
Abstract
Unicystic ameloblastoma (UAM) of the jaw can be effectively reduced in volume through decompression, which promotes bone regeneration and restores jaw symmetry. This study quantitatively evaluated changes in mandible volume and symmetry following decompression of mandibular UAM. This study included 17 patients who underwent surgical decompression followed by second-stage curettage for mandibular UAM. Preoperative and postoperative three-dimensional computed tomography (CT) images were collected. Bone volume and the area of cortical perforation were measured to assess bone growth during decompression. Mandibular volumetric symmetry was analyzed by calculating the volumetric ratio of the two sides of the mandible. Twelve pairs of landmarks were identified on the surface of the lesion regions, and their coordinates were used to calculate the mean asymmetry index (AI) of the mandible. Paired t-tests and the Mann–Whitney U test were used for statistical analysis, with p < 0.05 considered indicative of statistical significance. The mean duration of decompression was 9.41 ± 3.28 months. The mean bone volume increased by 8.07 ± 2.41%, and cortical perforation recovery was 71.97 ± 14.99%. The volumetric symmetry of the mandible improved significantly (p < 0.05), and a statistically significant decrease in AI was observed (p < 0.05). In conclusion, UAM decompression enhances bone growth and symmetry recovery of the mandible. The present evaluation technique is clinically useful for quantitatively assessing mandibular asymmetry.
Similar content being viewed by others


Introduction
Ameloblastoma is a benign but locally infiltrative odontogenic tumor accounting for approximately 9–11% of all odontogenic tumors1,2,3. Its growth can lead to bone destruction and mandibular deformities. Cystic ameloblastoma comprises about 5–22% of all ameloblastoma variants4,5. While invasive surgical treatments, such as bone resection, are commonly considered the treatment of choice, they can result in serious complications, including facial deformities, maxillary bone fractures, and dental losses. There is a general consensus that cystic ameloblastoma can be treated conservatively to avoid jaw resection6,7,8,9.
Both marsupialization and decompression are effective conservative treatments for large unicystic ameloblastomas (UAMs)7,10. These treatments aim to decrease the size of extensive cystic lesions prior to curettage by reducing intracystic pressure, thereby making second-stage surgery less invasive and safer. The main advantages include avoiding pathological fractures and bone resection, reducing intraoperative trauma and bleeding, and preserving adjacent structures such as the mandibular alveolar nerve and teeth1,11. Unlike marsupialization, decompression uses devices to keep the cystic cavity open, which can accelerate lesion reduction through active decompression12,13.
During decompression, primary changes include shrinkage of the lesion and the formation of new bone. The therapeutic effect of decompression is mainly assessed using radiographic imaging, such as CT and panoramic imaging6,14. Virtual measurement is commonly used to calculate the volumes of lesions3,4,14,15. As treatment progresses, new bone forms in the cavity, promoting changes in mandibular symmetry and contour. However, quantitative evaluation of these changes has rarely been reported16. Accurately measuring the post-decompression recovery of mandibular symmetry is challenging due to the irregular cortical defects and complex three-dimensional (3D) contour of the mandible.
In the present study, we developed a quantitative method to evaluate the bony volume and symmetry of the mandible following UAM decompression and to verify its efficacy by assessing postoperative improvement.
Materials and methods
This retrospective study included 17 patients with histologically diagnosed UAMs of the mandible, treated between 2016 and 2023 at the Department of Oral and Maxillofacial Surgery, First Affiliated Hospital, Zhejiang University School of Medicine. The study protocol was approved by the Clinical Research Ethics Committee of the First Affiliated Hospital, Zhejiang University School of Medicine. Informed consent was obtained from patients and/or their legal guardians. This cohort study was conducted in accordance with the ethical standards of the responsible committee on human experimentation and the Declaration of Helsinki.
This study included patients with initial lesions having a major diameter of > 4 cm located in the unilateral posterior mandible or ramus, as confirmed by X-ray or CT, and a pathological diagnosis of UAM. Patients were excluded if they had a recurrent ameloblastoma, acute infection, pathological fracture, or multilocular lesions. The basic information of the patients is presented in Table 1.
Surgical procedure
The treatment protocol involved initial decompression followed by secondary curettage of the UAM.
Under local anesthesia, decompression was performed through intraoral incisions in the region of swelling or alveolar crests. A portion of the overlying bone, mucoperiosteum, and cystic wall was excised to release intracystic pressure, and the specimen was sent for biopsy. A 4-mm-wide silicone tube was inserted into the lesion through the opening to maintain decompression (Fig. 1A). The other end of the tube remained in the oral cavity and was anchored to a bracket on an adjacent tooth using a stainless steel ligature wire (0.1000 Krugg ligature). Patients were instructed to irrigate the lesion cavities twice a day through the tube with normal saline using 20-mL syringes.

Decompression was maintained using a silicone tube. (A) Intraoral view. The decompression tube was fixed to the bracket on an adjacent tooth using a stainless steel ligature wire. (B) CT view. The decompression tube was inserted into the deep side of the lesion cavity through the opening.
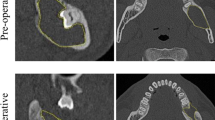
After the decompression surgery, patients were instructed to present for monthly follow-up visits. During these visits, the surgeon checked the patency of the tube and assessed the tumor size. Once the tumor had reduced in size and excess drainage was observed, the tube was replaced with a shorter one if necessary. A 64-slice CT of the mandible was performed every 3 months (Fig. 1B). Decompression continued until sufficient bone had formed in the cavity, as evidenced by new bone overlying the inferior alveolar nerve and sufficient bony thickness to prevent pathological fractures (i.e., at least 1.5 cm from the bottom of the mandible).
Second-stage curettage of the remnant tumor was performed under general anesthesia. Any impacted teeth involved in the lesion were also extracted. Additionally, approximately 0.3–0.5 cm of bone surrounding the tumor was removed to reduce the recurrence rate.
After the second-stage curettage, follow-up was performed every 3 months in the first year, every 6 months in the second year, and annually thereafter.
Outcome evaluation
CT data (CT 64 Slice; Philips Medical Systems, Best, the Netherlands) were collected before and after decompression. The scanning parameters were as follows: 0.75 mm slice thickness, 100 mAs, 120 kVp, and a 512 × 512 image matrix size. CT images were stored in Digital Imaging and Communications in Medicine format and subsequently imported into Mimics 13.1 (Materialise NV, Leuven, Belgium) to construct virtual 3D models of the tumors, impacted teeth, and mandibles (Fig. 2). The 3D models were rendered by summing each CT slice and then exported in STL format. The STL files were imported into 3-Matic (Materialise NV) for quantitative analysis. The volume (mL) of the tumor or mandible was measured automatically by the software.

Reconstruction of a 3D model of the mandible, impacted tooth, and lesion. (A) Coronal CT images of the mandible (purple), lesion (yellow), and impacted tooth (green) were selected. (B) A 3D image of the mandible showed severe swelling and resorption of the mandibular ramus and body, with a large defect in the cortical layer.
Bony volume measurement
The bony volumes of mandibles were measured excluding the tumors and impacted teeth. Postoperative change in bone volume (mL) was calculated as final bone volume − initial bone volume. Postoperative relative change in bone volume (mL) was calculated as (final bone volume − initial bone volume) × 100%/initial bone volume.
Area of cortical perforation
The region of cortical perforation was marked and projected to the lesion surface (Fig. 3).

Measurements of the area of cortical perforation in a representative case. (A) Alignment of the mandible and lesion. (B) Markings of the cortical layer, including the perforation. (C) The cortical perforation was projected to the lesion surface for measurement.
Subsequently, the area of cortical perforation (cm2) was calculated as the initial area of cortical defect − the final area of cortical defect.
Furthermore, the relative reduction in the area of the cortical perforation (cm2) was calculated as the (initial area of cortical perforation − final area of cortical perforation) × 100%/initial area of cortical perforation.
Volumetric analysis
The reconstructed mandible model was divided into two hemi-mandibles along the facial sagittal plane: lesion and healthy area. Each part was assessed for average volumetric discrepancy. Volumetric symmetry was calculated as the lesion health volumetric ratio, indicating the degree of similarity between the two parts:
Landmark-based mandibular symmetry analysis
Prior to analysis, a standard symmetrical mandible was constructed by mirroring the healthy part of the mandible and the lesion part. The median sagittal plane was considered the reference plane.
A 3D coordinate system was constructed based on the standard symmetrical mandible using Geomagic Studio (version 14.0; Geomagic, Morrisville, NC, USA) (Fig. 4A). The median sagittal plane was designated the YZ plane. The x-axis was defined as the line connecting bilateral gonions. The origin of coordinates (0, 0, 0) was the intersection between the x-axis and the YZ plane. The y-axis was drawn in the YZ plane, extending from the common origin toward the condylions. The z-axis included the common origin and was perpendicular to the XY plane. The pre- and postoperative CT models were superimposed onto the standard symmetrical mandible by aligning the nonsurgical parts (Fig. 4B).

Identification of landmarks for AI analysis. (A) Fabrication of the 3D coordinate system. (B) Alignment of the pre- and post-decompression mandible and the standard symmetrical mandible. (C) The preoperative mandible was remeshed. (D) The measurement landmarks were marked using nodes on the remeshed model. (E) Lines passing through the landmarks perpendicular to the YZ plane were marked. (F) Corresponding positions of landmarks on real mandibles.
The preoperative mandible was remeshed (Fig. 4C). Twelve landmarks were designated using the nodes on the remeshed model, ensuring a uniform distribution of landmarks on the lesion area (Fig. 4D). Their corresponding positions on different mandibular models were identified by extending a line perpendicular to the YZ plane and intersecting the surface of the aligned mandibles (Fig. 4E). Similarly, the contralateral positions of the landmarks were determined by the intersections of the perpendicular lines and the bone surface on the healthy part (Fig. 4F). Therefore, 10 pairs of landmarks were generated, with each pair ideally distributed symmetrically.
The X, Y, and Z coordinates of the landmarks were recorded. Similar to Huang et al.17, the asymmetry index (AI) was calculated as follows: \(\sqrt{{\left(Xl+Xr\right)}^{2}+{\left(Yl-Yr\right)}^{2}+{\left(Zl-Zr\right)}^{2}}\), where X, Y, and Z are the coordinates of a landmark, l indicates the left side, and r indicates the right side. A pair of perfectly symmetrical landmarks would have an AI of 0. Lower AI values indicate higher degrees of symmetry. The average AI for the landmarks was calculated at different time points.
Two examiners independently performed landmark identification and Al measurements following the same protocol. Both examiners were trained to use the software prior to the study.
Statistical analysis
Data are presented as mean ± standard deviation (SD). Statistical analysis was conducted using SPSS software (version 19.0; IBM Corp., Armonk, NY, USA). Paired t-tests were employed when data were normally distributed, whereas the Mann–Whitney U test was used when landmark-based AIs were not normally distributed. P-values < 0.05 were considered indicative of statistical significance.
The inter-examiner agreement of AI measurements was assessed using the intraclass correlation coefficient. Based on the 95% confidence interval (CI) of the estimated intraclass correlation coefficient (ICC), the following classifications were devised: 0.00–0.49 = poor agreement, 0.50–0.74 = moderate agreement, 0.75–0.89 = good agreement, and 0.90–1.00 = excellent agreement.
Results
The mean duration of decompression was 9.53 ± 3.22 (range: 3–15) months. All patients experienced visible growth of new bone and a decrease in tumor size during decompression, leading to improved facial symmetry. The mean follow-up duration after the secondary surgery was 19.34 (range: 14–41) months. Recurrence occurred in one patient at 10 months after curettage, resulting in a recurrence rate of 5.88%. The patient underwent repeat curettage for the recurrent tumor and has remained free of recurrence for 33 months to date.
As presented in Table 2, the lesion volume significantly decreased during decompression (p < 0.05). Conversely, the mandibular volume was significantly increased (p < 0.05), with a relative change in bone volume of 8.07 ± 2.41%. Additionally, the area of cortical perforation decreased significantly (p < 0.05), with a relative reduction of 71.97 ± 14.99%.
The changes in symmetry are summarized in Table 3. The volumetric discrepancy of bilateral mandibular bone volume was 5.77 ± 2.75 mL. Following decompression, this discrepancy decreased significantly to 3.13 ± 2.01 mL (p < 0.05). Initially, the volumetric ratio was 83.96 ± 8.03%. After decompression, the volumetric ratio increased to 98.27 ± 10.98%.
After decompression, a significant reduction in AI was achieved (p < 0.05). The intra-examiner reliability of AI measurements was excellent (0.90–0.99), with an ICC of 0.926 before decompression and 0.938 after decompression.
Discussion
Ameloblastoma predominantly affects young to middle-aged individuals, necessitating minimally invasive methods with low morbidity and long-term disease-free survival18. Marsupialization or decompression has been employed for this purpose, as these techniques are associated with a reduced risk of damaging bone structures. Therefore, quantitative analysis of bone remodeling using these procedures may facilitate treatment planning and provide evidence-based recommendations for managing cystic ameloblastomas. In the present retrospective study, we analyzed the effects of decompression on bony changes, revealing that decompression significantly stimulates bone growth and improves mandibular symmetry.
As decompression progresses, fundamental changes include shrinkage of lesions and the growth of new bone. The amount of newly formed bone in the cavity directly influences the risk of injuries necessitating secondary surgeries, such as pathological fractures and nerve injuries. Second-stage curettage can only be safely performed when sufficient bone has formed. Demirsoy et al.19 and Zhao et al.20 used grayscale values of panoramic images to visualize new bone formation. However, such measurements of bone volume were indirect, making it difficult to precisely assess the volume of new bone. In the present study, discrepancies between two mandibular volumes were used to estimate the volume of newly grown bone. The results showed that bone volume continuously increased throughout the decompression procedure. These changes contributed to the recovery of mechanical strength in the lesion area.
Cortical perforation is an important radiological feature in the management of ameloblastoma18,21. Lesions associated with cortical perforation may indicate a potential risk of postoperative recurrence22. One possible reason for this is that the barrier function of the cortical bone with respect to the lesion disappears once the cortical layer is damaged, allowing the ameloblastoma to adhere to the periosteum. The recovery of cortical perforation confines the boundary of the tumor, ensuring that secondary curettage of the residual tumor is precise and clear. However, precise measurement of cortical perforation is rarely reported because of difficulties in accurately identifying the complex contours of defects. In this study, the cortical defect area was projected onto the surface of the lesion, simplifying the measurement process.
Several different methods exist for measuring facial asymmetry, but a standard method has not yet been established23,24. Volume discrepancy has been shown to be a sensitive method for assessing mandibular asymmetry25,26. In this study, volume discrepancy significantly decreased during decompression, indicating a reduction in bony differences between the healthy and affected halves of the mandible. Additionally, the volumetric ratio between the two sides of the mandible was calculated. Interestingly, the ideal volumetric ratio was expected to be 100% in a perfectly symmetrical mandible, but this value was exceeded after decompression in this study. Thus, we believe that volume-based analysis primarily reflects the similarity of the bilateral bone amount but may not fully represent the symmetry of the mandibular contour.
The AI is another measure of the extent of symmetry in both bones and soft tissues24. Unlike volume analysis, the AI directly reflects the degree of symmetry of the mandibular contour. Common methods often rely on the Euclidean distance matrix analysis of anatomical landmarks that influence the facial outline. For example, Cao et al.27 used landmark-based scoring analysis to evaluate chin asymmetry. Similar methods were also employed in our previous studies to quantitatively assess changes in zygomatic symmetry after surgeries28. In this study, ameloblastomas occurred in different sites of the mandible, making it difficult to find suitable anatomical landmarks in all cases. To reduce bias, the lesion area was remeshed, and 12 nodes were uniformly distributed to identify landmarks. The mandible and lesion models were merged to facilitate application of the AI to the cortical defect region. The results showed that the degree of symmetry of the mandibular surface in the lesion area increased after decompression. ICC analysis demonstrated high reproducibility of this technique.
Decompression of ameloblastoma entails several risks. First, it has a higher recurrence rate compared to radical treatment27,29,30. However, secondary surgery in cases of recurrent cystic ameloblastoma has proven effective30. Nevertheless, the recurrence rate should not be the sole consideration given the benign nature of ameloblastoma. Radical surgery can result in facial deformity and dysfunction, negatively impacting facial growth, which should also be considered before treatment31. Second, accelerated growth of the solid component of ameloblastoma may unpredictably occur after long-term decompression or marsupialization. Yang et al.32 described five cases of such occurrences during marsupialization ultimately requiring wide resections. Therefore, it is crucial to closely monitor changes in lesions and bones during decompression, as well as consider the need for radical treatment if the tumor becomes enlarged.
The major limitation of this study was its retrospective nature, such that selection bias could not be avoided. Additionally, this study had a small sample size. Considering that our findings provide only preliminary evidence, further prospective trials using larger samples are needed.
This study describes 3D quantitative analysis for evaluating mandibular volume and symmetry, offering significant practical value for clinical use. The combination of volumetric analysis and landmark-based AI calculation facilitates the quantification of symmetry in cases with complex anatomy. In the future, this technique can be further utilized in research and enhanced through the integration of artificial intelligence. In conclusion, decompression for UAM can significantly benefit bone recovery and improve mandibular symmetry. Special attention should be paid to effectiveness and recurrence throughout the entire decompression process and postoperative follow-up.
Data availability
The data used and/or analyzed during this study are available from the corresponding author on reasonable request.
References
Vallicioni, J. et al. Ameloblastomas. Ann. Otolaryngol. Chir Cervicofac. 124, 166–171 (2007).
Kokubun, K. et al. Frequency of odontogenic tumors: A single center study of 1089 cases in japan and literature review. Head Neck Pathol. 16, 494–502 (2022).
Oginni, F. O. et al. A prospective epidemiological study on odontogenic tumours in a black African population, with emphasis on the relative frequency of ameloblastoma. Int. J. Oral Maxillofac. Surg. 44, 1099–1105 (2015).
Philipsen, H. P. & Reichart, P. A. Unicystic ameloblastoma. A review of 193 cases from the literature. Oral Oncol. 34, 317–325 (1998).
da Silva, Y. S., Sohal, K. S., Stoelinga, P. J. W. & Grillo, R. A meta-analysis on the presentation of unicystic ameloblastoma in the jaws and the consequences for their treatment. J. Stomatol. Oral Maxillofac. Surg. 123, e433–e438 (2022).
Pogrel, M. A. & Montes, D. M. Is there a role for enucleation in the management of ameloblastoma?. Int. J. Oral Maxillofac. Surg. 38, 807–812 (2009).
Wu, K. et al. Clinical evaluation of fenestration decompression combined with secondary curettage for ameloblastoma of the jaw: Retrospective radiographic analysis. BMC Oral Health 22, 443 (2022).
Leite-Lima, F. et al. A conservative approach for unicystic ameloblastoma: Retrospective clinic-pathologic analysis of 12 cases. J. Oral Pathol. Med. 52, 654–659 (2023).
Datarkar, A., Rai, A., Bhawalkar, A. & Jain, A. Clinical outcome following conservative treatment of 58 mandibular ameloblastoma patients: A retrospective study. Oral Maxillofac. Surg. 27, 601–608 (2023).
Song, I. S., Park, H. S., Seo, B. M., Lee, J. H. & Kim, M. J. Efect of decompression on cystic lesions of the mandible: 3-dimensional volumetric analysis. Br. J. Oral Maxillofac. Surg. 53, 841–848 (2015).
Liang, Y. J., He, W. J., Zheng, P. B. & Liao, G. Q. Inferior alveolar nerve function recovers after decompression of large mandibular cystic lesions. Oral Dis. 21, 674–678 (2015).
Wiscovitch, A. et al. Potential role of active decompression and distraction sugosteogenesis for the management of ameloblastomas: Report of two cases and review of the literature. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 134, e29–e38 (2022).
Silva, V. T., de Campos, W. G., Leone, C., de Abreu, A. F. & Lemos, C. A. Which devices can be used to decompress odontogenic cystic lesions in the oral cavity? A systematic review. Br. J. Oral Maxillofac. Surg. 62, 252–258 (2024).
Riachi, F., Khairallah, C. M., Ghosn, N. & Berberi, A. N. Cyst volume changes measured with a 3D reconstruction after decompression of a mandibular dentigerous cyst with an impacted third molar. Clin. Pract. 9, 1132 (2019).
Wongrattanakarn, S. et al. Factors affecting the reduction rate of odontogenic cysts after decompression based on 3-dimensional volumetric analysis. Imaging Sci. Dent. 53, 313–323 (2023).
Ku, J. K., Han, M., Yongvikul, A., Huh, J. K. & Kim, J. Y. Volumetric analysis of spontaneous bone healing after jaw cyst enucleation. Sci. Rep. 12, 14953 (2022).
Huang, C. S., Liu, X. Q. & Chen, Y. R. Facial asymmetry index in normal young adults. Orthod. Craniofac. Res. 16, 97–104 (2013).
Zheng, C. Y. et al. Marsupialisation for the treatment of unicystic ameloblastoma of the mandible: A long-term follow up of 116 cases. Br. J. Oral Maxillofac. Surg. 57, 655–662 (2019).
Demirsoy, M. S., Erdil, A., Çolak, S., Maden, A. & Tümer, M. K. Evaluation of postoperative changes in the course of mandibular canals impacted by cystic lesions. J. Stomatol. Oral Maxillofac. Surg. 123, 31–36 (2022).
Zhao, Y., Liu, B., Han, Q. B., Wang, S. P. & Wang, Y. N. Changes in bone density and cyst volume after marsupialization of mandibular odontogenic keratocysts (keratocystic odontogenic tumors). J. Oral Maxillofac. Surg. 69, 1361–1366 (2011).
Rosenstein, T. et al. Cystic ameloblastoma—Behavior and treatment of 21 cases. J. Oral Maxillofac. Surg. 59, 1311–1318 (2001).
Titinchi, F. & Brennan, P. A. Unicystic ameloblastoma: Analysis of surgical management and recurrence risk factors. Br. J. Oral Maxillofac. Surg. 60, 337–342 (2022).
Verhoeven, T. et al. Quantification of facial asymmetry: A comparative study of landmark-based and surface-based registrations. J. Craniomaxillofac. Surg. 44, 1131–1136 (2016).
Alqattan, M. et al. Comparison between landmark and surface-based three-dimensional analyses of facial asymmetry in adults. Eur. J. Orthod. 37, 1–12 (2015).
Lin, H. et al. Mandibular asymmetry: A three-dimensional quantification of bilateral condyles. Head Face Med. 9, 42 (2013).
Lin, H. et al. Comprehensive analysis of mandibular residual asymmetry after bilateral sagittal split ramus osteotomy correction of Menton point deviation. PLoS One 11, e0161601 (2016).
Cao, J., Shen, S., Liu, Z., Dai, J. & Wang, X. Evaluation of mandibular symmetry in patients with condylar osteochondroma who underwent intro-oral condylar resection and simultaneous bimaxillary orthognathic surgery. J. Craniofac. Surg. 31, 1390–1394 (2020).
Bao, T. et al. Quantitative evaluation of symmetry after navigation-guided surgical recontouring of zygomatic fibrous dysplasia: A comparative study. Int. J. Oral Maxillofac. Surg. 49, 1640–1647 (2020).
Hong, J. et al. Long-term follow up on recurrence of 305 ameloblastoma cases. Int. J. Oral Maxillofac. Surg. 36, 283–288 (2007).
Laborde, A., Nicot, R., Wojcik, T., Ferri, J. & Raoul, G. Ameloblastoma of the jaws: Management and recurrence rate. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 134, 7–11 (2017).
Huang, I. Y. et al. Surgical management of ameloblastoma in children. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 104, 478–485 (2007).
Yang, Z. et al. Marsupialization of mandibular cystic ameloblastoma: Retrospective study of 7 years. Head Neck 40, 2172–2180 (2018).
Acknowledgements
This work was supported by the Basic Public Welfare Research Project of Zhejiang Province, China (grant no. LGF20H140004).
Funding
This work was supported by the Basic Public Welfare Research Project of Zhejiang Province, China (grant no. LGF20H140004).
Author information
Authors and Affiliations
Contributions
Huiming Wang and Tingwei Bao organized the project. Di Yu, and Jiaqi Zheng collected the data. Wenyuan Zhu and Dong Wei performed data analysis and visualization. Tingwei Bao and Di Yu drafed the manuscript. Huiming Wang led the project and oversaw manuscript preparation. All authors have read and approved the submitted manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Bao, T., Yu, D., Zheng, J. et al. A three-dimensional quantitative assessment on bony growth and symmetrical recovery of mandible after decompression for unicystic ameloblastoma. Sci Rep 14, 15492 (2024). https://doi.org/10.1038/s41598-024-66411-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-66411-4
- Springer Nature Limited