
Abstract
Studies have demonstrated that exercise benefits executive function. However, it remains unclear which type of exercise is optimal for preserving executive function among young adults and the cerebral blood flow (CBF) mechanisms that underlie exercise-induced cognitive benefits. Therefore, this study aims to compare the intervention effects of high-intensity interval training (HIIT) and moderate-intensity continuous training (MICT) on executive function and the CBF mechanism. This was a double-blinded, randomized, controlled trial study conducted between October 2020 and January 2021 (ClinicalTrials.gov identifier: NCT04830059). Ninety-three healthy young adults (25.23 ± 2.18 years old; 49.82% male) were randomized into the HIIT (N = 33), MICT (N = 32), and control (N = 28) groups. Participants in exercise groups were guided to perform 40 min of HIIT and MICT three times a week for 12 weeks, while the control group received health education for the same period. The primary outcomes, changes in executive function assessed by the trail-making test (TMT), and CBF measured by transcranial Doppler flow analyzer (EMS-9WA), were evaluated before and after the interventions. The time taken to complete the TMT task improved significantly in the MICT group compared to the control group [β = −10.175, 95%, confidence interval (CI) = −20.320, −0.031]. Additionally, the MICT group showed significant improvements in the pulsatility index (PI) (β = 0.120, 95% CI = 0.018, 0.222), resistance index (RI) (β = 0.043, 95% CI = 0.005, 0.082), and peak-systolic/end-diastolic velocity (S/D) (β = 0.277, 95% CI = 0.048, 0.507) of CBF compared to the control group. The time taken to complete the TMT was associated with the velocity of peak-systolic (F = 5.414, P = 0.022), PI (F = 4.973, P = 0.012), and RI (F = 5.845, P = 0.006). Furthermore, the accuracy of TMT was associated with PI (F = 4.797, P = 0.036), RI (F = 5.394, P = 0.024), and S/D (F = 4.312, P = 0.05) of CBF. A 12-week MICT intervention improved CBF and executive function more effectively than HIIT among young adults. Furthermore, the findings suggest that CBF was one of the potential mechanisms underlying the cognitive benefits of exercise in young people. These results provide practical evidence supporting the promotion of regular exercise to maintain executive function and improve brain health.
Similar content being viewed by others


Introduction
Studies have reported the positive effect of exercise on the musculoskeletal system1, cardiovascular system2, respiratory system3, and other physical functions4. However, the benefits of exercise extend beyond physical health, and physically active individuals exhibit better neurocognitive function than inactive individuals5. Executive function is a central component of cognition, known to influence various cognitive processes relevant to many domains of daily living, including academic achievement4, vocational performance6, and quality of life7. The effects of exercise training on cognitive function are reported to be the largest for executive function compared to other cognitive domains8. Regular exercise improves executive function among adolescents, older adults, and even patients with cognitive impairments9,10. Prior studies confirmed that acute exercise could enhance working memory, processing speed, attention, and inhibition11,12. Limited research has explored the potential impact of chronic exercise on memory and cognitive control among young adults13,14,15. Nonetheless, further investigation is required to confirm the benefits of chronic exercise on executive function, particularly among young adults whose cognitive capacity is at its peak.
Aerobic exercise, including moderate-intensity continuous training (MICT), can enhance cognitive performance throughout the life span16. The available evidence emphasizes the significance of promoting physical activity across the lifespan to enhance cognitive abilities, counteract neural degeneration, and prevent neurodegenerative disease17,18,19. Over the past few years, a mounting body of evidence has demonstrated the efficiency of high-intensity interval training (HIIT), which involves alternating high-intensity exercise bouts with periods of rest (e.g., 30 s of high-intensity activity followed by 30 s of rest, repeated for 5 min), for enhancing physical and psychological health-related outcomes20,21. Compared to aerobic exercise, HIIT can achieve similar physiological adaptations within a shorter time frame22. Several studies have indicated that HIIT leads to greater improvements in cardiorespiratory fitness and vascular function compared to MICT23,24. Moreover, HIIT has been shown to enhance memory performance to a greater extent than MICT among sedentary elderly individuals25. HIIT has been shown to increase the production of lactic acid in the body, which can serve as an energy substrate in the brain and support brain metabolism26. Furthermore, lactic acid has been found to play a pivotal role in long-term potentiation and improvements in cognitive function27. However, few studies compared the effects of different modalities of chronic exercise on executive function, especially the cognitive benefit of exercise among young adults28. Such studies would be valuable in guiding physical activity recommendations for this population.
Despite accounting for only 2% of the human body mass, the brain consumes approximately one-fifth of the cardiac output, making it the most metabolically active organ in the human body29. Maintaining a relatively constant cerebral blood flow (CBF) is fundamental to preserving normal brain function and metabolic activities30. Previous research has suggested that no effect of acute exercise on CBF or cerebrovascular reactivity in the intracranial or extracranial arteries among young adults, indicating that CBF is rapidly and uniformly regulated after acute exercise31. However, evidence has shown that exercise training can alter CBF in older adults, with or without cognitive impairment32, and that the decrease in CBF could be mitigated by two-minute light-intensity walking breaks every 30 min33. Research indicated that one week of aerobic and resistance exercise training could selectively increase the blood flow in hippocampal regions34. In terms of the effect of exercise on CBF and cognition, evidence has demonstrated that CBF regulation partially mediates the link between physical activity and cognition in older adults, and that improvements in CBF regulation are associated with better cognitive functioning35. Specifically, increased middle cerebral artery blood velocity has been identified as a potential mechanism through which exercise can prevent cerebrovascular and neurological diseases36. Animal studies also revealed that exercise could increase the number of neurons in the hippocampus of rats with bilateral common carotid artery embolism and delay cognitive decline by promoting neurogenesis and enhancing the expression of brain-derived neurotrophic factor37. Exercise increases the production of neurotrophic and vascular growth factors, which promote new growth and plasticity and help maintain the structural integrity of the brain and cerebrovascular system23. This mechanism may help explain the effect of exercise on CBF. Thus, it is plausible to hypothesize that exercise training could enhance the executive function of young individuals by improving cerebral blood flow.
Therefore, despite the common assumption that cognitive functioning is at its peak in healthy young adults, recent research has indicated a positive association between habitual physical activity and cognitive performance38. Nevertheless, few studies have investigated the effects of exercise interventions on cognitive function and CBF in young individuals, and evidence is lacking regarding the potential CBF mechanisms underlying exercise-related improvements in executive function. Therefore, the present study aims to (1) compare the effects of 12 weeks of MICT and HIIT on cognitive function in young adults, and (2) investigate the potential role of cerebral blood flow mechanisms in the exercise-induced improvements in executive function.
Results
Descriptive analysis of the demographic information
The descriptive analysis of the study population is indicated in Table 1. Sixty-seven subjects were included in the data analysis (HIIT = 26, MICT = 21, control group = 20), and all participants were analyzed according to the initial grouping. There were no significant differences among groups in the demographic information, including age, height, Body Mass Index (BMI), years of education, and birthplace. No significant difference was found in baseline maximum oxygen uptake (VO2 max) between groups. Overall, 49.82% of the study population was male. Participants across all three groups were 25.23 ± 2.18 years old on average, with a mean BMI of 21.91 ± 2.92 kg/m2. The mean VO2 max of all the participants was 43.71 ± 6.98 mL/(kg·min). No significant differences were found in subjective fatigue and enjoyment between the MICT and HIIT groups, as measured by the rating of perceived exertion scale (RPE) and the physical activity enjoyment scale (PACES) (Supplementary Table S1). Furthermore, both the HIIT and MICT groups showed a decrease in blood pressure (systolic and diastolic) and resting heart rate after the intervention compared to the control group (Supplementary Table S2). However, no association was found between blood pressure and CBF.
Effects of exercise intervention on executive function
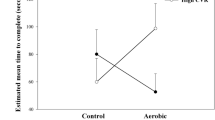
The cognitive differences between groups after three months of intervention indicated that the time of the TMT task among the MICT group improved significantly compared with the control group (β = −10.175, 95% CI = −20.320, −0.031). No significant difference was found in reaction time (RT) when comparing the HIIT vs. control groups and HIIT vs. MICT groups (Table 2). The reaction time of the TMT task improved significantly among MICT (estimated value = −17.34, P < 0.01) and HIIT (estimated value = −10.77, P < 0.01) groups after the 12-week intervention (Fig. 1 and Supplementary Table S4). Moreover, the accuracy of the TMT task improved in the MICT group (estimated value = 0.04, P < 0.05). The intra-group and inter-group comparisons indicated that three months of MICT and HIIT intervention improved the executive function of young adults, and MICT is more beneficial.

The effect of pre-post effect after 12-week intervention on cognitive performance and CBF. Executive function and CBF indicators measured in pre-post of 12-week exercise interventions. MICT moderate-intensity continuous training, HIIT high-intensity interval training. The estimated values of pairwise analysis between pre and post-measurement in different groups were shown in the subgraph (A–H). Asterisk: a statistically significant difference between groups during the pre-post intervention period. *p < 0.05; **p < 0.01.
Effects of exercise intervention on cerebral blood flow
The coefficient of variation of the CBF was shown in Supplementary Table S3. The pulsatility index (PI) (estimated value = 0.10, P < 0.01), resistance index (RI) (estimated value = 0.03, P < 0.01), and peak-systolic of cerebral blood flow/end-diastolic of cerebral blood flow (S/D) (estimated value = 0.23, P < 0.01) increased significantly among the MICT group after three months of intervention (Fig. 1 and Supplementary Table S4). The cognitive difference between groups after 3 months of the intervention indicated that the PI (β = 0.120, 95% CI = 0.018, 0.222), RI (β = 0.043, 95% CI = 0.005, 0.082), and S/D (β = 0.277, 95% CI = 0.048, 0.507) of the CBF among MICT group improved significantly compared with the control group (Table 2). We did not observe a significant change in the CBF index among the HIIT group after 3 months of intervention compared with the control group.
Associations between the cerebral blood flow and executive function
To assess dose–response and possible nonlinearity, we plotted bivariate associations of executive function and CBF using generalized additive models with the penalized spline. The results showed that the association of the accuracy of TMT with PI, RI, and S/D was approximately linear, while the time of TMT and CBF index were non-linear. (Fig. 2 and Supplementary Table S5). The time of TMT was associated with the velocity of peak-systolic (Vs) (F = 5.414, P = 0.022), PI (F = 4.973, P = 0.012), and RI (F = 5.845, P = 0.006). Moreover, the accuracy of TMT was associated with PI (F = 4.797, P = 0.036), RI (F = 5.394, P = 0.024), and S/D (F = 4.312, P = 0.05). The results indicated that the Vs, PI, and RI of CBF were associated with the time of TMT, and the PI, RI, and S/D of CBF were associated with the accuracy of TMT.

The dose–response associations between the executive function and CBF. TMT trail-making test, S/D peak-systolic of cerebral blood flow/end-diastolic of cerebral blood flow. Dose–response relationships were estimated by the generalized additive model with the penalized spline.
Materials and methods
Study design and population
We conducted a double-blind, randomized controlled trial (RCT) study from October 2020 to January 2021 using randomization, assignment concealment, and blinding methods (ClinicalTrials.gov identifier: NCT04830059. Data: 02/04/2021). Ninety-three participants met the inclusion criteria and were randomized into three groups: HIIT (N = 32), MICT (N = 33), and control (N = 28). Demographic information was collected, including age, gender, height, weight, family income, education level, and birthplace (rural or urban). Each participant had a unique identification number. They were randomly divided into different groups using a random number generator. The randomization process was carried out by a research staff member who did not participate in the assessment and analysis of the data. Group allocation was confidential to ensure the successful implementation of randomization. The participants’ identification number and grouping information were hidden in an opaque envelope, which was opened by themselves after the baseline assessment. Moreover, participants in the three groups came to the fitness centre on different days of the week, so they did not know the existence of other groups. Participants and evaluators were blinded to the group allocation of intervention assignments throughout the study. Detailed information on the randomization, assignment concealment, and blinding methods is described in the previous article39.
The sample size was calculated by the software of G-Power (Version 3.1.9.7). The effect sizes of exercise interventions on cognition ranges from 0.19 to 0.59 according to the previous studies12. For the repeated measures one-way analysis of variance (ANOVA) test, we assumed that the effect size of the exercise intervention was 0.4 (Cohen’s f = 0.40), 0.05 for “α error probability,” and 0.8 for “power (1 − β error probability)”40. Moreover, the study included three groups (MICT, HIIT, and control group). According to the G-Power software, a total sample size of 64 is needed in this study. Therefore, 100 individuals were initially recruited for this study, of whom 93 were found to meet the inclusion criteria.The trial profile is provided in Fig. 3. The inclusion criteria for this study were as follows: (1) healthy young college students aged 20–30 years with normal BMI, who reported no history of cardiovascular, cerebrovascular, or respiratory disease and were not taking any cardiovascular medications; (2) individuals with normal or corrected vision; (3) participants who reported being physically inactive in the past six months, as determined by the International Physical Activity Questionnaire screening; and (4) individuals without musculoskeletal conditions that could impede participation in physical activity39.

The CONSORT flow diagram. MICT moderate-intensity continuous training, HIIT high-intensity interval training, CON control, CBF cerebral blood flow.
This study was conducted in accordance with the International Conference on Harmonization guidelines for Good Clinical Practice and the Declaration of Helsinki. The academic ethics committee of Tsinghua university approved this study (IRB 20190091). All participants provided written informed consent prior to participation.
Procedures and interventions
Procedures
One week before the formal experiment after the group assignment, the participants were informed to wear comfortable sportswear and shoes to the laboratory for a VO2max test to determine the individual intensity of exercise training. The outcomes were assessed at the beginning of the first visit and on the second day of the final visit of the interventions. Specifically, on the first day of the intervention, all the participants completed the baseline assessment of the outcomes (pre-test). After that, they performed different types of exercise interventions under the guidance and supervision of two professional coaches. The HIIT and MICT groups were intervened three times a week for 12 weeks, and the control group visited two times a week for the same intervention period. The outcomes were repeatedly measured on the second day morning of the final visit (post-test). To minimize the impact of biological rhythms and dietary factors, participants were instructed to fast for 12 h before the two measurements(pre-test and post-test) and to abstain from eating after 8:00 PM on the preceding night. They were advised to sleep before 11:00 PM the night before to ensure adequate rest. All the measurements were scheduled in the morning between 8:00 AM and 12:00 PM. In the two repeated evaluations before and after the intervention, all the outcomes were measured by the same evaluator, respectively, to prevent measurement errors. Additionally, we conducted an assessment to identify any significant life events that may have influenced the participants’ condition, such as the loss of significant individuals, academic or work-related failures, and other significant setbacks. All the outcomes were measured in the laboratory, and the interventions were completed in the university’s fitness centre. To ensure completion of the experiment, participants were provided with appropriate compensation, including 200 RMB and other gift rewards. The schematic diagram of experimental procedures is described in Supplementary Fig. S1.
Interventions
The individual intensity of exercise interventions was determined by the maximum oxygen uptake for each participant. VO2 max was proven to be more accurate in determining the individual intensity of exercise intervention41. Cosmed Fitmate metabolic system (Cosmed, Rome, Italy) was used to obtain the parameters of oxygen consumption and VO2 max when the participants performed Bruce’s treadmill protocol42. The participants ran on the treadmill at a fixed speed and then gradually increased until they met the following criteria: (1) felt exhausted and unable to continue running anymore, with a score of RPE ≥ 19; (2) had symptoms of dyspnea, dizziness, extreme fatigue, or pale face. (3) arrhythmia; (4) The respiratory quotient was greater than or equal to 1.139,43.
We developed the training protocol referring to the previous studies44,45,46. The MICT group participants were instructed to run for 20 min at a running speed equivalent to 70–75% of their individual VO2 max. The HIIT group participants were directed to perform a running exercise protocol consisting of one minute at a speed equivalent to 100% of their individual VO2 max, followed by one minute of running at a speed equivalent to 50% of their individual VO2 max. This protocol was repeated ten times, with a total exercise duration of 20 min39. To monitor the real-time running speed, participants wore a heart rate band (Polar H10, Finland) on their chest. A 10-min warm-up and cool-down were performed before and after the 20-min intervention of HIIT and MICT, respectively, resulting in a total intervention time of 40 min. The control group participants were provided with health education lessons that did not involve any exercise. The health education primarily focused on four aspects: (1) assessment of body posture; (2) techniques for adjusting physical posture; (3) methods for stretching and relaxation; and (4) evaluation of body composition39.
Primary outcomes
Executive function
The executive function was measured by the accuracy and reaction time of the Trail Making Test (TMT) based on the computer task, which is widely used among young adults because of its high reliability and validity47,48. The screen presented 13 disordered numbers from 1 to 13 and letters from A to L at random. The participants needed to alternately connect the numbers and letters in order quickly and accurately (e.g., 1 with A, A with 2, and 2 with B). The reaction time and accuracy of the TMT were collected from all participants before and after the intervention.
Blood flow velocity
The diastolic and systolic CBF velocities of the participants’ middle cerebral artery of the brain were measured by a transcranial Doppler (TCD) flow analyzer (EMS-9WA) before and after interventions49. TCD ultrasound is a non-invasive and cost-effective sensing method. It measures cerebral blood velocities with high temporal resolution50. Vs, the velocity of end-diastolic (Vd), and the velocity of mean cerebral blood flow (Vm) of the participants were detected using a 2 MHz TCD probe over their temporal window. Insonation of the middle cerebral artery(MCA) was confirmed using established criteria, including the position and orientation of the probe, insonation depth, and direction of blood flow about the probe51. All repeated measurements within each participant were taken by a single, trained investigator at the same probe depth and position to ensure the recapture of the same cerebral artery. In addition, PI was calculated using the following formula: PI = (Vs − Vd)/Vm, as a measure of the downstream resistance in the cerebral arteries52. RI and S/D were calculated as RI = (Vs − Vd)/Vs, S/D = Vs/Vd.
Secondary outcomes
The feeling of subjective fatigue and enjoyment of exercise
We also measured the subjective feeling and enjoyment of HIIT and MICT before and after the acute exercise on the first day of the intervention. Participants’ fatigue feeling and exertion degree were recorded by the rating of RPE53. Studies have shown that RPE is highly believable and widely used to reflect the subjective feeling in the exercise process regarding strength, tension, fatigue, or other discomforts. Meanwhile, the PACES was employed to evaluate the subjective degree of enjoyment in carrying out physical activity. Higher scores reflect greater levels of enjoyment54. As the secondary outcome, we assessed the PACES of the participant during the first visit of the exercise intervention.
Blood pressure
Blood pressure (BP) and resting heart rate were measured using an automatic sphygmomanometer (YE670A, China). Blood pressure and resting heart rate of all participants were measured on the first day of the intervention in the morning and then repeatedly after the 12-week intervention. They were asked to sit quietly for 10 min before the test when they came to the lab. The measurement was performed twice, and the mean value was used to represent their blood pressure.
Statistical analyses
We conducted a descriptive analysis to obtain the frequency and percentage for categorical variables and mean and standard deviation (SD) for continuous variables. We used a one-way analysis of variance (ANOVA) for continuous variables and the chi-square test for categorical variables to determine differences between groups at baseline. Given the study's repeated measurement design, we utilized mixed-effect models with a random effect on individuals nested within the group to account for intrapersonal variation (R-packages: lme4). In this study, we employed a mixed-effect model that comprised the fixed effect of groups (control, MICT, and HIIT) and measurement time (pre and post-test), while controlling for gender, age, education level, residence, self-perceived income level, and body mass index (BMI) as covariates. The interaction effect of measurement time and groups indicated the changes in group differences from pre to post-test, which indicated the causal effect of the intervention. Pairwise comparisons of changing outcomes between groups during the intervention period were further performed (R-packages: emmeans). The generalized additive model with penalized spline was used to estimate the possible nonlinearity dose–response correlations between the performance of TMT response and CBF controlling the measurement time, education, birthplace, age, and BMI. Moreover, the independent sample t-test was used to compare PACES and RPE results among HIIT and MICT groups.
We performed a series of sensitivity analyses to assess the robustness of our findings: (1) We reran the main analysis using repeated measures analysis of variance; (2) we also re-analyzed the association of CBF and executive function using a generalized linear model (Supplementary Table S6). All data analysis and visualization were conducted using R software (Version 4.1.2), and a p-value less than 0.05 were considered statistically significant.
Discussion
In the 12-week double-blinded RCT study, we investigated the effect of HIIT and MICT on executive function in young adults and explored the potential underlying mechanism of exercise on cognitive performance through CB. Our findings revealed that cognitive performance improved significantly in both the HIIT and MICT groups, with MICT showing greater benefits. These results suggest that even in young adults with peak cognitive ability, exercise, especially MICT, can enhance executive function. We also observed a significant improvement in CBF, as evidenced by increased PI, RI, and S/D, in the MICT group after the 12-week intervention. Furthermore, we identified a significant association between CBF and executive function, suggesting that CBF may represent a potential mechanism through which exercise enhances executive function.
After a 12-week intervention, we observed a significant improvement in executive function among both the HIIT and MICT groups in young adults, with MICT demonstrating greater benefits. These findings are consistent with a previous study that investigated the effects of 12 weeks of combined aerobic and resistance exercise on neurocognitive performance in obese women. The study reported improvements in physical fitness, weight status, and cognitive interference inhibition following the intervention55. Furthermore, previous studies have demonstrated that long-term MICT and HIIT can enhance executive function in healthy elderly individuals and those with Alzheimer’s disease, which is in line with our finding10,56. Previous research has reported that six months of MICT (three days per week of 20–40 min at 30–70% heart rate reserve) augmented executive function in older adults, and this improvement has been associated with an enhancement in cerebrovascular regulation57. Additionally, chronic exercise has been found to have positive effects on the executive function of overweight children58. However, a previous study suggested that improving executive function may be more challenging in younger populations, as there may be less room for improvement22. Thus, our findings have expanded the population that may benefit from exercise on cognitive performance.
We sought to explore whether different exercise modalities (MICT and HIIT) had comparable effects on enhancing executive function in young adults. Our results demonstrated that the MICT intervention was more effective than HIIT after 12 weeks of interventions. This finding is consistent with a previous article, which reported that aerobic exercise, such as MICT, can create a nutritive environment in the brain by facilitating cortical activity, hemodynamics, and metabolism59. However, in older adults, evidence suggests that HIIT elicits more significant blood flow responses and fluctuations in metabolic intensity compared to MICT, leading to more remarkable changes in cerebrovascular function after six weeks of intervention60. These beneficial effects could translate to favourable improvements in higher-order cognitive functions60. HIIT seems to provide greater beneficial effects by increasing the amount of neurotrophic factor61,62. However, the inconsistent findings of previous studies on the effects of HIIT and MICT interventions may be attributed to variations in study populations and intervention duration. Additionally, prolonged HIIT may lead to fatigue, decreased cerebral oxygenation, and elevated blood lactate levels, which may reduce its facilitative effects63. Our study provides guidance for young adults to choose appropriate exercise modalities to enhance executive function and maintain brain health in real-life settings.
Following the 12-week intervention, statistically significant differences were observed in PI, RI, and S/D of the CBF, particularly in MICT group. Research has demonstrated that changes in CBF are intensity-dependent, with CBF velocity in the MCA increasing linearly with exercise intensity until approximately 60–70% of maximal VO2 max, as reported in previous studies64,65. Regarding the long-term effect of exercise on CBF, a previous longitudinal study observed an age-related decline in middle cerebral artery blood velocity (MCAv), which was consistently elevated in endurance-trained men across all age ranges66. Additionally, previous research has reported that a 12-week aerobic exercise training program significantly increased MCAv in both young and older participants67. The PI of the cerebral artery is widely regarded as an indicator of downstream arterial resistance68. Sympathetic nervous system activation during exercise has been reported to increase cerebral PI69. Consistent with prior findings, our study revealed an elevated PI value at rest, which may contribute to the increased Vs observed in the exercise groups70. A previous study also reported an elevation in MCAv and a reduction in resting heart rate following 12-week training, suggesting similar physiological adaptations in response to exercise70. However, the underlying mechanisms responsible for the observed changes in Vs in healthy young adults require further investigation.
Several studies have reported the effect of exercise on cognitive function, often focusing on changes in brain activation and synaptic plasticity assessed using fMRI and EEG in humans71. However, there is a lack of evidence regarding the underlying CBF mechanisms that contribute to the exercise-induced improvement of executive function. In this study, we examined the effect of exercise on CBF and found a significant association between CBF and executive function in young adults, providing insights into the CBF mechanisms underlying the exercise-cognition relationship. Consistent with our findings, animal studies have shown that long-term exercise induces angiogenesis and neurogenesis in the brain, leading to increased cerebral perfusion and metabolism72,73, which manifests as increased cerebral perfusion and metabolism74. In middle-aged animals, aerobic exercise also enhances vascular growth factor production and promotes angiogenesis, supporting optimal cerebrovascular functioning75,76, These findings may explain the link between exercise training, CBF, and higher executive function59.
Some limitations should be acknowledged in this study. Firstly, 12 weeks of intervention is relatively short for improving young adults’ CBF and executive function. Future studies with extended intervention periods are preferred to further explore the benefits. Secondly, our sample was small considering the methodological limitations, such as the challenges of CBF assessment with transcranial Doppler ultrasonography due to the thickness of the temporal bone, which even resulted in some participants from whom no signal could be acquired at all. However, all the CBF indexes were assessed by the same researcher and measured in a similar way during the whole process of the research. Additionally, we checked and confirmed data quality during preprocessing to ensure the measurement validity of CBF. Thirdly, the intermediary effect of CBF was not found, which may be due to the small sample size. We were able to identify a significant association between CBF and executive function. Thus, well-designed randomized controlled trials with larger sample sizes are needed to assess the effects of exercises on executive function and the mediation mechanism of CBF. Finally, the RCT study was conducted in a population of healthy young adults, so the study findings may not be generalizable to older people and clinical patients. However, this study also has notable strengths. First, to the best of our knowledge, this is the first double-blind RCT study that provides direct evidence comparing the effects of MICT and HIIT interventions on executive function in young adults. Secondly, to determine the appropriate MICT and HIIT protocol, an individual’s maximal oxygen uptake was measured through a laboratory cardiopulmonary exercise test. This approach is considered more precise than other methods employed in previous studies. Most importantly, this randomized controlled trial study provides valuable insights into the causal effects of MICT/HIIT intervention on executive function. Moreover, the evidence will be necessary for understanding why exercise can improve executive function and further confirm the CBF mechanism of exercise on executive function. The results provided suggestions to young adults when choosing different modalities of exercise in real life to improve executive function and maintain brain health.
Conclusions
This study is the first to demonstrate that a 12-week MICT intervention improves CBF and executive function to a greater extent than HIIT in young adults. Moreover, our findings suggest that CBF is a potential mechanism underlying the exercise-induced enhancement of executive function in young individuals, providing practical evidence to encourage regular exercise for maintaining cognitive function and promoting brain health.
Data availability
The dataset used and/or analysed during this current study are not publicly available as the raw dataset has incorporated with participants identifiable information, but are available from the corresponding author on reasonable request.
References
Folland, J. P. & Williams, A. G. The adaptations to strength training : Morphological and neurological contributions to increased strength. Sports Med. 37, 145–168. https://doi.org/10.2165/00007256-200737020-00004 (2007).
Fiuza-Luces, C. et al. Exercise benefits in cardiovascular disease: Beyond attenuation of traditional risk factors. Nat. Rev. Cardiol. 15, 731–743. https://doi.org/10.1038/s41569-018-0065-1 (2018).
Gloeckl, R., Schneeberger, T., Jarosch, I. & Kenn, K. Pulmonary rehabilitation and exercise training in chronic obstructive pulmonary disease. Dtsch. Arztebl. Int. 115, 117–123. https://doi.org/10.3238/arztebl.2018.0117 (2018).
Wang, S. & Gathercole, S. E. Working memory deficits in children with reading difficulties: Memory span and dual task coordination. J. Exp. Child Psychol. 115, 188–197 (2013).
Flöel, A. et al. Physical activity and memory functions: Are neurotrophins and cerebral gray matter volume the missing link?. Neuroimage 49, 2756–2763. https://doi.org/10.1016/j.neuroimage.2009.10.043 (2010).
Bailey, C. E. Cognitive accuracy and intelligent executive function in the brain and in business. Ann. N. Y. Acad. Sci. 1118, 122–141. https://doi.org/10.1196/annals.1412.011 (2007).
Davis, J. C., Marra, C. A., Najafzadeh, M. & Liu-Ambrose, T. The independent contribution of executive functions to health related quality of life in older women. BMC Geriatr. 10, 16. https://doi.org/10.1186/1471-2318-10-16 (2010).
Fang, et al. Affecting cognition and quality of life via aerobic exercise in Alzheimer’s disease. West. J. Nurs. Res. 35, 24–38 (2011).
Brown, A. D. et al. Effects of cardiorespiratory fitness and cerebral blood flow on cognitive outcomes in older women. Neurobiol. Aging 31, 2047–2057 (2010).
Erickson, K. I. et al. Exercise training increases size of hippocampus and improves memory. Proc. Natl. Acad. Sci. USA 108, 3017–3022. https://doi.org/10.1073/pnas.1015950108 (2011).
Weng, T. B., Pierce, G. L., Darling, W. G. & Voss, M. W. Differential effects of acute exercise on distinct aspects of executive function. Med. Sci. Sports Exerc. 47, 1460–1469. https://doi.org/10.1249/mss.0000000000000542 (2015).
Haverkamp, B. F. et al. Effects of physical activity interventions on cognitive outcomes and academic performance in adolescents and young adults: A meta-analysis. J. Sports Sci. 38, 2637–2660. https://doi.org/10.1080/02640414.2020.1794763 (2020).
Lennemann, L. M. et al. The influence of agility training on physiological and cognitive performance. J. Strength Cond. Res. 27, 3300–3309. https://doi.org/10.1519/JSC.0b013e31828ddf06 (2013).
Heisz, J. J. et al. The effects of physical exercise and cognitive training on memory and neurotrophic factors. J. Cogn. Neurosci. 29, 1895–1907. https://doi.org/10.1162/jocn_a_01164 (2017).
Stroth, S. et al. Impact of aerobic exercise training on cognitive functions and affect associated to the COMT polymorphism in young adults. Neurobiol. Learn. Mem. 94, 364–372. https://doi.org/10.1016/j.nlm.2010.08.003 (2010).
Hillman, C. H., Erickson, K. I. & Kramer, A. F. Be smart, exercise your heart: Exercise effects on brain and cognition. Nat. Rev. Neurosci. 9, 58–65. https://doi.org/10.1038/nrn2298 (2008).
Law, C. K., Lam, F. M., Chung, R. C. & Pang, M. Y. Physical exercise attenuates cognitive decline and reduces behavioural problems in people with mild cognitive impairment and dementia: A systematic review. J. Physiother. 66, 9–18. https://doi.org/10.1016/j.jphys.2019.11.014 (2020).
Brasure, M. et al. Physical activity interventions in preventing cognitive decline and Alzheimer-type dementia: A systematic review. Ann. Intern. Med. 168, 30–38. https://doi.org/10.7326/m17-1528 (2018).
Martin, A. et al. Physical activity, diet and other behavioural interventions for improving cognition and school achievement in children and adolescents with obesity or overweight. Cochrane Database Syst. Rev. 1, CD009728. https://doi.org/10.1002/14651858.CD009728.pub3 (2018).
Costigan, S. A. et al. Preliminary efficacy and feasibility of embedding high intensity interval training into the school day: A pilot randomized controlled trial. Prev. Med. Rep. 2, 973–979. https://doi.org/10.1016/j.pmedr.2015.11.001 (2015).
Costigan, S. A., Eather, N., Plotnikoff, R. C., Hillman, C. H. & Lubans, D. R. High-intensity interval training for cognitive and mental health in adolescents. Med. Sci. Sports Exerc. 48, 1985–1993. https://doi.org/10.1249/mss.0000000000000993 (2016).
Eather, N. et al. Efficacy and feasibility of HIIT training for university students: The Uni-HIIT RCT. J. Sci. Med. Sport 22, 596–601. https://doi.org/10.1016/j.jsams.2018.11.016 (2019).
Hötting, K. & Röder, B. Beneficial effects of physical exercise on neuroplasticity and cognition. Neurosci. Biobehav. Rev. 37, 2243–2257 (2013).
Ramos, J. S., Dalleck, L. C., Tjonna, A. E., Beetham, K. S. & Coombes, J. S. The impact of high-intensity interval training versus moderate-intensity continuous training on vascular function: A systematic review and meta-analysis. Sports Med. 45, 679–692 (2015).
Kovacevic, A., Fenesi, B., Paolucci, E. & Heisz, J. J. The effects of aerobic exercise intensity on memory in older adults. Appl. Physiol. Nutr. Metab. 45, 591–600. https://doi.org/10.1139/apnm-2019-0495 (2020).
Finsterwald, C., Magistretti, P. J. & Lengacher, S. Astrocytes: New targets for the treatment of neurodegenerative diseases. Curr. Pharm. Des. 21, 3570–3581. https://doi.org/10.2174/1381612821666150710144502 (2015).
Bélanger, M., Allaman, I. & Magistretti, P. J. Brain energy metabolism: Focus on astrocyte-neuron metabolic cooperation. Cell Metab. 14, 724–738. https://doi.org/10.1016/j.cmet.2011.08.016 (2011).
Calverley, T. A. et al. HIITing the brain with exercise: Mechanisms, consequences and practical recommendations. J. Physiol.-Lond. 598, 2513–2530. https://doi.org/10.1113/Jp275021 (2020).
Bundgaard-Nielsen, M., Sørensen, H., Dalsgaard, M., Rasmussen, P. & Secher, N. H. Relationship between stroke volume, cardiac output and filling of the heart during tilt. Acta Anaesthesiol. Scand. 53, 1324–1328. https://doi.org/10.1111/j.1399-6576.2009.02062.x (2009).
Singh, V. & Cheng, R. in Handbook of Clinical Neurology. Vol. 176 (eds. Hetts, S.W. & Cooke, D.L.). 71–80 (Elsevier, 2021).
Steventon, J. J. et al. Cerebrovascular function in the large arteries is maintained following moderate intensity exercise. Front. Physiol. 9, 1657. https://doi.org/10.3389/fphys.2018.01657 (2018).
Alfini, A. J., Weiss, L. R., Nielson, K. A., Verber, M. D. & Smith, J. C. Resting cerebral blood flow after exercise training in mild cognitive impairment. J. Alzheimers Dis. 67, 671–684. https://doi.org/10.3233/jad-180728 (2019).
Carter, S. E. et al. Regular walking breaks prevent the decline in cerebral blood flow associated with prolonged sitting. J. Appl. Physiol. 125, 790–798 (2018).
Steventon, J. J. et al. Changes in white matter microstructure and MRI-derived cerebral blood flow after 1-week of exercise training. Sci. Rep. 11, 22061. https://doi.org/10.1038/s41598-021-01630-7 (2021).
Guiney, H. et al. Evidence cerebral blood-flow regulation mediates exercise—Cognition links in healthy young adults. Neuropsychology 29, 1–9 (2015).
Murrell, C. J. et al. Cerebral blood flow and cerebrovascular reactivity at rest and during sub-maximal exercise: Effect of age and 12-week exercise training. Age (Dordr) 35, 905–920. https://doi.org/10.1007/s11357-012-9414-x (2013).
Choi, D. H., Lee, K. H. & Lee, J. Effect of exercise-induced neurogenesis on cognitive function deficit in a rat model of vascular dementia. Mol. Med. Rep. 13, 2981–2990. https://doi.org/10.3892/mmr.2016.4891 (2016).
Guiney, H. & Machado, L. Benefits of regular aerobic exercise for executive functioning in healthy populations. Psychon. Bull. Rev. 20, 73–86 (2013).
Liu, J. et al. Exercise improves mental health status of young adults via attenuating inflammation factors but modalities matter. Front. Psychiatry 13, 1067890. https://doi.org/10.3389/fpsyt.2022.1067890 (2022).
Kang, H. Sample size determination and power analysis using the G*Power software. J. Educ. Eval. Health Prof. 18, 17. https://doi.org/10.3352/jeehp.2021.18.17 (2021).
Hawkins, M. N., Raven, P. B., Snell, P. G., Stray-Gundersen, J. & Levine, B. D. Maximal oxygen uptake as a parametric measure of cardiorespiratory capacity. Med. Sci. Sports Exerc. 39, 103–107. https://doi.org/10.1249/01.mss.0000241641.75101.64 (2007).
Bruce, R. A., Kusumi, F. & Hosmer, D. Maximal oxygen intake and nomographic assessment of functional aerobic impairment in cardiovascular disease. Am. Heart J. 85, 546–562 (1973).
Hanson, N. J. et al. Modality determines VO2max achieved in self-paced exercise tests: Validation with the Bruce protocol. Eur. J. Appl. Physiol. 116, 1313–1319. https://doi.org/10.1007/s00421-016-3384-0 (2016).
Racil, G. et al. Effects of high vs. moderate exercise intensity during interval training on lipids and adiponectin levels in obese young females. Eur. J. Appl. Physiol. 113, 2531–2540. https://doi.org/10.1007/s00421-013-2689-5 (2013).
Poon, E. T., Siu, P. M., Wongpipit, W., Gibala, M. & Wong, S. H. Alternating high-intensity interval training and continuous training is efficacious in improving cardiometabolic health in obese middle-aged men. J. Exerc. Sci. Fit. 20, 40–47. https://doi.org/10.1016/j.jesf.2021.11.003 (2022).
Poon, E. T., Sheridan, S., Chung, A. P. & Wong, S. H. Age-specific affective responses and self-efficacy to acute high-intensity interval training and continuous exercise in insufficiently active young and middle-aged men. J. Exerc. Sci. Fit. 16, 106–111. https://doi.org/10.1016/j.jesf.2018.09.002 (2018).
Reitan, R. M. Validity of the trail making test as an indicator of organic brain damage. Percept. Mot. Skills 8, 271–276 (1958).
Flueckiger, L., Lieb, R., Meyer, A. H., Witthauer, C. & Mata, J. Day-to-day variations in health behaviors and daily functioning: Two intensive longitudinal studies. J. Behav. Med. 40, 307–319. https://doi.org/10.1007/s10865-016-9787-x (2017).
Phillips, A. A., Chan, F. H., Zheng, M. M., Krassioukov, A. V. & Ainslie, P. N. Neurovascular coupling in humans: Physiology, methodological advances and clinical implications. J. Cereb. Blood Flow Metab. 36, 647–664. https://doi.org/10.1177/0271678X15617954 (2016).
Tegeler, C. H. et al. Transcranial Doppler velocities in a large, healthy population. J. Neuroimaging 23, 466–472. https://doi.org/10.1111/j.1552-6569.2012.00711.x (2013).
Willie, C. K. et al. Utility of transcranial Doppler ultrasound for the integrative assessment of cerebrovascular function. J. Neurosci. Methods 196, 221–237. https://doi.org/10.1016/j.jneumeth.2011.01.011 (2011).
Gosling, R. G. & King, D. H. Arterial assessment by Doppler-shift ultrasound. Proc. R. Soc. Med. 67, 447–449 (1974).
Borg, G. A. V. Psychophysical bases of perceived exertion. Med. Sci. Sport Exerc. 14, 377–381. https://doi.org/10.1249/00005768-198205000-00012 (1982).
Deborah, K. & DeCarlo, K. J. Physical activity enjoyment scale: Two validation studies. J. Sport Exerc. Psychol. 13, 50–64 (1991).
Wen, H. J., Liu, S. H. & Tsai, C. L. Effects of 12 weeks of aerobic exercise combined with resistance training on neurocognitive performance in obese women. J. Exerc. Sci. Fit. 20, 291–304. https://doi.org/10.1016/j.jesf.2022.07.001 (2022).
Yu, F. et al. Affecting cognition and quality of life via aerobic exercise in Alzheimer’s disease. West. J. Nurs. Res. 35, 24–38. https://doi.org/10.1177/0193945911420174 (2013).
Guadagni, V., Drogos, L. L. & Tyndall, A. V. Aerobic exercise improves cognition and cerebrovascular regulation in older adults (vol 94, pg e2245, 2020). Neurology 95, 890–890. https://doi.org/10.1212/Wnl.0000000000010637 (2020).
Davis, C. L. et al. Exercise improves executive function and achievement and alters brain activation in overweight children: A randomized, controlled trial. Health Psychol. 30, 91–98. https://doi.org/10.1037/a0021766 (2011).
Quintero, A. P. et al. Acute effect of three different exercise training modalities on executive function in overweight inactive men: A secondary analysis of the BrainFit study. Physiol. Behav. 197, 22–28. https://doi.org/10.1016/j.physbeh.2018.09.010 (2018).
Mekari, S. et al. High-intensity interval training improves cognitive flexibility in older adults. Brain Sci. 10, 796. https://doi.org/10.3390/brainsci10110796 (2020).
Sarvat, S., Sabaghi, A., Yosofvand, N. & Ebrahimi, B. Effects of physical training in different modes on cognitive function and GNDF level in old mice. Neurophysiology 53, 132–139. https://doi.org/10.1007/s11062-022-09924-w (2022).
Martinez-Diaz, I. C., Escobar-Munoz, M. C. & Carrasco, L. Acute effects of high-intensity interval training on brain-derived neurotrophic factor, cortisol and working memory in physical education college students. Int. J. Environ. Res. Public Health 17, 8216. https://doi.org/10.3390/ijerph17218216 (2020).
Hsieh, S. S. et al. Systematic review of the acute and chronic effects of high-intensity interval training on executive function across the lifespan. J. Sport Sci. 39, 10–22. https://doi.org/10.1080/02640414.2020.1803630 (2021).
Ide, K. & Secher, N. H. Cerebral blood flow and metabolism during exercise. Prog. Neurobiol. 61, 397–414. https://doi.org/10.1016/s0301-0082(99)00057-x (2000).
Ogoh, S. & Ainslie, P. N. Regulatory mechanisms of cerebral blood flow during exercise: New concepts. Exerc. Sport Sci. Rev. 37, 123–129. https://doi.org/10.1097/JES.0b013e3181aa64d7 (2009).
Ainslie, P. N. et al. Elevation in cerebral blood flow velocity with aerobic fitness throughout healthy human ageing. J. Physiol.-Lond. 586, 4005–4010. https://doi.org/10.1113/jphysiol.2008.158279 (2008).
Murrell, C. J. et al. Cerebral blood flow and cerebrovascular reactivity at rest and during sub-maximal exercise: Effect of age and 12-week exercise training. Age 35, 905–920. https://doi.org/10.1007/s11357-012-9414-x (2013).
Kidwell, C. S. et al. Transcranial Doppler pulsatility indices as a measure of diffuse small-vessel disease. J. Neuroimaging 11, 229–235. https://doi.org/10.1111/j.1552-6569.2001.tb00039.x (2001).
Heckmann, J. G., Hilz, M. J., Mück-Weymann, M. & Neundörfer, B. Transcranial doppler sonography-ergometer test for the non-invasive assessment of cerebrovascular autoregulation in humans. J. Neurol. Sci. 177, 41–47. https://doi.org/10.1016/s0022-510x(00)00330-0 (2000).
Alwatban, M. R. et al. TCD cerebral hemodynamic changes during moderate-intensity exercise in older adults. J. Neuroimaging 30, 76–81. https://doi.org/10.1111/jon.12675 (2020).
Boecker, H. & Drzezga, A. A perspective on the future role of brain pet imaging in exercise science. Neuroimage 131, 73–80. https://doi.org/10.1016/j.neuroimage.2015.10.021 (2016).
Isaacs, K. R., Anderson, B. J., Alcantara, A. A., Black, J. E. & Greenough, W. T. Exercise and the brain: Angiogenesis in the adult rat cerebellum after vigorous physical activity and motor skill learning. J. Cereb. Blood Flow Metab. 12, 110–119. https://doi.org/10.1038/jcbfm.1992.14 (1992).
Black, M. A., Cable, N. T., Thijssen, D. H. & Green, D. J. Importance of measuring the time course of flow-mediated dilatation in humans. Hypertension 51, 203–210. https://doi.org/10.1161/HYPERTENSIONAHA.107.101014 (2008).
Nishijima, T. & Soya, H. Evidence of functional hyperemia in the rat hippocampus during mild treadmill running. Neurosci. Res. 54, 186–191. https://doi.org/10.1016/j.neures.2005.11.005 (2006).
Latimer, C. S. et al. Reversal of glial and neurovascular markers of unhealthy brain aging by exercise in middle-aged female mice. PLoS ONE 6, e26812. https://doi.org/10.1371/journal.pone.0026812 (2011).
Barnes, J. N. Exercise, cognitive function, and aging. Adv. Physiol. Educ. 39, 55–62. https://doi.org/10.1152/advan.00101.2014 (2015).
Acknowledgements
We appreciate the funding support from the project on on National Natural Science Foundation of China (No. 42277419), Ma John’s physical education thought and practice of Tsinghua University, China Postdoctoral Science Foundation (No. 2022M711858), and Social Project by the Ministry of Chinese Education (22YJC890024). The funders had no role in study design, data collection and analysis, the decision to publish, or the preparation of the manuscript. We appreciate the physical training and rehabilitation research centre of Tsinghua University for providing venues and professional coaches.
Author information
Authors and Affiliations
Contributions
X.D.M., Q.D. and J.X.L. contributed to conception and design of the study; L.Z.M. and J.X.L. completed the experiment; R.D.L., and L.Z.M. collected data of executive function and CBF; R.D.L., performed the intervention of different groups; X.Y.Z. and M.T.W., processed the data analysis; J.X.L. and L.Z.M. wrote and edited the manuscript; X.D.M., Q.D. and J.X.L. revised the manuscript; All authors were involved in the experiment, critical review of the manuscript. All authors approved the final version.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Liu, J., Min, L., Liu, R. et al. The effect of exercise on cerebral blood flow and executive function among young adults: a double-blinded randomized controlled trial. Sci Rep 13, 8269 (2023). https://doi.org/10.1038/s41598-023-33063-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-33063-9
- Springer Nature Limited