
Abstract
Rapid eating has been demonstrated to be associated with obesity and overweight. However, few studies have characterized the separate relationships of eating speed with visceral and subcutaneous fat mass or circulating adiponectin concentration. We hypothesized that rapid eating is associated with the larger visceral fat tissue (VFT) area and lower adiponectin concentration, but not with the subcutaneous fat tissue (SFT) area in men and women. We performed a cross-sectional study of 712 adults aged 20–86 years (528 men and 184 women; mean ± SD age 59.36 ± 13.61 years). The participants completed a self-reported questionnaire, and underwent anthropometric and laboratory measurements and computed tomographic imaging of the abdomen as a part of annual medical check-ups. Multivariate linear regression analyses revealed that rapid eating was associated with larger visceral (B = 24.74; 95% CI 8.87–40.61, p = 0.002) and subcutaneous fat areas (B = 31.31; 95% CI 12.23–50.38, p = 0.001), lower adiponectin concentration (B = − 2.92; 95% CI − 4.39– − 1.46, p < 0.001), higher body mass index (BMI) (B = 2.13; 95% CI 1.02–3.25, p < 0.001), and larger waist circumference (B = 5.23; 95% CI 2.16–8.30, p < 0.001) in men, which is partially consistent with the hypothesis. In contrast, rapid eating was found to be associated only with BMI, and not with abdominal adipose area or adiponectin concentration in women, which is a result that is not consistent with the hypothesis. These results suggest that there is no difference in the association of rapid eating with VFT and SFT areas.
Similar content being viewed by others

Introduction
Obesity and overweight are defined as abnormal or excessive fat accumulation that poses a risk to health. According to the World Health Organization criteria, overweight is characterized by a body mass index (BMI) of ≥ 25 kg/m2 and obesity by a BMI of ≥ 30 kg/m2. Approximately 52% of adults aged ≥ 18 years had overweight or obesity1. Obesity and overweight are known risk factors for cardiovascular diseases, type 2 diabetes, and musculoskeletal disorders1.
Eating behavior is one of the contributors to obesity and overweight. A meta-analysis demonstrated that rapid eating, the consumption of a larger-than-normal amount of food per unit time, is associated with obesity and overweight2. The results were derived from community studies3,4 and from studies of patients with diabetes and hyperlipidemia5,6. This relationship was also identified in children and adolescents7,8. Although most of these findings were made in Asian countries, others conducted in non-Asian countries have generated similar results9,10. Longitudinal studies have demonstrated that rapid eating is predictive of future obesity and overweight11,12, and interventions aimed at reducing eating speed have been shown to reduce BMI in adults with obesity13. Taken together, these results suggest that rapid eating causes obesity and overweight.
In most previous studies, anthropometric techniques have been used to assess abdominal fat mass, including BMI, waist circumference (WC), and waist-to-hip ratio (WHR). While these anthropometric techniques are readily performed, they are not particularly accurate, specific, or reproducible measures of abdominal fat mass14. In addition, they are incapable of differentiating the visceral fat tissue (VFT) located around the abdominal viscera, in the mesentery and omentum, and the subcutaneous fat tissue (SFT) situated under the skin.
VFT and SAT have distinct lipid storage and metabolic properties. In particular, VFT mass is more predictive of developing cardiovascular disease, type 2 diabetes, and hyperlipidemia15,16. Computed tomography (CT) and magnetic resonance imaging (MRI) are the gold-standard methods of assessing abdominal fat mass, because they provide highly accurate and specific quantitative data and can be used to measure the VFT and SFT areas separately14. However, CT and MRI have been used to evaluate the relationships between eating speed and abdominal fat components in few studies. Previous CT and MRI-based studies have shown that rapid eating is associated with a larger VFT area but no difference in SFT area in non-obese adults17, apparently healthy adult men18, or children19. To the best of our knowledge, the relationships of eating speed with the VFT and SFT areas in both adult men and women have only been assessed in one previous study17 using CT or MRI. Because sex-differences in relevant parameters, including eating speed, metabolism, and visceral and subcutaneous fat distribution, have been found, further studies are necessary to confirm whether rapid eating is only associated with VFT, regardless of sex.
Adipocytes are thought to represent an endocrine organ because they secrete a large number of bioactive compounds, referred to as adipokines. Adiponectin is one of these adipokines; is mostly secreted by white adipose tissue; has insulin sensitizing, anti-inflammatory, and anti-arteriosclerotic effects; and is thought to protect against the development of metabolic syndrome and cardiometabolic diseases20,21. Adiponectin synthesis and secretion decrease with adipose hypertrophy, and lower adiponectin concentrations are associated with obesity and overweight22. Given that rapid eating is associated with obesity and overweight, it is also likely to be associated with lower adiponectin concentration. A previous laboratory study demonstrated that higher postprandial adiponectin concentrations are associated with rapid eating, rather than with slower eating23. However, to our knowledge, no studies have yet focused on the relationship between long-term habitual eating speed and circulating adiponectin concentration.
In the present study, we aimed to evaluate the relationships of eating speed with VFT, SFT, and adiponectin concentration in adult men and women. On the basis of the results of previous studies that showed relationships of abdominal fat mass and adiponectin with rapid eating3,23, we hypothesized that rapid eating is associated with larger VFT area and lower adiponectin concentration, but not with SFT area in men and women.
Methods
Study sample and protocol
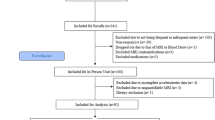
We performed a cross-sectional study of 712 adults aged 20–86 years (528 men and 184 women, mean ± SD age 59.36 ± 13.61 years) who underwent annual medical check-ups provided by the Health Promotion and Health Check-up Center, JA-Shimane, in Shimane Prefecture, Japan. The participants comprised agricultural workers, employees of agriculture-related companies, and their families. They each completed a questionnaire and the medical check-up staff checked the submitted questionnaires and asked the participants to complete any incomplete items. Well-trained medical staff performed anthropometric measurements, blood sample collection, and CT imaging of the abdomen for each participant as part of their medical check-up.
The study was conducted according to the principles of the Declaration of Helsinki. The study was approved by the Medical Research Ethics Committee, Shimane University Faculty of Medicine (No. 20150630-1, approved on July 10, 2015). All the participants received detailed information about the study and provided their written informed consent before participation.
Self-reported questionnaire
The self-reported questionnaire was composed of items regarding demographics (age and sex), lifestyle factors, and depression. Eating speed was rated on a 3-point Likert scale as “rapid”, “moderate”, or “slow” in response to the question “How do you eat in comparison to others?” The validity of this question had been demonstrated by the substantial agreements of self-reported eating speed with objectively measured eating speed24,25 and friend-reported eating speed26. This question has been shown to yield repeatable outcomes for 1 year27. With respect to lifestyle parameters that are thought to be associated with obesity and overweight, current alcohol consumption frequency (every day, sometimes, or rarely), current smoking (yes or no), skipping breakfast three or more times a week (yes or no), eating snacks after dinner three or more times a week (yes or no), having dinner within 2 h of bedtime three or more times a week (yes or no), and engaging in habitual physical activity (yes or no) were assessed. Depression was assessed using a two-item screen28. Respondents answered either “yes” or no” in response to the two questions, “During the past month, have you often been bothered by feeling down, depressed, or hopeless?” and “During the past month, have you often been bothered by having little interest or pleasure in doing things?”. A positive response to both items was considered to indicate possible depression.
Physical and laboratory examinations
Height (in cm) and body mass (in kg) were measured using portable stadiometers, with the participants not wearing shoes, to the nearest 0.1 cm and 0.1 kg, respectively. BMI was calculated as body mass in kg divided by height in m, squared. WC was measured using a tape measure to the nearest 0.1 cm at the level of the umbilicus while the participants were in a standing position. Venous blood samples were collected in the morning after an overnight fast of at least 10 h. The plasma concentration of adiponectin was measured using a latex particle-enhanced turbidimetric immunoassay and an automated analyzer (Adiponectin Latex Kit, Otsuka Pharmaceutical Co., Ltd., Tokyo, Japan). The inter-assay coefficient of variation was < 10.0%, and tests of stored specimens have shown no biological degradation, indicating that the measurements were highly valid. The serum concentrations of low-density lipoprotein (LDL)-cholesterol, high-density lipoprotein (HDL)-cholesterol, and triglyceride were measured using enzymatic assay kits (Kyowa Chemical, Japan) and an Autoanalyzer 7350 (Hitachi Ltd., Tokyo, Japan). The VFT and SFT areas were measured at the level of the umbilicus using a car-mounted multi-slice CT scanner (ELCOS, Hitachi Ltd., Ibaraki, Japan) and specific software for the measurement of abdominal fat area (Hitachi Ltd.).
Statistical analysis
Descriptive data are presented according to sex as mean and standard deviation (SD) for continuous data and percentage and frequency for categorical data. Continuous datasets were compared using one-way between-subject analysis of variance, followed by post-hoc pairwise comparisons using the Holm method; and categorical datasets were compared using Fisher’s exact test. To evaluate the relationships of eating speed with the SFT and VFT areas and adiponectin concentration, multivariate linear regression analysis, involving a forced entry method, was conducted, with adjustment for age, the frequency of current alcohol consumption, current smoking, skipping breakfast, eating snacks, having dinner within 2 h of bedtime, habitual physical activity, and depression. In addition, we evaluated the relationships of eating speed with BMI and WC using multivariate linear regression analysis and the forced entry method, adjusting for the covariates listed above. Variance inflation factors (VIFs) were computed for the relationships between explanatory variables to check for multicollinearity. All the analyses were conducted separately for men and women. Because the data were obtained from all the participants in annual medical check-ups, a sample size calculation was not performed. Two-sided p values < 0.05 were regarded as statistically significant. All the analyses were conducted using R (version 4.2.1; R Foundation for Statistical Computing, Vienna, Austria)29.
Results
Eating speed
The characteristics of the participants, categorized according to sex and eating speed, are shown in Table 1. Among the men, 161 (30.5%) had a rapid eating speed, 326 (61.7%) had a moderate eating speed, and 41 (7.8%) had a slow eating speed. Among the women, 42 (22.8%) had a rapid eating speed, 128 (70%) had a moderate eating speed, and 14 (7.6%) had a slow eating speed.
VFT and SFT areas
The results of the multivariate linear regression analyses for the VFT and SFT areas are shown in Table 2. For the men, the models for VFT area (F(11, 516) = 6.32, p < 0.001, adjusted R2 = 0.100), SFT area (F(11, 516) = 4.52, p < 0.001, adjusted R2 = 0.068), and adiponectin concentration (F(11, 516) = 6.96, p < 0.001, adjusted R2 = 0.111) were significant. Rapid eating was significantly associated with larger VFT and SFT areas, and rapid and moderate eating speeds were significantly associated with lower adiponectin concentration, after adjustment for age, the frequency of alcohol consumption, current smoking status, skipping breakfast, having snacks, having dinner within 2 h of bedtime, habitual physical activity, and depression.
For the women, the models for VFT area (F(11, 172) = 2.93, p = 0.001, adjusted R2 = 0.104) and adiponectin concentration (F(11, 172) = 2.69, p = 0.003, adjusted R2 = 0.092) were significant, whereas the model for SFT area was not (F(11, 172) = 1.40, p = 0.176, adjusted R2 = 0.024). Eating speed was not significantly associated with the VFT or SFT areas or adiponectin concentration after adjustment for the listed covariates. VIFs for the explanatory variables of 1.01 to 1.14 were obtained for all the regression models, which implies the absence of substantial multicollinearity.
Anthropometric data
The results of the multivariate linear regression analyses for BMI and WC are shown in Table 3. For men, the models for BMI (F(11, 516) = 4.11, p < 0.001, adjusted R2 = 0.061) and WC (F(11, 516) = 3.03, p < 0.001, adjusted R2 = 0.041) were significant. Rapid and moderate eating was significantly associated with higher BMI, and rapid eating speeds were significantly associated with larger WC, after adjustment for the listed covariates. For women, the model for BMI was significant (F(11, 172) = 2.16, p = 0.019, adjusted R2 = 0.065), whereas the model for WC was not (F(11, 172) = 1.39, p = 0.179, adjusted R2 = 0.023). Rapid eating speed was significantly associated with higher BMI, but eating speed was not significantly associated with WC, after adjustment for the covariates. We obtained VIFs for the explanatory variables of 1.01 to 1.16 in all the regression models, which implies the absence of substantial multicollinearity.
Discussion
In the present cross-sectional study, we aimed to evaluate the relationships of eating speed with abdominal fat and adiponectin in adult men and women. Specifically, we evaluated the relationships of self-reported eating speed with the VFT and SFT areas, measured using CT, and with the plasma adiponectin concentration. We found that rapid eating was associated with larger VFT and SFT areas and lower adiponectin concentration in men, which is partially consistent with the hypothesis. However, in women, rapid eating was found to be associated only with BMI; there were no significant relationships of eating speed with abdominal fat mass or adiponectin concentration, which is a result that is not consistent with the hypothesis. These findings suggest that there is no difference in the association of rapid eating with VFT and SFT areas.
We found that rapid eating was associated with the larger VFT and SFT areas in men but was also associated with higher BMI and larger WC. These results are consistent with those of previous anthropometric studies, which showed that rapid eating is associated with obesity and overweight3,4. In previous CT and MRI-based studies in which VFT and SFT components were separately measured, contrasting results were obtained. Iwasaki et al.17 and Mochizuki et al.18 reported that rapid eating is associated with larger VFT but not SFT area in adults, whereas Fogel et al.19 showed that rapid eating is associated with larger VFT and SFT volumes in children. These differing findings may be explained by the varied characteristics of the participants in the studies. For example, the male participants in the present study were older than those in the studies of Iwasaki et al.17 and Mochizuki et al.18. Low testosterone and osteocalcin concentrations, which are known to be associated with high adiposity30,31,32, and low muscle mass and basal metabolism may modulate the effects of rapid eating on SFT, as well as VFT, in older participants.
The mechanism underlying the relationship between rapid eating and abdominal fat accumulation remains unclear. One possibility is that rapid eating may cause insufficient satiety, leading to overeating and a higher total energy intake33, possibly because brief periods of sensory exposure provide insufficient cues for satiety34 and are associated with lower secretion of gastrointestinal hormones that control this35. A previous laboratory study showed that rapid eating induces lower postprandial energy expenditure23, which may contribute to fat accumulation, even in the absence of overeating.
Unlike in men, eating speed was shown not to be associated with either the VFT or the SFT areas in women. Instead, it was found to be associated only with BMI. BMI is a measure of body mass that is adjusted for height, and therefore does not depend solely on abdominal fat mass. Adipose tissue is more likely to accumulate in the abdomen in men, while women more frequently accumulate fat in the gluteofemoral region. Thus, rapid eating may be associated with fat accumulation in the gluteofemoral region, rather than in the abdomen, in women.
The present findings in women are not consistent with the results of previous CT and MRI-based studies, which have shown that rapid eating is associated with larger abdominal fat depots in adult men and women17, and also in boys and girls19. Although some studies using anthropometric measures have shown that rapid eating is associated with larger abdominal fat depots in men and women (e.g. Otsuka et al.3; Wuren et al.4), others have shown that a relationship between rapid eating and higher BMI6,36 exists in men, but not in women. In contrast to the consistent results obtained for men, contradictory results have been obtained for women. Women have been shown to prefer less caloric foods37 and are more likely to engage in dieting behavior to improve their physical appearance38. These eating behaviors may attenuate the effects of eating speed on abdominal fat mass. Alternatively, because estrogen and progesterone regulate hunger and appetite39, and the participants in the present study were relatively old, low estrogen and progesterone levels or an imbalance of the two may explain the lack of a relationship between rapid eating and abdominal fat mass in these older women.
We have also shown that rapid eating is associated with low adiponectin concentration in men. To the best of our knowledge, this is the first study to show a relationship between eating speed and adiponectin. However, the finding is consistent with previous findings that rapid eating is associated with the levels of metabolic markers associated with obesity and overweight, such as low HDL-cholesterol concentration, high TG concentration, and high alanine aminotransferase (ALT) activity36,40,41. Rapid eating would be expected to be associated with a lower concentration of adiponectin, at least partly because of its effect to cause the accumulation of abdominal fat. In women, we found no relationship between eating speed and adiponectin concentration. This may be because eating speed is not related to abdominal fat mass in women. Previous studies have demonstrated that adiponectin concentration is related to smoking status42, exercise, diet43, and coffee consumption44. The results of the present study extend the list of lifestyle factors, which are associated with adiponectin concentration, to include eating speed.
Eating speed can be controllable, and the reduction of eating speed represents a potential intervention strategy for the treatment of obesity and overweight. Previous intervention studies have shown that reducing eating speed by means of chewing food in the mouth at least 30 times reduces BMI in patients with obesity13. The findings of the present study may imply that reducing eating speed may reduce VFT and SFT mass and increase adiponectin concentration, particularly in men. Future intervention studies should test these possibilities.
The present study had several limitations. Eating speed was assessed using a self-reported, single-item questionnaire. This method has frequently been used in previous studies on the relationships between eating speed and obesity and related diseases, and has been validated using objective measures of eating speed24,25. However, previous research has reported a lack of high agreement between eating speed assessed using this self-reported questionnaire and objectively measured eating speed at an individual level45. Another single-item eating speed questionnaire46 measures the time taken to consume meals; respondents are asked “How long does it take you to eat a meal?” for each of breakfast, lunch, and dinner. This latter questionnaire may reduce the bias caused by subjective self-evaluation of eating speed. The subscale “Slowness in Eating,” which comprises four items on the Adult Eating Behavior Questionnaire47 has also been used to evaluate eating speed. This self-reported questionnaire is a psychometrically valid and reliable measure of eating behavior. In the laboratory setting, eating speed has been assessed using various objective measures, including continuous weighing of foods using an electronic balance48 and overall food consumption time13,49. The types and amounts of test foods vary among studies13,49. There is no standardized protocol for assessing eating speed45, which limits comparability across studies. Future studies should aim to develop a standardized protocol and use it to attempt to replicate the present findings.
In the present study, the sample of women (n = 184) was smaller than that of men (n = 528). However, the number of female participants in this study is comparable to the number of female participants in some previous studies17,50. Nevertheless, the smaller female sample size may have reduced the statistical power to detect an association between women’s eating speed and abdominal fat mass and adiponectin. These associations in women were similar to those in men, although they were not significant. Thus, the lack of significant results for women mean that the findings should be interpreted with caution. Furthermore, it was cross-sectional in nature, and thus conclusions cannot be drawn regarding causal relationships of eating speed with abdominal fat mass and adiponectin concentration. We did not have information regarding the type or amount of food consumed, and therefore we could not test the effects of the diet consumed on the relationship between eating speed and abdominal fat mass. Finally, the study sample was limited to workers in agriculture and related industries and their families living in a rural area of Japan, which may reduce the external validity of the findings.
In conclusion, in the present study, we have shown that rapid eating is associated with larger VFT and SFT areas and lower adiponectin concentration in men. In contrast, while rapid eating was found to be associated only with BMI, eating speed was found not to be associated with abdominal fat mass or adiponectin concentration in women. The present findings are consistent with previous findings that rapid eating is associated with the development of obesity and overweight, and imply that adult men may benefit more from reducing their eating speed.
Data availability
The datasets generated during and/or analyzed during the current study are not publicly available due to participants’ confidentiality concerns but are available from the corresponding author on reasonable request.
References
World Health Organization. Obesity and overweight. https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (2021).
Kolay, E. et al. Self-reported eating speed is associated with indicators of obesity in adults: A systematic review and meta-analysis. Healthcare 9, 1559 (2021).
Otsuka, R. et al. Eating fast leads to obesity: Findings based on self-administered questionnaires among middle-aged Japanese men and women. J. Epidemiol. 16, 117–124 (2006).
Wuren, Endoh, K., Kuriki, K., Shizuoka-Sakuragaoka J-MICC Study group. Eating rate as risk for body mass index and waist circumference obesity with appropriate confounding factors: A cross-sectional analysis of the Shizuoka-Sakuragaoka J-MICC Study. Asia Pac. J. Clin. Nutr. 28, 79–91 (2019).
Hurst, Y. & Fukuda, H. Effects of changes in eating speed on obesity in patients with diabetes: A secondary analysis of longitudinal health check-up data. BMJ Open 8, e019589 (2018).
Takayama, S. et al. Rate of eating and body weight in patients with type 2 diabetes or hyperlipidaemia. J. Int. Med. Res. 30, 442–444 (2002).
Garcidueñas-Fimbres, T. E., Paz-Graniel, I., Nishi, S. K., Salas-Salvadó, J. & Babio, N. Eating speed, eating frequency, and their relationships with diet quality, adiposity, and metabolic syndrome, or its components. Nutrients 13, 1687 (2021).
Xie, Q. et al. Effect of eating habits on obesity in adolescents: A study among Chinese college students. J. Int. Med. Res. 48, 030006051988973 (2020).
Leong, S. L., Madden, C., Gray, A., Waters, D. & Horwath, C. Faster self-reported speed of eating is related to higher body mass index in a nationwide survey of middle-aged women. J. Am. Diet. Assoc. 111, 1192–1197 (2011).
Oda-Montecinos, C., Saldaña, C. & Andrés, A. Eating behaviors are risk factors for the development of overweight. Nutr. Res. N. Y. N 33, 796–802 (2013).
Ochiai, H. et al. The impact of eating quickly on anthropometric variables among schoolgirls: A prospective cohort study in Japan. Eur. J. Public Health 24, 691–695 (2014).
Zhu, B., Haruyama, Y., Muto, T. & Yamazaki, T. Association between eating speed and metabolic syndrome in a three-year population-based cohort study. J. Epidemiol. 25, 332–336 (2015).
Ekuni, D., Furuta, M., Takeuchi, N., Tomofuji, T. & Morita, M. Self-reports of eating quickly are related to a decreased number of chews until first swallow, total number of chews, and total duration of chewing in young people. Arch. Oral Biol. 57, 981–986 (2012).
Shuster, A., Patlas, M., Pinthus, J. H. & Mourtzakis, M. The clinical importance of visceral adiposity: A critical review of methods for visceral adipose tissue analysis. Br. J. Radiol. 85, 1–10 (2012).
Neeland, I. J. et al. Body fat distribution and incident cardiovascular disease in obese adults. J. Am. Coll. Cardiol. 65, 2150–2151 (2015).
Fox, C. S. et al. Abdominal visceral and subcutaneous adipose tissue compartments. Circulation 116, 39–48 (2007).
Iwasaki, T. et al. Self-reported behavior of eating quickly is correlated with visceral fat area in Japanese non-obese adults. Asia Pac. J. Clin. Nutr. 28, 92–98 (2019).
Mochizuki, K. et al. Self-reported faster eating is positively associated with accumulation of visceral fat in middle-aged apparently healthy Japanese men. Eur. J. Nutr. 53, 1187–1194 (2014).
Fogel, A. et al. Faster eating rates are associated with higher energy intakes during an ad libitum meal, higher BMI and greater adiposity among 4·5-year-old children: Results from the Growing Up in Singapore Towards Healthy Outcomes (GUSTO) cohort. Br. J. Nutr. 117, 1042–1051 (2017).
Peng, J., Chen, Q. & Chuncao, W. The role of adiponectin in cardiovascular disease. Cardiovasc. Pathol. 64, 107514. https://doi.org/10.1016/j.carpath.2022.107514 (2023).
Lei, X., Qiu, S., Yang, G. & Wu, Q. Adiponectin and metabolic cardiovascular diseases: Therapeutic opportunities and challenges. Genes Dis. https://doi.org/10.1016/j.gendis.2022.10.018 (2022).
Arita, Y. et al. Paradoxical decrease of an adipose-specific protein, adiponectin, in obesity. Biochem. Biophys. Res. Commun. 257, 79–83 (1999).
Reddy, N. L. et al. Enhanced thermic effect of food, postprandial NEFA suppression and raised adiponectin in obese women who eat slowly. Clin. Endocrinol. (Oxf.) 82, 831–837 (2015).
Hamada, Y. et al. Objective and subjective eating speeds are related to body composition and shape in female college students. J. Nutr. Sci. Vitaminol. (Tokyo) 63, 174–179 (2017).
van den Boer, J. H. W. et al. Self-reported eating rate is associated with weight status in a Dutch population: A validation study and a cross-sectional study. Int. J. Behav. Nutr. Phys. Act. 14, 121 (2017).
Sasaki, S., Katagiri, A., Tsuji, T., Shimoda, T. & Amano, K. Self-reported rate of eating correlates with body mass index in 18-y-old Japanese women. Int. J. Obes. Relat Metab. Disord. J. Int. Assoc. Study Obes. 27, 1405–1410 (2003).
Maruyama, K. et al. The joint impact on being overweight of self reported behaviours of eating quickly and eating until full: Cross sectional survey. BMJ 337, a2002–a2002 (2008).
Whooley, M. A., Avins, A. L., Miranda, J. & Browner, W. S. Case-finding instruments for depression: Two questions are as good as many. J. Gen. Intern. Med. 12, 439–445 (1997).
R Core Team R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. https://www.R-project.org/ (2018).
Han, S. et al. Testosterone is associated with abdominal body composition derived from computed tomography: A large cross sectional study. Sci. Rep. 12, 22528 (2022).
Kim, C. et al. Changes in visceral adiposity, subcutaneous adiposity, and sex hormones in the diabetes prevention program. J. Clin. Endocrinol. Metab. 102, 3381–3389 (2017).
Kindblom, J. M. et al. Plasma osteocalcin is inversely related to fat mass and plasma glucose in elderly Swedish men. J. Bone Miner. Res. 24, 785–791 (2009).
Robinson, E. et al. A systematic review and meta-analysis examining the effect of eating rate on energy intake and hunger. Am. J. Clin. Nutr. 100, 123–151 (2014).
de Graaf, C. & Kok, F. J. Slow food, fast food and the control of food intake. Nat. Rev. Endocrinol. 6, 290–293 (2010).
Galhardo, J. et al. Normalizing eating behavior reduces body weight and improves gastrointestinal hormonal secretion in obese adolescents. J. Clin. Endocrinol. Metab. 97, E193-201 (2012).
Lee, K. S. et al. Eating rate is associated with cardiometabolic risk factors in Korean adults. Nutr. Metab. Cardiovasc. Dis. 23, 635–641 (2013).
Manippa, V., Padulo, C., van der Laan, L. N. & Brancucci, A. Gender differences in food choice: Effects of superior temporal sulcus stimulation. Front. Hum. Neurosci. https://doi.org/10.3389/fnhum.2017.00597 (2017).
Davy, S. R., Benes, B. A. & Driskell, J. A. Sex differences in dieting trends, eating habits, and nutrition beliefs of a group of midwestern college students. J. Am. Diet. Assoc. 106, 1673–1677 (2006).
Hirschberg, A. L. Sex hormones, appetite and eating behaviour in women. Maturitas 71, 248–256 (2012).
Mochizuki, K. et al. Self-reported faster eating associated with higher ALT activity in middle-aged, apparently healthy Japanese women. Nutr. Burbank Los Angel. Cty. Calif. 30, 69–74 (2014).
Nagahama, S. et al. Self-reported eating rate and metabolic syndrome in Japanese people: Cross-sectional study. BMJ Open 4, e005241–e005241 (2014).
Takefuji, S. et al. Smoking status and adiponectin in healthy Japanese men and women. Prev. Med. 45, 471–475 (2007).
Khalafi, M., Hossein Sakhaei, M., Kheradmand, S., Symonds, M. E. & Rosenkranz, S. K. The impact of exercise and dietary interventions on circulating leptin and adiponectin in individuals who are overweight and those with obesity: A systematic review and meta-analysis. Adv. Nutr. https://doi.org/10.1016/j.advnut.2022.10.001 (2022).
Linden-Torres, E., Zambrano-Galván, G., Sahebkar, A., Ríos-Mier, M. & Simental-Mendía, L. E. Coffee consumption has no effect on circulating markers of liver function but increases adiponectin concentrations: A systematic review and meta-analysis of randomized controlled trials. Nutr. Res. 106, 24–34 (2022).
Woodward, E., Haszard, J., Worsfold, A. & Venn, B. Comparison of self-reported speed of eating with an objective measure of eating rate. Nutrients 12, 599 (2020).
Garcidueñas-Fimbres, T. E. et al. Associations between eating speed, diet quality, adiposity, and cardiometabolic risk factors. J. Pediatr. 252, 31-39.e1 (2023).
Hunot-Alexander, C. et al. Confirmation of the factor structure and reliability of the ‘Adult Eating Behavior Questionnaire’ in an adolescent sample. Front. Psychol. https://doi.org/10.3389/fpsyg.2019.01991 (2019).
Kissileff, H. R., Klingsberg, G. & Van Itallie, T. B. Universal eating monitor for continuous recording of solid or liquid consumption in man. Am. J. Physiol.-Regul. Integr. Comp. Physiol. 238, R14–R22 (1980).
Viskaal-van Dongen, M., Kok, F. J. & de Graaf, C. Eating rate of commonly consumed foods promotes food and energy intake. Appetite 56, 25–31 (2011).
Yi, W. et al. Association between visceral adipose tissue volume, measured using computed tomography, and cardio-metabolic risk factors. Sci. Rep. 12, 387 (2022).
Acknowledgements
We would like to acknowledge the thoughtful cooperation and support of the staff in the Health Promotion and Health Checkup Center, JA-Shimane. We also thank Mark Cleasby, PhD from Edanz (https://jp.edanz.com/ac) for editing a draft of this manuscript.
Funding
The funding was provided by Shimane University.
Author information
Authors and Affiliations
Contributions
H.T., M.F., T.H., R.S., R.T. and H.K. conceived and designed the study. H.T., M.F. and R.S. collected the data. H.T., M.F., T.H., R.S. and H.K. analyzed and interpreted the data. H.T., M.F., T.H., R.S., R.T. and H.K. wrote the paper. All the authors have read the manuscript and have approved this submission.
Corresponding author
Ethics declarations
Competing interests
Dr. Hideki Tsumura was supported by support funds of Shimane University for young researchers. Shimane university had no role in the study design, collection, analysis, or interpretation of the data, writing the article, or submitting the article for publication. Dr. Mari Fukuda, Dr. Takashi Hisamatsu, Dr. Rie Sato, Ms. Rina Tsuchie, and Dr. Hideyuki Kanda declare no potential conflict of interest.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Tsumura, H., Fukuda, M., Hisamatsu, T. et al. Relationships of rapid eating with visceral and subcutaneous fat mass and plasma adiponectin concentration. Sci Rep 13, 11491 (2023). https://doi.org/10.1038/s41598-023-38623-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-38623-7
- Springer Nature Limited