
Abstract
Shift work has become increasingly common in modern society. Shift work has been associated with a range of negative health outcomes. Therefore, this 10-years retrospective cohort study, aimed to investigate the relationship between shift work and blood and metabolic parameters. This retrospective cohort study was conducted in a metal parts manufacturing industry in 2023. In this study, 204 shift workers and 204 day workers were examined. All the studied blood and metabolic parameters were collected by reviewing the medical records of all participants during a 10-years period (2013–2022). Moreover, the amounts of physical, chemical, and ergonomics harmful agents in the work environment were investigated. All the collected data were analyzed using SPSS version 25.0. The values of Body Mass Index (BMI), Red Blood Cell Count (RBC), Platelets Count (PLT), Thyroid-Stimulating Hormone Level (TSH), Fasting Blood Sugar Level (FBS), Creatinine, Triglyceride (TG), Liver Enzymes level (SGOT and SGPT), and Systolic Blood Pressure (SBP) were higher among the shift work employees, and a significant difference was observed between the values of these parameters between the two groups. The results of logistic regression showed that the highest effect of shift work was observed on the parameters of FBS, TG, SGPT, TSH, Physical activity, BMI, Sleep duration, PLT, and Sleep quality with beta coefficient values of 0.49, 0.33, 0.29, 0.29, 0.20, 0.18, 0.14, 0.13 and, 0.11, respectively (p-value < 0.01). The present study contributes to a growing body of evidence that blood and metabolic factors are likely to be influenced by shift work. These findings have important implications for policy makers, highlighting the need for interventions to mitigate the negative health effects of shift work on workers.
Similar content being viewed by others


Introduction
In today's society, working night shifts and other shifts outside of normal working hours is an integral part of many workers' jobs. As shift work is likely to exist in the future, it is important to study the potential health consequences of shift work1. The term shift work related to any work schedule that performed outside the hours of 7:00 am and 6:00 pm. Shift work can consist of evening, night, and early morning shifts, as well as fixed or rotating programs. Currently, nearly one-fifth of the total global workforce works on a shift basis2,3. The prevalence of shift work in many European countries is between 15 and 20 percent of the total working population, while in the United States of America this amount is 20 percent, in Singapore is 32 percent, and in Korea is 25 percent of the total working population4. According to available statistics, the prevalence of shift work has increased among many European by 15% and in the United States this amount is reached to 20% in men and 11% in women5.
Studies show that shift workers have a strong tendency to consume sweet and fast foods such as sausages and fatty foods. This diet can cause a variety of health problems, and diseases like obesity, high blood pressure and cardiovascular disease and cancer. Also, many studies revealed that shift workers suffer from mental disorders more compared to day workers6.
Shift work systems cause many health problems due to changes in the body's biological rhythm. Many functions of the body's circadian system depend on the body's metabolism and physiological functions7,8. Sleep disturbance in shift work systems, in addition to harming the performance of job duties and other psychological and social stressors, causes negative effects on the health of employees. Shift work is one of the common features of modern society. Many reports and researches in the past few decades have pointed to disruption of the endogenous circadian rhythm as the primary effect of shift work on health status9,10.
There are strong reasons that lack of sleep can impose adverse effects on the body metabolism and the immune system. Previous study revealed that individuals with low sleep quality had higher amounts of hemoglobin and hematocrit, monocytes, red blood cells, and platelet. The body's immune system has specialized cells that are responsible for defending the body against infection and foreign agents entering the body. The neutrophils and macrophages of the immune system make the first phase of defense against any microorganisms11. Previous findings revealed that the average of white blood cells increases in shift workers12. Sooriyaarachchi et al. reported that the level of white blood cells of health care workers with shift work is higher than others11.
Shift workers are exposed to risk factors for chronic non-communicable diseases such as hypertension, overweight/obesity, high blood cholesterol, and metabolic syndrome, as well as cardiovascular disorders such as acute myocardial infarction, stroke, and coronary artery disease. Other effects of shift work include disorders such as digestive and mental disorders, diabetes, changes in blood parameters such as cholesterol, glucose, HDL and LDL13,14,15,16,17.
Since shift work is a growing social trend and hypertension is a major risk factor for cardiovascular disease, it is important to demonstrate and evaluate the potential impact of shift work, especially when robust data are lacking18. Researchers have shown different results in the study of the relationship between shift work and blood pressure, so that in some studies it has been shown that shift work can cause an increase in blood pressure in employees18,19.
A study determined that the average fasting blood sugar (FBS), and SGOT liver enzyme in shift workers is higher than day workers. Moreover, the average systolic and diastolic blood pressure in shift workers was higher than day workers20. Also, researchers have reported conflicting information on the relationship between shift work and obesity. Some studies have shown that shift work systems are one of the risk factors of obesity for employees21,22,23, while some studies did not report any significant relationship between shift work and workers' BMI20,24.
Shift work can disrupt the body clock rhythm, sleep, and family and social life. This phenomenon can cause acute effects on worker's mood and performance, which may lead to long-term effects on mental health. Moreover, these may have an impact on both safety and health. In general, it can be said that shift work can change the metabolic reactions by changing the biological rhythm of the body, disturb the sleep pattern of people, affect the function of the digestive system, affect many blood parameters and highlighted as an important risk factor for cardiovascular diseases.
All the above-mentioned show that different studies have reported different findings about the effect of shift work on blood parameters. Most of the studies were cross-sectional and the obtained data were related to a time slice, and in most cases, the situation of exposure to harmful factors in the work environment as an important confounder variable has not been investigated. Therefore, according to the existing research gap in this field, and due to the importance of examining this issue and its extensive effects on the health of the workforce, in this 10-year retrospective cohort study, we aim to investigate the relationship between shift work and blood and metabolic parameters, in order to better understand the potential health impacts of this increasingly prevalent work pattern.
Method
Study design
The present study is a retrospective cohort study and was conducted in a metal parts manufacturing industry in Iran in 2023. The present study was conducted with the aim of investigating the effect of shift work on blood and metabolic parameters in a metal parts manufacturing industry during the 10 years. During the present study baseline data on blood and metabolic parameters were collected from participants using standardized measurement techniques. Additionally, demographic information, occupational exposure history, lifestyle factors, and medical history were obtained.
Sample selection process
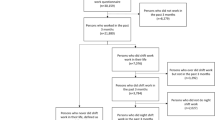
For this purpose, at first, the list of all shift workers was extracted and examined. The term shift work in the present study refers to any working schedule that performed outside the hours of 7:15 am and 4:15 pm. Shift work employees can work in the evening, night, and early morning shifts in the rotating schedules situations. It was found that a total of 498 workers working in operational jobs have been on shift work in the last 10 years. Therefore, the sample size was calculated by the census method of all eligible employees in the studied industry.
After determining the shift workers, the workers who were in the age range of 55 years and older, subjects with underlying diseases and a history of smoking and drug use were also excluded from the study due to the elimination of the effect of confounding variables on the studied parameters. After refining shift workers, 310 workers remained in the list. In the final stage of selecting the study sample, 310 employees with similar jobs who did not have shift work during the last 10 years were also considered as the control group and day workers. Finally, in order to eliminate confounding variables, the case and control groups were matched in terms of background variables such as age, work experience, body mass index, and working hours per day at the baseline period.
In the last phase of selecting the study subjects, according to the dropout rate of the study subjects, the number of 204 shift workers and 204 day workers were examined (NTotal = 408). It should be noted that all subjects were male that employed in operating jobs. The lack of employment of women in jobs with a shift work schedule made it impossible to study women as well.
Inclusion criteria
The inclusion criteria included not having a second job, no underlying disease, no smoking, age below 55 years, no continuous drug use, no exposure to harmful factors in other non-occupational environments, experience of ten years of shift work for the case group and 10 years of day work for the control group, ten years of continuous participation in medical examinations, and also sufficient informed consent to participate in the study. Subjects were able to withdraw from the study at any stage. The participants were assured that the evaluated data would remain anonymous and confidential. The study was conducted according to the principles of the Declaration of Helsinki25. It should be noted that the present study was approved by the ethics committee of Qom University of Medical Sciences (ethics code: IR.MUQ.REC.1402.248).
Demographic parameters
All demographic parameters including age, work history, work experience, job type, body mass index, working hours per day, the state of performing sports activities, and exercise, sleep duration, sleep quality, marital status, and education level were collected by a researcher-made demographic questionnaire. World Health Organization (WHO) defines physical activity as any bodily movement produced by skeletal muscles that requires energy consuming. Popular ways to be active include walking, cycling, sports, etc. In this study, the criterion of physical activity was doing sports activities at least three times a week.
Moreover, considering the effect of sleep quality on other parameters investigated in this study, the standard Pittsburgh Sleep Quality Index (PSQI) was used to determine sleep quality.
Pittsburgh Sleep Quality Index (PSQI)
PSQI is a self-report tool that evaluate sleep quality and disturbances over a 1-month time period. This tool used seven scales that include subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleeping medication, and daytime dysfunction. The rate of each scale is between 0 and 3, and the score of 3 in each scale demonstrates the maximum negative score. The total score of this questionnaire is between 0 and 21, and the score of 6 and above shows low sleep quality. The validity and reliability of this index has been approved in previous studies (Cronbach's alpha: 0.83)26,27.
Examination of blood and metabolic parameters
All the studied blood parameters were collected by reviewing the medical records of all participants during a 10-years period (2013–2022). It should be noted that all the medical tests conducted during the 10-years period were performed by the same Laboratory was approved by Deputy Minister of Medicine, Health and Medical Education of Iran.
The Lab technicians gathered the necessary equipment, including a needle, syringe, and selected tubes for collecting blood. They also cleaned the area where the blood will be drawn with Ethanol 70% as an antiseptic solution.
Blood samples were collected by the standard phlebotomy technique of venipuncture of forearm veins. The Lab technicians collected enough blood to fill the required tubes for testing. Then, the tubes of blood were labeled with the worker's information and transported to the laboratory for analysis. CBC (Count Blood Cells) tests were done by cell counter (made in Japan) and at most 30 min after sampling. Biochemical tests were performed in the laboratory by using special kits approved by the Ministry of Health and BT 3000 Italian auto-analyzer.
In order to measure blood pressure, the participants first rested for 5 min. Then after five minutes of rest, blood pressure was measured on the left arm three times in intervals of one minute. The average of three measurements was recorded as systolic and diastolic blood pressure values. Before measuring the blood pressure, it was ensured that the participants had not eaten or drunk anything for 30 min and had emptied their bladder. Subjects were not allowed to talk during blood pressure measurement. Blood pressure values were measured by Paramed Blood Pressure Monitor, Model B22 (Paramed Company, Canada). The blood parameters examined in the present study are listed in Table 1.
Examination of harmful agents in the work environment
In this study, considering the importance of occupational exposure to harmful agents in the work environment on the blood and metabolic parameters and in order to ensure that it does not affect the studied variables and eliminate its confounding effect, the amounts of harmful agents in the work environment in the three main categories of physical, chemical, and ergonomics harmful agents were investigated. Due to the absence of biological factors in the studied industry, due to the nature of the work, this harmful factor was not investigated. It should be noted that in order to evaluate the effects of these factors, the measurement reports of the 10-years study (2013–2022) were used and controlled. In order to reduce the amount of error caused by measurement and analysis devices, it was ensured that all measurements were carried out by the same qualified company during these 10 years.
Physical harmful agents
This component included six parameters of noise, vibration, radiation, lighting, electromagnetic field and thermal stress in the work environment.
In order to measure the occupational noise and sound pressure level (SPL) in decibels in all workstations, a KIMO-DB300 sound analyzer model was applied in accordance with the ISO 961228 standard. Before the measurement, the sound meter was calibrated using TENMARS-TM100 calibrator. All measurements were performed in the A frequency weighing network and Slow speed mode.
Due to the lack of obtaining the necessary standards for measuring the whole-body and hand-arm vibration, in this study, occupational exposure to vibration was determined qualitatively and using a question with a three-mode answer in the questionnaire with the options, including: "I do not experience any vibration during work shifts", "I have occupational exposure to vibration during work shifts (at least once a week and or more)" and "I have occupational exposure to vibrating devices continuously and every day during the work shift" were measured.
The intensity of public lighting was measured using a regular grid method with calibrated HAGNER Screen Master illuminance meter.
During the current study, Wet Bulb Globe Temperature (WBGT) was determined at different hours based on the ISO7243 standard29. Due to the homogeneity of temperature conditions at different heights, the measurement was carried out in the waist area of people. In each measurement phase, the device was fixed in its place for 30 min to be at the same temperature as the environment.
Finally, the amount of non-ionizing radiation was measured using a HAGNER UV, and IR meter. The measurement of ionizing radiation was also done by installing film badge on the chest area of people and then analyzing them. Electromagnetic fields were also measured using Tenmars TM-192 Triaxial Magnetic Field Meter by relevant instructions.
Chemical harmful agents
This component included the assessment of occupational exposure to volatile organic compounds (VOCs), fumes, oil mists and dust.
Sampling of occupational exposure to benzene, toluene, ethyl benzene and xylene (BTEX) compounds was also carried out using NIOSH 1501 method30 and activated charcoal tubes installed in worker's breathing area and individual sampling pump. After sampling, the samples were brought to the laboratory on ice and analyzed by gas chromatography (GC).
Inhalable particles concentration, fume concentration, and oil mist were also measured using the NIOSH 060031, NIOSH 730032, and NIOSH 502633 standard methods, respectively.
Ergonomics harmful agents
This component included the assessment of the prevalence of work-related musculoskeletal disorders (WRMSDs) using the Cornell Musculoskeletal Disorders Questionnaire (CMDQ), as well as the risk level of occupational postures using the REBA (Rapid Entire Body Assessment) and RULA (Rapid Upper Limb Assessment) method34.
The measurement of harmful factors was done according to the latest version of TLVs and BEIs Based on the Documentation of the Threshold Limit Values for Chemical Substances and Physical Agents and Biological Exposure Indices reported by American Conference of Governmental Industrial Hygienists (ACGIH)35 and NIOSH Manual of Analytical Methods (NMAM)36. The schematic of the study implementation process is presented in Fig. 1.

The schematic of the study implementation process.
Assessing accuracy and reliability of data collected
In the present study, to ensure the validity and reliability of data different tools such as standardized data collection protocols (for maintain consistency and reduce measurement variability), quality control measures (implementation of quality control measures, such as regular data audits, cross-check, double data entry, and validation checks), data validation (validating collected data against external sources, such as medical records or lab reports), and regular training and calibration (providing training to study personnel, calibrating measurement tools, and conducting periodic refresher sessions) were applied in different stages of data collection.
Data analysis
Finally, all the collected data were analyzed using IBM SPSS version 25.0 software (SPSS Inc Chicago, Illinois). Descriptive statistics were reported using mean, standard deviation and frequency indicators. Non-parametric Kolmogorov–Smirnov test was used to check data distribution. The normality test findings demonstrated that the data distribution was normal in all cases (p-value > 0.05). Adjustments were made for potential confounding variables. To analyze the data, Independent-Samples T-Test, Chi-square (χ2), and Repeated Measure Analysis of Variance were applied. Leven test was employed to assess the equality of variances. To assess the homogeneity of variances in the studied variables and validate a repeated measures analysis of variance the Mauchly's sphericity test was applied. Logistic regression analysis was applied to study the relationship between shift work and different blood and metabolic parameters. The final regression model was obtained by the backward elimination method. The Nagelkerke and Cox & Snell R-square were applied to measure the predictive performance. Model calibration was evaluated by the Hosmer–Lemeshow goodness-of-fit test. A significance level of 0.05 was considered for all tests (p-value < 0.05).
Results
Demographic parameters values
The mean age, work experience and working hours per day between shift workers and day workers group were 40.27 ± 8.34–40.96 ± 7.87 years, 11.30 ± 5.56–10.98 ± 6.31 years, and 9.14 ± 2.62–9.02 ± 2.40 h, respectively. The average value of BMI between the case and, control groups were 25.94 ± 4.36, and 23.91 ± 5.13 kg m−2, respectively.
It was found that there is no significant relationship between the values of the studied demographic parameters, except for the quality and quantity of sleep, as well as sports and physical activity between the shift and day workers' groups. The results revealed that the mean sleep duration in the shift workers, and day workers group was 5.84 ± 1.63, and 6.56 ± 3.39 h, respectively. Also, the day workers group experienced better sleep quality compared to the shift workers. The amount of physical activities among the day workers group was much higher than the shift workers group. Other values related to demographic information are presented in Table 2.
Workplace harmful agents' values
In this study, exposure to harmful physical, chemical and ergonomic factors in the work environment was also controlled among the two study groups.
The physical harmful factors of the work environment included parameters of noise, vibration, lighting, thermal stresses, ionizing and non-ionizing rays, and electromagnetic fields. The results showed that the exposure to physical harmful factors was within the occupational exposure limits in all parameters, except for the lighting, which was below the recommended permissible limit in all stations according to the nature of the work (250–300 lx). It was also found that there is no significant difference between the amounts of exposure to physical harmful factors between the two studied groups (p-value > 0.05).
The harmful chemical factors of the work environment included exposure to volatile organic compounds (benzene, toluene, ethylbenzene, and xylene), welding fumes (manganese, cobalt, chromium, nickel, and iron oxide), oil mist, and particles. The results showed that the situation of exposure to harmful chemical agents in all parameters is within the permissible range. It was also found that there is no significant difference between the amounts of exposure to harmful chemical agents between the two studied groups (p-value > 0.05).
Finally, the results of the evaluation of the ergonomic status of the subjects showed that the prevalence of musculoskeletal disorders among the shift workers, and day workers group was 45.4% and 41.3%, respectively. It was also found that 25% and 24% of subjects in shift work, and day work schedule were at high ergonomic risk level, respectively. No significant difference was found between the ergonomic risk factors values between the two studied groups (p-value > 0.05). Other results related to the monitoring of the study subjects' exposure to harmful factors in the work environment are presented in Table 3.
Blood parameters values
The values of each of the blood and metabolic parameters were analyzed in two sections, the average in 2022 and the 10-years average. The results revealed that there was no significant relationship between the BMI values in 2022, but a significant relationship was found between the 10-year values, so that the average BMI was higher among the shift work group (p-value < 0.05).
There was no significant difference between the WBC, and RBC values between the two groups (p-value > 0.05). The 10-year average values of WBC and RBC in the shift work group were 7.13 ± 2.96 103/µL, and 5.36 ± 1.21 106/µL, respectively, and the 10-year average values of WBC, and RBC in the day work group were also determined as 7.16 ± 3.21 103/µL, and 5.15 ± 1.73 106/µL, respectively. The results showed that there is significant difference between the average blood platelets between the two groups examined in 2022 (p-value < 0.05), but in the 10-years study, significant difference was not observed between the two groups (p-value > 0.05).
It was found that there was a significant difference between the 10-year average values of thyroid stimulating hormones (TSH) in the two groups under investigation (p-value < 0.05), and the values of this parameter between the shift workers and day worker's groups were 4.36 ± 1.84, and 3.18 ± 1.77 MicIU/ml, respectively. The findings revealed that there was a significant difference between the average values of fasting blood sugar (FBS) in the two studied groups (p-value < 0.05), and the 10-year average values of this parameter between the groups of shift workers and day workers were 94.56 ± 13.29, and 85.13 ± 9.65 mg/dL, respectively. The findings showed that there is a significant relationship between the average values of creatinine in the two studied groups (p-value < 0.05).
It was found that there is no significant relationship between the average cholesterol values between the two studied groups (p-value > 0.05), however, the 10-year average cholesterol values between the shift work and day work groups were 168 ± 28, and 173 ± 29 mg/dL, respectively. Unlike cholesterol, there was a significant difference between the 10-year average values of triglycerides between the two groups (p-value < 0.05). Triglyceride values were 184 ± 19, and 177 ± 11 mg/dL between shift work and day work groups, respectively. Among the liver enzymes, the 10-year average values of SGPT in the shift work and day work groups were 31 ± 9, and 27 ± 5 IU/L, respectively, and a significant difference was observed between the mentioned values in the two groups (p-value < 0.05).
The examination of blood pressure values, including systolic and diastolic blood pressure parameters, revealed that there was no significant difference between the 10-year average values of the mentioned parameters between the two groups (p-value > 0.05), however, the systolic blood pressure (SBP) values between the shift work and day work groups were 121 ± 10, and 120 ± 8 mmHg, respectively, and the value SBP was higher in shift work group compared to day work group. Other information related to the values of blood and metabolic parameters between the two studied groups is presented in Table 4.
The trend of changes in blood and metabolic parameters
The results of evaluating the changes in blood parameters between the shift work and day work groups showed that in the shift work group, the values of changes in BMI, WBC, PLT, TSH, FBS, Cr., TG. SGPT, SGOT, and SBP parameters have significant differences (p-value < 0.05). Moreover, in the day work group the values of changes in BMI, SGOT, and SGPT parameters have significant differences groups (p-value < 0.05) (Table 5).
The effect of shift work on the blood and metabolic parameters and demographic variables
The results of the evaluation of the effect of shift work on the investigated parameters using logistic regression showed the highest effect of shift work was observed on the parameters of FBS, TG, SGPT, TSH, Physical activity, BMI, Sleep duration, PLT, and Sleep quality with beta coefficient values of 0.49, 0.33, 0.29, 0.29, 0.20, 0.18, 0.14, 0.13 and, 0.11, respectively (p-value < 0.01) (Table 6).
Discussion
The theme of this retrospective cohort study is to exhibit the association between shift work and blood parameters. Investigating the relationship between the study groups concerning the demographic features showed that regular physical activities and quality of sleep in the control group was significantly higher than those who were shift workers. Since shift workers suffer from sleep deprivation, they have to make up for their lack of sleep during daytime, which will ultimately lead to poor quality of sleep37. In fact, the insufficient sleep and poor sleep quality among shift workers can be attributed to circadian rhythm disruption and physiological disorders38. Previous researches have suggested that shift work has an adverse effect on sleep quality, which is consistent with the findings of the present study39,40.
Sedentary behaviors are recognized as the underlying mechanism among the shift workers in causing adverse health effects41. Our results are aligned with findings obtained by Loef et al. and Vandelanottet et al., which demonstrated that less physical activity is observed more among shift workers in comparison with day workers42,43. Such result is due to the time constraint to carry out physical activity. Moreover, regarding the life style of shift workers, the odds of not performing physical activity was higher than the other variables such as sleep duration and sleep quality. There is strong evidence regarding the relationship between sleep deprivation and desynchronization of circadian rhythm with increased risk of health problems including cardiovascular disease (CVD), depression of the immune system, hormonal changes and metabolic disturbances and type II diabetes44,45.
Some epidemiological studies have investigated the relationship between hematological parameters and work shift. It was reported that increased WBC count and hematocrit among shift workers46,47,48. On the contrary, the present study results indicated that there is no significant difference between the number of WBCs between the studied groups. In addition, there was no significant difference in the higher average of RBC and PLT among shift employment compared to the control group. Similar results were observed in a study conducted among healthcare workers11. In order to better understand the relationship between shift work and metabolic risk factors, we considered BMI, cholesterol, triglyceride and fasting blood sugar (FBS) parameters. As to the literature, a debate exists between two perspectives concerning how shift work impacts the metabolic syndrome and its components (obesity, hyperglycemia, dyslipidemia, low HDL cholesterol and hypertension). Some hold the opinion that there is a favorable connection between shift work and metabolic syndrome (MetS)49 while others are against this viewpoint when confounding variables are included50.
In accordance with the results of previous studies51,52, no meaningful relationship between shift work and total cholesterol was found in the current research. On the other hand, while the study conducted by Loef et al.51 did not determine a clear connection between shift work and triglyceride, our findings contradict this claim. Discrepancies between the results could be probably related to the difference in the study population, the control of confounding variables and the quality of the study. Two recent systematic reviews53,54 have inferred a positive association between shift work and increased risk of type 2 diabetes, which is in line with our findings. A possible explanation for this could be that the shift workers have a disturbance in the chronobiological rhythms due to exposure to light during night shifts as well as interference in food absorption and subsequently disruption in rhythm of glucose metabolism53.
Also, the logistic regression results discovered that the greatest effect of shift work on blood parameters is associated with the increased odds of glucose level. Similar to what other papers concluded55,56, we observed a higher odds of BMI in shift workers compared to comparison group. This is probably due to excessive consumption of food that is high in sugar and fat, which can result in accumulation of subcutaneous fat and weight gain57.
Furthermore, the 10-year average change in BMI value of shift workers showed a significant upward trend. However, some studies have shown that shift workers are more likely to develop high blood pressure due to the effect of shift work on melatonin secretion15,58, our findings do not support such claim. This may be due to differences in study type, sample size, demographic characteristics and measurement methods. Review of published articles about the effect of employee work schedules on liver dysfunction indicates that workers who engaged in shift work are at a higher risk of liver abnormalities59,60.
Khosravipour et al., and Wang et al., conducted surveys which demonstrated that shift workers are prone to developing abnormal level of liver enzymes61,62. According to these findings, we claim that there is a greater odd of elevated SGPT and SGOT among shift workers than day time workers which can be attributed to circadian misalignment, as well as the lifestyle and nutritional habits of the subjects. Moreover, examining the trend of changes in blood parameters during the last ten years in this study significantly confirms the increase in the levels of liver enzymes in shift workers.
A systematic review by Leso et al., examined the effect of shift work on the thyroid function. It suggested that most studies reported high serum levels of TSH among shift workers. Dysfunction of the thyroid due to interruption in the circadian rhyme of TSH can occur for reasons such as changes in the time and quality of sleep63. In this regard, our results are compatible with findings obtained by Moon et al.,64 regarding the increased risk of thyroid imbalance among shift workers. Exposure to the hazards of workplace and work shift may have an adverse effect on blood parameters65,66. Hence, harmful agents including chemical, physical and ergonomic factors were evaluated among the studied groups, and the results exhibited that both shift and non-shift groups are equally exposed to workplace hazard.
The results of our 10-year retrospective cohort study provide robust evidence for the association between shift work schedules and adverse changes in blood parameters. These findings are consistent with previous research, but our study adds to the literature by providing longitudinal data over a 10-years period with controlling the occupational exposer to physical, chemical and ergonomics risk factors in the workplace. The mechanisms underlying the association between shift work and adverse changes in blood parameters are not fully understood, but several hypotheses have been proposed.
One possibility is that disruption of the circadian rhythm, which controls many physiological processes, may contribute to metabolic dysregulation. Another possibility is that shift work may lead to unhealthy behaviors, such as poor diet and inadequate exercise, which could contribute to adverse changes in blood parameters. Our findings have important implications for healthcare professionals and policy makers. Healthcare professionals should be aware of the potential health risks associated with shift work and should consider screening workers for metabolic abnormalities. Policy makers should consider implementing interventions to mitigate the negative health effects of shift work, such as providing healthier food options and promoting physical activity during work hours. Overall, our study highlights the need for further research on the relationship between shift work and health outcomes, as well as the need for interventions to protect the health of shift workers.
Strengths and limitations
A major strength of the current study is the use of longitudinal data, which made it possible to examine the 10-year trend changes of blood parameters in shift workers. Furthermore, harmful agents were evaluated as confounding factors that could affect our findings. Despite some strengths of this research, we also faced several limitations. First, considering that the studied samples were male, therefore, the results cannot be generalized to the whole community. Moreover, the impact of gender variations on blood parameters in shift workers could not be evaluated. Second, different types of shift work schedules were not included in this study. The role of chorotype and diet pattern were not studied during shift work as well which, may result in bias in our conclusions. Further research is needed to provide deep insights to causal relationship between shift work and blood parameters. It is also suggested to conduct objective investigations regarding the measurement of melatonin as a biomarker of circadian disorder to deduce explicit conclusions.
Conclusion
In conclusion, the present retrospective cohort study contributes to a growing body of evidence that platelet count, level of SGPT and TSH as well as metabolic factors including BMI, triglyceride levels and fasting glucose are likely to be influenced shift work. It is noteworthy that controlling of occupational exposure confounding factors in our study has led to a clearer relationship between shift work and blood parameters. On the basis of our findings, life style behaviors including poor sleep quality and physical inactivity are underlying contributors to the development of a heightened chance for blood parameter changes in shift workers when compared with fix daytime employees. The outcome of this study can be used by the occupational health practitioners to intervene in the lifestyle of shift workers by positively modifying certain behaviors. These interventions such as exercising regularly as well as having a healthy diet prevents long term chronic diseases among shift workers. These findings have important implications for healthcare professionals and policy makers, highlighting the need for interventions to mitigate the negative health effects of shift work on workers. Moreover, further research is warranted to delve deeper into the mechanisms underlying these relationships and to develop strategies aimed at promoting metabolic health and reducing the health risks associated with non-standard work schedules.
Data availability
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
References
Costa, G. Shift work and health: Current problems and preventive actions. Saf. Health Work 1, 112–123 (2010).
Ganesan, S. et al. Sleep, alertness and performance across a first and a second night shift in mining haul truck drivers. Chronobiol. Int. 39, 769–780 (2022).
Härmä, M., Ojajärvi, A., Koskinen, A., Lie, J.-A. & Hansen, J. Shift work with and without night shifts and breast cancer risk in a cohort study from Finland. Occup. Environ. Med. 80, 1–6 (2023).
Ha, M. & Park, J. Shiftwork and metabolic risk factors of cardiovascular disease. J. Occup. Health 47, 89–95 (2005).
Rajaratnam, S. M., Howard, M. E. & Grunstein, R. R. Sleep loss and circadian disruption in shift work: Health burden and management. Med. J. Aust. 199, S11–S15 (2013).
Buja, A. et al. Strain and health implications of nurses’ shift work. Int. J. Occup. Med. Environ. Health 26, 511–521 (2013).
Di Lorenzo, L. et al. Effect of shift work on body mass index: Results of a study performed in 319 glucose-tolerant men working in a Southern Italian industry. Int. J. Obes. 27, 1353–1358 (2003).
Ansu Baidoo, V. & Knutson, K. L. Associations between circadian disruption and cardiometabolic disease risk: A review. Obesity 31, 615–624 (2023).
Gohari, A., Wiebe, D. & Ayas, N. Shift working and cardiovascular health. Chronobiol. Int. 40, 27–32 (2023).
Cheng, H., Liu, G., Yang, J., Wang, Q. & Yang, H. Shift work disorder, mental health and burnout among nurses: A cross-sectional study. Nurs. Open 10, 2611–2620 (2023).
Sooriyaarachchi, P., Jayawardena, R., Pavey, T. & King, N. A. The effect of shift work on different hematological parameters among healthcare workers. Chronobiol. Int. 40, 918–925 (2023).
Sookoian, S. et al. Effects of rotating shift work on biomarkers of metabolic syndrome and inflammation. J. Intern. Med. 261, 285–292 (2007).
Karlsson, B., Knutsson, A. & Lindahl, B. Is there an association between shift work and having a metabolic syndrome? Results from a population based study of 27 485 people. Occup. Environ. Med. 58, 747–752 (2001).
Gamboa Madeira, S., Fernandes, C., Paiva, T., Santos Moreira, C. & Caldeira, D. Does shift work affect blood pressure values and hypertension risk? A systematic review and meta-analysis. Eur. J. Prev. Cardiol. 28, zwab061-311 (2021).
Khosravipour, M. et al. The association between rotating night shift work and hypertension: A cross-sectional study among male workers. Eur. J. Prev. Cardiol. 28, E41–E44 (2021).
Gamboa Madeira, S., Fernandes, C., Paiva, T., Santos Moreira, C. & Caldeira, D. The impact of different types of shift work on blood pressure and hypertension: A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 18, 6738 (2021).
Bahinipati, J., Sarangi, R., Pathak, M. & Mohapatra, S. Effect of night shift on development of metabolic syndrome among health care workers. J. Fam. Med. Primary Care 11, 1710 (2022).
Shah, A. et al. Is shift work sleep disorder a risk factor for metabolic syndrome and its components? A systematic review of cross-sectional studies. Metab. Syndr. Relat. Disord. 20, 1–10 (2022).
Sooriyaarachchi, P., Jayawardena, R., Pavey, T. & King, N. A. Shift work and the risk for metabolic syndrome among healthcare workers: A systematic review and meta-analysis. Obes. Rev. 23, e13489 (2022).
Harati, A., Shahtaheri, S. J., Harati, B. & Honarjoy, A. Investigation of relation between shift work and biomarkers of metabolic syndrome of workers, a case study at a petrochemical industry. Iran Occup. Health J. 15, 66–76 (2018).
Antunes, L. D. C., Levandovski, R., Dantas, G., Caumo, W. & Hidalgo, M. Obesity and shift work: Chronobiological aspects. Nutr. Res. Rev. 23, 155–168 (2010).
Morikawa, Y. et al. Effect of shift work on body mass index and metabolic parameters. Scand. J. Work Environ. Health 33, 45–50 (2007).
Hulsegge, G. et al. The mediating role of lifestyle in the relationship between shift work, obesity and diabetes. Int. Arch. Occup. Environ. Health 94, 1287–1295 (2021).
Parkes, K. R. Shift work and age as interactive predictors of body mass index among offshore workers. Scand. J. Work Environ. Health 28, 64–71 (2002).
Association, G. A. o. t. W. M. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. J. Am. Coll. Dent. 81, 14–18.
Sadeghi-Yarandi, M., Ghasemi, M., Ghanjal, A., Sepandi, M. & Soltanzadeh, A. The prediction of chronicity in patients with acute and subacute nonspecific low back pain and associated risk factors: A case–control study. Pain Manag. Nurs. 23, 838–847 (2022).
Khosravi, A., Emamian, M. H., Hashemi, H. & Fotouhi, A. Components of Pittsburgh Sleep Quality Index in Iranian adult population: An item response theory model. Sleep Med. X 3, 100038 (2021).
Arezes, P. M., Bernardo, C. & Mateus, O. A. Measurement strategies for occupational noise exposure assessment: A comparison study in different industrial environments. Int. J. Ind. Ergon. 42, 172–177 (2012).
Parsons, K. Heat stress standard ISO 7243 and its global application. Ind. Health 44, 368–379 (2006).
Abouee-Mehrizi, A., Soltanpour, Z., Mohammadian, Y., Sokouti, A. & Barzegar, S. Health risk assessment of exposure to benzene, toluene, ethyl benzene, and xylene in shoe industry-related workplaces. Toxicol. Ind. Health 40, 33–40 (2024).
NIOSH Manual of Analytical Methods-0600. NIOSH Manual of Analytical Methods (NMAM), Fourth Edition, https://www.cdc.gov/niosh/docs/2003-2154/pdfs/0600.pdf.
NIOSH Manual of Analytical Methods-7300. NIOSH Manual of Analytical Methods (NMAM), Fourth Edition, https://www.cdc.gov/niosh/docs/2003-2154/pdfs/7300.pdf.
NIOSH Manual of Analytical Methods-5026. NIOSH Manual of Analytical Methods (NMAM), Fourth Edition, https://www.cdc.gov/niosh/docs/2003-2154/pdfs/5026.pdf.
Sadeghi Yarandi, M. et al. Effectiveness of three ergonomic risk assessment tools, namely NERPA, RULA, and REBA, for screening musculoskeletal disorders. Arch. Hygiene Sci. 8, 188–201 (2019).
ACGIH. (ACGIH Cincinnati, OH, 2023).
Andrews, R. & O’Connor, P. F. NIOSH manual of analytical methods (NMAM) (2020).
Athar, M. E., Atef-Vahid, M.-K. & Ashouri, A. The influence of shift work on the quality of sleep and executive functions. J. Circad. Rhythms 18, 4 (2020).
Ko, S. B. Night shift work, sleep quality, and obesity. J. Lifestyle Med. 3, 110 (2013).
Lim, Y. C., Hoe, V. C., Darus, A. & Bhoo-Pathy, N. Association between night-shift work, sleep quality and metabolic syndrome. Occup. Environ. Med. 75, 716–723 (2018).
Lin, S. H., Liao, W. C., Chen, M. Y. & Fan, J. Y. The impact of shift work on nurses’ job stress, sleep quality and self-perceived health status. J. Nurs. Manag. 22, 604–612 (2014).
Pepłońska, B. et al. Night shift work and modifiable lifestyle factors. Int. J. Occup. Med. Environ. Health 27, 693–706 (2014).
Vandelanotte, C. et al. How do different occupational factors influence total, occupational, and leisure-time physical activity?. J. Phys. Act. Health 12, 200–207 (2015).
Loef, B. et al. Non-occupational physical activity levels of shift workers compared with non-shift workers. Occup. Environ. Med. 74, 328–335 (2017).
Skogstad, M. et al. Shift work including night work and long working hours in industrial plants increases the risk of atherosclerosis. Int. J. Environ. Res. Public Health 16, 521 (2019).
Lunde, L.-K. et al. Cardiovascular health effects of shift work with long working hours and night shifts: Study protocol for a three-year prospective follow-up study on industrial workers. Int. J. Environ. Res. Public Health 17, 589 (2020).
Chang, W.-P. & Lin, Y.-K. Relationship between rotating shift work and white blood cell count, white blood cell differential count, obesity, and metabolic syndrome of nurses. Chronobiol. Int. 39, 159–168 (2022).
Yen Jean, M. C. et al. Association between lifestyle and hematological parameters: A study of Chinese male steelworkers. J. Clin. Lab. Anal. 33, e22946 (2019).
Lu, L. F. et al. Relationship between shift work and peripheral total and differential leukocyte counts in Chinese steel workers. J. Occup. Health 58, 81–88 (2016).
Yang, X. et al. Association between shift work and risk of metabolic syndrome: A systematic review and meta-analysis. Nutr. Metab. Cardiovasc. Dis. 31, 2792–2799 (2021).
Canuto, R., Garcez, A. S. & Olinto, M. T. Metabolic syndrome and shift work: A systematic review. Sleep Med. Rev. 17, 425–431 (2013).
Loef, B. et al. The association between exposure to different aspects of shift work and metabolic risk factors in health care workers, and the role of chronotype. PLoS ONE 14, e0211557 (2019).
Esquirol, Y. et al. Shift work and cardiovascular risk factors: New knowledge from the past decade. Arch. Cardiovasc. Dis. 104, 636–668 (2011).
Gao, Y. et al. Association between shift work and risk of type 2 diabetes mellitus: A systematic review and dose–response meta-analysis of observational studies. Chronobiol. Int. 37, 29–46 (2020).
Li, W. et al. A meta-analysis of cohort studies including dose-response relationship between shift work and the risk of diabetes mellitus. Eur. J. Epidemiol. 34, 1013–1024 (2019).
Buchvold, H. V., Pallesen, S., Øyane, N. M. & Bjorvatn, B. Associations between night work and BMI, alcohol, smoking, caffeine and exercise: A cross-sectional study. BMC Public Health 15, 1–8 (2015).
Liu, Q. et al. Is shift work associated with a higher risk of overweight or obesity? A systematic review of observational studies with meta-analysis. Int. J. Epidemiol. 47, 1956–1971 (2018).
Samhat, Z., Attieh, R. & Sacre, Y. Relationship between night shift work, eating habits and BMI among nurses in Lebanon. BMC Nurs. 19, 1–6 (2020).
Solymanzadeh, F., Rokhafroz, D., Asadizaker, M. & Dastoorpoor, M. The relationship between rotating shift work and blood pressure among nurses working in hospitals of Abadan, Iran. Chronobiol. Int. 38, 1569–1574 (2021).
Choi, H. et al. Relationship between shift work and liver enzymes: A cross-sectional study based on the Korea National Health and Examination Survey (2007–2015). Ann. Occup. Environ. Med. 31, e15 (2019).
Zhang, S. et al. Rotating night shift work and non-alcoholic fatty liver disease among steelworkers in China: A cross-sectional survey. Occup. Environ. Med. 77, 333–339 (2020).
Khosravipour, M. et al. Independent, modified, and interacting effects of long-term noise, extremely low-frequency electromagnetic fields, and shift work exposures on liver enzymes. Environ. Pollut. 333, 122036 (2023).
Wang, F. et al. Night shift work and abnormal liver function: is non-alcohol fatty liver a necessary mediator?. Occup. Environ. Med. 76, 83–89 (2019).
Leso, V., Vetrani, I., Sicignano, A., Romano, R. & Iavicoli, I. The impact of shift-work and night shift-work on thyroid: A systematic review. Int. J. Environ. Res. Public Health 17, 1527 (2020).
Moon, S.-H., Lee, B.-J., Kim, S.-J. & Kim, H.-C. Relationship between thyroid stimulating hormone and night shift work. Ann. Occup. Environ. Med. 28, 1–5 (2016).
Ismaila, S. O. & Odusote, A. Noise exposure as a factor in the increase of blood pressure of workers in a sack manufacturing industry. Beni-Suef Univ. J. Basic Appl. Sci. 3, 116–121 (2014).
Feriel, J., Tchipeva, D. & Depasse, F. Effects of circadian variation, lifestyle and environment on hematological parameters: A narrative review. Int. J. Lab. Hematol. 43, 917–926 (2021).
Acknowledgements
The authors express their gratitude to all the subjects who participated in this research as well as Qom University of Medical Sciences.
Author information
Authors and Affiliations
Contributions
A.S., M.S.Y. and M.E. conceived this study and designed the related tools. M.M. and M.R. performed data analysis, interpreted the results. M.S.Y. wrote the paper. M.S.Y., N.G.H. and M.B. collected and entered the relevant data, contributed to the interpretation of the results. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Soltanzadeh, A., Eyvazlou, M., Mohammad-ghasemi, M. et al. Investigating the relationship between shift work schedule and blood and metabolic parameters: a 10-years retrospective cohort study. Sci Rep 14, 17297 (2024). https://doi.org/10.1038/s41598-024-68378-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-68378-8
- Springer Nature Limited