
Abstract
Using a system that incorporates a variety of food items rather than focusing on individual components can aid in assessing the inflammatory effects of a diet on disease outcomes such as chronic kidney disease (CKD). Therefore, we decided to investigate the association between dietary inflammatory index (DII) and the risk of protein–energy wasting (PEW) and sarcopenia in patients with CKD. In this cross-sectional study, 109 patients with CKD were selected from two clinics in Shiraz, Iran. The intake of individuals’ diets was recorded using a validated 168-item food frequency questionnaire. Additionally, Asian Working Group for Sarcopenia (AWGS) guidelines were utilized to evaluate muscles’ strength, mass, and function. Also, four International Society of Renal Nutrition and Metabolism (ISRNM) criteria (body mass index, intake of protein, albumin, and urine creatinine) were used to diagnose PEW. Logistic regression was used to assess the association between DII and sarcopenia as well as PEW. The results showed that the intake of saturated fatty acids, trans fatty acids, niacin, beta-carotene, and vitamin C was significantly different between lower and higher DII groups. In the univariate model, higher odds of sarcopenia was observed by each unit increase in DII (odds ratio (OR) = 1.379, 95% confidence interval (CI): 1.042–1.824) and age (OR = 1.073, 95% CI: 1.017–1.132). Additionally, in the multivariate model, the association between DII and age with odds of sarcopenia remained significant (DII: OR = 1.379, 95% CI: 1.030–1.846 and age: OR = 1.063, 95% CI: 1.007–1.121). The current study suggests the possible role of pro-inflammatory foods in worsening muscle health, specifically sarcopenia, in CKD patients. Future longitudinal studies may reveal the causative nature of these correlations.
Similar content being viewed by others


Introduction
Chronic kidney disease (CKD) is defined as the progressive loss of kidney function leading to irreversible kidney failure1. The global prevalence of CKD in 2022 was estimated to be more than 10%2; however, studies have shown a higher prevalence of CKD among the Iranian population3.
Loss of muscle mass and function, known as sarcopenia, is a frequent finding in CKD, particularly in end-stage renal disease (ESRD)4. Negative protein balance can result from various factors such as anorexia, increased energy expenditure, metabolic acidosis, insulin resistance, hormonal degradation, and inflammation5. Loss of muscle mass, especially skeletal muscle, is associated with lower quality of life, cardiovascular complications, graft loss, and postoperative complications in kidney transplant, higher risk of falls, loss of personal autonomy, hospitalization and death6,7,8. Therefore, sarcopenia is considered a negative prognostic factor in CKD patients and requires prevention and treatment in these patients.
Also, protein–energy wasting (PEW), a state of nutritional and metabolic imbalances, is characterized by the loss of body protein and energy stores, leading to muscle and fat mass loss and cachexia in CKD patients. PEW can be caused by hypermetabolic status, uremic toxins, malnutrition, and inflammation9.
Previous interventions to prevent and treat sarcopenia have focused on increasing protein intake10. However, inflammation is considered one of the underlying mechanisms explaining sarcopenia. Studies have demonstrated that low-grade inflammation may contribute to the development of sarcopenia11,12. For instance, a systematic review and meta-analysis showed that inflammatory cytokines are inversely associated with muscle strength and mass12. CKD progression is known to lead to inflammation and oxidative stress13. Indeed, individuals with CKD typically experience low-grade chronic inflammation14.
Previous studies have shown that various food items such as whole grains, fruits, vegetables, fish, and certain nutrients including vitamins E and C, omega-3, and magnesium have anti-inflammatory properties. Conversely, refined sugars, simple sugars, red meat, and high-fat dairy have been shown to have pro-inflammatory effects15,16. Using a system that incorporates a variety of food items rather than focusing on individual components can aid in assessing the inflammatory effects of a diet on disease outcomes such as CKD.
The dietary inflammatory index (DII) is a literature-based scoring system designed to evaluate the inflammatory potential of a diet by considering both pro- and anti-inflammatory food items17. Previous studies have shown a negative association between DII and various diseases such as colorectal cancer18, prediabetes and insulin resistance19, frailty, and 8-year mortality20, as well as the risk and progression of kidney disease21,22. A meta-analysis study indicated an adverse association between DII and sarcopenia23. However, there is limited evidence regarding the association between DII and sarcopenia in individuals with CKD in the Iranian population. To our knowledge, only one study based on the National Health and Nutrition Examination Survey (NHANES) has shown a positive association between higher DII and sarcopenia in CKD patients24. Giving the different dietary habits between the United States (US) and Iran, our study aimed to investigate the association between DII and the risk of PEW and sarcopenia in patients with CKD.
Methods
Study population
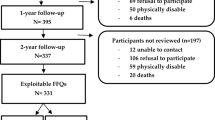
This cross-sectional study was conducted at Motahari and Imam Reza clinics in Shiraz, Fars province, Iran, between January and October 2022. Some books or guidelines suggest using an expected prevalence of 50% if we cannot obtain the prevalence at all25,26,27, and the sample size was calculated based on this assumption. The sample size was calculated as 97 individuals (with (p) = 0.5, d = 0.1, and α = 0.05), and accounting for a 12% drop-out rate, the estimated number of participants was 109 individuals.
The inclusion criteria were age > 18 years, glomerular filtration rate (GFR) less than 60 mL/min/173m2, and the absence of cognitive problems. Conversely, the exclusion criteria were an energy intake of more than 4200 or less than 800 kcal/day and a questionnaire response rate less than 60%. This study was approved by the Medical Research and Ethics Committee of Shiraz University of Medical Sciences (IR.SUMS.SCHEANUT.REC.1402.061) and conducted in accordance with the ethical standards of the Declaration of Helsinki.
Data collection
The percentage of muscle and fat mass was assessed by bioelectrical impedance analysis (BIA). Participants’ weight was measured with a precision of 0.1 kg, and the height and mid-arm circumference (MAC) were determined with an accuracy of 0.5 cm. Also, body mass index (BMI) was calculated. Physical activity was assessed using the International Physical Activity Questionnaire (IPAQ)28. For evaluation of biochemical variables, 5 mL blood samples were collected from each participants.
Sarcopenia and PEW diagnosis
The Asian Working Group for Sarcopenia (AWGS) guidelines were utilized to evaluate muscle strength, mass, and function29,30. Handgrip strength (HGS) was measured using a dynamometer to assess muscle strength. Muscle function was evaluated using gait speed (walking speed in 6 m) and the five-time chair-stand test. Skeletal muscle mass index (SMI) was calculated as skeletal muscle mass divided by the square of height. The criteria for the diagnosis of sarcopenia were as follows: SMI < 7 kg/m2 for men or SMI < 5.7 kg/m2 for women was the first criterion. Additionally, a gait speed of fewer than 1 m/s or more than 12 s in the five-time chair-stand test, and/or an HGS of less than 28 kg for men and 18 kg for women, were used to confirm the diagnosis of sarcopenia29,30.
According to the International Society of Renal Nutrition and Metabolism (ISRNM), four criteria were used to distinguish PEW: BMI < 23 kg/m2, protein intake < 0.6 g/kg/day, biochemical parameters such as albumin < 3.8 g/dL, and lower quartile of urine creatinine excretion (UCE) in 24 h based on sex. PEW was defined as meeting three or more of these criteria31.
Dietary assessment
The intake of individuals’ diets was recorded using a validated 168-item food frequency questionnaire (FFQ)32. After calculating food grams and multiplying by the daily intake frequency, the amount of each item was determined. FFQ was used to calculate the DII. Initially, the residual method was employed to adjust energy intake for each nutrient33. The DII score was determined according to the method described by Shivappa et al.34. To calculate DII, 31 food parameters were considered, including energy, fat, protein, carbohydrates, various vitamins (B1, B2, B3, B6, B9, B12, C, A, D, and E), beta-carotene, fiber, trans fatty acid (TFA), cholesterol, saturated fatty acid (SFA), polyunsaturated fatty acids (PUFA), monounsaturated fatty acids (MUFA), iron, selenium, magnesium, zinc, omega-6, omega-3, caffeine, onion, garlic, and tea.
For each participant, a Z-score was calculated by subtracting the mean of the global standard from the amount consumed and dividing it by the global standard deviation (SD). This Z-score was then converted to a percentile, multiplied by two, and adjusted by subtracting one, to minimize the influence of outliers. Additionally, this value was multiplied by the corresponding food inflammatory effect score to obtain the specific DII score for each food parameter. Finally, the overall DII score was calculated by summing all these individual scores. A higher DII score indicates a higher pro-inflammatory potential of the diet.
Statistical analysis
For statistical analysis, SPSS software (version 22) was used. Continuous variables were described using mean ± SD or median (interquartile range (IQR)), while categorical variables were presented as percentages. An independent sample T-test assessed parametric continuous variables, whereas the Mann–Whitney test was employed for non-parametric continuous variables. The chi-square test was applied for categorical variables. Additionally, logistic regression was conducted to assess the association between DII and sarcopenia as well as PEW. The multivariate model was adjusted for age, energy, protein, fat, and salt intake, sex and smoking history. Statistical significance was defined as a p-value less than 0.05.
Ethics approval and consent to participate
This study was approved by the medical research and ethics committee of Shiraz University of Medical Science and the informed consents were completed by all participants.
Results
The baseline features of the study population, according to the lower and higher mean of DII, are reported in Table 1. The median total iron-binding capacity (TIBC) (P = 0.031) and the DII total score (P˂0.001) were significantly greater in the higher DII group compared to the lower DII group. Other variables did not show significant differences between the two groups.
The intake of DII components based on lower and higher than the mean DII is shown in Table 2. According to the table, SFA (P = 0.001), TFA (P = 0.017), niacin (P = 0.036), beta-carotene (P = 0.005), and vitamin C (P = 0.033) were significantly different between the two groups.
The association between the DII score and the odds of sarcopenia in univariate and multivariate models is shown in Table 3. In the univariate model, a significant increase in the odds of sarcopenia was observed with each unit increase in DII (odds ratio (OR) = 1.379, 95% confidence interval (CI): 1.042–1.824) and age (OR = 1.073, 95% CI: 1.017–1.132). In the multivariate model, the association between DII and age with the odds of sarcopenia remained significant (DII: OR = 1.379, 95% CI: 1.030–1.846 and age: OR = 1.063, 95% CI: 1.007–1.121).
The association between the DII score and the odds of PEW in univariate and multivariate models is shown in Table 4. In both models, no significant association was observed.
Discussion
The main finding of our study was the significant association between a higher DII score and an increased risk of sarcopenia in CKD patients. Dietary inflammation appears to compromise muscle health in these patients. Contrary to expectations, our results did not show a significant association between DII scores and PEW.
Inflammation is common in patients with CKD, and the level of inflammation increases as kidney function worsens. Impaired kidney function results in the accumulation of uremic toxins, which exacerbate inflammatory states35. Elevated inflammatory markers, including C-reactive protein (CRP), interleukin (IL)-6, and tumor necrosis factor-alpha (TNF-α), exacerbate muscle protein catabolism, contributing to sarcopenia36. Anti-inflammatory interventions have shown promise in reducing CKD progression and attenuating sarcopenia37,38. These approaches attempt to disrupt the harmful loop that connects CKD and sarcopenia by targeting inflammation and providing a potential therapeutic tool to enhance the quality of life for CKD patients. Our findings revealed that a lower DII score was associated with less sarcopenia. This finding aligns with previous studies that have reported a positive association between DII and muscle mass in children, as well as sarcopenia in patients with CKD and Crohn’s disease39,40,41.
A pro-inflammatory diet may cause muscle mass loss by intensifying systemic inflammation12, and protective dietary patterns should be considered as a modifiable preventive factor for CKD-related sarcopenia. The DII, a novel dietary index that determines the total inflammatory potential of a diet, has been validated against systemic inflammatory biomarkers42. The DII score considers how various foods and nutrients interact with each other, rather than examining each nutrient or food independently concerning the disease. Consequently, it may offer more promising methods for disease prevention and control43,44.
There are several potential mechanisms explaining how high-inflammatory diets can exacerbate sarcopenia. A pro-inflammatory diet may heighten systemic inflammation, resulting in elevated levels of cytokines that inhibit muscle protein synthesis40. This can harm muscular health and increase oxidative stress, insulin resistance, and nutrient deficiencies45,46. Additionally, a pro-inflammatory diet may affect the gut flora, leading to muscle wasting by impairing the absorption of nutrients essential for muscle health and increasing systemic inflammation and insulin resistance47.
The present study did not show a significant association between DII and PEW. Few studies have investigated this association in CKD patients. However, a cross-sectional study of 105 subjects with ESRD did show associations between PEW and a pro-inflammatory diet48. One explanation for this discrepancy is that participants in our study were in the moderate stage of CKD, while the mentioned study examined ESRD. The prevalence of PEW in stages 3–5 is 11–46%, whereas in dialysis patients, it ranges from 28 to 80%49. The results may have also been impacted by methodological considerations such as sample size, PEW measurement techniques, or other confounding variables. It is also conceivable that, despite certain areas of overlap, the mechanisms behind sarcopenia and PEW have significant differences50,51, and DII might affect only a subset of these pathways. Further research is required to understand the underlying causes of this unequal connection and to consider other potential confounding factors.
In the present study, we observed that levels of SFA and TFA increased, and the levels of niacin, beta-carotene, and vitamin C decreased with an increase in the DII score. Additionally, the DII score was positively associated with sarcopenia status. These components have previously been linked to inflammatory responses in CKD patients. For example, high intakes of SFA and TFA are associated with pro-inflammatory markers and muscle mass52,53. Conversely, nutrients such as beta-carotene and vitamin C possess anti-inflammatory and muscle-building properties54,55,56. Although these nutrients were consumed around the recommended dietary allowance (RDA), research has indicated that patients experienced better outcomes when supplemented with nutrients56,57. However, more studies are needed to evaluate the safety and effectiveness of combined supplementation of anti-inflammatory nutrients. Furthermore, diets that replace SFA and TFA with healthier MUFA and PUFA have been shown to reduce inflammation levels52,58 and have positive effects on animal muscles. However, clinical trials have yielded contradictory results regarding their impact on muscles, necessitating further research52.
Although the current study provides insightful findings, it is important to acknowledge potential limitations. Due to the cross-sectional nature of our study, longitudinal studies are still needed to confirm causation and evaluate the long-term effects of diet modification in CKD patients. Also, further research is necessary to elucidate mechanistic pathways linking dietary inflammation to CKD outcomes. Such studies could inform the development of nutritional therapies tailored specifically to the requirements of CKD patients.
Another limitation of the present study was the small sample size. Furthermore, nutrient intake was assessed using the FFQ, which may introduce recall bias. Moreover, certain confounding variables were not controlled for in our study.
Conclusions
The current study highlighted the possible role of pro-inflammatory foods in exacerbating muscle health issues, specifically sarcopenia, in CKD patients. Future longitudinal studies could elucidate the causal relationships of these associations and potentially facilitate the development of nutritional therapies aimed at mitigating muscle-related problems in CKD.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Levey, A. S. & Coresh, J. Chronic kidney disease. Lancet 379, 165–180. https://doi.org/10.1016/s0140-6736(11)60178-5 (2012).
Kovesdy, C. P. Epidemiology of chronic kidney disease: an update 2022. Kidney Int. Suppl. 2011(12), 7–11. https://doi.org/10.1016/j.kisu.2021.11.003 (2022).
Hosseinpanah, F., Kasraei, F., Nassiri, A. A. & Azizi, F. High prevalence of chronic kidney disease in Iran: A large population-based study. BMC Publ. Health 9, 44. https://doi.org/10.1186/1471-2458-9-44 (2009).
Foley, R. N., Wang, C., Ishani, A., Collins, A. J. & Murray, A. M. Kidney function and sarcopenia in the United States general population: NHANES III. Am. J. Nephrol. 27, 279–286. https://doi.org/10.1159/000101827 (2007).
Raj, D. S., Sun, Y. & Tzamaloukas, A. H. Hypercatabolism in dialysis patients. Curr. Opin. Nephrol. Hypertens 17, 589–594. https://doi.org/10.1097/MNH.0b013e32830d5bfa (2008).
Doherty, T. J. Invited review: Aging and sarcopenia. J. Appl. Physiol. 1985(95), 1717–1727. https://doi.org/10.1152/japplphysiol.00347.2003 (2003).
Noce, A. et al. Cardiovascular protection of nephropathic male patients by oral food supplements. Cardiovasc. Ther. 2020, 1807941. https://doi.org/10.1155/2020/1807941 (2020).
Bocedi, A. et al. Erythrocyte glutathione transferase in kidney transplantation: A probe for kidney detoxification efficiency. Cell Death Dis. 9, 288. https://doi.org/10.1038/s41419-018-0289-3 (2018).
Fouque, D. et al. A proposed nomenclature and diagnostic criteria for protein–energy wasting in acute and chronic kidney disease. Kidney Int. 73, 391–398 (2008).
Kovesdy, C. P., Kopple, J. D. & Kalantar-Zadeh, K. Management of protein–energy wasting in non-dialysis-dependent chronic kidney disease: Reconciling low protein intake with nutritional therapy. Am. J. Clin. Nutr. 97, 1163–1177. https://doi.org/10.3945/ajcn.112.036418 (2013).
Chung, H. Y. et al. Molecular inflammation: Underpinnings of aging and age-related diseases. Ageing Res. Rev. 8, 18–30. https://doi.org/10.1016/j.arr.2008.07.002 (2009).
Bano, G. et al. Inflammation and sarcopenia: A systematic review and meta-analysis. Maturitas 96, 10–15. https://doi.org/10.1016/j.maturitas.2016.11.006 (2017).
Popolo, A., Autore, G., Pinto, A. & Marzocco, S. Oxidative stress in patients with cardiovascular disease and chronic renal failure. Free Radic. Res. 47, 346–356. https://doi.org/10.3109/10715762.2013.779373 (2013).
Qian, Q. Inflammation: A key contributor to the genesis and progression of chronic kidney disease. Contrib. Nephrol. 191, 72–83. https://doi.org/10.1159/000479257 (2017).
Shivappa, N. et al. A population-based dietary inflammatory index predicts levels of C-reactive protein in the seasonal variation of blood cholesterol study (SEASONS). Public Health Nutr. 17, 1825–1833. https://doi.org/10.1017/s1368980013002565 (2014).
Tabung, F. K. et al. Construct validation of the dietary inflammatory index among postmenopausal women. Ann. Epidemiol. 25, 398–405. https://doi.org/10.1016/j.annepidem.2015.03.009 (2015).
Galas, A., Kulig, P. & Kulig, J. Dietary inflammatory index as a potential determinant of a length of hospitalization among surgical patients treated for colorectal cancer. Eur. J. Clinic. Nutr. 68, 1168–1174. https://doi.org/10.1038/ejcn.2014.120 (2014).
Syed Soffian, S. S. et al. Meta-analysis of the association between dietary inflammatory index (DII) and colorectal cancer. Nutrients https://doi.org/10.3390/nu14081555 (2022).
Shu, Y. et al. Associations of dietary inflammatory index with prediabetes and insulin resistance. Front. Endocrinol. 13, 820932. https://doi.org/10.3389/fendo.2022.820932 (2022).
Jayanama, K. et al. Relationship between diet quality scores and the risk of frailty and mortality in adults across a wide age spectrum. BMC Med. 19, 64. https://doi.org/10.1186/s12916-021-01918-5 (2021).
Rouhani, M. H. et al. Dietary inflammatory index and its association with renal function and progression of chronic kidney disease. Clin. Nutr. ESPEN 29, 237–241. https://doi.org/10.1016/j.clnesp.2018.09.001 (2019).
Mazidi, M., Shivappa, N., Wirth, M. D., Hebert, J. R. & Kengne, A. P. Greater dietary inflammatory index score is associated with higher likelihood of chronic kidney disease. Br. J. Nutr. 120, 204–209. https://doi.org/10.1017/s0007114518001071 (2018).
Diao, H. et al. Association between dietary inflammatory index and sarcopenia: A meta-analysis. Nutrients https://doi.org/10.3390/nu15010219 (2023).
Huang, Y. et al. Dietary inflammatory potential is associated with sarcopenia among chronic kidney disease population. Front. Nutr. 9, 856726. https://doi.org/10.3389/fnut.2022.856726 (2022).
Daniel, W. W. & Cross, C. L. Biostatistics: A Foundation for Analysis in the Health Sciences (Wiley, London, 2018).
Draugalis, J. R. & Plaza, C. M. Best practices for survey research reports revisited: Implications of target population, probability sampling, and response rate. Am. J. Pharmac. Educ. 73, 142 (2009).
Lwanga, S. K., Lemeshow, S. & Organization, W. H. Sample Size Determination in Health Studies: A Practical Manual (World Health Organization, UK, 1991).
Moghaddam, M. B. et al. The Iranian version of international physical activity questionnaire (IPAQ) in Iran: Content and construct validity, factor structure, internal consistency and stability. World Appl Sci J 18, 1073–1080 (2012).
Chen, L.-K. et al. Sarcopenia in Asia: Consensus report of the Asian working group for sarcopenia. J. Am. Med. Dir. Assoc. 15, 95–101 (2014).
Mahmoodi, M. et al. Validation of the Persian version of the sarcopenia-specific quality of life questionnaire (SarQoL®-IR). Aging Clin. Exp. Res. 35, 137–145 (2023).
Hyun, Y. Y. et al. Nutritional status in adults with predialysis chronic kidney disease: KNOW-CKD study. J. Korean Med. Sci. 32, 257–263 (2017).
Mirmiran, P., Esfahani, F. H., Mehrabi, Y., Hedayati, M. & Azizi, F. Reliability and relative validity of an FFQ for nutrients in the Tehran lipid and glucose study. Public health nutrition 13, 654–662 (2010).
Willett, W. C., Howe, G. R. & Kushi, L. H. Adjustment for total energy intake in epidemiologic studies. Am. J. Clin. Nutr. 65, S1220–S1228 (1997).
Shivappa, N., Steck, S. E., Hurley, T. G., Hussey, J. R. & Hébert, J. R. Designing and developing a literature-derived, population-based dietary inflammatory index. Public Health Nutr. 17, 1689–1696 (2014).
Rapa, S. F., Di Iorio, B. R., Campiglia, P., Heidland, A. & Marzocco, S. Inflammation and oxidative stress in chronic kidney disease-potential therapeutic role of minerals, vitamins and plant-derived metabolites. Int. J. Mol. Sci. https://doi.org/10.3390/ijms21010263 (2019).
Kamper, R. S. et al. Associations between inflammatory markers, body composition, and physical function: the Copenhagen sarcopenia study. J. Cachexia Sarcopenia Muscle 12, 1641–1652. https://doi.org/10.1002/jcsm.12832 (2021).
Pérez-Torres, A., Caverni-Muñoz, A. & González García, E. Mediterranean diet and chronic kidney disease (CKD): A practical approach. Nutrients https://doi.org/10.3390/nu15010097 (2022).
Ganapathy, A. & Nieves, J. W. Nutrition and sarcopenia—what do we know?. Nutrients https://doi.org/10.3390/nu12061755 (2020).
Amakye, W. et al. The relationship between dietary inflammatory index (DII) and muscle mass and strength in Chinese children aged 6–9 years. Asia Pac. J. Clin. Nutr. 27, 1315–1324. https://doi.org/10.6133/apjcn.201811_27(6).0019 (2018).
Huang, Y. et al. Dietary inflammatory potential is associated with sarcopenia among chronic kidney disease population. Front. Nutr. 9, 856726 (2022).
Bian, D. et al. Association between dietary inflammatory index and sarcopenia in Crohn’s disease patients. Nutrients https://doi.org/10.3390/nu14040901 (2022).
Byrd, D. A. et al. Development and validation of novel dietary and lifestyle inflammation scores. J. Nutr. 149, 2206–2218. https://doi.org/10.1093/jn/nxz165 (2019).
Firoozi, D. et al. The association between energy-adjusted dietary inflammatory index, body composition, and anthropometric indices in COVID-19-infected patients: A case-control study in Shiraz Iran. Int. J. Clin. Pract. 2022, 5452488. https://doi.org/10.1155/2022/5452488 (2022).
Hébert, J. R., Shivappa, N., Wirth, M. D., Hussey, J. R. & Hurley, T. G. Perspective: The dietary inflammatory index (DII)-lessons learned, improvements made, and future directions. Adv. Nutr. 10, 185–195. https://doi.org/10.1093/advances/nmy071 (2019).
Picca, A. & Calvani, R. Molecular mechanism and pathogenesis of sarcopenia: An overview. Int. J. Mol. Sci. https://doi.org/10.3390/ijms22063032 (2021).
Bloom, I., Shand, C., Cooper, C., Robinson, S. & Baird, J. Diet quality and sarcopenia in older adults: A systematic review. Nutrients https://doi.org/10.3390/nu10030308 (2018).
Liu, C. et al. Understanding the gut microbiota and sarcopenia: A systematic review. J Cachexia Sarcopenia Muscle 12, 1393–1407. https://doi.org/10.1002/jcsm.12784 (2021).
Kizil, M. et al. Dietary inflammatory index is associated with serum C-reactive protein and protein energy wasting in hemodialysis patients: A cross-sectional study. Nutr. Res. Pract. 10, 404–410 (2016).
Koppe, L., Fouque, D. & Kalantar-Zadeh, K. Kidney cachexia or protein–energy wasting in chronic kidney disease: Facts and numbers. J Cachexia Sarcopenia Muscle 10, 479–484. https://doi.org/10.1002/jcsm.12421 (2019).
Hanna, R. M., Ghobry, L., Wassef, O., Rhee, C. M. & Kalantar-Zadeh, K. A practical approach to nutrition, protein–energy wasting, sarcopenia, and cachexia in patients with chronic kidney disease. Blood Purif. 49(1–2), 202–211. https://doi.org/10.1159/000504240 (2020).
Kim, D. W. & Song, S. H. Sarcopenia in chronic kidney disease: From bench to bedside. Korean J. Intern. Med. 38, 303–321. https://doi.org/10.3904/kjim.2022.338 (2023).
Huang, X., Lindholm, B., Stenvinkel, P. & Carrero, J. J. Dietary fat modification in patients with chronic kidney disease: n-3 fatty acids and beyond. J. Nephrol. 26, 960–974. https://doi.org/10.5301/jn.5000284 (2013).
Huang, T. et al. Potential of fatty acids in treating sarcopenia: A systematic review. Nutrients https://doi.org/10.3390/nu15163613 (2023).
Kawamura, A. et al. Combined intake of astaxanthin, β-carotene, and resveratrol elevates protein synthesis during muscle hypertrophy in mice. Nutrition 69, 110561. https://doi.org/10.1016/j.nut.2019.110561 (2020).
Kitakaze, T., Harada, N., Imagita, H. & Yamaji, R. β-carotene increases muscle mass and hypertrophy in the soleus muscle in mice. J. Nutr. Sci. Vitaminol. 61, 481–487. https://doi.org/10.3177/jnsv.61.481 (2015).
Juszczak, A. B., Kupczak, M. & Konecki, T. Does vitamin supplementation play a role in chronic kidney disease?. Nutrients https://doi.org/10.3390/nu15132847 (2023).
Liu, S., Zhang, L. & Li, S. Advances in nutritional supplementation for sarcopenia management. Front. Nutr. 10, 1189522. https://doi.org/10.3389/fnut.2023.1189522 (2023).
Malesza, I. J. et al. High-fat, western-style diet, systemic inflammation, and gut microbiota: A narrative review. Cells https://doi.org/10.3390/cells10113164 (2021).
Acknowledgements
We sincerely thank all field investigators, staff, and participants of the present study.
Author information
Authors and Affiliations
Contributions
F.M, F.J, S.R, F.S, Z.S and M.N; Contributed to writing the first draft. M.N; Contributed to all data, statistical analysis, and interpretation of data. S.E.J, and S.B; Contributed to the research concept, supervised the work, and revised the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Mansouri, F., Jafari, F., Ranjbar, S. et al. Dietary inflammatory index could increase the risk of sarcopenia in patients with chronic kidney disease. Sci Rep 14, 15284 (2024). https://doi.org/10.1038/s41598-024-65340-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-65340-6
- Springer Nature Limited