
Abstract
Nonalcoholic fatty liver disease (NAFLD) is one of major causes of end-stage liver disease in the coming decades, but it shows few symptoms until it develops into cirrhosis. We aim to develop classification models with machine learning to screen NAFLD patients among general adults. This study included 14,439 adults who took health examination. We developed classification models to classify subjects with or without NAFLD using decision tree, random forest (RF), extreme gradient boosting (XGBoost) and support vector machine (SVM). The classifier with SVM was showed the best performance with the highest accuracy (0.801), positive predictive value (PPV) (0.795), F1 score (0.795), Kappa score (0.508) and area under the precision-recall curve (AUPRC) (0.712), and the second top of area under receiver operating characteristic curve (AUROC) (0.850). The second-best classifier was RF model, which was showed the highest AUROC (0.852) and the second top of accuracy (0.789), PPV (0.782), F1 score (0.782), Kappa score (0.478) and AUPRC (0.708). In conclusion, the classifier with SVM is the best one to screen NAFLD in general population based on the results from physical examination and blood testing, followed by the classifier with RF. Those classifiers have a potential to screen NAFLD in general population for physician and primary care doctors, which could benefit to NAFLD patients from early diagnosis.
Similar content being viewed by others


Introduction
Nonalcoholic fatty liver disease (NAFLD) is one of the most important causes of liver disease with approximately 25% in the estimated prevalence worldwide, and it will become one of major causes of end-stage liver disease in the coming decades1,2. NAFLD is also the most quickly growing cause of hepatocellular carcinoma in liver transplant in the United States3. However, NAFLD shows few or no symptoms until it develops into cirrhosis4. This process usually takes more than seven years4. Thus, NAFLD patients will benefit from early diagnosis and appropriate management.
Machine learning has been used to develop models to classify subjects with or without NAFLD5,6. However, those previous studies included subjects from the same center in 2010 or 2014. The health status of general people recently should be different from 7 or 12 years ago. Moreover, previous models used a plentiful of clinical features, which included results from physical examination, complete blood count, liver function testing, lipid panel, renal function testing and tumor markers5,6. Those complex features could help enhance the performance of models. However, they also reduce the simplicity and practicability when the model is applied by primary care doctors.
Therefore, in this study, we develop machine learning models to screen NAFLD patients from general population using data from annual health examination in 2021. We respectively adopted decision tree, random forest (RF), extreme gradient boosting (XGBoost) and support vector machine (SVM) algorithm to develop our models. All of those algorithms are classic in machine learning, and have stable performance in medical models7. They also could show important features in the model, which could provide clinical information on NAFLD screening. Moreover, our models included less candidate features than previous ones5,6. That could make more applicable for primary care doctors to screen NAFLD, and keep a good performance at the same time.
Results
Subjects’ characteristics
This study finally enrolled 14,439 subjects, including 4411 in NAFLD group and 10,028 in non-NAFLD group. The subjects in NAFLD group had higher body mass index (BMI) (NAFLD group vs non-NAFLD group = 27.2 ± 3.2 vs 23.5 ± 3.0), higher blood pressure (systolic blood pressure (SP): 132 ± 18 vs 122 ± 18 mmHg; diastolic blood pressure (DP): 78 ± 12 vs 71 ± 11 mmHg), higher red blood cell count (RBC) (5.22 ± 0.55 vs 4.95 ± 0.57 × 109/L), higher white blood cell count (WBC) (7.32 ± 1.78 vs 6.50 ± 1.58 × 109/L), higher monocyte count (MONO) (0.50 ± 0.16 vs 0.43 ± 0.15 × 109/L), higher lymphocyte count (LY) (2.50 ± 0.76 vs 2.20 ± 0.62 × 109/L), higher neutrophil count (NE) (4.10 ± 1.30 vs 3.66 ± 1.19 × 109/L) and higher eosinophil count (EO) (0.19 ± 0.15 vs 0.17 ± 0.16 × 109/L) than those in non-NAFLD group (Table 1).
Moreover, when compared with the subjects in non-NAFLD group, those in NAFLD group had an increased ratio of AST/ALT (0.91 ± 0.55 vs 1.27 ± 0.60), a higher level of alanine aminotransferase (ALT) (33 ± 22 vs 19 ± 15 U/L), aspartate aminotransferase (AST) (25 ± 13 vs 20 ± 13 U/L), γ-Glutamyltransferase (γ-GT) (55 ± 57 vs 31 ± 34 U/L), triglyceride (TG) (2.71 ± 2.70 vs 1.44 ± 1.13 mmol/L), total cholesterol (TC) (5.24 ± 1.02 vs 4.89 ± 0.93 mmol/L), low-density lipoprotein cholesterol (LDL) (3.25 ± 0.79 vs 2.83 ± 0.76 mmol/L) and very low-density lipoprotein cholesterol (VLDL) (1.20 ± 1.20 vs 0.64 ± 0.50 mmol/L), and a lower level of high-density lipoprotein cholesterol) (HDL) (1.18 ± 0.30 vs 1.43 ± 0.34 mmol/L) (Table 1).
Model performance
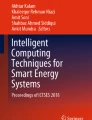
Table 2 and Fig. 1 illustrate the performance of all classifiers. The model based on SVM was showed the best performance with comprehensive evaluation, which included the highest accuracy (0.801), positive predictive value (PPV) (0.795), F1 score (0.795), Kappa score (0.508) and area under the precision-recall curve (AUPRC) (0.712), and the second top of area under receiver operating characteristic curve (AUROC) (0.850). The second-best classifier was that using RF, which was showed the highest AUROC (0.852) and the second top of accuracy (0.789), PPV (0.782), F1 score (0.782) and Kappa score (0.478) and AUPRC (0.708). The performance of XGBoost classifier follows RF (AUROC: 0.833, accuracy: 0.781, PPV: 0.778, F1 score: 0.779, Kappa score: 0.478 and AUPRC: 0.704). The worst performance was showed in the classifier based on decision tree.

Receiver operator characteristic curves and precision-recall curve. (A) Receiver operating characteristic curve. (B) Precision-recall curve. XGBoost extreme gradient boosting. SVM support vector machine. ROC operating characteristic curve. AUC area under curve. AUPRC area under the precision-recall curve.
Important features from models
All of the classifiers in the study could show important features in each model. For the classifier using decision tree, BMI, the level of TG and ALT, and the ratio of AST/ALT were the important features to decide the tree model (Fig. 2). The classifier from XGBoost showed the same features as that from decision tree (Fig. 3). The classifier based on RF also showed those exactly features and VLDL-C. For the classifier from SVM, more important features were showed in the model, including sex, age, BMI, hematocrit (HCT), mean corpuscular hemoglobin (MCH), mean corpuscular volume (MCV), mean platelet volume (MPV), platelet larger cell ratio (P-LCR), thrombocytocrit (PCT), platelet (PLT), hemoglobin (HGB), MONO, monocyte ratio (MONO%), eosinophil ratio (EO%), EO, ALT, AST, globulin (GLO), total protein (TP), LDL, TG, VLDL-C and TC.

Classifier based on Decision tree. BMI body mass index; TG triglyceride; ALT alanine aminotransferase; AST aspartate aminotransferase; ASTALT the ratio of AST/ALT.

Features importance in classifier based on XGBoost. f2: BMI; f42: TG; f29: ALT; f30: ratio of AST/ALT. BMI body mass index; TG triglyceride; ALT alanine aminotransferase; AST aspartate aminotransferase.
Discussions
In this study, we developed classification models using decision tree, RF, XGBoost and SVM to screen subjects with NAFLD from asymptomatic and general adults. All models were assessed by accuracy, PPV, F1 score, AUROC and AUPRC. The best performance was showed in the model based on SVM, followed by RF.
Our results showed that the model with SVM was the best one in performance, followed by RF model. RF model showed good performance in previous study on NAFLD screening5. SVM has been showed good performance in developing medical models, including those for classifying NAFLD patients5,6,8. Thus, our results were in consistent with previous studies5,6.
Moreover, our results showed that RF and XGBoost models performed better than decision tree, particularly the RF model. Since RF and XGBoost models integrated decision trees9,10, those models performed better than single decision tree model. In our study, the RF model was showed a bit better performance than XGBoost model. That may be partly related with our data, which were not absolutely balanced between the two groups (non-NAFLD group vs NAFLD group = 10,028 vs 4411). RF algorithm can balance the error of unbalance data and then get good result9. Even though, the performance of model from XGBoost was quite close to that from RF, and most of the assessed results for performance were within 0.01 between them (Table 2). Moreover, since our models based on the NAFLD prevalence in real world, our models may be more applicable than that from intentionally designed samples in the real world without an absolutely balanced sample.
The performance of our models in accuracy, PPV, AUROC and AUPRC was similar with those reported in previous studies5,6 (Supplementary table 1). When compared with models using the same algorithms in Liu’s work, the PPV in our models with XGBoost and SVM was similar with that in previous study6 (PPV: XGBoost: 0.778 vs 0.806, SVM: 0.792 vs 0.768). For AUROC, it’s was a bit better for XGBoost model in the previous one than ours, whereas it’s similar for SVM model in both studies (XGBoost: 0.833 vs 0.873; SVM: 0.850 vs 0.865). For AUPRC, models with XGBoost and SVM in Liu’s report was a bit better than ours6 (XGBoost: 0.704 vs 0.810; SVM: 0.712 vs 0.800). The accuracy in our models with RF and SVM was slightly lower than the previous one in Ma’s report5 (RF: 0.789 vs 0.827, SVM: 0.798 vs 0.827). In contrast, our models showed a bit higher F1 score than Ma’s report and Liu’s reported5,6 (Compared with Ma’s report: Decision tree: 0.764 vs 0.569; RF: 0.782 vs 0.579; SVM: 0.792 vs 0.557. Compared with Liu’s report: XGBoost: 0.779 vs 0.695; SVM: 0.792 vs 0.713). F1 score is a more appropriate index than accuracy score to assess the accuracy of model using data without absolute balance in both groups. Thus, our models were showed similar performances with previous one.
That previous study6 included features from physical examination, complete blood count, liver function testing, lipid panel, renal function testing and tumor markers. The more features, close to NAFLD or not, may increase the performance of models. However, more features and more complex of model could lead to more difficult in extending and application for primary care doctors. In contrast, the features in our models were simpler, which included results from physical examination, complete blood count, liver function testing and lipid panel (Supplementary table 2). Thus, our models may be more application in primary care practice, and also have a similar performance, when compared with the previous ones.
From our models, the most important features were BMI, the level of TG, VLDL-C, ALT and the ratio of AST/ALT in blood. Our results were in consistent with those in previous studies5,6. BMI and TG are risk factors for NAFLD in adults11,12, which were identified in all of our models. That may be related with an aberrant regulation of hepatic TG accumulation via de novo lipogenesis in NAFLD13. Moreover, the liver secretes TG in the form of VLDL for delivery to peripheral tissues. VLDL-C overproduction is one of characteristics of NAFLD13. That reflects an increased de novo lipogenesis plus lipolysis of intrahepatic and intra-abdominal fat in NAFLD14. In addition, in Chinese individuals without obesity, an increased ratio of ALT/AST is associated with the risk of new-onset NAFLD15. The decreased ratio of AST/ALT in NAFLD in our study was in consistent the previous finding15. That may be due to many reasons, for instance, a decreased AST/ALT ratio is related with chronic inflammation in liver, insulin resistance or steatosis of the liver, which leads to NAFLD16,17. Therefore, models in our study identified the importance of BMI, TG, VLDL-C, ALT and ratio of AST/ALT in NAFLD. And we further suggested those features should be important in screening NAFLD in general and asymptomatic adults.
We acknowledged that in our study, the diagnosis of NAFLD was based on abdominal ultrasound examination, instead of liver biopsy. That’s because liver biopsy was not permitted to screen NAFLD among general and health population according to ethic principles and the declaration of Helsinki. Abdominal ultrasound has been widely accepted to serve as an accurate and non-invasive tool in diagnosing NAFLD18. In our study, the prevalence of NAFLD was 30.5% (4411/14,439). That is similar with the national prevalence 29.2% in China, which was based on the database from 2008 to 2018 and has been increased over years19. Thus, the diagnosis of NAFLD from abdominal ultrasound could be accurate and reliable in our study. Moreover, type 2 diabetes mellitus (T2D) history wasn’t included into the candidate features. That’s because we can’t diagnose T2D from our subjects based on our data, and personal-reported history can’t be excluded bias. Since T2D is a risk factor of NAFLD11,12, the performance of our models should be improved if T2D was included as candidate feature.
In conclusion, the classification models could be developed using machine learning based on the data of annual health examination, which could screen NAFLD in general adults without redundant examination. The model using SVM is the best one, followed by that using RF. Those models may provide a readily available tool for physician and primary care doctors to screen NAFLD in general population, which could benefit to NAFLD patients from early diagnosis.
Methods
Study population
The subjects (age ≥ 18 years) were recruited into our study from general people who attended an annual health examination in Guilin People’s Hospital, from January to December in 2021. All laboratory testing and quality control were carried out by the laboratory analysis center of the hospital. The study protocol was approved by the Research Ethics Committee of Guilin People’s Hospital, and confirmed to the declaration of Helsinki. Written informed consent was obtained from each subject. NAFLD was diagnosed by exporters with at least 5 years’ experience, when there was evidence of hepatic steatosis by color Doppler ultrasound with a 3.5-MHZ probe (GE LOGIQ, Suzhou, China)20.
The subjects were excluded when they were: (1) had alcohol consumption > 210 g/week for men and 140 g/week for women; (2) had a history and/or laboratory evidences of viral hepatitis, autoimmune hepatitis, drug-induced liver disease or other chronic liver diseases, and secondary fatty liver; (3) in an acute or chronic infections; (4) in pregnancy or lactation; (5) had psychiatric disorders; or (6) had malignant tumor.
Candidate features to classify subjects
The candidate features were collected from the electronic medical record, including age, sex, BMI (BMI = weight/height2), systolic blood pressure (SP), diastolic blood pressure (DP) and blood testing.
The blood testing was as following:(1) complete blood count: WBC, RBC, HGB, HCT, MCV, MCH, mean corpuscular hemoglobin concentration (MCHC), PLT, standard deviation in red cell distribution width (RDW-SD), coefficient variation of red cell volume distribution width (RDW-CV), platelet distribution width (PDW), MPV, P-LCR, PCT, NE, LY, MONO, EO, basophil count (BA), neutrophil ratio (NE%), lymphocyte ratio (LY%), MONO%, EO%, basophil ratio (BA%); (2) liver function: total bilirubin (TBIL), direct bilirubin (DBIL), indirect bilirubin (IDBIL), ALT, AST, ratio of AST/ALT, γ-GT, alkaline phosphatase (ALP), TP, albumin (ALB), GLO, ratio of ALB/GLO; (3) lipid panel: TG, TC, HDL, LDL, VLDL.
Machine learning classifiers
The subjects were randomly divided into training set and testing set at a ratio of 7:3. The training set was used to develop the model, whereas the testing set was served to test the model. The data in training set were standardized using z-score transformation, and the data in testing set were transformed using the same parameters as those from the training data.
The models were developed based on training set by using Python3.7.6 programming language (http://www.python.org), scikit-learn22.2 library (https://scikit-learn.org/stable/). The models to classify subjects with or without NAFLD using decision tree, RF, XGBoost and SVM. SVM is an effective approach for classification by using linear functions or special nonlinear functions to transform the input space into a multidimensional space21. RF and XGBoost models respectively integrated decision trees based on a bagging combination of multiple tree models or a gradient increase framework10,11.
The hyper parameters with training set were estimated using grid-search and tenfold cross-validation. The best parameter combination in the model was selected when it led to the highest efficiency of the model. The gini criterion was selected with grid-search in the decision tree, which means CART tree was developed in our study. The performance of classifiers was tested on the testing set. The performance of models was assessed using accuracy, PPV, F1 score, AUROC, Kappa score and AUPRC.
Statistical analysis
The Student’s t test or Mann–Whitney U test was used for comparing continuous data, and the Chi-square test was used for categorical variables. P-values < 0.05 were considered statistically significant. The statistical analyses were performed using SAS 9.4 (SAS Institute Inc., Cary, NC, USA).
Data availability
The dataset generated and/or analyzed during the current study are not publicly available but are available from the corresponding author and the first author on reasonable request. The code was based on Python3.7.6 programming language (http://www.python.org), scikit-learn22.2 library (https://scikit-learn.org/stable/). The codes are available from the corresponding author on reasonable request.
References
Younossi, Z. et al. Global burden of NAFLD and NASH: Trends, predictions, risk factors and prevention. Nat. Rev. Gastroenterol. Hepatol. 15, 11–20 (2018).
Younossi, Z. M. et al. Global epidemiology of nonalcoholic fatty liver disease-meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 64, 73–84 (2016).
Younossi, Z. et al. Nonalcoholic steatohepatitis is the fastest growing cause of hepatocellular carcinoma in liver transplant candidates. Clin. Gastroenterol. Hepatol. 17, 748-755.e3 (2019).
Singh, S., Allen, A. M., Wang, Z., Prokop, L. J., Murad, M. H. & Loomba, R. Fibrosis progression in nonalcoholic fatty liver vs nonalcoholic steatohepatitis: a systematic review and meta-analysis of paired-biopsy studies. Clin. Gastroenterol. Hepatol. 13, 643–54.e1–9; quiz e39–40 (2015).
Ma, H., Xu, C. F., Shen, Z., Yu, C. H. & Li, Y. M. Application of machine learning techniques for clinical predictive modeling: A cross-sectional study on nonalcoholic fatty liver disease in China. Biomed Res Int. 2018, 4304376 (2018).
Liu, Y. X. et al. Comparison and development of advanced machine learning tools to predict nonalcoholic fatty liver disease: An extended study. Hepatobiliary Pancreat Dis. Int. 20, 409–415 (2021).
Rajkomar, A., Dean, J. & Kohane, I. Machine learning in medicine. N. Engl. J. Med. 380, 1347–1358 (2019).
Cornforth, D. M. et al. Pseudomonas aeruginosa transcriptome during human infection. Proc. Natl. Acad. Sci. USA. 115, E5125–E5134 (2018).
Breiman, L. Random forests. Mach. Learn. 45, 5–32 (2001).
Friedman, J. H. Greedy function approximation: A gradient boosting machine. Ann. Stat. 29, 1189–1232 (2001).
Non-Alcoholic Fatty Liver Disease: Assessment and Management. NICE Guideline, No. 49. National Guideline Centre (UK). London: National Institute for Health and Care Excellence (NICE) (2016).
Younossi, Z. M. Non-alcoholic fatty liver disease—A global public health perspective. J Hepatol. 70, 531–544 (2019).
Kawano, Y. & Cohen, D. E. Mechanisms of hepatic triglyceride accumulation in non-alcoholic fatty liver disease. J. Gastroenterol. 48, 434–441 (2013).
Fabbrini, E. et al. Alterations in adipose tissue and hepatic lipid kinetics in obese men and women with nonalcoholic fatty liver disease. Gastroenterology 134(2), 424–431 (2008).
Zou, Y., Zhong, L., Hu, C. & Sheng, G. Association between the alanine aminotransferase/aspartate aminotransferase ratio and new-onset non-alcoholic fatty liver disease in a nonobese Chinese population: A population-based longitudinal study. Lipids Health Dis. 19, 245 (2020).
Kwon, S. S. & Lee, S. G. A high alanine aminotransferase/aspartate aminotransferase ratio determines insulin resistance and metabolically healthy/unhealthy obesity in a general adult population in Korea: The Korean National Health and Nutritional Examination Survey 2007–2010. Exp. Clin. Endocrinol. Diabetes 127(10), 677–684 (2019).
Rinella, M. E. Nonalcoholic fatty liver disease: A systematic review. JAMA 313(22), 2263–2273 (2015).
Khov, N., Sharma, A. & Riley, T. R. Bedside ultrasound in the diagnosis of nonalcoholic fatty liver disease. World J. Gastroenterol. 20, 6821–6825 (2014).
Zhou, F. et al. Unexpected rapid increase in the burden of NAFLD in China From 2008 to 2018: A systematic review and meta-analysis. Hepatology 70, 1119–1133 (2019).
Fan, J. G., Wei, L., Zhuang, H. & National Workshop on Fatty Liver and Alcoholic Liver Disease, Chinese Society of Hepatology, Chinese Medical Association, et al. Guidelines of prevention and treatment of nonalcoholic fatty liver disease (2018, China). J. Dig. Dis. 20(4), 163–173 (2019).
Yu, W., Liu, T., Valdez, R., Gwinn, M. & Khoury, M. J. Application of support vector machine modeling for prediction of common diseases: The case of diabetes and pre-diabetes. BMC Med. Inform DecisMak. 10, 16 (2010).
Acknowledgements
This work was supported by the Guilin scientific research and technology development project (2020011207-6).
Author information
Authors and Affiliations
Contributions
S.Q. and S.C. designed the study. S.Q., X.H., Y.W., C.W., X.T., H.T., Q.A. and J.L. contributed to data collection. S.C. and S.Q. developed the models and wrote the manuscript. All authors contributed to the revision and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Qin, S., Hou, X., Wen, Y. et al. Machine learning classifiers for screening nonalcoholic fatty liver disease in general adults. Sci Rep 13, 3638 (2023). https://doi.org/10.1038/s41598-023-30750-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-30750-5
- Springer Nature Limited