n = 28 in normal vaginal delivery) or cooking fuel use (n = 71) were excluded. Matlab Hospital does not offer cesarean delivery services. If a cesarean delivery is indicated, pregnant women are referred to other facilities that offer the service. Since cesarean section deliveries do not occur at Matlab Hospital, data on birth anthropometry, especially head circumference and length, are not available in the hospital database. Women using electricity (n = 2) or both gas and biomass (n = 146) as cooking fuel were also excluded from the analysis. Figure 1 illustrates the selection of the sample for this study.

The process of selecting the sample for the study.
Cooking fuel
Information on women’s household-level cooking fuel use around the time of delivery of the child included in the study was retrieved from the electronic database of HDSS. Wood, wood dust, paddy husk, crop residues (straw), and dry leaves comprised biomass fuel. Gas included natural gas (gas line) and liquid petroleum gas (gas cylinder).
Covariates
We carefully reviewed the literature to choose the covariates for this study35,36,37,38,39,40. Covariates considered were maternal age (≤ 19 years, 20–34 years, ≥ 35 years), parity (nulliparous, 1 prior birth, 2 prior births, 3 or more prior births), height (≤ 145 cm, > 145 cm), level of education (≤ 5 years, 6–9 years, ≥ 10 years), length of gestation (days), rate of weight gain during the 2nd and 3rd trimester of pregnancy (kg/week), infant sex, and socioeconomic status (wealth quintile). The rate of weight gain was calculated by subtracting the weight measured during the prenatal visit from the weight measured before childbirth and dividing it by the difference between the weeks. Wealth quintile, an indicator of household-level wealth consistent with expenditure and income measures, was constructed by dividing a calculated household asset score into five quantiles. The household asset score was derived using principal component analysis (PCA) of the variables indicating possession of household assets35.
Outcomes
Infant’s weight (g), length (cm), head circumference (cm), small for gestational age (SGAW), short for gestational age (SGAL), low head circumference for gestational age (SGAHC), ponderal index and cephalization index at birth were the outcomes of the present study. An infant was defined SGAW if his/her birth weight was less than the 10th percentile of birth weight7,41, SGAL if his/her crown-heel length at birth was less than the 10th percentile of birth length42 and SGAHC if his/her birth head circumference was less than the 10th percentile of birth head circumference for specific sex and gestational age as compared to the international newborn standards from the INTERGROWTH-21st project40 Ponderal index (birth weight in grams/crown-heel birth length in centimeters cubed × 100), reflects thinness of the newborn and the magnitude of the asymmetry in fetal growth—the lower the ponderal index, the higher the asymmetry43. Cephalization index (birth head circumference in centimeters/birth weight in grams × 100) is an indicator of the severity of FGR and the extent of the brain-sparing process—the higher the cephalization index, the higher the brain-sparing effect44.
Statistical analysis
We presented the sample characteristics as mean ± standard deviation or frequency measures, as appropriate. We compared the background characteristics of the participants in the present sample with those who were excluded from the original dataset using the Student’s t-test for continuous variables and the chi-square test for categorical variables. The characteristics of the gas users and biomass fuel users were compared using the Student’s t-test or the chi-square test, as appropriate.
Simple and multivariable linear regression models were fitted to assess the association of biomass fuel use with infant weight, length, head circumference, ponderal index, and cephalization index at birth. The strength of association was expressed as mean difference (β) with a 95% confidence interval (95% CI), considering gas users as the reference group. To assess the association of biomass fuel use with SGAW, SGAL, and SGAHC, simple and multivariable logistic regression models were fitted. The strength of association was expressed as odds ratio (OR) with 95% CI; gas users constituted the reference group.
All the multivariable linear regression models included the following covariates of a priori interest: maternal age, height, parity, length of gestation, rate of weight gain during the 2nd and 3rd trimester, level of education, wealth quintile, and infant sex. All the multivariable logistic regression models included the following covariates of a priori interest: maternal age, height, parity, rate of weight gain during the 2nd and 3rd trimester, level of education, and wealth quintile.
All statistical tests were two-sided, and statistical significance was evaluated at p < 0.05. The percentiles of birth weight, length and head circumference were derived using the INTERGROWTH-21st tool “Neonatal Size Calculator for newborn infants between 24 + 0 and 42 + 6 weeks’ gestation”. Other statistical analyses were performed with Stata/PC (StataCorp, College Station, Texas 77845 USA, version 15.1).
Ethical statement
This study was conducted under the oversight of the Institutional Review Board of icddr,b and in accordance with the principles of the Declaration of Helsinki. The original study protocol (PR-16028) was reviewed and approved by the icddr,b research and ethical review committees (Institutional Review Board of icddr,b).
The study used de-identified routinely collected surveillance and service data that were available through the electronic databases of Matlab Health and Demographic Surveillance System (HDSS) and Matlab Hospital of icddr,b. The study did not involve any primary interviews with the participants or collect biological samples from them. Since data were evaluated retrospectively, pseudonymously, and were solely obtained for treatment and surveillance purposes, the requirement for informed consent was waived by the Institutional Review Board of icddr,b.
Results
The study population differed in several background characteristics from those excluded from the original dataset (Supplementary Table 1). The proportion of nulliparous women was lower in the present sample (35.2% vs. 52.0%). Women in the present sample were more frequently from the lowest two wealth quintiles (39.9% vs. 26.5%), while those who completed secondary education were less frequent (15.8% vs. 26.3%). The rate of weight gain (kg/week) during the 2nd and 3rd trimester of pregnancy was also lower among women in the present sample compared to those who were excluded (0.32 ± 0.2 vs. 0.37 ± 0.2).
The study included a sample of 909 women, out of which 79.3% relied on biomass fuel for cooking in their households, while 20.7% used gas, as shown in Table 1. Among the women, the highest percentage (73.8%) belonged to the age group of 20 to 34 years, while 19.3% were adolescents, as shown in Table 2. The study also revealed that 13.9% of the mothers had a height of less than or equal to 145 cm, and 57.8% of the women had 6–9 years of education. Furthermore, 35.2% of the women in the sample were nulliparous, meaning that they had not given birth to a child before (Table 2).
Results indicate that mothers who used gas as cooking fuel during the 2nd and 3rd trimester of pregnancy gained weight at a higher rate (0.36 ± 0.19 kg/week) than those who used biomass fuel (0.31 ± 0.20 kg/week). Infants born to gas users had a higher body weight (2913.0 ± 378.7 g), length (48.0 ± 1.7 cm), and head circumference (33.3 ± 1.3 cm), but a lower cephalization index (1.16 ± 0.13) at birth compared to those born to mothers who relied on biomass fuel. This suggests that gas usage during pregnancy may significantly promote fetal growth (t-test, p < 0.05) regarding anthropometric characteristics. Compared to gas users, infants born to biomass fuel users had a significantly (χ2-test, p < 0.05) higher prevalence of SGAW (44.5% vs. 31.9%), SGAL (37.9% vs. 27.7%), and SGAHC (32.3% vs. 22.3%). This indicates that using biomass fuel during pregnancy may hinder fetal growth, leading to a higher proportion of infants being smaller than expected for their gestational age.
In Table 3, the adjusted models revealed that infants born to mothers who depended on biomass for cooking had significantly lower weight (β − 94.3, CI − 155.9, − 32.6; p 0.003), length (β − 0.36, CI − 0.68, − 0.04; p 0.025) and head circumference (β − 0.24, CI − 0.47, − 0.02; p 0.036) at birth when compared to those born to mothers who depended on gas for cooking.
The findings from Table 4, which presents the results of the multivariable logistic regression models, indicate that women who use biomass for cooking have significantly higher odds of giving birth to infants with SGAW (OR 1.6, CI 1.1, 2.3; p 0.021), SGAL (OR 1.5, CI 1.0, 2.2; p 0.054), and SGAHC (OR 1.6, CI 1.1, 2.5; p 0.023) than their counterparts who use gas for cooking. This indicates that cooking with biomass could have detrimental effects on fetal growth and development.
The association of derived measures such as cephalization index and ponderal index with the use of cooking fuel type was shown in Table 5. Whereas in adjusted models, compared to children born to mothers who used gas for cooking, those born to biomass users had higher cephalization index (β 0.03, CI 0.01, 0.05; p 0.011), but there was no significant difference in ponderal index (β − 0.01, CI − 0.08, 0.07; p 0.892). This indicates that there was no significant difference in ponderal index between infants born to mothers exposed to gas or biomass.
Discussion
The present study was conducted to evaluate the impact of cooking fuel on fetal growth and development, including weight, length, and head circumference at birth. The research showed that an overwhelming 79.3% of women relied on biomass fuel as their primary energy source for cooking. These results are consistent with previous studies that found over 80% of households in developing countries use biofuels for cooking and heating6. Overall, the study suggests that the type of fuel used during pregnancy has an impact on fetal development and birth outcomes.
The present study has identified a significant association between maternal biomass fuel exposure and adverse fetal outcomes, including small for gestational age (SGAW), short for gestational age (SGAL), and low head circumference for gestational age (SGAHC). This finding is consistent with the results of a pair-matched case–control study conducted in a Peruvian population, which revealed that the use of biomass as cooking fuel was associated with a higher risk of low birth weight (LBW) and a significantly increased risk of SGA45,46. Exposure to indoor biomass fuel has been found to be strongly associated with SGA (small for gestational age) infants, as per a population-based cohort study conducted in South India47. Additionally, it has been established through previous research that toxic or chemical exposure is a major contributing factor to SGA infants26,48,49.
Biomass fuel is a type of fuel known for its relatively low efficiency due to incomplete combustion45,47,50, which results in the emission of airborne particulate matter (PM) and toxic chemicals such as aromatic hydrocarbons, oxygenated organics, free radicals, and carbon monoxide, at a high level51,52. Traditionally, biomass fuels have been used in partially confined cooking spaces, with women of childbearing age being the most vulnerable. As women typically continue to perform domestic and cooking duties throughout their pregnancy, the growing fetus is also indirectly exposed to these toxic substances of biomass fuels53. Previous research has suggested that indoor exposure to the toxic substances of biomass fuels can compromise fetal growth, even in populations where low birth weight is relatively rare6,47,54.
Carbon monoxide (CO), one of the main toxic substances of biomass smoke, crosses the placental barrier55 and compromises oxygen transfer to the tissue of the fetus56 because CO binds more readily with fetal hemoglobin than adult hemoglobin57. The fetal growth may be reduced as a result of this tissue hypoxia. PM exposure may cause oxidative stress, activate pulmonary and placental inflammation, alter blood coagulation factors, influence endothelial functions, and provoke hemodynamic responses through impaired transplacental oxygen and nutrient exchange, which restrict fetal growth58. Due to their reaction with placental growth factor receptors, polycyclic aromatic hydrocarbons (PAHs) may directly affect early trophoblast proliferation. They hamper the fetoplacental exchange of oxygen and nutrients and ultimately impair the growth of the fetus59. Because of these reasons, CO has been directly associated with increased infant mortality, LBW, preterm birth (PTB)60, particulate matters with SGA births61,62, and PAHs with fetal developmental abnormalities, LBW and SGA births47,63.
A study conducted in Washington and New York found that prenatal exposure to PAH increased the risk of symmetric intrauterine growth restriction by twofold64. Similarly, the present analysis showed that maternal exposure to biomass cooking fuel is associated with a decrease in birth weight, head circumference, and length. These findings suggest that maternal biomass fuel exposure leads to proportionate SGA. Additionally, the study found that maternal exposure to biomass cooking fuel is significantly associated with higher odds of SGA for weight and head circumference and marginally associated with SGA for length. This study also indicates that biomass fuel exposure is associated with increased cephalization index. A prospective study conducted among 10-year-old children in Tel Aviv found that a larger head size relative to body weight was associated with lower neurodevelopmental scores, IQ, and academic performance44. The more severe the clinical pathology, especially the probability of developing cerebral palsy and severe psychomotor retardation, the higher the cephalization score, which indicates a larger degree of brain vulnerability65.
In this study, mothers exposed to biomass cooking fuel are more likely to have babies with symmetric or proportionate SGA. However, there is some evidence that this type of exposure may have a sparing effect on the brain—although this requires further investigation to understand both the mechanisms at play and the potential consequences. The smoke of biomass fuel containing a complex mixture of various gases and breathable particles has been linked to adverse effects on human reproduction, including low birth weight (LBW) and small for gestational age (SGA)6,14,50,66. Although previous research studies were not able to shed light on the association between maternal biomass fuel exposure and proportionality at the birth of children, they clearly indicated that biomass fuel exposure is strongly associated with LBW as well as SGA47,60,63. In order to support fetal growth and promote well-being, it is crucial to minimize maternal exposure to biomass fuel, particularly in developing countries where negative pregnancy outcomes are already common. Unfortunately, despite the known risks to maternal and child health, biofuel usage remains widespread in rural areas due to its affordability and lack of awareness45.
It’s important to take action to prevent harmful smoke exposure during pregnancy, which can cause both symmetric and asymmetric SGA in newborns. The goal of interventions should be to reduce exposure to biomass fuel smoke and to ensure safety, fuel efficiency, and environmental protection. Along with these, interventions should be cost-effective and sustainable. Gas (natural or liquefied petroleum gas) is a better choice for cooking to prevent exposure to biomass fuel. However, gas supply is not always cost-effective in resource-poor settings. To mitigate this issue, our neighboring country, India, recently executed two innovative programs—Give It Up (GIU) and Smokeless Village (SV)—to bring clean cooking via liquefied petroleum gas (LPG) to the rural poor. The GIU initiative encourages better-off Indian households to voluntarily give up their LPG subsidies and redirects those subsidies one-for-one to below-poverty-line families. This strategy connects every household in a village to LPG and involves close collaboration with India’s three national oil companies67. Our government, stakeholders, and policymakers could apply these strategies to make cleaner fuel available. Given limited resources, the government and stakeholders can prioritize the need for cleaner fuel by focusing on the rural population, where 95% of households cook using biomass fuels.
Improved stoves can be an excellent alternative to conventional biomass stoves in terms of cost-effectiveness and sustainability. Previous research has shown that improved stoves can reduce ambient pollution and personal exposure68,69,70. A multi-year cookstove intervention study in rural India found that improved stoves like rockets and gasifiers could be possible alternatives to traditional biomass stoves71. Better housing facilities with proper ventilation systems also play an important role in reducing the level of exposure to toxic fumes from biomass. Separate kitchens, outdoor kitchens, or kitchens with long chimneys could be incorporated into rural household architectures to reduce exposure to harmful substances from biomass11. Additionally, raising awareness among rural people through community and health education about household air pollution and the health hazards of exposure to biomass fuel are important approaches72.
Strength and limitations
The strengths of this study include comprehensive data on 909 mother-infant pairs, covering information on socioeconomic, demographic, health, and nutrition-related variables. However, the findings should be interpreted with caution due to several important limitations. The study utilized routinely collected service and surveillance data retrieved from electronic databases. Such routine data may contain errors, data linkage issues, and misclassification biases. Routine anthropometric measurements, especially head circumference, are prone to measurement errors. Another limitation is the cross-sectional and binary nature of the exposure measurement; the lack of information on the duration and intensity of exposure may lead to misclassification bias. Lastly, the exclusion of many mother-infant pairs, especially those with preterm and cesarean births, may limit the generalizability of the findings to the broader community. Interestingly, many women in Matlab end up delivering by cesarean section at private clinics, most of which are not clinically indicated. In Bangladesh, the rate of clinically non-indicated cesarean deliveries is increasing dramatically73,74. Currently, 45% of all births in Bangladesh are delivered via cesarean section, and Matlab is no exception75. In Matlab, most of the cesarean sections are done on maternal request and are not associated with any biological causes or clinical indications36,73. Nonetheless, community-based prospective studies with comprehensive data on the magnitude, length, and nature of biomass fuel exposure, household environment, and extending the analyses to preterm and cesarean births are needed to inform the external validity of the present study.
Conclusion
The current study revealed that maternal biomass exposure is likely to contribute to the occurrence of symmetric SGA with some brain-sparing effect. This study provided evidence supporting the importance of achieving the following sustainable development goals—SDG3 Good health & wellbeing, SDG7 Affordable and clean energy, SDG11 Sustainable cities and communities. This study recommended that access to clean household energy is a possible solution to combat the adverse effects on maternal and child health. It is important to consider the implications of these findings, particularly as we strive to promote sustainability and environmental responsibility. We recommend that further research be conducted to explore the potential effects of different fuel sources on maternal and fetal health. This will enable us to make informed choices that balance environmental sustainability with the health and well-being of mothers and their fetuses.
Data availability
Data described in the article, code book, and analytic code will be made available upon request, pending adequate permissions. Interested researchers may contact Shiblee Sayeed, Senior Manager, Research Administration, icddr,b (shiblee_s@icddrb.org) to request access to the data.
References
Black, R. E. et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 382, 427–451. https://doi.org/10.1016/s0140-6736(13)60937-x (2013).
IOM (Institute of Medicine). Weight Gain During Pregnancy: Reexamining the Guidelines (The National Academies Press, 2009).
Barker, D. J. Fetal nutrition and cardiovascular disease in later life. Br. Med. Bull. 53, 96–108. https://doi.org/10.1093/oxfordjournals.bmb.a011609 (1997).
Bertino, E., Milani, S., Fabris, C. & De Curtis, M. Neonatal anthropometric charts: What they are, what they are not. Arch. Dis. Child Fetal Neonatal Ed. 92, F7–F10. https://doi.org/10.1136/adc.2006.096214 (2007).
Lee, A. C. et al. Estimates of burden and consequences of infants born small for gestational age in low and middle income countries with INTERGROWTH-21(st) standard: Analysis of CHERG datasets. BMJ 358, j3677. https://doi.org/10.1136/bmj.j3677 (2017).
Boy, E., Bruce, N. & Delgado, H. Birth weight and exposure to kitchen wood smoke during pregnancy in rural Guatemala. Environ. Health Perspect. 110, 109–114. https://doi.org/10.1289/ehp.02110109 (2002).
Hasan, S. M. T., Khan, M. A. & Ahmed, T. Inadequate maternal weight gain in the third trimester increases the risk of intrauterine growth restriction in rural Bangladesh. PLoS ONE 14, e0212116. https://doi.org/10.1371/journal.pone.0212116 (2019).
Ornoy, A. Prenatal origin of obesity and their complications: Gestational diabetes, maternal overweight and the paradoxical effects of fetal growth restriction and macrosomia. Reprod. Toxicol. 32, 205–212. https://doi.org/10.1016/j.reprotox.2011.05.002 (2011).
Jiang, M. et al. Exposure to cooking fuels and birth weight in Lanzhou, China: A birth cohort study. BMC Public Health 15, 712. https://doi.org/10.1186/s12889-015-2038-1 (2015).
Smith, K. R., Mehta, S. & Maeusezahl-Feuz, M. Indoor air pollution from household use of solid fuels. In Comparative Quantification of Health Risks: Global and Regional Burden of Disease Attributable to Selected Major Risk Factors, Vol. 2, 1435–1493 (2004).
Prasad, R., Singh, A., Garg, R. & Giridhar, G. B. Biomass fuel exposure and respiratory diseases in India. Biosci. Trends 6, 219–228. https://doi.org/10.5582/bst.2012.v6.5.219 (2012).
World Resources Institute, UNEP, UNDP & World Bank. 1998–1999 World Resources: A Guide to the Global Environment (Oxford University Press, 1998).
National Institute of Population Research and Training (NIPORT), Mitra and Associates, ICF International. Bangladesh Demographic and Health Survey 2014 (NIPORT, Mitra and Associates, and ICF International, 2016).
Naeher, L. P. et al. Woodsmoke health effects: A review. Inhal. Toxicol. 19, 67–106. https://doi.org/10.1080/08958370600985875 (2007).
de Koning, H. W., Smith, K. R. & Last, J. M. Biomass fuel combustion and health. Bull. World Health Organ. 63, 11–26 (1985).
Bruce, N., Perez-Padilla, R. & Albalak, R. Indoor air pollution in developing countries: A major environmental and public health challenge. Bull. World Health Organ. 78, 1078–1092 (2000).
Lee, B. E. et al. Exposure to air pollution during different gestational phases contributes to risks of low birth weight. Hum. Reprod. 18, 638–643. https://doi.org/10.1093/humrep/deg102 (2003).
Dejmek, J., Selevan, S. G., Benes, I., Solanský, I. & Srám, R. J. Fetal growth and maternal exposure to particulate matter during pregnancy. Environ. Health Perspect. 107, 475–480. https://doi.org/10.1289/ehp.99107475 (1999).
Bobak, M. Outdoor air pollution, low birth weight, and prematurity. Environ. Health Perspect. 108, 173–176. https://doi.org/10.1289/ehp.00108173 (2000).
Amegah, A. K., Quansah, R. & Jaakkola, J. J. Household air pollution from solid fuel use and risk of adverse pregnancy outcomes: A systematic review and meta-analysis of the empirical evidence. PLoS ONE 9, e113920. https://doi.org/10.1371/journal.pone.0113920 (2014).
Delpisheh, A., Brabin, L., Drummond, S. & Brabin, B. J. Prenatal smoking exposure and asymmetric fetal growth restriction. Ann. Hum. Biol. 35, 573–583. https://doi.org/10.1080/03014460802375596 (2008).
Akram, D. S. & Arif, F. Ponderal index of low birth weight babies—A hospital based study. J. Pak. Med. Assoc. 55, 229–231 (2005).
Barker, D. J. Fetal origins of coronary heart disease. BMJ 311, 171–174. https://doi.org/10.1136/bmj.311.6998.171 (1995).
Davies, D. P. & Abernethy, M. Cigarette smoking in pregnancy: Associations with maternal weight gain and fetal growth. Lancet 1, 385–387. https://doi.org/10.1016/s0140-6736(76)90215-4 (1976).
Boström, C. E. et al. Cancer risk assessment, indicators, and guidelines for polycyclic aromatic hydrocarbons in the ambient air. Environ. Health Perspect. 110(Suppl 3), 451–488. https://doi.org/10.1289/ehp.110-1241197 (2002).
Maciejewski, E., Hamon, I., Fresson, J. & Hascoet, J. M. Growth and neurodevelopment outcome in symmetric versus asymmetric small for gestational age term infants. J. Perinatol. 36, 670–675. https://doi.org/10.1038/jp.2016.48 (2016).
Bakketeig, L. S. Current growth standards, definitions, diagnosis and classification of fetal growth retardation. Eur. J. Clin. Nutr. 52(Suppl 1), S1–S4 (1998).
Aagaard-Tillery, K. M., Porter, T. F., Lane, R. H., Varner, M. W. & Lacoursiere, D. Y. In utero tobacco exposure is associated with modified effects of maternal factors on fetal growth. Am. J. Obstet. Gynecol. 198(66), e61–e66. https://doi.org/10.1016/j.ajog.2007.06.078 (2008).
Resnik, R. Intrauterine growth restriction. Obstetr. Gynecol. 99, 490–496 (2002).
Villar, J., Altobelli, L., Kestler, E. & Beliźan, J. A health priority for developing countries: The prevention of chronic fetal malnutrition. Bull. World Health Organ. 64, 847–851 (1986).
Stieb, D. M., Chen, L., Eshoul, M. & Judek, S. Ambient air pollution, birth weight and preterm birth: A systematic review and meta-analysis. Environ. Res. 117, 100–111. https://doi.org/10.1016/j.envres.2012.05.007 (2012).
Berg, C. J., Wilcox, L. S. & d’Almada, P. J. The prevalence of socioeconomic and behavioral characteristics and their impact on very low birth weight in black and white infants in Georgia. Matern. Child Health J. 5, 75–84. https://doi.org/10.1023/a:1011344914802 (2001).
Juárez, S., Revuelta-Eugercios, B. A., Ramiro-Fariñas, D. & Viciana-Fernández, F. Maternal education and perinatal outcomes among Spanish women residing in southern Spain (2001–2011). Matern. Child Health J. 18, 1814–1822. https://doi.org/10.1007/s10995-013-1425-4 (2014).
icddr,b. Health and Demographic Surveillance System-Matlab, v. 51. Registration of Health and Demographic Events 2016, Scientific Report No. 138 (icddr,b, 2018).
icddr,b. Health and Demographic Surveillance System–Matlab, v. 48. Household Socio Economic Census 2014. http://dspace.icddrb.org:8080/jspui/bitstream/123456789/6323/5/HSEC_Matlab%20HDSS_%202014%20Final_09May2016.pdf (icddr,b, 2016).
Hasan, S. M. T., Khan, M. A. & Ahmed, T. Institute of medicine recommendations on the rate of gestational weight gain and perinatal outcomes in Rural Bangladesh. Int. J. Environ. Res. Public Health 18, 519. https://doi.org/10.3390/ijerph18126519 (2021).
Hasan, S. M. T. et al. Magnitude and determinants of inadequate third-trimester weight gain in rural Bangladesh. PLoS ONE 13, e0196190. https://doi.org/10.1371/journal.pone.0196190 (2018).
Strauss, R. S. & Dietz, W. H. Low maternal weight gain in the second or third trimester increases the risk for intrauterine growth retardation. J. Nutr. 129, 988–993. https://doi.org/10.1093/jn/129.5.988 (1999).
Bisai, S. Maternal height as an independent risk factor for neonatal size among adolescent Bengalees in Kolkata, India. Ethiop. J. Health Sci. 20, 153–158. https://doi.org/10.4314/ejhs.v20i3.69444 (2010).
Villar, J. et al. International standards for newborn weight, length, and head circumference by gestational age and sex: The Newborn Cross-Sectional Study of the INTERGROWTH-21st Project. Lancet 384, 857–868. https://doi.org/10.1016/s0140-6736(14)60932-6 (2014).
de Onis, M. & Habicht, J. P. Anthropometric reference data for international use: Recommendations from a World Health Organization Expert Committee. Am. J. Clin. Nutr. 64, 650–658. https://doi.org/10.1093/ajcn/64.4.650 (1996).
Baum, U., Leino, T., Gissler, M., Kilpi, T. & Jokinen, J. Perinatal survival and health after maternal influenza A(H1N1)pdm09 vaccination: A cohort study of pregnancies stratified by trimester of vaccination. Vaccine 33, 4850–4857. https://doi.org/10.1016/j.vaccine.2015.07.061 (2015).
Choi, H., Rauh, V., Garfinkel, R., Tu, Y. & Perera, F. P. Prenatal exposure to airborne polycyclic aromatic hydrocarbons and risk of intrauterine growth restriction. Environ. Health Perspect. 116, 658–665. https://doi.org/10.1289/ehp.10958 (2008).
Leitner, Y. et al. Neurodevelopmental outcome of children with intrauterine growth retardation: A longitudinal, 10-year prospective study. J. Child Neurol. 22, 580–587. https://doi.org/10.1177/0883073807302605 (2007).
Yucra, S., Tapia, V., Steenland, K., Naeher, L. P. & Gonzales, G. F. Association between biofuel exposure and adverse birth outcomes at high altitudes in Peru: A matched case-control study. Int. J. Occup. Environ. Health 17, 307–313. https://doi.org/10.1179/107735211799041869 (2011).
Rich, D. Q. et al. Ambient air pollutant concentrations during pregnancy and the risk of fetal growth restriction. J. Epidemiol. Community Health 63, 488–496. https://doi.org/10.1136/jech.2008.082792 (2009).
Tielsch, J. M. et al. Exposure to indoor biomass fuel and tobacco smoke and risk of adverse reproductive outcomes, mortality, respiratory morbidity and growth among newborn infants in south India. Int. J. Epidemiol. 38, 1351–1363. https://doi.org/10.1093/ije/dyp286 (2009).
Moh, W., Graham, J. M. Jr., Wadhawan, I. & Sanchez-Lara, P. A. Extrinsic factors influencing fetal deformations and intrauterine growth restriction. J. Pregn. 2012, 750485. https://doi.org/10.1155/2012/750485 (2012).
Kaur, H., Bhalla, A. K. & Kumar, P. Longitudinal growth of head circumference in term symmetric and asymmetric small for gestational age infants. Early Hum. Dev. 88, 473–478. https://doi.org/10.1016/j.earlhumdev.2011.11.007 (2012).
Rinne, S. T. et al. Relationship of pulmonary function among women and children to indoor air pollution from biomass use in rural Ecuador. Respir. Med. 100, 1208–1215. https://doi.org/10.1016/j.rmed.2005.10.020 (2006).
Balakrishnan, K., Sambandam, S., Ramaswamy, P., Mehta, S. & Smith, K. R. Exposure assessment for respirable particulates associated with household fuel use in rural districts of Andhra Pradesh, India. J. Expo Anal. Environ. Epidemiol. 14(Suppl 1), S14–S25. https://doi.org/10.1038/sj.jea.7500354 (2004).
Pope, D. P. et al. Risk of low birth weight and stillbirth associated with indoor air pollution from solid fuel use in developing countries. Epidemiol. Rev. 32, 70–81. https://doi.org/10.1093/epirev/mxq005 (2010).
World Health Organization. The World Health Report: 2005: Make Every Mother and Child Count (World Health Organization, 2005).
Mishra, V., Dai, X., Smith, K. R. & Mika, L. Maternal exposure to biomass smoke and reduced birth weight in Zimbabwe. Ann. Epidemiol. 14, 740–747. https://doi.org/10.1016/j.annepidem.2004.01.009 (2004).
Sangalli, M. R., McLean, A. J., Peek, M. J., Rivory, L. P. & Le Couteur, D. G. Carbon monoxide disposition and permeability-surface area product in the foetal circulation of the perfused term human placenta. Placenta 24, 8–11. https://doi.org/10.1053/plac.2002.0877 (2003).
Di Cera, E. et al. Carbon monoxide and oxygen binding to human hemoglobin F0. Biochemistry 28, 2631–2638. https://doi.org/10.1021/bi00432a041 (1989).
Longo, L. D. The biological effects of carbon monoxide on the pregnant woman, fetus, and newborn infant. Am. J. Obstet. Gynecol. 129, 69–103. https://doi.org/10.1016/0002-9378(77)90824-9 (1977).
Kannan, S., Misra, D. P., Dvonch, J. T. & Krishnakumar, A. Exposures to airborne particulate matter and adverse perinatal outcomes: A biologically plausible mechanistic framework for exploring potential effect modification by nutrition. Environ. Health Perspect. 114, 1636–1642. https://doi.org/10.1289/ehp.9081 (2006).
Dejmek, J., Solanský, I., Benes, I., Lenícek, J. & Srám, R. J. The impact of polycyclic aromatic hydrocarbons and fine particles on pregnancy outcome. Environ. Health Perspect. 108, 1159–1164. https://doi.org/10.1289/ehp.001081159 (2000).
Currie, J. & Schmieder, J. F. Fetal exposures to toxic releases and infant health. Am. Econ. Rev. 99, 177–183. https://doi.org/10.1257/aer.99.2.177 (2009).
Wang, X., Ding, H., Ryan, L. & Xu, X. Association between air pollution and low birth weight: A community-based study. Environ. Health Perspect. 105, 514–520. https://doi.org/10.1289/ehp.97105514 (1997).
Shah, P. S. & Balkhair, T. Air pollution and birth outcomes: A systematic review. Environ. Int. 37, 498–516. https://doi.org/10.1016/j.envint.2010.10.009 (2011).
Ballester, F. et al. Air pollution exposure during pregnancy and reduced birth size: A prospective birth cohort study in Valencia, Spain. Environ. Health 9, 6. https://doi.org/10.1186/1476-069x-9-6 (2010).
Perera, F. P. et al. Effects of transplacental exposure to environmental pollutants on birth outcomes in a multiethnic population. Environ. Health Perspect. 111, 201–205. https://doi.org/10.1289/ehp.5742 (2003).
Harel, S., Tomer, A., Barak, Y., Binderman, I. & Yavin, E. The cephalization index: A screening device for brain maturity and vulnerability in normal and intrauterine growth retarded newborns. Brain Dev. 7, 580–584. https://doi.org/10.1016/s0387-7604(85)80005-x (1985).
Siddiqui, A. R. et al. Prenatal exposure to wood fuel smoke and low birth weight. Environ. Health Perspect. 116, 543–549. https://doi.org/10.1289/ehp.10782 (2008).
Smith, K. R. & Sagar, A. Making the clean available: Escaping India’s Chulha Trap. Energy Policy 75, 410–414. https://doi.org/10.1016/j.enpol.2014.09.024 (2014).
Lin, D. The development and prospective of bioenergy technology in China. Biomass Bioenergy 15, 181–186. https://doi.org/10.1016/S0961-9534(98)00007-5 (1998).
Ezzati, M., Mbinda, B. M. & Kammen, D. M. Comparison of emissions and residential exposure from traditional and improved cookstoves in Kenya. Environ. Sci. Technol. 34, 578–583. https://doi.org/10.1021/es9905795 (2000).
Pillarisetti, A., Jamison, D. T. & Smith, K. R. In Injury Prevention and Environmental Health (eds Jamison, D. T. et al.) (The International Bank for Reconstruction and Development/The World Bank, 2017).
Islam, M. M. et al. In-use emissions from biomass and LPG stoves measured during a large, multi-year cookstove intervention study in rural India. Sci. Total Environ. 758, 143698. https://doi.org/10.1016/j.scitotenv.2020.143698 (2021).
Pratiti, R. Household air pollution related to biomass cook stove emissions and its interaction with improved cookstoves. AIMS Public Health 8, 309–321. https://doi.org/10.3934/publichealth.2021024 (2021).
Begum, T. et al. Indications and determinants of caesarean section delivery: Evidence from a population-based study in Matlab, Bangladesh. PLoS ONE 12, e0188074. https://doi.org/10.1371/journal.pone.0188074 (2017).
Begum, T. et al. A qualitative study to explore the attitudes of women and obstetricians towards caesarean delivery in rural Bangladesh. BMC Pregn. Childbirth 18, 368. https://doi.org/10.1186/s12884-018-1993-9 (2018).
National Institute of Population Research and Training (NIPORT), ICF International. Bangladesh Demographic and Health Survey 2022 (NIPORT and ICF International, 2023).
Funding
Data for this study were derived from the Pregnancy weight-gain study, which was supported by the Swedish International Development Cooperation Agency (Sida) (to S. M. Tafsir Hasan). The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript. However, no funding was available for this analysis.
Author information
Authors and Affiliations
Contributions
The authors’ responsibilities were as follows—SMTH: designed research; SMTH, KNS, MAK, TA: conducted research; ZN, SMTH: analyzed data or performed statistical analysis; ZN and SMTH: wrote paper; TA, SMTH, ZN: had primary responsibility for final content; TA, SMTH, MAK: project administration; TA: study supervision; ZN, SMTH, KNS, MAK, TA: All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Nyma, Z., Hasan, S., Saqeeb, K. et al. Effects of maternal exposure to biomass cooking fuel on birth size and body proportionality in full-term infants born by vaginal delivery. Sci Rep 14, 18218 (2024). https://doi.org/10.1038/s41598-024-68821-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-68821-w
- Springer Nature Limited