
Abstract
The associations between particulate matter (PM) and overall and specific mental disorders (MDs) are investigated using data from two general hospitals in Shijiazhuang, China, from January 2014 to December 2019. A longitudinal time series study, as one type of ecological study, is conducted using a generalized additive model to examine the relationship between short-term exposure to PM2.5, PM10, and daily hospital admissions for MDs, and further stratification by subtypes, age, and gender. A total of 10,709 cases of hospital admissions for MDs have been identified. The significant short-time effects of PM2.5 on overall MDs at lag01 and PM10 at lag05 are observed, respectively. For specific mental disorders, there are substantial associations of PM pollution with mood disorders and organic mental disorders. PM2.5 has the greatest cumulative effect on daily admissions of mood disorders and organic mental disorders in lag01, and PM 10 has the greatest cumulative effect in lag05. Moreover, the effect modification by sex or age is statistically significant, with males and the elderly (≥ 45 years) having a stronger effect. Short-term exposure to PM2.5 and PM10can be associated with an increased risk of daily hospital admissions for MDs.
Similar content being viewed by others


Introduction
Mental disorders are a class of syndromes characterized by clinically significant dysfunctions in cognition, emotion regulation, or behavior. The etiology of mental disorders is unknown, and its pathogenesis is closely related to genetic-environmental factors. Environmental pollution has been identified as a risk factor for mental health1. It had been found that air pollution can exacerbate symptoms of Alzheimer’s disease, schizophrenia, psychiatric emergencies, or increase emergency hospital admissions in Spain2, Japan3, Italy4, etc. A total of 20,000 residents in 25 regions in China were surveyed from 2010 to 20145, and the result revealed that increases in air pollution and temperature changes were associated with an increase in mental health problems. In a review, Omar also described increasing evidence that proinflammatory mediators and reactive oxygen species can affect the health of the central nervous system and brain after exposure to various air pollutants, leading to the occurrence of various MDs6.Particulate matter (PM) is an important component of air pollution, and its link to mental health is receivingincreasing attention. PM10, PM2.5, PM1, black carbon, smoking and cooking fumes, and so on are all examples of PM. PM2.5 has a large surface area and a small diameter than PM10. It can suspend in the air for a long time and travel long distances. In the air, various harmful substances, such as heavy metals and polycyclic aromatic hydrocarbons, are easily absorbed. Although both PM2.5 and PM10 are inhalable particles, some of PM10 can be excreted through sputum and blocked by the villi inside the nasal cavity; PM2.5, on the other hand, can partially enter the gas exchange area of the human lungs, pass through the respiratory barrier, enter the circulatory system, and spread throughout the body, making PM2.5 more harmful to the human body than PM10. Shijiazhuang, one of the most polluted cities in northern China, under went a study from 2014 to 2016 that focused on the effect of PM2.5 and PM10 on the daily admission rates for mental and behavioral disorders6. It demonstrated that various air pollutants, particularly PM and monoxide nitrogen, were related to poor mental health. However, the study was conducted over a short period of time, and the effects of PM on the subtypes of MDs were unclear. Therefore, a longer study of the relationship between air pollution and MDs in Shijiazhuang will be required, as will further research into the effect of PM on specific MDs. We collected air quality data and hospital admissions for MDs from 2014 to 2019 to investigate the impact of air pollution on hospital admissions for general and specific MDs using time series regression analysis.
Methods
Data collection
Shijiazhuang City is the capital of Hebei Province, which is located in the southwest of Hebei Province, China, at latitude 114°26′E and longitude 38°03′N. As of the end of 2019, the permanent population was 10.39 million in Shijiazhuang. It has to a typical temperate monsoon climate with distinct seasonal fluctuations. This study was performed in accordance with the tenets of the Declaration of Helsinki and was approved by the ethics committee of the First Hospital of Hebei Medical University.
The data were retrieved from the First Hospital of Hebei Medical University and the Third Hospital of Shijiazhuang, both of which were general hospitals in Shijiazhuang. During the study period, the patients admitted to the hospital due to mental disorders were pulled from the hospital information system every day (January 1, 2014, to December 31, 2019). Mental disorders were classified using the International Classification of Diseases-10th Edition (ICD-10).
This study was an ecological study and applied the average method to evaluate the level of air pollutants. The average method refers to calculating the average value of certain air pollutants at air detection stations in a certain area as the exposure value for all research objects in that area.The daily air pollution data forgaseous pollutants such as PM2.5 (μg/m3) and PM10 (μg/m3) were obtained from the Ministry of Environmental Protection of China’s website (https://www.aqistudy.cn/). The daily average concentration of air pollutants was recordedat seven fixed stations in the traditional urban area of Shijiazhuang City. These stations are required to be located far away from major roadways, industrial sources, buildings, or domesticcoal, oil, or trashburning emission sources, with a good reflection of the level of air pollution in the city. Daily weather data, including daily average temperature (°C) and relative humidity (%), came from the China Meteorological Data Sharing Service System (http://data.cma.cn/).
Statistical analyses
We applied a time-series approach to analyze the data, which has the advantage of automatically controlling for time-invariant confounders at the population level. An over-dispersed generalized additive model (GAM) was applied to analyze the association between PM (PM2.5 and PM10) and daily hospital admissions for mental and behavioral disorders. Several covariates were introduced to control for potential confounding effects: (1) a natural cubic regression smooth function of calendar time with sevendegrees of freedom (df) per year (2) natural smooth functions of the mean temperature (6, df) and relative humidity (3, df) to account for the nonlinear confounding effects of weather conditions; (3) indicator variables for “day of the week”. The main model is described as follow: logE(Yt) = βZt + ns (time, df) + ns(temperature, 6) + ns(humidity, 3) + DOW + intercept, where E(Yt) represents the expected number of hospital admissions for mental and behavioral disorders at day t; β represents the log-related rate of mental and behavioral disorders admission rate associated with a unit increase of PM pollutants; Zt represents the pollutant concentrations at day t; DOW is a dummy variable for the day of the week; ns indicates natural cubic regression smooth function. After the basic model was established, we further introduced both single-day lags from 0 to 7and moving average exposure of multiple days, including lag0–1, 0–2, 0–3, 0–4, 0–5, 0–6, 0–7. The exposure-response relationship curves between PM2.5, PM10, and hospital admissions for mental and behavioral disorders were plotted by including a natural spline function with 3 df in the above model. Two sensitivity analyses were performed to ensure the stability of our model. First, we selected alternative df with 4–10 per year for the smoothness of time trends. Second, we created two-pollutant models to examine the robustness of the effect estimates after adjusting for co-pollutants.
Furthermore, we conducted stratification analyses to explore the potential effect of modification by age (<45, ≥45)7, and sex. We further evaluated the statistical significance for the differences in estimates across strata by calculating 95% confidence intervals (CI) as (\(\widehat{\mathrm{Q}}1-\widehat{\mathrm{Q}}2)\pm 1.96 \sqrt {S\hat{E}_{1}^{2} + S\hat{E}_{2}^{2} }\),where \(\widehat{\mathrm{Q}}1\) and \(\widehat{\mathrm{Q}}2\) are the estimates for two categories, \(\mathrm{and}\) \(S\hat{E}_{1}^{2}\) and \(S\hat{E}_{2}^{2}\) are their standard errors.
The statistical tests were two-sided, and effects of P<0.05 were considered statistically significant. All statistical models were run in R software (version 4.1.1) using the MGCV package. Excess risk (ER)=(OR–1)×100%, which represents the percentage of change in daily hospital admissions for mental and behavioral disorders per 10 μg/m3 increase of PM (PM2.5 and PM10).
Ethics approval and consent to participate
This study was performed in accordance with the tenets of the Declaration of Helsinki and was approved by the ethics committee of the First Hospital of Hebei Medical University. All participants provided written informed consent before admission.
Results
Data description
From January 1st, 2014 to December 31st, 2019, a total of 10,709 patients met the ICD-10 diagnostic criteria for mental disorders in the two hospitals, with 32.99% being males and 54.51% being 45 years or younger. The daily average PM2.5 and PM10 concentrations were 89.25 and 157.16μg/m3, respectively, the number of days abovethe average daily PM2.5 (≥75μg/m3) concentrations in Chinaper year was 240, 177, 164, 146, 140, 89 (the 6-year average was 159) from 2014 to 2019, while 234, 146, 141, 148, 125, 93 (the 6-year average was 148) for PM10 (≥150μg/m3), respectively. The daily average temperature was 14.98 °C, with a humidity of 55.15%. As shown in Table 1, the distributions of data on daily admissions for mental disorders and subtypes are listed. The distribution of PM2.5 from 2014 to 2019 is shown in Fig. 1. And the distribution of PM10, SO2, CO, NO2, O3 is displayed in Supplementary Figs. 1 to 5, respectively.

Distribution of PM2.5 from 2014 to 2019.
Single-pollutant model analysis
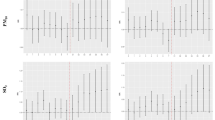
Figure 2A depicted the lag–response relationships for the impact of PM2.5 on the daily hospital admissions for mental disorders. The lag effect of PM2.5 on daily admissions for all mental disorders was statistically significant at lag0 and lag1, and its cumulative effect was greatest at lag01. The excess risk (ER) value of admission for mental disorders was 1.18% for every 10g/m3 increase in PM2.5 concentration(95% CI 0.63–1.73%).

Association between PM2.5 and daily hospital admission for mental disorders, Shijiazhuang, China, 2014–2019. Results express as percentage change (95% CI) in daily hospital admission per 10 μg/m3 increase in PM2.5 concentration. (A) all mental disorders; (B) schizophrenia and other primary psychotic disorders; (C) mood disorders (including manic episodes, bipolar disorder, depressive episodes, etc.); (D) anxiety disorders and fear-related disorders, obsessive-compulsive disorders, somatoform disorder, dissociation (conversion) disorder; (E) organic mental disorder (including Alzheimer’s disease, vascular dementia, delirium, etc.), (F) other mental disorders (including mental and behavioral disorders caused by alcohol, stress-related disorders, personality disorders, sleep disorders, neurodevelopmental disorders, etc.).
The results of the exposure-response relationship between specific mental disorders and PM2.5 were inconsistent in the subgroup of mental disorders, with statistically significant differences only in mood disorders and organic mental disorders (Fig. 2B–F). The lag effect of PM2.5 on daily hospital admission for mood disorders/organic mental disorders was statistically significant at lag0/lag0, lag1, and the greatest cumulative effect was at lag01, with the statistical significance for mood disorders at lag01 and organic mental disorders at lag01-lag06. The effect of PM2.5 on daily admissions of schizophrenia and primary psychotic disorders, anxiety and related disorders, and other mental disorders was similar to the trend of the aforementioned diseases, but there was no statistically significant difference.
The lag effect of PM10 on all mental disorders was evident in Fig. 3A, with statistical differences at lag0, lag1, and lag2, and the peak of the cumulative effect of PM10 was at lag05. The ER value of admission for mental disorders was 1.01% for every 10μg/m3 increase in PM10 concentration (95%CI 0.32–1.71%).

Association between PM10 and daily hospital admission for mental disorders, Shijiazhuang, China, 2014–2019. Results expressed as a percentage change (95% CI) in daily hospital admission per 10 μg/m3 increase in PM10 concentration. (A) all mental disorders; (B) schizophrenia and other primary psychotic disorders; (C) mood disorders (including manic episodes, bipolar disorder, depressive episodes, etc.); (D) anxiety disorders and fear-related disorders, obsessive-compulsive disorders, somatoform disorder, dissociation (conversion) disorder; (E) organic mental disorder (including Alzheimer’s disease, vascular dementia, delirium, etc.), (F) other mental disorders (including mental and behavioral disorders caused by alcohol, stress-related disorders, personality disorders, sleep disorders, neurodevelopmental disorders, etc.).
The results of the exposure-response relationship among specific mental disorders and PM10 were analogous to PM2.5 in the subgroup of mental disorders(Fig. 3B–F). The lag effect of PM10 on the daily hospital admission for mood disorders/organic mental disorders was statistically significant at lag0/lag0 to lag4, and the greatest cumulative effect were both at lag05, with statistical significance at lag01-lag06. In addition, statistically significant lag effects of PM10 on the daily admission for schizophrenia and primary psychotic disorders and other mental disorders were found at lag0, butonly cumulative effect at lag01. However,there was no statistically significant difference between PM10 and anxiety and related disorders.
The daily hospitalization of PM and mental disorders was associated with the exposure-response relationship curve when accumulating lag 01 (PM2.5) and 05 (PM10), respectively, as shown in Figs. 4 and 5. Both the curves of PM2.5 and PM10 tended to alinear trend, indicating that there was no threshold for the association between PM2.5 or PM10 and daily hospitalization for mental disorders.The results of PM2.5 and PM10 sensitivity analyses confirmed that our models were stable at Table 2.

The exposure-response relationship curves for the lag01 day concentrations of PM2.5 with daily hospital admissions for mental disorders. The solid line represents mean estimates, and the dashed lines for 95% confidence intervals.

The exposure-response relationship curves for the lag05 day concentrations of PM10 with daily hospital admissions for mental disorders. The solid line represents mean estimates, and the dashed lines for 95% confidence intervals.
Effects by sex and age
PM2.5 and PM10 were significantly positively correlated with changes in the admission for mental disorders in both males and females, but more so in males. Table 3 shows a positive relationshipbetween PM and hospitalization for mental disorders in younger (less 45-year old) and older (45-year and more) people, which was more pronounced in the elderly.
Two-pollutant models analysis
In the two-pollutant model of PM2.5 and SO2, CO, NO2, and O3, there were significant positive correlations between the change of mental disorders admission at cumulative lag01, with statistically significant differences. The results of PM10 and SO2, CO, NO2, and O3 were similar to PM2.5 in the dual pollutant model at lag05, with statistically significant differences, as Table 4 showed.
Discussion
Similar to previous studies7, our study found that PM2.5 and PM10 were positively correlated with the daily hospital admission for mental disorders in Shijiazhuang from 2014 to 2019, but our findings suggested that the cumulative effect of PM2.5 was the most obvious at lag01, as the risk for mental disorders admissions increases (excess risk, ER) 1.18% (95% CI 0.63–1.73%) for every 10 μg/m3 increase in PM2.5 concentration; PM10 has the greatest cumulative effect at lag05, whose ER value for admission to the mental disorders was 1.01% (95% CI 0.32–1.71%) with a 10μg/m3 increase of PM10, which were significantly higher than the results of Song et al.7. They showed that for every unit increase in PM2.5 and PM10 concentrations (both lag02), the daily admissions for mental disorders increased by 0.48% (95% CI 0.18–0.79%) and 0.32% (95% CI 0.03–0.62%), respectively. Although their study was also conducted in Shijiazhuang, our study was longer, contained 6 years of data, and covered admissions for mental disorders in two comprehensive tertiary hospitals, with a bigger sample size. These may lead to discrepancies between the two studies. A study conducted in Shenzhen, China, also showed that as the concentration of air pollutants increase, so did the number of daily outpatient visits for mental disorders, such as PM2.5 at lag0 (ER=1.20%, 95% CI 0.28–2.13%), PM10 (ER = 0.99%, 95% CI 0.36–1.62%)8. The study of Chengdu from 2015 to 2016 displayed that at lag06 PM2.5 and PM10 increased by 10μg/m3, the daily hospitalization for mental disorders increased by 2.89% (95% CI 0.75–5.08%), 1.91% (95% CI 0.57–3.28%), respectively9. According to another survey conducted in Chengdu between 2013 and 2017, the exposure-response effects of PM pollution on hospital admissions for the overall and specific mental disorder were strong, at the cumulative lag03 day would be 3.25% (95% CI 2.34–4.16%) for PM2.5, and 6.38% (95% CI 4.79–7.97%) for PM1010. The results differed slightly from city to city, presumably due to climate differences. Thus, both PM2.5 and PM10 can increase the risk of daily hospital admissions for overall mental disorders, with PM2.5 having a more immediate effect than PM10.
Moreover, we analyzed the impact of PM on the daily admission in specific mental disorders. The results showed that the daily admission for mood disorders and organic mental disorders accumulated at lag01(PM2.5) and lag05(PM10) during short-time PM exposures. The effect of PM2.5 and PM10 had the strongest influences, which were the same as the overall mental disorder, but there was no statistical difference in the influence on schizophrenia and other primary psychotic disorders, anxiety disorders, and other mental disorders. A study in Madrid also showed that PM2.5 concentration at lag2 was related to Alzheimer's disease admission (RR=1.38, 95% CI 1.15–1.65)2; Similar results have been found in Zhejiang, China, where the risk of AD rised by 2%-5% per increase 10 μg/m3 in PM2.5, from 2013 to 201711. A survey of 26 cities in China from 2013 to 2015 found that PM was positively correlated with hospital admissions for depression, PM10 was the strongest at lag0, PM2.5 was highest at lag0 and lag5, and the elderly (over 65 years) were more sensitive to PM, which was consistent with our findings12. Moreover, the high level of PM was related to the elevated suicide events among major depressive disorder patients, which was proved by research from 2004 to 2017 in Korean13. A Japanese study suggested that short-term PM2.5 exposure was associated with worsening symptoms in hospitalized schizophreniapatients (1193 cases)3. In addition, asurvey (11,373 cases) conducted in Hefei, China, from 2014 to 2016, suggested that short-term NO2 exposure may be related to the increase in hospitalizations for schizophrenia14. However, Carugno et al. found increasing PM10 levels shifts the manic episode towards the depressive pole of the bipolar disorder spectrum without increasing the risk of psychotic symptoms at admission15. A UK Biobank study (2006–2010) found that for per per 10 μg/m3 increase in PM2.5, the risk of major depression and bipolar disorder increased by 2.26 and 4.99 times, respectively16. Positive associations between PM2.5 or PM10 and anxiety admissions were found in a Chinese multicity case-crossover study17, and the highest RR of emergency room visit for anxiety disorder due to PM2.5(RR=1.709) and PM10(RR=2.618) in South Korea18. These results differed from ours and could be attributed to differences in sample size and air pollution levels. A meta-analysis showed that short-term PM10 build up was significantly associated with suicide in the first 2 days19. Furthermore, a Canadian study discovered that PM2.5 and PM10 levels were positively correlated with emergency department visits for alcohol and drug abuse. In our study, due to the modest number of suicides and substance use disorders, they were not evaluated as subgroups.
Although there was a positive correlation between particulate pollution and the daily admission for mental disorders in both males and females, over 45 and less than 45 years old, this effect was more pronounced in men and over 45 years of age. The results were consistent with past studies7,10,20. Other research had shown that female patients were more vulnerableto PM9,17.
The two-pollutant model revealedthat PM2.5 and PM10 were positively correlated with SO2, CO, NO2, O3, and the daily hospital admission for mental disorders, with PM10 and CO having the largest influence. Similar to aprevious study in South Korea, the two-pollutant model exhibiteda slightly improved influence on emergency hospital admissions for mental disorders21. A study in Italy had shown that short-term O3 exposure may increase the number of psychiatric hospital admissions eachday18.
There was evidence that inflammation and oxidative stress were key factors in the pathophysiology of diseases caused by air pollution, which was producedby increased production of pro-inflammatory mediators and reactive oxygen species as a result of exposure to various air pollutants22. Exposure to PM2.5 was associated with a reduction in the volume of the bilateral superior, middle, and medial frontal gyri cortex, as well aswhite matter in the frontal lobe with the largest clusters, temporal, parietal, and occipital lobes with small clusters23. These brain areas were involved in higher-level cognitive functions, such as working memory, episodic memory, and executive function. Long-term exposure to PM2.5 may hasten gray matter loss in elderly women, while the decreasedgray matter volume representedneutron atrophy and a decrease in the number of synaptic spines, dendritic branches, and synapses, which can severely impair cognitive performance23. The effects of PM on white matter volume were mainly concentrated in the frontal, parietal and temporal lobes, with regional distribution features. The decrease in white matter volume reflected oligodendrocytes and/or myelin degredation, which were related to cognitive function decline. Long-term exposure to PM2.5 is associated with lower total brain volume and more cryptogenic cerebral infarctions24. It was proved that PM2.5 can caused neuronal apoptosis and damage to the blood brain barrier25, that PM2.5 may be invovled in possible causative mechanisms of dementia. PM and ozone, two prevalent pollutants with different characteristics and reactivity, can stimulatedthe hypothalamic-pituitary-adrenal axis and trigger cortisol release, resulting in a neuroendocrine stress response26.
Our study had the following limitations. Firstly, this study was an ecological design study and could not avoid the ecological fallacy. Although time series studies had been used to control for some confounding factors, it was still not possible to completely rule out the influence of individual confounding factors, such as physical illness, occupation, lifestyle habits (smoking, drinking, liking outdoor activities, etc.). Estimating the average level of pollutants in the city to estimate the average exposure level of the population would result in certain errors, without considering the impact of indoor pollutant PM2.5. Secondly, due to the limited number of cases of some specific mental disorders, a more detailed grouping analysis was not carried out. Thirdly, the pathophysiology of mental disorders is not clear, but both hereditary and environmental factors have an impact on its pathogenesis. Our study did not investigate genetics-related factors. Finally, we have not done our best in controlling confounding factors, such as the patient's living environment, seasonal factors, light pollution, noise pollution, and other pollutant levels that may lead to individual differences in patients, which is also an important direction for our future inclusion and in-depth research.
In conclusion, short-term particulate pollution has a positive correlation with the daily hospital admission for mental disorders, especially among elderly men. At the same time, the combined effect of air pollutants and particulate pollutants might amplifythis effect.
Data availability
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- ER:
-
Excess risk
- MD:
-
Mental disorders
- PM:
-
Particulate matter
References
Arango, C. et al. Preventive strategies for mental health. Lancet Psychiatry 5(7), 591–604 (2018).
Culqui, D. R. et al. Association between environmental factors and emergency hospital admissions due to Alzheimer’s disease in Madrid. Sci. Total Environ. 592, 451–7 (2017).
Eguchi, R. et al. The relationship between fine particulate matter (PM(2.5)) and schizophrenia severity. Int. Arch. Occup. Environ. Health 91(5), 613–22 (2018).
Bernardini, F. et al. Air pollutants and daily number of admissions to psychiatric emergency services: Evidence for detrimental mental health effects of ozone. Epidemiol. Psychiatr. Sci. 29, e66 (2019).
Xue, T. et al. Declines in mental health associated with air pollution and temperature variability in China. Nat. Commun. 10(1), 2165 (2019).
Hahad, O. et al. Ambient air pollution increases the risk of cerebrovascular and neuropsychiatric disorders through induction of inflammation and oxidative stress. Int. J. Mol. Sci. 21(12), 4306 (2020).
Song, J. et al. Acute effects of ambient particulate matter pollution on hospital admissions for mental and behavioral disorders: A time-series study in Shijiazhuang, China. Sci. Total Environ. 636, 205–11 (2018).
Li, H. et al. Short-term effects of air pollution on cause-specific mental disorders in three subtropical Chinese cities. Environ. Res. 191, 110214 (2020).
Qiu, H. et al. Attributable risk of hospital admissions for overall and specific mental disorders due to particulate matter pollution: A time-series study in Chengdu, China. Environ. Res. 170, 230–7 (2019).
Zhang, P. & Zhou, X. Health and economic impacts of particulate matter pollution on hospital admissions for mental disorders in Chengdu, Southwestern China. Sci. Total Environ. 733, 139114 (2020).
Yang, L. et al. Associations between PM2.5 exposure and Alzheimer’s disease prevalence among elderly in Eastern China. Environ. Health 21(1), 119 (2022).
Wang, F. et al. Ambient concentrations of particulate matter and hospitalization for depression in 26 Chinese cities: A case-crossover study. Environ. Int. 114, 115–22 (2018).
Hwang, I. Y. et al. Association of short-term particulate matter exposure with suicide death among major depressive disorder patients: A time-stratified case-crossover analysis. Sci. Rep. 12(1), 8471 (2022).
Bai, L. et al. Ambient concentrations of NO(2) and hospital admissions for schizophrenia. Occup. Environ. Med. 76(2), 125–31 (2019).
Carugno, M. et al. Short-term air pollution exposure is associated with lower severity and mixed features of manic episodes in hospitalized bipolar patients: A cross-sectional study in Milan, Italy. Environ. Res. 196, 110943 (2021).
Hao, G. et al. Associations of PM2.5 and road traffic noise with mental health: Evidence from UK Biobank. Environ. Res. 207, 112221 (2022).
Yue, J. L. et al. Association between ambient particulate matter and hospitalization for anxiety in China: A multicity case-crossover study. Int. J. Hyg. Environ. Health 223(1), 171–8 (2020).
Hong, J., Kang, J. M., Cho, S. E., Jung, J. & Kang, S. G. Significant association between increased risk of emergency department visits for psychiatric disorders and air pollutants in South Korea. J. Expo. Sci. Environ. Epidemiol. https://doi.org/10.1038/s41370-022-00504-y (2022).
Braithwaite, I. et al. Air pollution (particulate matter) exposure and associations with depression, anxiety, bipolar, psychosis and suicide risk: A systematic review and meta-analysis. Environ. Health Perspect. 127(12), 126002 (2019).
Wu, Z. et al. Attributable risk and economic cost of hospital admissions for mental disorders due to PM(2.5) in Beijing. Sci. Total Environ. 718, 137274 (2020).
Lee, S. et al. Short-term PM(2.5) exposure and emergency hospital admissions for mental disease. Environ. Res. 171, 313–20 (2019).
Buoli, M. et al. Is there a link between air pollution and mental disorders?. Environ. Int. 118, 154–68 (2018).
Casanova, R. et al. A voxel-based morphometry study reveals local brain structural alterations associated with ambient fine particles in older women. Front. Hum. Neurosci. 10, 495 (2016).
Wilker, E. H. et al. Long-term exposure to fine particulate matter, residential proximity to major roads and measures of brain structure. Stroke 46(5), 1161–6 (2015).
Thiankhaw, K., Chattipakorn, N. & Chattipakorn, S. C. PM2.5 exposure in association with AD-related neuropathology and cognitive outcomes. Environ. Pollut. 292(Pt A), 118320 (2022).
Toledo-Corral, C. M. et al. Ambient air pollutants are associated with morning serum cortisol in overweight and obese Latino youth in Los Angeles. Environ. Health 20(1), 39 (2021).
Acknowledgements
Authors of this manuscript would like to thank all study investigators.
Funding
This work was supported by the Special Fund Project of the Central Government to Guide the Local Science and Technology Development of Hebei Province [grant numbers [199477138G], National Science Foundation of Hebei Province[No. H2022206544], the Government funded Clinical Medicine Excellent Talents Training Project of Hebei Province [LS202009]. Science and Technology Program of Hebei Province [SG2021189].
Author information
Authors and Affiliations
Contributions
L.W.: Investigation, Formal analysis, Writing-original draft. X.G.: Formal analysis, Data curation. R.W.: Investigation. M.S.: Investigation. X.L.: Investigation. X.W.: Conceptualization. C.A.: Conceptualization, Funding acquisition, Writing –review & editing. The author(s) read and approved the final manuscript. Permission for publication was obtained from The First Hospital of Hebei Medical University.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.





Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cite this article
Wang, L., Gao, X., Wang, R. et al. Ecological correlation between short term exposure to particulate matter and hospitalization for mental disorders in Shijiazhuang, China. Sci Rep 13, 11412 (2023). https://doi.org/10.1038/s41598-023-37279-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-37279-7
- Springer Nature Limited