
Abstract
Insertion mutations in exon 20 of the epidermal growth factor receptor gene (EGFR exon20ins) are rare, heterogeneous alterations observed in non-small cell lung cancer (NSCLC). With a few exceptions, they are associated with primary resistance to established EGFR tyrosine kinase inhibitors (TKIs). As patients carrying EGFR exon20ins may be eligible for treatment with novel therapeutics—the bispecific antibody amivantamab, the TKI mobocertinib, or potential future innovations—they need to be identified reliably in clinical practice for which quality-based routine genetic testing is crucial. Spearheaded by the German Quality Assurance Initiative Pathology two international proficiency tests were run, assessing the performance of 104 participating institutes detecting EGFR exon20ins in tissue and/or plasma samples. EGFR exon20ins were most reliably identified using next-generation sequencing (NGS). Interestingly, success rates of institutes using commercially available mutation-/allele-specific quantitative (q)PCR were below 30% for tissue samples and 0% for plasma samples. Most of these mutation-/allele-specific (q)PCR assays are not designed to detect the whole spectrum of EGFR exon20ins mutations leading to false negative results. These data suggest that NGS is a suitable method to detect EGFR exon20ins in various types of patient samples and is superior to the detection spectrum of commercially available assays.
Similar content being viewed by others

Introduction
EGFR exon20ins are rare somatic alterations observed in NSCLC, which make up between 2 and 12% of all EGFR gene alterations1,2,3. They are a largely heterogeneous group of mutations and most frequently occur in the region encoding for amino acids Asp761 to Cys775 of the C-helix domain and the loop following the C-helix domain1,4,5. With a few exceptions, EGFR exon20ins are generally associated with resistance to first-, second- and third-generation EGFR TKIs1. A key challenge in the detection of patients with EGFR exon20ins mutation is the large heterogeneity of these mutations. First-generation EGFR inhibitors (gefitinib and erlotinib) turned out to be an ineffective therapeutic option in the vast majority of patients harboring an EGFR exon20ins mutation3. Only few exceptions, e.g. the p.Ala763_Tyr764insPheGlnGluAla mutation, seem to respond to these inhibitors whereas the most common EGFR exon20ins mutations e.g. p.Ala767_Val769dup, p.Ser768_Asp770dup and p.Asn771_His773dup show high IC50 values (IC50 > 100) for erlotinib and gefitinib6. For second-line inhibitors (e.g. neratinib, dacomitinib and afatinib) there is limited clinical evidence for the effective use in patients with EGFR exon20ins mutations. Regarding third-generation EGFR inhibitors, Poziotinib is one of the most advanced inhibitors showing response rates against e.g. p.Asp770insAsnProGly or p.Asn771delinsPheHis6. Osimertinib shows high IC50 values (IC50 > 100) for the p.Ser768_Asp770dup and p.Asn_771_His773dup mutations and intermediate IC50 values (IC50 < 10 < 100) for e.g. p.Ala_Val769dup. However, these third-generation EGFR inhibitors also demonstrated activity against wildtype EGFR which may cause dose limitations in patients with EGFR exon20ins mutations.
Fortunately efficacious targeted therapies are slowly emerging: in December 2021, the bispecific antibody amivantamab was the first of its kind to be approved by the European Commission for the treatment of patients with advanced NSCLC and activating EGFR exon20ins, after failure of platinum-based therapy7. While the TKI mobocertinib is available for the same indication in the United States (US) as well as the United Kingdom (UK), the European marketing authorization application was withdrawn by the manufacturer in July 20228,9. Further therapeutic approaches targeting EGFR exon20ins are currently in the pipeline10.
To identify patients eligible for treatment with these innovative targeted therapies, molecular testing is a prerequisite. The three most common EGFR ex20ins mutations account for less than 50% showing the high heterogeneity of this group of mutations. Therefore, reliable as well as sensitive detection methods are needed. Methodological standardization is of utmost importance to ensure the accuracy and reproducibility of molecular testing, especially when performed in a decentralized manner. Activities to achieve this goal include internal quality assessments, e.g., routine testing of known positive and negative samples, as well as external quality assessments, e.g., regular participation in proficiency testing.
Since patient data are often analyzed according to the type of mutation—for example, treatment responses may differ depending on the alteration present—, EGFR exon20ins, as other mutations, must be described in a standardized manner. To enable the consistent identification of patients carrying the same aberrations, the Human Genome Variation Society (HGVS) proposed guidelines for the unambiguous description of sequence variants11,12. In this context, a duplication has to be prioritized when a variant can be described as either duplication or insertion, and the most possible 3′ position should be used for all descriptions of variants11,12.
QuIP®, a joint venture of the German Society of Pathology (Deutsche Gesellschaft für Pathologie, DGP) and the Federal Association of German Pathologists (Bundesverband Deutscher Pathologen, BDP), coordinates regular proficiency tests to monitor performance quality of institutes in the field of diagnostic immunohistochemistry and molecular pathology. Here, we report the results of two such proficiency tests, assessing the performance of a total of 104 international pathology institutes with regard to the detection of a pre-specified set of EGFR exon20ins variants present in either formalin-fixed, paraffin-embedded (FFPE) tissue or liquid biopsy samples.
Results
Selection of reference samples
Reference samples for the external proficiency tests were chosen based on the mutational spectrum of EGFR exon20ins and the respective prevalence detected in a patient cohort from Cologne upon performing a retrospective database analysis (Figs. 1 and 2; Table S1). Overall, 203 patients with a total of 56 different EGFR exon20ins were identified; prevalence ranged between 0.5 and 17.7% within this group of patients. The mutations with the highest prevalence were chosen for the proficiency tests as they are clinically most relevant and cover the heterogeneity of EGFR exon20ins mutations.

Spectrum of EGFR exon20ins. Insertions in exon 20 of the EGFR gene are heterogeneous: in a patient cohort from Cologne (n = 203; recorded at the Institute of Pathology of the University of Cologne, Faculty of Medicine, and University Hospital Cologne), a total of 50 distinct EGFR exon20ins variants were identified on the protein level, covering the entire C-helix as well as the loop following the C-helix. Proficiency test samples were chosen based on these findings to feature a wide range of different EGFR exon20ins variants occurring in clinical practice. Ref-Seq ID: NM_005228.

Prevalence of EGFR exon20ins. In a patient cohort from Cologne (n = 203; recorded at the Institute of Pathology of the University of Cologne, Faculty of Medicine, and University Hospital Cologne), a total of 50 distinct EGFR exon20ins variants were observed on the protein level, with prevalence ranging between ~ 0.5% and ~ 5% of all EGFR exon20ins (excluding the three most common alterations). The most common EGFR exon20ins occurring in this cohort were c.2300_2308dup (p.Ala767_Val769dup; 17.7%), c.2303_2311dup (p.Ser768_Asp770dup; 17.2%), and c.2311_2319 dup (p.Asn771_His773dup; 10.3%). Approximately 50% of the detected EGFR exon20ins have a prevalence of < 1%. Ref-Seq ID: NM_005228.
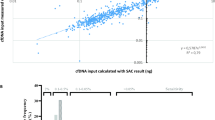
To simulate real-life conditions, i.e., to ensure that participating institutes were able to detect low allelic fractions potentially occurring in patients´ samples, different allelic fractions were chosen for the liquid biopsy samples. According to the German uniform assessment standard (Einheitlicher Bewertungsmaßstab, EBM) regulating the reimbursement of services provided by statutory health insurance-(SHI)-accredited physicians, the EGFR exon20ins detection method of choice must have a limit of detection (LOD) ≤ 1%13. The minimal allelic fraction and the region to be covered by this proficiency test was stated in the instructions. Each participant could check whether the established test would be suitable for this proficiency test. The responsibility for choosing a suitable assay covering the mutational spectrum and the limit of detection requested rested with the respective participants.
Assessment of laboratory performance (DACH proficiency test)
A total of 37 institutes signed up for participation in the DACH proficiency test. After receiving their respective test sets, 19 institutes submitted results for both methodological parts, tissue and liquid biopsy, while 18 institutes submitted results for the tissue part only.
Tissue part
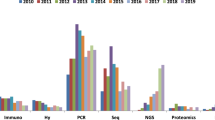
Out of the 37 institutes submitting results, 32 (86.5%) received certificates of successful participation. Samples 1, 4 and 5 were most often falsely described as wildtype when in fact carrying EGFR exon20ins (Table S2). Successful participation did not depend on the DNA extraction kit used by participants, but rather on the subsequently employed EGFR exon20ins detection method (Fig. 3A). NGS (65%) and mutation-/allele-specific quantitative (q)PCR methods (19%) were used more frequently than Sanger sequencing (13%) or pyrosequencing (3%). All institutes using NGS, pyro- or Sanger sequencing passed the proficiency test, while only 2 of the 7 institutes (28.5%) using commercially available mutation-/allele-specific (q)PCR did (Table S3). Notably, all institutes misclassifying cases 1, 4 and 5 had employed PCR-based methods. No specific kit or platform was associated with successful participation: institutes utilized numerous devices and platforms as well as various kits or panels for the detection of EGFR exon20ins (Table S3).

Overview of proficiency test outcomes depending on methods used for EGFR exon20ins testing. Successful participation in the proficiency tests did not depend on the kit used to extract (cf)DNA, but on the method subsequently used to detect EGFR exon20ins. Overall, institutes utilizing NGS and Sanger sequencing had higher success rates than institutes employing mutation-/allele-specific (q)PCR. Panel (A) shows the results of the tissue part of the DACH proficiency test. All participants using NGS, pyro- or Sanger sequencing as method of choice passed, whereas only 2 of the 7 institutes using mutation-/allele-specific (q)PCR did. Panel (B) displays the outcomes of the liquid biopsy part of the DACH proficiency test. None of the participating institutes using mutation-/allele-specific (q)PCR passed, while 84% of the institutes utilizing NGS participated successfully. Panel (C) shows the results of the tissue part of the international proficiency test: 89.8% of the participating institutes employing NGS or Sanger sequencing as their method of choice passed the quality control test, whereas only 2 of the 18 institutes (11.1%) using mutation-/allele-specific (q)PCR did. Panel (D) displays the outcomes of the liquid biopsy part of the international proficiency test. None of the participating institutes utilizing mutation-/allele-specific (q)PCR or pyrosequencing passed, while 81.5% of the institutes using NGS participated successfully. Details on suppliers can be found in the Supplement.
Despite not influencing the performance rating, it is worth mentioning that sample 9 was incorrectly annotated by most participating institutes. In this sample, nucleotides 2300 to 2308 are duplicated, resulting in a duplication of amino acids 767 to 769 (p.Ala767_Val769dup). Yet, it was often classified as insertion instead of a duplication (Fig. S1). Furthermore, participants did not follow the HGVS 3′ rule according to which the most 3′ position possible of the reference sequence is arbitrarily assigned to be changed11,12. In this particular case, annotation leads to a shift of the mutation description by three base pairs towards the 3′ end of the gene.
The remainder of the samples were correctly annotated by most of the participating institutes.
Liquid biopsy part
Out of 19 participating institutes submitting results, 12 (66.7%) received certificates of successful participation. Samples 1, 2, 4, 5, 6, and 7 were most frequently misclassified as wildtype when in fact carrying EGFR exon20ins (Table S4). Case 2 had a low allelic fraction of 1%; eight institutes did not detect this mutation. Different commercially available kits were used to extract cell-free DNA (cfDNA) from plasma samples. Successful participation did not seem to depend on the extraction kit used but rather on the detection method subsequently employed (Fig. 3B). EGFR exon20ins detection methods included NGS (72%), fragment analysis (6%) and commercially available mutation-/allele-specific (q)PCR (22%). Multiple devices and platforms as well as kits or panels were used for the detection of EGFR exon20ins (Table S5). None of the institutes using commercially available mutation-/allele-specific (q)PCR passed the proficiency test, while 84% of the institutes utilizing NGS participated successfully (Table S5). One institute using fragment analysis (laboratory-developed test, LDT) passed.
Assessment of laboratory performance (international proficiency test)
Of the 76 international institutes, which had registered to participate, 48 submitted results for both parts, 19 submitted results for the tissue part only, 1 submitted results for the liquid biopsy part only, and 8 did not submit any results at all. One institute submitted an empty questionnaire which counts as a submission; however, this institute was not considered in the subsequent analysis.
Tissue part
Of the 67 institutes entering test results for the tissue part, 46 (68.7%) received certificates of successful participation. Cases 4 and 5 were most often mislabeled as wildtype when in fact carrying EGFR exon20ins (Table S6). In line with the DACH proficiency test, participating institutes used different DNA extraction kits as well as different EGFR exon20ins detection methods (NGS: 70%, mutation-/allele-specific (q)PCR: 27%, and Sanger sequencing: 3%). Most institutes (89.8%) using NGS or Sanger sequencing passed the proficiency test, while only 2 of the 18 institutes (11.1%) using commercially available mutation-/allele-specific (q)PCR participated successfully (Fig. 3C). Institutes successfully using NGS or Sanger sequencing, passed regardless of the kit or platform that was chosen to detect EGFR exon20ins mutations (Table S7).
Liquid biopsy part
Of the 48 institutes submitting results for the liquid biopsy part, 22 (45.8%) participated successfully. False variant description occurred for all cases but one (case 3 [wildtype]; Table S6). None of the cases were removed from the current analysis, as mislabeling of the samples was not a consequence of material-related problems, but rather a problem of applying an inadequate detection method.
Various commercially available kits were utilized for cfDNA extraction; again, successful participation did not depend on the type of extraction kit used, but on the detection method employed afterwards (Fig. 3D). Molecular methods for EGFR exon20ins testing comprised NGS (56%), pyrosequencing (2%), and commercially available mutation-/allele-specific (q)PCR (42%)—different devices and platforms as well as kits and panels were used. None of the participating institutes utilizing either mutation-/allele-specific (q)PCR or pyrosequencing passed the proficiency test, while 22 of the 27 institutes (81.5%) using NGS participated successfully (Table S8). Although case 5 (p.His773dup) had a low allelic fraction of 2%, it was identified correctly by 87.5% of the participating institutes. Notably, 5 institutes using the Ion GeneStudio S5 as their NGS platform failed. However, this seems not to be a general problem with this platform as seven other institutes using the same platform succeeded in the proficiency test.
Discussion
In clinical patient care setting, the detection of heterogeneous EGFR ex20ins mutations is challenging for molecular diagnostics laboratories. Two proficiency tests were performed to compare the results of EGFR ex20ins mutation detection of molecular diagnostic laboratories. Clinical NSCLC tissue and artificial liquid biopsy samples with and without EGFR ex20ins mutations were used: one test covered institutes from Germany, Austria, and Switzerland only (further referred to as “DACH”) and one covered institutes from Austria, Belgium, Estonia, France, Germany, Greece, Hungary, Ireland, Italy, Lithuania, Netherlands, Poland, Portugal, Russia, Slovakia, Switzerland, and Turkey (further referred to as “international”).
Success rate for the DACH proficiency test for the tissue part was almost 90% showing a high-quality standard in these countries. Most frequently NGS (65%) was used followed by mutation-/allele-specific (q)PCR (19%). In the international proficiency test success rate was lower with almost 70%. Again, most frequently used method of choice was NGS (70%) and mutation-/allele-specific (q)PCR (27%). However, 30% of the participants failed to succeed in the international proficiency test for the detection of EGFR ex20ins mutations indicationg the need to optimize molecular diagnostics. Appropriate and regularly updated validation, standardization and quality control guidelines might help achieve better results in the future14.
The results of the proficiency tests on liquid biopsy samples further confirms this observation. In the DACH proficiency test for liquid biopsy samples almost 70% of the participants succeeded, whereas in the international proficiency test only half of the participants succeeded. In both tests, method of choice was NGS again followed by mutation-/allele-specific (q)PCR. However, in the international proficiency test qPCR was used in 42% of participants; in the DACH proficiency test only 22% used qPCR.
Due to the wide range of different mutations as well as the overall rarity of EGFR exon20ins, the respective detection method necessitates sufficient analytical sensitivity, as well as specificity and needs to span the whole EGFR exon 20 region. Most commercially available mutation-/allele-specific (q)PCR kits, however, only detect a limited number of distinct EGFR exon20ins (Fig. S2); therefore, the spectrum of mutations covered by a specific test kit must be carefully scrutinized. NGS, in contrast, can cover the entirety of exon 20 of the EGFR gene with sufficient sensitivity to detect even low allelic fractions within the range of 1%.
In a sample cohort from Cologne, 54 different mutations were detected on DNA level, spanning nucleotides 2300 to 2378 and resulting in 50 distinct alterations on protein level (Fig. 2; Table S1). The three most common EGFR ex20ins mutations account for less than 50% showing the high heterogeneity of this group of mutations. This is in accordance with other publications: for example, Bauml et al.1 identified 40 unique EGFR exon20ins variants in a cohort of 175 patients15. In addition, Vyse and Huang as well as Yasuda et al.16 demonstrated that EGFR exon20ins occur throughout the entire region encoding the C-helix as well as the loop following the C-helix. In the cohort from Cologne, the mutations p.Ala767_Val769dup (17.7% of all EGFR exon20ins recorded), p.Ser768_Asp770dup (17.2% of all EGFR exon20ins recorded) and p.Asn771_His773dup (10.3% of all EGFR exon20ins recorded) occurred most frequently (Fig. 2; Table S1). Vyse et al.1 published similar numbers, and while Leal et al.17 described lower frequencies, they showed that p.Ala767_Val769dup and p.Ser768_Asp770dup were among the most frequent EGFR exon20ins. Yet, only p.Ala767_Val769 can be detected by all six commercially available mutation-/allele-specific (q)PCR kits shown in Fig. S2. In contrast, p.Ser768_Asp770dup can be detected by 5 of the 6 mutation-/allele-specific (q)PCR kits displayed and p.Asn771_His773dup is only covered by one of these assays. In line with this, 71% of the DACH region institutes and 88.8% of the international institutes using commercially available mutation-/allele-specific (q)PCR for the tissue parts failed their proficiency tests. Unsuccessful participation was not associated with a single system but could be observed across different PCR kits from various providers showing that the detection spectrum of these assays is not sufficient. In contrast, all DACH region institutes and 89.8% of the international institutes using NGS or Sanger sequencing for the tissue parts succeeded.
None of the institutes employing commercially available mutation-/allele-specific (q)PCR for their respective liquid biopsy parts passed. In contrast, the sole institute performing fragment analysis for the liquid biopsy part succeeded. Our data indicate that fragment analysis, in general, works for the detection of insertion mutations. However, it needs subsequent analysis to determine the exact underlying mutation as the different EGFR exon20ins mutations show different response rates to inhibitors6,18,19.
Confirming our observations, a recent publication demonstrated that PCR-based assays only detect about 50% of the EGFR exon20ins variants identified by NGS15. Similarly, Arcila et al.20 observed that the Idylla™ EGFR assay, while suitable for the detection of common EGFR mutations, did not detect certain EGFR exon20ins mutations identified by NGS. Most commercially available mutation-/allele-specific (q)PCR assays are simply not designed to detect the whole range of relevant EGFR exon20ins. If the probe-based mutation-/allele-specific (q)PCR lacks a probe for a specific mutation, the assay is not able to detect this mutation (Fig. S3). In a worst case scenario, up to 50% of patients with an EGFR ex20ins mutation would obtain false negative test results, consequently not receiving targeted treatment. Amivantamab, a bispecific antibody targeting MET and EGFR showed in a post platinum population a response rate of 40% and a progression free survival of 8.3 month. However, this targeted therapy is only approved for the treatment of patients with advanced NSCLC with activating EGFR ex20ins, after failure of platinum-based therapy. Therefore, the correct identification of EGFR ex20ins mutations is essential for therapeutic decisions.
Furthermore, results for reference sample 5 of the liquid biopsy part of the international proficiency test revealed that the limit of detection (LOD) might differ depending on the detection method used: as shown in Fig. S2, this specific mutation is covered by all six mutation-/allele-specific (q)PCR kits; however, none of the institutes using commercially available mutation-/allele-specific (q)PCR were able to identify it correctly. As it was stated in the proficiency test instructions that the minimal allelic fraction might be as low as 1%, institutes would have been required to choose a test that guarantees a sufficient limit of detection.
Interestingly, 2 of the 13 institutes using NGS in the DACH proficiency test failed to detect the mutation at an allelic fraction of 1% (case 2). As other participants with the same NGS platform or bioinformatics pipeline could detect these variants with low allelic fraction, This seems to be not a general NGS platform or pipeline specific problem. Furthermore, in the liquid biopsy part of the international proficiency test 5 institutes using the Ion GeneStudio S5 failed. However, seven other participants using the same platform succeeded in the proficiency test. It is unknown whether the variant was not called by the bioinformatic software tool, or if the variant was not detectable in the raw data.
The false-negative results may be caused by problems during cfDNA extraction, library preparation, sequencing or the bioinformatic analysis. To draw a final conclusion, more participants are needed with the same complete workflow to compare the whole analysis process. Our results indicate that both, the design of the method applied must be considered, and the entire analysis process needs to be validated under high quality standards to ensure sufficient sensitivity and specificity.
It is noteworthy to mention that in Europe, laboratories are generally free to choose the diagnostic method they use for the detection of molecular alterations (although recommendations have been issued for certain indications and biomarkers21). In contrast, the US FDA approves companion diagnostics together with the corresponding therapeutic product, or a non-companion diagnostic assay can be used in a laboratory that follows the Clinical Laboratory Improvement Amendments (CLIA), thereby restricting the freedom of methodological choice22. In case of PIK3CA mutation analysis in advanced breast cancer this approach has been shown to be possibly detrimental: in a study by Martinez-Saez et al.23, up to 95% of the patients potentially eligible for treatment with a PI3K inhibitor were missed by the mutation-/allele-specific (q)PCR kit approved as a companion diagnostic by the FDA. In comparison, two NGS-based tests detecting EGFR exon20ins are currently approved as companion diagnostics for targeted therapies, both of which have been shown to reliably identify patients benefiting from treatment with amivantamab22,24.
To consistently identify all patients with NSCLC potentially eligible for treatment with novel targeted therapies in clinical practice, the European Society for Medical Oncology (ESMO) recommends routine molecular diagnostic testing of tumor or plasma samples, using comprehensive NGS panels21,25, highlighting the priority of NGS in clinical routine practice. However, it seems that using NGS is not the current state-of-the-art in many laboratories. One reason might be high costs, the workload to establish this method and the high amount of bioinformatic data that need to be analyzed. Compared to NGS, mutation-/allele-specific (q)PCR and Sanger sequencing are easier to establish, have a shorter turn-around time and are accompanied by lower costs (Table 1).
While correct labeling of the different variants according to HGVS guidelines was not related to performance in the proficiency tests, it is noteworthy to mention that participating institutes mainly disregarded the following three rules when naming EGFR exon20ins: (1) insertion of nucleotide repeats should be designated a duplication, (2) for all descriptions of variants, the most 3′ position possible should be used, (3) three letter code is preferred over one letter code11. For example, most participants did not use the correct nomenclature to describe the mutation in case nine of the national proficiency test (Fig. S1). There were more than six different descriptions of this particular mutation (correctly named p.Ala767_Val769dup). Whether this was due to bioinformatic errors or to human errors was not evaluated. However, some bioinformatic tools are known to be prone to incorrect annotations. For example, the software tool ANNOVAR, that functionally annotates genetic variants, is known to generate misclassifications. In contrast, the Ensembl Variant Effect Predictor (VEP) for example is a more accurate tool showing a 99,6% concordance with HGVS nomenclature in the study of Tuteja et al.26.
To facilitate inter-patient comparisons, as part of real-world data analyses, or intra-patient comparisons, (when performing a re-biopsy), it is essential to follow a consistent naming convention for EGFR exon20ins. In addition, as different EGFR exon20ins may result in different conformations on the protein level, not every mutation will respond to targeted therapy in the same way6,18,19. It is therefore of utmost importance to differentiate distinct EGFR exon20ins variants.
Non-compliance with HGVS recommendations when reporting biomarker variants is a known problem of external quality assessments27. While compliance has increased over the years, especially upon repeat participation of laboratories in multiple proficiency tests, there is still room for improvement with regards to clinical test reporting27. Our results further support this finding.
Inconsistent nomenclature of somatic variants also concerns descriptions of EGFR exon20ins in datasheets accompanying certain mutation-/allele-specific (q)PCR kits. In 6 different (q)PCR manuals, the mutation p.His773dup is described in three different ways (p.H773_V774insH, c.2319_2320insCAC and p.His773_V774insH; Fig. S2) and is only annotated correctly according to HGVS in one datasheet.
In summary, these two independent international proficiency tests have demonstrated that in large parts of Europe, a broad range of EGFR exon20ins can be detected reliably in routine tissue and liquid biopsy samples, if the test is suitable and validated. In terms of sample suitability, both, the internal and external proficiency tests have shown that—if processed correctly—artificial samples are a good alternative to routine pathology samples.
Materials and methods
Compilation of the mutational spectrum and clinical samples
To collate the mutational spectrum for the internal as well as the external proficiency tests, an extensive retrospective database analysis of clinical samples which had been examined by targeted NGS at the Institute of Pathology at the University of Cologne, Faculty of Medicine and University Hospital Cologne between 2013 and 2021 was performed, and the prevalence of the different EGFR exon20ins were calculated (study was approved by the Medical Ethics Committee of the University of Cologne, Faculty of Medicine, and University Hospital Cologne [ethical approval no. 22-1343-retro]). Clinical samples suitable for the proficiency tests were identified; samples were collected with informed consent from each patient and under approval of local ethical protocols. All methods were performed in accordance with the relevant guidelines and regulations of the Deutsche Akkreditierungsstelle (DAkkS). All patients´ samples were resection specimens of the lung. Tumor type was determined as non-small cell lung cancer (NSCLC). Tumor cell content of the samples was determined by experienced, board certified pathologists and had to be at least 30%. Necrosis could not exceed 10%. Furthermore, samples with one of the most common EGFR ex20ins mutation were chosen. As for clinical samples, two different mutations were chosen (p.Ala767_Val769dup and p.Ser768_Asp770dup) showing at least an allelic fraction of more than 20% and a coverage of > 200 × in the NGS analysis to be reliably detectable.
Internal proficiency test
To determine the suitability of pre-selected reference samples for external EGFR exon20ins proficiency testing, an internal EGFR exon20ins proficiency test was established by the QuIP® lead panel institute, the Institute of Pathology at the University of Cologne, Faculty of Medicine and University Hospital Cologne.
Proficiency test specimens
Tissue reference samples comprised either pseudo-anonymized clinical or artificial FFPE material. Artificial samples were specifically provided by SensID GmbH (Rostock, Germany): the clinically relevant mutation sequences were synthesized as high fidelity dsDNA fragments with a size distribution similar to cfDNA/ctDNA by an EN ISO 13485-certified service provider. For artificial FFPE samples the mutation sequences were used to change the genomic profile of BDXXP4 cells (lymphoblastoid wt cell line), which were subsequently converted to FFPE cell blocks and sectioned with a microtome. Cell density was adjusted to yield > 400 ng DNA/section as determined by fluorometry (Qubit, Thermo Fisher Scientific Inc., Waltham, MA, USA).
Functionality and allelic fraction of artificial FFPE samples were tested by validated ddPCR assays (Bio-Rad QX200, Bio-Rad Laboratories, Hercules, California, USA). Each batch of artificial samples was quality-controlled for DNA quantity and VAF according to ISO 2850 (Acceptable Quality Levels) prior to testing for compatibility with NGS methods by lead panel institutes. All manufacturing steps and assays followed EN ISO 13485-certified standard operating procedures.
Cross-validation of the tissue samples for EGFR exon20ins was performed by six panel institutes based in Germany: the Institute of Tissue Diagnostics, MVZ at Helios Klinikum Emil von Behring, Berlin, the Institute of Pathology at the University Hospital Dresden, the Institute of Pathology at the University Hospital Erlangen, the Institute of Surgical Pathology at the Medical Center Freiburg, the Institute of Pathology at the University Hospital Halle (Saale) and the Institute of Pathology at the University Hospital Regensburg.
Panel institutes each received four sections of FFPE tissue mounted on glass slides: one 2 µm and two 10 µm-thick sections (clinical samples), or one 10 µm thick section in a screw cap tube (artificial samples).
For artificial liquid biopsy samples, gDNA was purified from Ashkenazim Son cells (GM24385, wt) and sheared ultrasonically to achieve a size profile of 167 ± 25 bp. Mutation sequences were spiked to achieve different variant allele frequencies (VAF) and added to the wt DNA. The DNA mix was added to DNA-free human plasma (SensID GmbH, Rostock, Germany) for a final concentration of 30 ng/ml. Functionality and allelic fraction determination were the same as for artificial FFPE samples.
Liquid biopsy reference samples were counter-tested for EGFR exon20ins by three of the six panel institutes: the Institute of Tissue Diagnostics, MVZ at Helios Klinikum Emil von Behring, Berlin, the Institute of Pathology at the University Hospital Dresden and the Institute of Clinical Pathology at the University Hospital Freiburg. Only artificial samples were used: panel institutes received 2 ml of human plasma spiked with 60 ng of fragmented wild-type or mutant DNA at various allelic fractions above 1%. To resemble patient material, fragment sizes ranged between 50 and 490 base pairs (bp), with a peak at 170 bp.
External proficiency test
Following successful cross-validation of the tissue and liquid biopsy reference samples, two external EGFR exon20ins proficiency tests were launched: one covering institutes from Germany, Austria, and Switzerland only (further referred to as “DACH”) and one covering institutes from Austria, Belgium, Estonia, France, Germany, Greece, Hungary, Ireland, Italy, Lithuania, Netherlands, Poland, Portugal, Russia, Slovakia, Switzerland, and Turkey (further referred to as “international”). One institute from Germany, which had already participated in the DACH proficiency test, re-submitted results for the liquid biopsy part of the international proficiency test. German, Austrian, and Swiss institutes taking part in the international proficiency test did not overlap with institutes participating in the DACH proficiency test. The detection method was not pre-specified by QuIP®, i.e., participating institutes were free to choose their approach to EGFR exon20ins testing. The instructions for the proficiency tests stated only the range of expected mutations (‘insertions of known significance in the region between amino acids D761 to C775’) and the minimal allelic fraction to be detected (‘The minimum allele frequency here is 1%’). Based on this information, the participants were responsible to choose a suitable molecular method that covers the range of expected mutations and provides a sufficient limit of detection.
Proficiency test specimens
Samples for the DACH and international proficiency tests differed with regard to numbers and types of EGFR exon20ins covered. For the tissue part of the DACH proficiency test, participating institutes were sent two FFPE clinical samples carrying EGFR exon20ins as well as eight artificial FFPE samples—two wildtype samples and six samples with EGFR exon20ins (Table 2). Each of the two clinical samples were sub-divided into two 10 µm-thick sections for EGFR exon20ins testing and one 2 µm-thick section for H&E staining. For artificial tissue, participating institutes received one 10 µm-thick section per sample, without a corresponding section for H&E staining. FFPE blocks derived from clinical material were sectioned by the lead panel institute, the Institute of Pathology at University Hospital Cologne, FFPE blocks derived from artificial material were prepared by SensID.
Samples for the liquid biopsy part of the DACH proficiency test comprised two wildtype samples, six samples carrying the same EGFR exon20ins as the respective artificial samples in the tissue part, and two samples with EGFR exon20ins from the sample pool but with different allelic fractions (Table 3). Reference samples were produced by SensID; participating institutes received 2 ml of human plasma spiked with 60 ng of fragmented DNA at different allelic fractions above 1%.
For the tissue part of the international proficiency test, participating institutes received five artificial FFPE samples—one wildtype sample and four samples carrying different EGFR exon20ins—each with a thickness of 10 µm (Table 4). Test sets for the liquid biopsy part comprised one wildtype sample, two samples carrying the same EGFR exon20ins as the respective artificial samples in the tissue part, and two samples with EGFR exon20ins from the sample pool but with different allelic fractions (Table 4). As before, 2 ml of human plasma were spiked with 60 ng of fragmented DNA. All samples were prepared by SensID. The international proficiency test comprised a different number of samples compared to the national proficiency test due to the limited availability of clinical samples and the cost–benefit calculation for participating institutes.
Proficiency test evaluation
For the DACH proficiency test, participating institutes were given 20 working days to perform their analyses and submit their results to the QuIP® website. Two points were awarded for each correctly identified sample (mutation detected ‘yes’ or ‘no’), resulting in a maximum score of 10 samples × 2 points = 20 points per part. If the sample could not be evaluated due to technical problems, one point was awarded per sample. The passing score for both parts was 90%, i.e., the total required score for successful participation was 18 points per part.
For the international proficiency test, participating institutes were initially given 20 working days to perform their analyses and submit their results to the QuIP® website. However, due to supply difficulties of several manufacturers reported by numerous institutes in various countries due to the corona virus pandemic, the submission deadline was later extended to 40 working days. Two points were awarded for each correctly identified sample (mutation detected ‘yes’ or ‘no’), resulting in a maximum score of 5 samples × 2 points = 10 points per part. For the international proficiency test only five samples had to be analyzed, as consequence, not one sample could be excluded from evaluation due to technical problems. Therefore, the passing score for both parts was 100% due to the low number of samples to be tested.
Data availability
The datasets generated and analyzed during the current study by next generation sequencing are available in the BIG SUB; Big submission portal repository [https://bigd.big.ac.cn/gsa-human/browse/HRA006093].
References
Vyse, S. & Huang, P. H. Targeting EGFR exon 20 insertion mutations in non-small cell lung cancer. Signal Transduct. Target Ther. 4, 5. https://doi.org/10.1038/s41392-019-0038-9 (2019).
Wang, F., Li, C., Wu, Q. & Lu, H. EGFR exon 20 insertion mutations in non-small cell lung cancer. Transl. Cancer Res. 9, 2982–2991. https://doi.org/10.21037/tcr.2020.03.10 (2020).
Arcila, M. E. et al. EGFR exon 20 insertion mutations in lung adenocarcinomas: prevalence, molecular heterogeneity, and clinicopathologic characteristics. Mol. Cancer Ther. 12, 220–229. https://doi.org/10.1158/1535-7163.MCT-12-0620 (2013).
Pacini, L. et al. Tackling drug resistance in EGFR Exon 20 insertion mutant lung cancer. Pharmgenom. Pers. Med. 14, 301–317. https://doi.org/10.2147/PGPM.S242045 (2021).
Chelabi, S. et al. EGFR Exon 20 insertion in metastatic non-small-cell lung cancer: survival and clinical efficacy of EGFR tyrosine-kinase inhibitor and chemotherapy. Cancers Basel 13, 20. https://doi.org/10.3390/cancers13205132 (2021).
Low, J. L., Lim, S. M., Lee, J. B., Cho, B. C. & Soo, R. Advances in the management of non-small-cell lung cancer harbouring EGFR exon 20 insertion mutations. Ther. Adv. Med. Oncol. 15, 1–19. https://doi.org/10.1177/17588359221146131 (2023).
Rybrevant. https://www.ema.europa.eu/en/medicines/human/EPAR/rybrevant (2023).
FDA grants accelerated approval to mobocertinib for metastatic non-small cell lung cancer with EGFR exon 20 insertion mutations. https://www.fda.gov/drugs/resources-information-approved-drugs/fda-grants-accelerated-approval-mobocertinib-metastatic-non-small-cell-lung-cancer-egfr-exon-20 (2021).
Exkivity: Withdrawal of the marketing authorisation application. https://www.ema.europa.eu/en/medicines/human/withdrawn-applications/exkivity (2022).
Baraibar, I., Mezquita, L., Gil-Bazo, I. & Planchard, D. Novel drugs targeting EGFR and HER2 exon 20 mutations in metastatic NSCLC. Crit. Rev. Oncol. Hematol. 148, 102906. https://doi.org/10.1016/j.critrevonc.2020.102906 (2020).
Sequence Variant Nomenclature—DNA recommendations. https://varnomen.hgvs.org/recommendations/DNA/ (2023).
den Dunnen, J. T. et al. HGVS recommendations for the description of sequence variants: 2016 update. Hum. Mutat. 37, 564–569. https://doi.org/10.1002/humu.22981 (2016).
EBM Gebührenordnungsposition 19461: Nachweis oder Ausschluss von allen bekannten EGFR-aktivierenden Mutationen in den Exonen 18 bis 21 mittels Flüssigbiopsie. https://www.kbv.de/tools/ebm/html/19461_2900246571064542636576.html (2023).
Ahmad-Nejad, P. et al. Current and future challenges in quality assurance in molecular diagnostics. Clin. Chim. Acta 519, 239–246. https://doi.org/10.1016/j.cca.2021.05.004 (2021).
Bauml, J. M. et al. In International Association for the Study of Lung Cancer’s (IASLC) 2020 World Conference on Lung Cancer (WCLC) (virtuell, 2021).
Yasuda, H., Kobayashi, S. & Costa, D. B. EGFR exon 20 insertion mutations in non-small-cell lung cancer: Preclinical data and clinical implications. Lancet Oncol. 13, e23-31. https://doi.org/10.1016/S1470-2045(11)70129-2 (2012).
Leal, J. L. et al. EGFR Exon 20 insertion mutations: Clinicopathological characteristics and treatment outcomes in advanced non-small cell lung cancer. Clin. Lung Cancer 22, e859–e869. https://doi.org/10.1016/j.cllc.2021.04.009 (2021).
Park, K. et al. Amivantamab in EGFR Exon 20 insertion-mutated non-small-cell lung cancer progressing on platinum chemotherapy: Initial results from the CHRYSALIS phase I study. J. Clin. Oncol. 39, 3391–3402. https://doi.org/10.1200/JCO.21.00662 (2021).
Hirose, T. et al. Extensive functional evaluation of exon 20 insertion mutations of EGFR. Lung Cancer 152, 135–142. https://doi.org/10.1016/j.lungcan.2020.12.023 (2021).
Arcila, M. E. et al. Ultrarapid EGFR mutation screening followed by comprehensive next-generation sequencing: A feasible, informative approach for lung carcinoma cytology specimens with a high success rate. JTO Clin. Res. Rep. 1, 3. https://doi.org/10.1016/j.jtocrr.2020.100077 (2020).
Mosele, F. et al. Recommendations for the use of next-generation sequencing (NGS) for patients with metastatic cancers: A report from the ESMO Precision Medicine Working Group. Ann. Oncol. 31, 1491–1505. https://doi.org/10.1016/j.annonc.2020.07.014 (2020).
List of cleared or approved companion diagnostic devices (in vitro and imaging tools). Content current as of February 2023. https://www.fda.gov/medical-devices/in-vitro-diagnostics/list-cleared-or-approved-companion-diagnostic-devices-in-vitro-and-imaging-tools (2023).
Martinez-Saez, O. et al. Frequency and spectrum of PIK3CA somatic mutations in breast cancer. Breast Cancer Res. 22, 45. https://doi.org/10.1186/s13058-020-01284-9 (2020).
Jatkoe, T. et al. Clinical validation of companion diagnostics for the selection of patients with non-small cell lung cancer tumors harboring epidermal growth factor receptor exon 20 insertion mutations for treatment with amivantamab. J. Mol. Diagn. 24, 1181–1188. https://doi.org/10.1016/j.jmoldx.2022.07.003 (2022).
Passaro, A. et al. ESMO expert consensus statements on the management of EGFR mutant Non-Small Cell Lung Cancer. Ann. Oncol. 33, 466–487. https://doi.org/10.1016/j.annonc.2022.02.003 (2022).
Tuteja, S., Kadri, S. & Yap, K. L. A performance evaluation study: Variant annotation tools—the enigma of clinical next generation sequencing (NGS) based genetic testing. J. Pathol. Inform. 13, 100130. https://doi.org/10.1016/j.jpi.2022.100130 (2022).
Keppens, C. et al. Variation in nomenclature of somatic variants for selection of oncological therapies: Can we reach a consensus soon?. Hum. Mutat. 41, 7–16. https://doi.org/10.1002/humu.23926 (2020).
Acknowledgements
Both proficiency tests—DACH and international—were organized and run by the Quality Assurance Initiative Pathology (Qualitätssicherungs-Initiative Pathologie [QuIP®]). With friendly support from Janssen-Cilag GmbH.
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
DV, FB, MAI, MGN, SMB concept and design of the proficency test RS, FH, SH, DA, WD, ME, AH, MES, AH, SL, MW, AS, TM cross-validation of experiments, supervision of experiments MAI, MGN, CH, AMS, SMB selected clinical samples and performed data analysis MGN, MAI, SMB wrote the manuscript All authors approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
Michaela A. Ihle. Consulting fees: Novartis Pharma GmbH. Payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing, or educational events: AstraZeneca GmbH (to MAI and her institution), Bristol-Myers Squibb GmbH & Co. KGaA (to MAI and to MAI’s institution), Merck KGaA (to MAI), ZytoVision GmbH (to MAI’s institution), and Janssen-Cilag GmbH (to MAI’s institution) Carina Heydt. Payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing, or educational events: Molecular Health GmbH, Illumina, Inc., Bristol-Myers Squibb GmbH & Co. KGaA, AstraZeneca GmbH, Thermo Fisher Scientific Inc. Support for attending meetings and/or travel: Covaris, LLC, Illumina, Inc., Thermo Fisher Scientific Inc. Anne Schultheis none Robert Stöhr none Florian Hallernone Sylvia Herold none Daniela Aust. Payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing, or educational events: Novartis Pharma GmbH, AstraZeneca GmbH, Pfizer Pharma GmbH. Participation on a data safety monitoring board or advisory board: Novartis Pharma GmbH, Roche Deutschland Holding GmbH Wolfgang Dietmaier none Matthias Evertnone Markus Eszlinger none Anja Haak none Silke Laßmann none for EGFR testing (subject of manuscript) Daniela Vorholt full-time employee at Janssen-Cilag GmbH Frank Breitenbücher Former full-time employee at Janssen-Cilag GmbH Martin Wernernone for EGFR testing (subject of manuscript) Anna Streubelnone Thomas Mairinger. Payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing, or educational events: Astra Zeneca GmbH, Novartis Pharma GmbH, Bristol-Myers Squibb GmbH & Co. KGaA, Lilly Deutschland GmbH, Roche Deutschland Holding GmbH, Boehringer Ingelheim Pharma GmbH & Co. KG. Participation on a data safety monitoring board or advisory board: Astra Zeneca GmbH, Novartis Pharma GmbH, Bristol-Myers Squibb GmbH & Co. KGaA, Lilly Deutschland GmbH, Roche Deutschland Holding GmbH, Boehringer Ingelheim Pharma GmbH & Co. KG Maja Grassow-Narlik full-time employee at QuIP GmbH Sabine Merkelbach-Bruse. Payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing, or educational events: AstraZeneca GmbH, QuIP GmbH, DLS, Novartis Pharma GmbH, GlaxoSmithKline GmbH & Co. KG, Janssen-Cilag GmbH, Bristol-Myers Squibb GmbH & Co. KGaA, MSD (Merck & Co., Inc.), Merck KGaA, Amgen GmbH, Bayer AG. Support for attending meetings and/or travel: Bristol-Myers Squibb GmbH & Co. KGaA. Participation on a data safety monitoring board or advisory board: Amgen GmbH, AstraZeneca GmbH, Bayer AG, Janssen-Cilag GmbH, Novartis Pharma GmbH.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ihle, M.A., Heydt, C., Schultheis, A.M. et al. Multinational proficiency tests for EGFR exon 20 insertions reveal that the assay design matters. Sci Rep 14, 13069 (2024). https://doi.org/10.1038/s41598-024-63821-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-63821-2
- Springer Nature Limited