
Abstract
Muscular strength represents a specific component of health-related fitness. Hand grip strength is used as a simple and dynamic marker of maximum voluntary force of the hand and to estimate overall strength. Today, little is known about the relationship between grip strength and health in forcibly displaced populations. In the present study, we examined whether grip strength is associated with various health outcomes in a sample of forcibly displaced people living in a Greek refugee camp. The present analyses are part of a larger pragmatic randomized controlled trial. In this paper, cross-sectional baseline data of 143 participants (71 men, 72 women) will be presented. In addition to grip strength, the following physical and mental health outcomes were assessed: body weight and body composition, blood pressure, total cholesterol, low- and high-density lipoprotein cholesterol, triglycerides, blood glucose levels (HbA1c), post-traumatic stress disorder (PTSD) symptoms, depressive and anxiety symptoms, pain, and quality of life. Linear regression analyses were carried out to examine how grip strength is associated with the health outcomes, separately for absolute and normalized grip strength scores. Grip strength was positively and strongly associated with percentage muscle mass (normalized grip strength: Stand. B = 0.58, p < .001), whereas a negative association existed for percentage body fat (normalized grip strength: Stand. B = − 0.58, p < .001). No statistically significant associations occurred between grip strength and the other cardiovascular risk markers. In contrast, we found that participants with higher normalized grip strength reported higher levels of PTSD (normalized grip strength: Stand. B = 0.36, p < .05) and depressive symptoms (normalized grip strength: Stand. B = 0.29, p < .05). No significant association occurred between grip strength, anxiety, pain and quality of life. Measuring grip strength in forcibly displaced people can be a useful way to assess their overall muscle strength. Grip strength tests are easy to implement, and results can be used to assess the effects of specific intervention measures. Nevertheless, our results question the usefulness of grip strength as a marker of cardiovascular health and mental wellbeing in a refugee camp setting.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Introduction
Muscular strength represents a specific component of health-related fitness and is defined as the ability to generate maximal muscle force1. Hand grip strength is used as a simple and dynamic marker of maximum voluntary force of the hand2, and to estimate overall strength3. In line with this, grip strength was found to be associated with arm, back and leg strength in adult populations4. More generally, poor grip strength may be understood as an indicator of weakness, fatigue, and/or malnutrition, all of which can have negative impacts on a person’s overall health and ability to perform daily tasks. Accordingly, prior research has shown that poor grip strength correlates with a variety of health-related outcomes including nutritional status5, activities of daily living6, depressive symptoms7, impaired health-related quality of life8, chronic physical conditions and physical multimorbidity9, cancer10, cardiovascular diseases11, as well as cardiovascular and all-cause mortality11,12. Interestingly, muscle strength turned out to be a better predictor of mortality than overall muscle mass13. Accordingly, grip strength has the potential to be applied as an inexpensive and easy-to-use risk-stratification method to estimate an individuals’ risk of cardiovascular disease14,15.
In the present study, we examined whether grip strength is associated with various health outcomes in a sample of forcibly displaced people living in a Greek refugee camp. As shown in previous research, refugees have a higher risk for mental health issues such as post-traumatic stress disorder (PTSD), depression, and non-communicable diseases16,17. Many of them were forcibly displaced due to war, persecution or other forms of violence, and are often left with few resources, little support, and limited access to basic necessities such as food, water and shelter18. Refugees often have limited legal rights and protections, and face an increased risk of exploitation and abuse19. Today, however, still little is known about the relationship between grip strength and health in forcibly displaced populations. For instance, one study was carried out with older Rwandan refugees living in a refugee camp in Tanzania and showed that poor grip strength is associated with poor nutritional status20. In another study, refugees from North Korea were compared with an age-matched sample of controls from South Korea showing that refugees had significantly lower grip strength scores21. However, no relationships with other health markers were reported. Thus, while the former study provides some evidence for the association between grip strength and health outcomes among refugees, more research on the relationship between grip strength and health outcomes is needed. Given that access to healthcare is often limited among forcibly displaced people living in refugee camps18, easy-to-use screening tools such as the grip strength test could be valuable in identifying people who are at particularly high risk to face physical and mental health challenges.
Given this background, the overall purpose of the present study was to examine whether in a diverse sample of forcibly displaced people living in a refugee camp in Greece, grip strength would be associated with various health outcomes, including cardiorespiratory fitness (VO2max), body composition (percentage muscle mass and body fat), blood pressure, blood lipids (cholesterol, triglycerides), blood glucose, symptoms of PTSD, depression and generalized anxiety disorder, pain, and quality of life. To this end, different analyses were performed:
First, we examined associations between absolute grip strength scores and the assessed health measures, after controlling for age, sex, and body mass index (BMI). With regard to age, research has shown that grip strength increases through childhood and adolescence22,23 and peaks around the age of 40 years. After that, grip strength declines in a relatively linear way2 due to various ageing-related factors such as a decline in muscle mass and strength, changes in joint mobility and flexibility, and changes in the nervous system. With regard to sex, grip strength proved to be higher in men than in women24. However, grip strength can vary greatly between individuals of the same sex, and there is considerable overlap between grip strength of men and women25. After puberty, there is an exponential progression in muscle strength among boys, which has been ascribed to the increase of testosterone among boys26, and the increase of body fat among girls22,27.
Second, we examined associations between grip strength and health outcomes after normalization of grip strength scores. Normalization of grip strength is a process that involves adjusting the grip strength measurement to account for individual differences in body weight and height28,29. Normalization for participants’ BMI could be relevant because normalized grip strength turned out to be more closely associated with health outcomes than absolute grip strength30.
Third, we examined whether participants who fall below or exceed specific grip strength cut-points differ in the assessed health outcomes. While cut-points can vary depending on the population being studied and the purpose of the measurement2,31, we used cut-points that have previously been applied in participants in low-to-middle-income countries (LMICs)9.
Based on previous investigations, our hypotheses were that men would report higher grip strength than women (Hypothesis 1)24,25. We further assumed that the relationship between grip strength and age would be curvilinear with a peak around the age of 40 years (Hypothesis 2)2. As strength and cardiovascular fitness reflect different fitness components32, we only expected weak positive associations between grip strength and VO2max (Hypothesis 3)33,34. Regarding the association between grip strength and the various health outcomes, we expected that higher grip strength would be associated with higher muscle mass35, lower fat mass36, lower cardiovascular risk37,38, and better mental health (Hypothesis 4)7,39. While we expected similar associations for absolute and normalized grip strength scores40, we expected slightly stronger associations for normalized compared to absolute grip strength (Hypothesis 5)30.
Methods
Participants and procedures
The present analyses are part of a larger pragmatic randomized controlled trial (RCT)41. In this paper, cross-sectional baseline data will be presented. Ethical approval was obtained from the local ethical review boards, and all procedures were performed in accordance with the relevant guidelines and regulations, including the ethical principles of the Declaration of Helsinki and the guidelines of Good Clinical Practice (GCP). The study took place in a remote area in Central Greece in a refugee camp, which is under the governance of the Ministry of Migration and Asylum. In the camp, residents live in containers (equipped with a bathroom and kitchen), either together with family members or with max. four people of the same sex and origin. The residents spend most of their time in the camp. Due to legal barriers, they are not allowed to work. Leisure activities are scarce, and the remote location makes it difficult to escape the camp's daily routine.
Participants were eligible if they met the following inclusion criteria: (a) living in the selected refugee camp, (b) 16–59 years old, (c) able to read in English, Arabic, Farsi, or French, and (d) provided written informed consent. The focus of the present study was on older adolescents and adults. Minors (children and younger adolescents < 16 years) were excluded to ensure cognitive understanding of the items included in the psychological questionnaires. Older adults (> 60 years of age) were excluded to facilitate the implementation of the intervention due to decreasing fitness among elderly people32. A screening was performed with potentially eligible households to draw a random sample stratified by sex. For the RCT, the minimal estimated sample size was 136 participants to demonstrate an intervention effect on PTSD symptoms41.
The screening, recruitment, and data assessment took place in May 2021 by the research team together with 10 trained research assistants who were familiar with the residents' cultural background and the camp's contextual setting. Both written and verbal information were given to the participants in their native languages, and participants provided written informed consent before the first data assessment. All participants were assured that participation is voluntary, and that withdrawal is possible at any time without any disadvantages, particularly with regard to the asylum process. The 10 research assistants were recruited from the camp population and had to be diverse in sociodemographic background (sex and origin) and fluent in English and one of the other languages used in the study. Research assistants received training on the study's purpose and the practical and theoretical elements of data collection and translation (e.g., verbatim translation and confidentiality). Given their familiarity with camp residents’ cultural backgrounds and the camp's contextual environment, the research assistants played an important role in interacting with residents, explaining study procedures, obtaining informed consent, performing translation tasks, and aiding in data collection. Data assessment was carried out at the nearby Department of Physical Education and Sport Science. Participants received information about their results after completion of the assessment and were referred to a specialist in case of a potential health risk. As further incentives, participants received a meal and some sport equipment.
Measures
For reasons of space, the instruments are only briefly described here. More detailed information can be found in the published study protocol41. Table 1 provides information about the internal consistency of the measurements in the present sample.
To assess upper-body muscle strength, the Grip Strength Test was applied42, using a hydraulic hand dynamometer (Saaehan, Tisselt, Belgium). Participants held their arm in a position at a 90° angle, while being seated and an upright and relaxed position. Participants performed six trials, with 30-s resting periods between trials and alternating between the left and right hand. Data was recorded in kg (to the nearest of 1 kg). The Grip Strength Test has been previously applied in refugee studies20. Weak grip strength was defined as < 30 kg for men and < 20 kg for women9, using the mean score of all six measurements.
Body weight and body composition were assessed with a digital weighing scale (BC-545, Tanita, USA) that also allowed bioelectrical impedance analysis to measure the percentage of body fat and muscle mass. Body height was assessed with a stadiometer. Blood pressure was assessed with an Omron® digital blood pressure monitor, after participants had rested for 5 min in a seated position43. Finger prick methodology was used to obtain capillary blood samples. Total cholesterol, low- (LDL) and high-density (HDL) lipoprotein cholesterol, triglycerides and blood glucose levels (HbA1c) were analysed via Afinion 2 analysers (Abbott, Wädenswil, Switzerland). Afinion 2 point-of-care (PAC) analyser results correspond well with laboratory tests for both lipid levels and HbA1c44,45.
All psychological measures were assessed with instruments that have been previously used with forcibly displaced adults46,47,48,49. Given that many participants had limited English skills, the questionnaires were available in English, Arabic, Farsi, and French language, and translators supported the data assessment process. All instruments have been validated previously in English, Arabic, Farsi, and French41, and the scales had acceptable or good internal consistency (Cronbach’s alpha > 0.7) in our pilot study50. PTSD symptoms were measured with the 22-item Impact of Event Scale-Revised (IES-R)51, which refers to DSM-552 and ICD-1053 criteria of PTSD. Answers were given on a five-point Likert scale from 0 (not at all) to 4 (extremely), resulting in an overall index between 0 and 88 points. Depressive symptoms were measured with the 9-item Patient Health Questionnaire (PHQ-9)54, which refer to DSM-5 criteria for major depression52. Answers were given on a four-point Likert scale from 0 (not at all) to 3 (nearly every day), with overall scores varying between 0 and 27. Anxiety symptoms were measured with the 7-item General Anxiety Disorder scale (GAD-7)55, which refers to DSM-5 criteria for generalized anxiety disorder52. Answers were given on a four-point Likert scale from 0 (not at all) to 3 (nearly every day), with overall scores ranging between 0 to 21. Pain was measured with the 5-item Visual Analogue Scale for Pain (VAS)56, which asked for pain over the last week in the head, back, chest, stomach, arms and legs. Item scores ranged from 0 (no pain) to 100 (pain as bad as it could be) and the average was calculated, to build a total index between 0 and 100. Quality of life was measured with the 5-item World Health Organization (WHO) Index57. Answers were given on a Likert scale from 0 (at no time) to 5 (all the time). Items are summed up and multiplied by 4, resulting in an overall index between 0 and 10058.
Statistical analyses
Descriptive statistics (n, %, M, SD, Min, Max, Skew, Kurt) are presented to describe the characteristics of the sample and distribution of the study variables. Associations with sex and age were tested via analyses of covariance (ANCOVAs), chi2-tests, and (linear/quadratic) regression analyses. Linear regression analyses were carried out to examine how grip strength is associated with the health outcomes, separately for absolute and normalized grip strength scores. Age and sex were used as covariates if normalized grip strength was used as independent variable. Beyond age and sex, BMI was considered as additional covariate in the analyses with absolute grip strength as independent variable. Multicollinearity was examined via variance inflation factor (VIF) scores. Two-way ANCOVAs were used to test differences between participants with weak grip strength and their stronger counterparts. In these analyses, grip strength was used as independent variable, and sex was conceptualized as moderating variable. To examine whether sex moderates the relationship between grip strength and the dependent variables, the interaction term was included. Age and BMI were considered as covariates. All analyses were carried out with SPSS version 28 for Mac (IBM Corporation, Armonk, USA), and the level of significance was set at p < 0.05 across all analyses.
Ethics approval and consent to participate
All procedures were approved by the Research Ethics Committee of the University of Thessaly, ref approval no. 39 (date of approval: 19/11/2020), the Ethics Com-mittee of the Department of Physical Education & Sport Science, ref approval no. 1701 (date of approval: 09/12/ 2020) and the ethical review board of Northwest and Central Switzerland, ref approval no. AO_2020-00036 (date of approval: 26/11/2020). Prior to data assessment, all participants signed written informed consent.
Results
Sample characteristics
In total, 150 participants (76 men, 74 women) had valid grip strength measurements. However, 7 participants did not have valid data for age, and were therefore excluded from the further data analyses. The remaining sample of 143 participants was composed of 71 men and 72 women, with a mean age of M = 29.00 years (SD = 9.32) and a mean BMI of M = 25.83 kg/m2 (SD = 5.27) (see Table 1). On average, participants were away from their home country for M = 34.68 months (SD = 38.05), and lived for M = 14.67 months (SD = 10.14) in the camp where the current study took place. The following countries of origin were reported n: Afghanistan (n = 71), Cameroon (n = 1), Congo (n = 18), Guinea (n = 1), Iraq (n = 3), Iran (n = 8), Pakistan (n = 1), Sierra Leone (n = 2), Somalia (n = 21), Syria (n = 12) and Turkey (n = 2) (did not answer: n = 3). Most of the participants completed the survey in Farsi (n = 83), followed by Arabic (n = 31), French (n = 21) and English (n = 8). With regard to educational background, 35 participants reported not to have formal education, 51 completed primary school, 33 high school and 20 completed higher education (university) (did not answer: n = 4).
Descriptive statistics
Table 1 shows the descriptive statistics for all metric study variables. With the exception of one variable (months away from home), none of the variables showed major deviations from normality (defined as Skew > 2 and/or Kurt > 7)59. The internal consistency was good for grip strength, blood pressure and across all mental health outcomes.
Association of grip strength with sex and age
With regard to sex, after controlling for age and BMI, ANCOVAS showed that men (M = 35.42 kg, SD = 6.95) achieved higher absolute grip strength scores than women (M = 19.58 kg, SD = 5.04), F(1,142) = 245.43, p < 0.001, η2 = 0.638. A similar sex effect was found for normalized grip strength, after controlling for age, F(1,142) = 249.91, p < 0.001, η2 = 0.641. In line with this, chi2-analyses revealed that women (43.1%) were more likely to be classified into the group with weak grip strength than men (25.4%), χ2(1,143) = 4.97, p < 0.05, ϕ = 0.183.
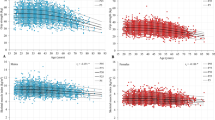
With regard to age, after controlling for sex and BMI, linear regression analyses showed that age was neither associated with absolute (β = − 0.068, p = 0.231) nor normalized grip strength (β = − 0.076, p = 0.131). As shown in Fig. 1, the use of quadratic regression did not result in statistically significant relationships. Finally, after controlling for sex and BMI, participants with weak grip strength (M = 27.88 years, SD = 9.00) did not differ in age from their stronger counterparts (M = 29.59, SD = 9.47), F(1,142) = 0.17, p = 0.685, η2 = 0.001.

Association between grip strength and age.
Associations between absolute grip strength and health outcomes
Table 2 shows that there was no statistically significant association between absolute grip strength and estimated VO2max (β = 0.100, p = 0.402). In turn, a positive association was found for percentage muscle mass (β = 0.204, p < 0.001), whereas a negative relation existed for percentage body fat (β = -0.208, p < 0.001). Absolute grip strength was not statistically significantly associated with any of the cardiovascular risk markers, but with more PTSD symptoms (β = 0.304, p < 0.05) and more depressive symptoms (β = 0.231, p < 0.05).
Table 2 further shows that women had significantly lower VO2max, lower muscle mass, higher percentage body fat, and lower blood pressure. Moreover, women reported higher symptoms of PTSD, depression, anxiety, and pain, whereas they had lower ratings on quality of life. Age was negatively associated with VO2max, whereas a positive association existed with nearly all cardiovascular risk markers (with the exception of HDL cholesterol). Older participants also reported higher symptoms of PTSD, depression, anxiety and pain. Finally, BMI was negatively associated with VO2max and muscle mass, whereas positive associations existed with percentage body fat and nearly all cardiovascular risk markers (except HDL cholesterol). In turn, participants with higher BMI reported lower symptoms of PTSD and depression.
Associations between normalized grip strength and health outcomes
The pattern for normalized grip strength was similar to that described previously for the absolute values (Table 3), but some of the associations were stronger. Relatively strong associations were observed for both percentage muscle mass (β = 0.575, p < 0.001, Fig. 2A) and body fat (β = − 0.582, p < 0.001; Fig. 2B). Normalized grip strength was also positively associated with VO2max (β = 0.286, p < 0.05). Finally, higher normalized grip strength was associated with more symptoms of PTSD (β = 0.363, p < 0.05) and depression (β = 0.292, p < 0.05). No statistically significant associations were found for the remaining health outcomes.

Association between normalized grip strength and percentage muscle mass (A) and body fat (B).
Differences in health outcomes between participants with low vs. higher grip strength
Table 4 confirms differences in body composition between participants with weak grip strength and their stronger counterparts, with the former having lower muscle mass and higher fat mass. Participants with weak grip strength also report lower scores for PTSD, depression and pain. No statistically significant differences were found for VO2max and the cardiovascular risk markers. Whereas the previously described sex differences were corroborated in the ANCOVAs, no statistically significant interactions were observed between grip strength and sex for any of the outcomes.
Discussion
The key findings of the present study are that in a diverse sample of forcibly displaced people living in a Greek refugee camp, grip strength was positively associated with percentage muscle mass, whereas a negative association existed for percentage body fat. No statistically significant associations occurred between grip strength and cardiovascular risk markers. In contrast, we found that participants with higher normalized grip strength reported higher levels of PTSD and depressive symptoms.
Five hypotheses were formulated, and each of these will now be discussed separately. Our first hypothesis claimed that men would report higher grip strength than women. In line with previous research24,25, this hypothesis was supported and similarly strong effects were found for absolute and normalized grip strength scores (approximately 64% of explained variance).
In contrast, our second hypothesis, which suggested a curvilinear relationship between grip strength and age with a peak around the age of 40 years, was not supported by our empirical data. This contrasts with previous research in younger populations showing that muscle strength increases from childhood to younger adulthood due to changes in muscle mass and muscle fiber size3. Whereas we found an increase in grip strength until the age of 30 years, the quadratic regression model did not reach statistical significance. One reason for the absence of a statistically significant relationship might be that due to our inclusion criteria, all participants were between 16 and 59 years of age, whereas the age-related increase in grip strength is strongest during childhood and early adolescence2, and the strongest decline occurs after the age of 60 years60,61. Thus, excluding younger and older participants may have resulted in a relatively flat curve.
Our third hypothesis assumed a weak positive association between grip strength and cardiorespiratory fitness. This hypothesis was supported in the sense that higher VO2max was associated with higher normalized grip strength. However, no statistically significant relation was found for absolute grip strength, or when participants with weak grip strength were compared to their stronger counterparts. This is in line with the conceptual idea that muscle strength and cardiorespiratory fitness represent clearly distinguishable components of physical fitness32, and that muscular strength and cardiorespiratory fitness are independent predictors of health-related quality of life62 and mortality63. Our data also support previous research showing that after controlling for relevant confounders, only weak associations existed between grip strength and VO2max33,61.
Our fourth hypothesis focused on the association between grip strength and the various health outcomes. Our findings were mixed and did not fully support a general relation between these variables. Expectedly, higher grip strength was associated with higher relative muscle mass. This is in line with previous investigations showing that grip strength is a good indicator of both whole- and upper-body muscular strength3,64. In contrast, a negative association was observed between grip strength and percentage body fat, which corroborates previous research showing that overweight and obese people often achieve lower grip strength values65. This finding might seem paradoxical as overweight and obese people have greater (absolute) muscle mass, which in turn is associated with muscle strength66,67. Furthermore, overweight and obesity might induce a certain training effect via weight bearing, which can strengthen the muscles. However, this effect might be more obvious for the lower extremities68. On the flipside, overweight and obese people tend to engage in more sedentary activities and less physical activity69,70. Overweight and obesity may also induce pain, which can have a negative impact on the performance in muscle strength tests71. Studies also showed that there are differences in muscles between overweight/obese and normal weight people. Thus, while the former have fewer type I muscles, they seem to possess more type IIb muscle fibres72.
The fact that we did not observe any statistically significant associations between grip strength and the cardiovascular risk markers was unexpected and contrasts with a relatively large body of previous studies, in which higher grip strength scores were associated with more favourable cardiovascular risk profiles, fewer cardiovascular diseases and lower risk of cardiovascular mortality37,38,73,74. Accordingly, previous studies showed that lower grip strength is associated with higher risk of hypertension75, metabolic syndrome30,38, and diabetes75,76. A recent meta-analysis further showed that accounting for cardiovascular risk factors attenuated the relationship between grip strength and mortality11. The reason why this association was not supported in our sample is not clear. Our assumption is that other factors that were not systematically assessed in the present study (e.g. dietary behaviour) may have had a stronger influence on cardiovascular risk markers, and thus have overlaid the relationships observed in other populations.
Finally, prior investigations have shown close links between grip strength and mental health outcomes, indicating that people with higher grip strength report better general health perceptions77, better health-related quality of life8,39, and less depressive symptoms7,78. The associations with the above mental health outcomes have been attributed to stronger declines in physical functioning among people with lower grip strength through an association with adverse health behaviours (e.g., dietary behavior, physical activity), increased frailty, limitations in activities of daily living, and or social isolation79. It is also believed that muscle contraction increases the release of cytokines and myokines into the circulation, which in turn can decrease the risk of mental health issues80. Moreover, it has been argued that sarcopenia might be related with inflammatory profiles that are associated with an increased risk of mental health problems80. In marked contrast to these findings, our results showed that participants with higher grip strength reported more symptoms of PTSD and depression, whereas no statistically significant associations were found with anxiety and quality of life. Again, these relationships were unexpected, and we can only speculate about the underlying reasons. One possible explanation is that grip strength is associated with higher levels of sensation seeking81, which can lead to participants being more willing to take risks before and during the flight or while living in the refugee camp; this in turn, can increase their individual risk to be exposed to traumatic experiences. Alternatively, it could also be that people with higher grip strength have more confidence in their physical ability. Such people may feel capable of a more difficult flight, which in turn increases the risk of traumatic experiences. Accordingly, the underlying mechanism would not be an increased willingness to take risks, but rather a higher level of confidence in one's own (physical) abilities. A further alternative explanation could be that being stuck in a refugee camp is a frustrating (and sometimes traumatising) experience82,83. Since in Greece camp residents are not given the opportunity to pursue a gainful employment, the level of frustration might be particularly pronounced among residents who feel strong and fit.
Our fifth hypothesis was generally supported. Thus, the relationships between grip strength and the various health outcomes pointed in the same direction independent on whether absolute or normalized grip strength were used, or whether comparisons were made between participants with weak versus higher grip strength. In line with previous research30, however, our data showed that some associations were stronger for normalized scores. Currently, researchers still do not agree on whether grip strength should be adjusted for body mass. While some experts recommend this procedure28,29, others criticize that normalization might lead to overscaling and simply reverse what was a positive correlation between body mass and the scaled variable into a negative relationship29. However, such an inversion was not observed in the present sample, which corresponds well with UK Biobank data (based on more than 350′000 participants), where grip strength was associated with health outcomes, independent of whether grip strength was expressed in absolute (kg) or in relative terms (with reference to height/ weight, fat-free mass, BMI, Fat-free mass index, or as z-scores40.
The strengths of our paper are that we focused on a so-far under-researched vulnerable population, that both physical and mental health outcomes were addressed, and that grip strength was assessed repeatedly with both the dominant and non-dominant hand. Potential limitations are that some possible influences were not assessed, which were associated with grip strength in prior studies. These factors include socioeconomic status84, smoking85, dietary behaviour86,87, and time of the day88. Because our data are cross-sectional, we also acknowledge that no causal conclusions are possible11. While we applied grip strength cut-offs that were previously used with participants from LMICs, it is difficult to generalize grip strength norms across populations2,89. For instance, as shown by Dodds et al.31, grip strength scores are significantly higher in participants from industrialized to less industrialized countries. While we were able to control motivation during the assessment of cardiorespiratory fitness by using a sub-maximal fitness test, this was not possible for the grip strength test. Thus, although support for the internal consistency of the grip strength assessments was found, performance motivation might have influenced the results. Finally, we caution against a too broad generalization of the findings beyond our sample because forcibly displaced individuals constitute a diverse population, and because health risks among forcibly displaced people can vary based on numerous sociodemographic and structural determinants, including behavioral factors, origin, migration status, duration of residence, living conditions, migration policies, and access to health services90,91.
From a practical point of view, measuring muscle strength in large populations can be complex and costly77, whereas the application of the grip strength test is non-invasive, simple to implement, inexpensive and reliable92,93. Accordingly, assessments are quickly obtainable by a range of different health professionals94, and hand grip strength is often used in diagnostic algorithms for sarcopenia77. Additionally, the grip strength test can not only be used in adults, but also proved to be a suitable indicator for musculoskeletal fitness in children95,96. Accordingly, the assessment of handgrip strength is recommended by the American Academy of Medicine97 as part of school-based fitness testing and as a screening tool for adequate levels of muscle strength for bone health. Moreover, public health recommendations suggest that forcibly displaced people should engage in muscle-strengthening activities at least two hours per week. Accordingly, intervention policies should be formulated in a way so that they encourage weight training in both men and women74. Given this background, grip strength has the potential to be used as an easy-to-implement measure to assess changes in upper-body muscle strength in resource-limited settings.
Conclusions
Measuring grip strength in forcibly displaced people can be a useful way to assess their overall muscle strength and body composition. Grip strength tests are easy to implement, and results can be used to assess the effects of specific intervention measures. Nevertheless, our results question the usefulness of grip strength as a marker of cardiovascular health and mental wellbeing in a refugee camp setting.
Data availability
The datasets used and analyzed during the current study are available as supplementary online material (SPSS file and Syntax).
Abbreviations
- ANCOVAs:
-
Analyses of covariance
- BMI:
-
Body mass index
- DSM-5:
-
Diagnostic and statistical manual of mental disorders 5
- GAD-7:
-
General Anxiety Disorder scale
- HbA1c:
-
Glygated hemoglobin
- HDL:
-
High-density lipoprotein
- ICD-10:
-
International classification of diseases, 10th revision, of the World Health Organization
- IES-R:
-
Impact of Event Scale-Revised
- Kurt:
-
Kurtosis
- LDL:
-
Low-density lipoprotein
- LMICs:
-
Low-to-middle-income countries
- PAC:
-
Point-of-care
- PHQ-9:
-
Patient Health Questionnaire
- PTSD:
-
Post-traumatic stress disorder
- RCT:
-
Randomized controlled trial
- Skew:
-
Skewness
- SPSS:
-
Statistical Package for the Social Sciences
- VAS:
-
Visual Analogue Scale
- VIF:
-
Variance inflation factor
- VO2max:
-
Maximum oxygen uptake
- WHO:
-
World Health Organization
References
American College of Sports Medicine. ACSM’s Health-Related Physical Fitness Assessment Manual (Lippincott Williams & Wilkins, Philadelphia, 2013).
Wong, S. L. Grip strength reference values for Canadians aged 6 to 79: Canadian health measure survey, 2007 to 2013. Health Rep. 27, 3–10 (2016).
Wind, A. E., Takken, T., Helders, P. J. & Engelbert, R. H. Is grip strength a predictor for total muscle strength in healthy children, adolescents, and young adults?. Eur. J. Pediatr. 169, 281–287 (2010).
Wang, M., Leger, A. B. & Dumas, G. A. Prediction of back strength using anthropometric and strength measurements in healthy females. Clin. Biomech. 20, 685–692 (2005).
Norman, K., Stobäus, N., Gonzalez, M. C., Schulzke, J. D. & Pirlich, M. Hand grip strength: Outcome predictor and marker of nutritional status. Clin. Nutr. 30, 135–142 (2011).
Matsui, Y. et al. Association of grip strength and related indices with independence of activities of daily living in older adults, investigated by a newly-eveloped grip strength measuring device. Geriatr. Gerontol. Int. 14, 77–86 (2014).
Ashdown-Franks, G. et al. Handgrip strength and depression among 34,129 adults aged 50 years and older in six low- and middle-income countries. J. Affect. Disord. 243, 448–454 (2019).
Hart, P. D. Grip strength and health-related quality of life in U.S. adult males. J. Lifestyle Med. 9, 102–110 (2019).
Vancampfort, D., Stubbs, B., Firth, J. & Koyanagi, A. Handgrip strength, chronic physical conditions and physical multimorbidity in middle-aged and older adults in six lo- and middle income countries. Eur. J. Int. Med. 61, 96–102 (2019).
Celis-Morales, C. A. et al. Associations of grip strength with cardiovascular, respiratory, and cancer outcomes and all cause mortality: Prospective cohort study of half a million UK Biobank participants. BMJ. 361, k1651 (2018).
Wu, Y., Wang, W., Liu, T. & Zhang, D. Association of grip strength with risk of all-cause mortality, cardiovascular diseases, and cancer in community-dwelling populations: A meta-analysis of prospective cohort studies. JAMDA. 18, 551.e17-e35 (2017).
Ganna, A. & Ingelsson, E. 5 year mortality predictors in 498 103 UK Biobank participants: A prospective population-based study. Lancet. 386, 533–540 (2015).
Newman, A. B. et al. Strength, but not muscle mass, is associated with mortality in the health, aging and body composition study cohort. J. Gerontol. 61, 72–77 (2006).
Mearns, B. M. Hand grip strength predicts cardiovascular risk. Natl. Rev. Cardiol. 12, 379 (2015).
Leong, D. P. et al. Prognostic value of grip strength: Findings from the prospective urban rural epidemiology (PURE) study. Lancet. 386, 266–273 (2015).
Mahmood, H. N., Ibrahim, H., Goessmann, K., Ismail, A. A. & Neuner, F. Post-traumatic stress disorder and depression among Syrian refugees residing in the Kurdistan region of Iraq. Conf. Health https://doi.org/10.1186/s13031-019-0238-5 (2019).
Perini, W., Snijder, M. B., Peters, R. J. G., Stronks, K. & Kunst, A. E. Increased cardiovascular disease risk in international migrants is independent of residence duration or cultural orientation: The HELIUS study. J. Epidemiol. Community Health. 72, 825–831 (2018).
WHO. World report on the health of refugees and migrants. (Geneva: World Health Organization; 2022).
Bartolini, L. & Zakoska-Todorovska, I. Vulnerability to exploitation and abuse along the Mediterranean migration routes to Italy. In Migration in West and North Africa and across the Mediterranean: Trends, risks, development and governance (eds Fargues, P. & Rango, M.) 189–200 (International Organization for Migration, 2020).
Pieterse, S., Manandhar, M. & Ismail, S. The association between nutritional status and handgrip strength in older Rwandan refugees. Eur. J. Clin. Nutr. 56, 933–939 (2002).
Cho, S. W., Lee, S. H., Koh, E. S., Kim, S. E. & Kim, S. J. Characteristics of body composition and muscle strength of North Korean Refugees during South Korean stay. Endocrinol. Metab. 30, 551–556 (2015).
Sartorio, A., Lafortuna, C. L., Pogliaghi, S. & Trecate, L. The impact of gender, body dimension and body composition on hand-grip strength in healthy children. J. Endocrinol. Invest. 25, 431–435 (2002).
Amo-Sétien FJ, Leal-Costa C, Abajas-Bustillo R, Gonzalez-Lamuno D, Redondo-Figuero C, EXERNET Research Group. Factors associated with grip strength among adolescents: An observational study. J. Hand. Ther. 33, 96–102 (2018).
Peterson, E., Murray, W. & Hiebert, J. M. Effect of gender and exercise typoe on relative hand grip strength. J. Strength Cond. Res. https://doi.org/10.1097/01.JSC.0000367192.78257.72 (2010).
Dodds, R. M. et al. Grip strength across the life course: Normative data from twelve British studies. PLoS One 9, e113637 (2014).
Round, J. M., Jones, D. A., Honour, J. W. & Nevill, A. M. Hormonal factors in the development of differences in strength between boys and girls during adolescence: a longitudinal study. Ann. Hum. Biol. 26, 49–62 (1999).
Dore, E. et al. Gender differences in peak muscle performance during growth. Int. J. Sports Med. 26, 274–280 (2005).
Vanderburgh, P. M., Mahar, M. T. & Chou, C. H. Allometric scaling of grip strength by body mass in college-age men and women. Res. Q. Exerc. Sport 66, 80–84 (1995).
Kocher, M. H. et al. Allometric grip strength norms for American children. J. Strength Cond. Res. 33, 2251–2261 (2019).
Chun, S.-W., Kim, W. & Choi, K. H. Comparison between grip strength and grip strength divided by body weight in their relationship with metabolic syndrom and quality of life in the elderly. PLos One 14, e0222040 (2019).
Dodds, R. M. et al. Global variation in grip strength: A systematic review and meta-analysis of normative data. Age Ageing 45, 209–216 (2016).
ACSM. ACSM’s guidelines for exercise testing and prescription. (Philadelphia: Lippincott Williams & Wilkins; 2010).
Ajepe, O., Mgbemena, N., Okafor, U., Ehuwa, O. & Okeke, C. Relationship between estimated VO2max and handgrip strength in healthy young Nigerian adults. Internet J. Allied Health Sci. Pract. 20, 17 (2022).
Dag, F. G., Tas, S. & Cimen, O. B. Hand-grip strength is correlated with aerobic capacity in healthy sedentary young females. Monten. J. Sport 10, 55–60 (2021).
Lee, S. Y. Handgrip strength: An irreplaceable indicator of muscle function. Ann. Rehabil. Med. 45, 167–169 (2021).
Confortin, S. C. et al. Are fat mass and lean mass associated with grip strength in adolescents?. Nutrients https://doi.org/10.3390/nu14163259 (2022).
Gubelmann, C., Vollenweider, P. & Marques-Vidal, P. Association of grip strength with cardiovascular risk markers. Eur. J. Prev. Cardiol. 24, 514–521 (2017).
Sayer, A. A. et al. The relationship between grip strength and features of the metabolic syndrome: Findings from the hertfordshire cohort study. QJM. 100, 707–713 (2007).
Kim, J.-H. Effect of grip strength on mental health. J. Affect. Disord. 245, 371–376 (2019).
Ho, F. K. W. et al. The association of grip strength with health outcomes does not differ if grip strength is used in absolute or relative terms: A prospective cohort study. Age Ageing 48, 683–691 (2019).
Gerber, M., Colledge, F., de Quervain, D., Filippou, K., Havas, E., Knappe, F., et al. Effects of an exercise and sport intervention among refugees living in a Greek refugee camp on mental health, physical fitness and cardiovascular risk markers: study protocol for the SALEEM pragmatic randomized controlled trial. Trials. 22, (2021).
Council of Europe. Testing physical fitness: Eurofit experimental battery. Strasbourg: Council of Europe; (1983).
Ostchega, Y., Nwankwo, T., Sorlie, P. D., Wolz, M. & Zipf, G. Assessing the validity of the Omron HEM-907XL oscillometric blood pressure measurement device in a national survey environment. J. Clin. Hypertens. 12, 22–28 (2009).
Abbai, N. S., Nyirenda, M., Reddy, T. & Ramjee, G. Good correlation between the Afinion AS100 analyser and the ABX Pentra 400 analyser for the measurement of glycosylated haemoglobin and lipid levels in older adults in Durban, South Africa. S. Afr. Med. J. 108, 50–55 (2018).
Foerster, V. & Severn, M. Point-of-care glycated hemoglobin testing to diagnose type 2 diabetes. Issues Emerg. Health Technol. 156, 1–8 (2016).
Morina, N., Ehring, T. & Priebe, S. Diagnostic utility of the impact of event scale–revised in two sample of survivors of war. PLoS One https://doi.org/10.1371/journal.pone.0083916 (2013).
Feyera, F., Mihretie, G., Bedaso, A., Gedle, D. & Kumera, G. Prevalence of depression and associated factors among Somali refugee at Melkadida camp, southeast Ethiopia: A cross-sectional study. BMC Psychiatry. 15, 211. https://doi.org/10.1186/s12888-015-0539-1 (2015).
Hermansson, A. C., Thyberg, M., Timpka, T. & Gerdle, B. Survival with pain: An eight-year follow-up of war-wounded refugee. Med. Confl. Surviv. 17, 102–111 (2001).
Sundquist, J., Hagströmer, M., Johansson, S. E., Sundquist, K. Effect of a primary health-care-based controlled trial for cardiorespiratory fitness in refugee women. BMC Fam. Pract. (2010). 11. 10.1471-2296/11/55.
Knappe, F., Colledge, F. & Gerber, M. Impact of an 8-week exercise and sport intervention on post-traumatic stress disorder symptoms, mental health, and physical fitness among male refugees living in a Greek refugee camp. Int. J. Environ. Res. Public Health 16, 20. https://doi.org/10.3390/ijerph16203904 (2019).
Weiss, D. S. & Marmar, C. R. The Impact of Event Scale—Revised. In Assessing psychological trauma and PTSD (eds Wilson, J. P. & Keane, T. M.) 399–411 (Guilford Press, New York, 1997).
American Psychiatric Association. Diagnostic and statistical manual of mental disorders 5 (DSM-5). 5th edition ed. Washington: APA; (2013).
WHO. ICD-10: International statistical classification of diseases and related health problems: Tenth revision, 2nd ed. World Health Organization. Geneva: World Health Organization; (2004).
Kroenke, K. & Spitzer, R. L. The PHQ-9: A new depression diagnostic and severity measure. Psychiatr. Ann. 32, 509–515 (2002).
Spitzer, R. L., Kroenke, K., Williams, J. B. W. & Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Int. Med. 166, 1092–1097 (2006).
Carlsson, A. M. Assessment of chronic pain. I. Aspects of the reliability and validity of the Visual Analogue Scale. Pain. 16, 87–101 (1983).
Blom, E. H., Bech, P., Högberg, G., Larsson, J. O. & Serlachius, E. Screening for depressed mood in an adolescent psychiatric context by brief self- assessment scales—testing psychometric validity of WHO-5 and BDI-6 indices by latent trait analyses. Health Qual. Life Outcoes 10, 149 (2012).
WHO. Wellbeing measures in primary health care/the DepCare Project. Report on a WHO meeting: Stockholm, Sweden, 12–13 February 1998: Regional Office for Europe. Geneva: World Health Organization. (1998).
West, S. G., Finch, J. F. & Curran, P. J. Structural equation models with nonnormal variables: Problems and remedies. In Structural equation modeling Concepts, issues, and applications (ed. Hoyle, R. H.) 56–75 (Sage, 1995).
Kuh, D., Hardy, R., Blodgett, J. M. & Cooper, R. Developmental factors associated with decline in grip strength from midlife to old age: A British birth cohort study. BMJ Open 9, e025755 (2019).
Pratt, J. et al. Grip strength performance from 9431 participants of the GenoFit study: Normative data and associated factors. Geroscience. 43, 2533–2546 (2021).
Appelqvist-Schmidlechner, K. et al. Muscular and cardiorespiratory fitness are associated with health-related quality of life among young adult men. BMC Public Health https://doi.org/10.1186/s12889-020-08969-y (2020).
Kim, Y. et al. The combination of cardiorespiratory fitness and muscle strength, and mortality risk. Eur. J. Epidemiol. 33, 953–964 (2018).
Trosclair, D. et al. Hand-grip strength as a predictor of muscular strength and endurance. J. Strength Cond. Res. https://doi.org/10.1097/01.JSC.0000395736.42557.bc (2011).
Park, K. N. & Kim, S. H. Comparison of grip strength, gait speed, and quality of life among obese, overweight, and nonobese older adults: A cross-sectional study. Top Geriatr. Rehabil. 38, 88–92 (2022).
Harris, T. Muscle mass and strength: relation to function in population studies. J. Nutr. 127, 1004S-S1006 (1997).
Hulens, M. et al. Study of differences in peripheral muscle strength of lean versus obese women: An allometric approach. Int. J. Obes. Relat. Metab. Disord. 25, 676–681 (2001).
Rolland, Y. et al. Muscle strength in obese elderly women: Effect of recreational physical activity in a cross-sectional study. Am. J. Clin. Nutr. 79, 552–557 (2004).
Cleven, L., Krell-Roesch, J., Nigg, C. R. & Woll, A. The association between physical activity with incident obesity, coronary heart disease, diabetes and hypertension in adults: A systematic review of longitudinal studies published after 2012. BMC Public Health https://doi.org/10.1186/s12889-020-08715-4 (2020).
Silveira, E. A. et al. Sedentary behavior, physical inactivity, abdominal obesity and obesity in adults and older adults: A systematic review and meta-analysis. Clin. Nutr. ESPEN 50, 63–73 (2022).
Norman, K., Stobäus, N., Cristina Gonzalez, M., Schulzke, J.-D. & Pirlich, M. Hand grip strength: Outcome predictor and marker of nutritional status. Clin. Nutri. 30, 135–142 (2011).
Tanner, C. J. et al. Muscle fiber type is associated with obesity and weight loss. Am. J. Physiol. Endocrin. ol Metab. 282, E1191–E1196 (2002).
Celis-Morales, C. A. et al. Associations between diabetes and both cardiovascular disease and all-cause mortality are modified by grip strength: Evidence from UK Biobank, a prospective population-based cohort study. Diabetes Care 40, 1710–1718 (2017).
Kim, Y. et al. Independent and joint associations of grip strength and adiposity with all-cause and cardiovascular disease mortality in 403’199 adults: The UK Biobank study. Am. J. Clin. Nutr. 106, 773–782 (2017).
Mainous, A. G. I., Tanner, R. J., Anton, S. D. & Jo, A. Grip strength as a marker of hypertension and diabetes in healthy weight adults. Am. J. Prev. Med. 49, 850–858 (2015).
Ntuk, U. E. et al. Association between grip strength and diabetes prevalence in black, South-Asian, and white European ethnic groups: a cross-sectional analy- sis of 418 656 participants in the UK Biobank study. Diabetes Med. 34, 1120–1128 (2017).
Jang, S.-K. & Kim, J.-H. Association between hand grip strength and self-rated health in middle- and old-aged Korean citizens. Korean J. Fam. Med. 41, 53–60 (2020).
McDowell, C. P., Gordon, B. R. & Herring, M. P. Sex-related differences in the association between grip strength and depression: Results from the Irish longitudinal study of ageing. Exp. Gernontol. 104, 147–152 (2018).
Smith, L. et al. The association of grip strength with depressive symptoms and cortisol in hair: A cross-sectional study of older adults. Scand. J. Med. Sci. Spor. 29, 1604–1609 (2019).
Marques, A. et al. Grip strength and depression symptoms among middle-age and older adults. Mayo. Clin. Proc. 95, 2134–43 (2020).
Fink, B., Hamdaoui, A., Wenig, F. & Neave, N. Hand-grip strength and sensation seeking. Pers. Individ. Diff. 49(7), 789–793 (2010).
Perez-Sales, P., Galan-Santamarina, A., Zunzunegui, M. V. & Lopez-Martin, S. Refugee camps as torturing environments-An analysis of the conditions in the Moria reception center (Greece) based on the torturing environment scale. Int. J. Environ. Res. Public Health https://doi.org/10.3390/ijerph191610233 (2022).
Syam, H. et al. With every passing day I feel like a candle, melting little by little. Experiences of long-term displacement amongst Syrian refugees in Shatila, Lebanon. Conf. Health 13, 22. https://doi.org/10.1186/s13031-019-0228-7 (2019).
Thorpe, R. J. J., Simonsick, E., Zonderman, A. & Evans, M. K. Association between race, poverty status and grip strength in middle to old age adults. Ethn. Dis. 26, 493–500 (2016).
Ramirez-Velez, R., Tordecilla-Sanders, A., Correa-Bautista, J. E., Peterson, M. D. & Garcia-Hermoso, A. Handgrip strength and ideal cardiovascular health among Colombian children and adolescents. J. Pediatr. 179, 82–89 (2016).
Kim, H. R. & Kwon, O. Higher diet quality is associated with lower odds of low hand grip strength in the Korean elderly population. Nutrients 11, 1487 (2019).
Kuczmarski, M. F., Pohlig, R. T., Shupe, E. S., Zonderman, A. B. & Evans, M. K. Dietary protein intake and overall diet quality are associated with handgrip strength in African American and white adults. J. Nutr. Health Aging 22, 700–709 (2018).
Jasper, I., Häussler, A., Baur, B., Marquardt, C. & Hermsdörfer, J. Circadian variations in the kinematics of handwriting and grip strength. Chronobiol. Int. 26, 576–594 (2009).
Innes, E. Handgrip strength testing: A review of the literature. Aust. Occup. Ther. J. 46, 120–140 (1999).
Nisar, M., Uddin, R., Kolbe-Alexander, T. & Khan, A. The prevalence of chronic diseases in international immigrants: A systematic review and meta-analysis. Scan J. Public Health. 51, 442–453 (2023).
Agyemang, C. & van den Born, B.-J. Cardiovascular health and disease in migrant populations: A call to action. Nat. Rev. Cardiol. 19, 1–2 (2022).
Gasior, J. S., Pawlowski, M., Williams, C. A., Dabrowski, M. J. & Rameckers, E. A. Assessment of maximal isometric hand grip strength in school-aged children. Open Med. 13, 22–28 (2018).
Roberts, H. C. et al. A review of the measurement of grip strength in clinical and epidemio- logical studies: Towards a standardised approach. Age Ageing. 40, 423–429 (2011).
Ploegmakers, J. J., Hepping, A. M., Geertzen, J. H., Bulstra, S. K. & Stevens, M. Grip strength is strongly associated with height, weight and gender in childhood: A cross sectional study of 2241 children and adolescents providing reference values. J. Physiotherap. 59, 255–261 (2013).
Ruiz, J. R. et al. Field-based fitness assessment in young people: the ALPHA health-related fitness test battery for children and adolescents. Br. J. Sports Med. 45, 518–524 (2011).
Ortega, F. B. et al. Systematic review and proposal of a field-based physical fitness-test battery in preschool children: The PREFIT battery. Sports Med. 45, 533–555 (2015).
Institute of Medicine. Fitness Measures and Health Outcomes in Youth (National Academies Press, Washington, 2012).
Acknowledgements
We thank the Hellenic Army and the Ministry of Migration and Asylum for supporting this study. We also thank all other non-governmental organizations in the Koutsochero refugee camp for their cooperation. Finally, we thank all participants, translators, coaches and data assessors for their valuable contribution to this study.
Funding
This study is partly funded by the Swiss Network for International Studies (SNIS). The funding source has no influence on the design of the study, the collection, management, analysis and interpretation of the data, the writing of the manuscript or on the selection of the journal.
Author information
Authors and Affiliations
Contributions
M.G., K.F., F.K., I.D.M., E.T., E.H., H.S., F.C., S.L., M.M., Y.T., R.v.K., U.P., and A.H. were involved in the design of the study or contributed to the refinement of methods. A.H., I.D.M. and M.G. supervised the study. F.K. and K.F. coordinated the fieldwork. M.G. analyzed the data and drafted the initial manuscript. K.F., F.K., I.D.M., E.T., E.H., H.S., F.C., S.L., M.M., Y.T., R.v.K., U.P., and A.H. contributed to revising and editing the final manuscript. F.C. carried out the final language check. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Gerber, M., Filippou, K., Knappe, F. et al. Associations between grip strength, cardiorespiratory fitness, cardiovascular risk and mental health in forcibly displaced people from a Greek refugee camp. Sci Rep 13, 20970 (2023). https://doi.org/10.1038/s41598-023-48032-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-48032-5
- Springer Nature Limited