
Abstract
The aim of this study was to compare the trueness of complete- and partial-arch impressions obtained using conventional impression materials and intraoral scanners in vivo. Full-arch impressions were taken using polyether and polyvinylsiloxane. Gypsum casts were digitized using a laboratory scanner (IM, AF). Casts obtained from polyether impressions were also scanned using an industrial blue light scanner to construct 3D reference models. Intraoral scanning was performed using CEREC Omnicam (CO) and Trios 3 (TR). Surface matching software (Atos Professional) enabled to determine the mean deviations (mean distances) from the reference casts. Statistically significant discrepancies were calculated using the Wilcoxon signed-rank test. The mean distance for trueness ranged from 0.005 mm (TR) to 0.023 mm (IM) for the full arch, from 0.001 mm (CO) to 0.068 mm (IM) for the anterior segment, and from 0.019 mm (AF) to 0.042 mm (IM) for the posterior segment. Comparing the anterior vs. the posterior segment, significantly less deviations were observed for anterior with CO (p < 0.001) and TR (p < 0.001). Full-arch comparisons revealed significant differences between AF vs. IM (p = 0.014), IM vs. CO (p = 0.002), and IM vs. TR (p = 0.001). Full-arch trueness was comparable when using Affinis and the two intraoral scanners CEREC Omnicam and Trios 3. The digital impression devices yielded higher local deviations within the complete arch. Digital impressions of the complete arch are a suitable and reliable alternative to conventional impressions. However, they should be used with caution in the posterior region.
Trial registration: Registration number at the German Clinical Trial Register (04.02.2022): DRKS00027988 (https://trialsearch.who.int/).
Similar content being viewed by others

Introduction
There exist several available intraoral scanning systems that use advanced technology. The scanning of an impression or gypsum model is being progressively replaced by direct powder-free intraoral three-dimensional data collection1,2,3,4. The adoption of such techniques over conventional impression methods is mainly due to the reduced overall treatment time, ease of use, higher inter-operator reproducibility, and the ability to perform a quick repeat if imprecise scanned areas are noticed2,5,6,7,8,9,10,11,12. When fixed dental prostheses are fully digitally fabricated using computer-aided design and computer-aided manufacturing (CAD-CAM), without any gypsum cast, they often provide a better marginal and internal fit13,14.
The digital workflow is already routinely used in dental surgery, especially in implantology, and is increasingly utilized for the design and production of dental splints, and fixed dental protheses. Digital workflow use is now well-established for single crowns and fixed partial dentures with up to six units6,11,13,15,16,17,18,19,20. There are numerous indirect approaches for comparing the conventional and digital workflows, including the examination of restoration fit after each working technique13,14,16,21,22. Best-fit alignment is the most common direct method for accuracy evaluations of different impressions7,12,23,24.
In general, the scanned field can include individual teeth up to segments, quadrants, or even the full arch. Based on the present knowledge, the scanning of small divisions yields digital impressions with clinically satisfactory accuracy. However, the scanning of larger fields presents a challenge, especially if they are of similar quality. Therefore, the use of digital methods must be improved for removable dentures, such as total dentures25,26.
Regarding the complete arch, researchers have mainly focused on in vitro studies, in which they use a typodont or other individual model as a reference model and record the mean deviation therefrom12,24,27,28,29,30. Current studies indicate that digital imaging of the complete jaw is still a challenge12,31,32,33. There is a scarcity of investigations involving in vivo full-arch comparisons, and thus there remains a high demand for clinical studies of this matter12,28,34,35,36.
The aim of the present study was to respond to this request by comparing the trueness of complete-arch impressions obtained using two conventional impression materials and two intraoral scanners in vivo. It should be clarified whether intraoral scanning devices can replace full-arch conventional impressions under clinical conditions. The null hypothesis was that there are no statistically significant differences in trueness between the conventional and digital impression techniques.
Materials and methods
Participants and inclusion criteria
For this study, 31 adult participants (23 females, 7 males; mean age: 24 years, range: 22–32 years) with complete natural dentition (at least from the second molar to the contralateral second molar), good oral hygiene, and no ongoing dental or orthodontic treatments were recruited. Exclusion criteria were teeth damaged by caries or periodontal disease, present dental prosthesis, severe crowding, dentofacial deformity, or any intolerance or allergy to the utilized materials. All participants had to give their written consent. The experimental procedures were approved by the Medical Ethics Committee of Friedrich-Alexander University Erlangen-Nuremberg (approval number: 416_18B), and the study was registered in the German Register for Clinical Studies (reference number: DRKS00027988).
Conventional and digital impressions
For all participants, full-arch conventional impressions of the upper jaw were taken both with a polyether impression material (Impregum Penta Soft; 3M ESPE, Neuss, Germany) as a monophasic impression, and with an addition curing silicone material (Affinis heavy/regular body; Coltène Whaledent, Langenau, Germany). Since the two-step impression was described to be more accurate compared to the one-step technique the two-step two-viscosity technique was used37,38. Thus, to obtain the silicone impressions, the tray was first filled with the heavy body, using a pentamix device. After removal from the mouth, the cured heavy body was prepared to be corrected by cutting it out and using a carving knife to create uniform ventilation channels on each tooth of the subject for an even layer thickness of the regular body. Then a second impression was taken with the regular body above the heavy body. To prevent dental movements, the conventional impressions were taken on two different days. To ensure a consistent impression technique and seating pressure, all impressions were taken by only one operator who had years of experience, and ventilation channels were created as already mentioned. Consistent ambient humidity and room temperature were maintained while taking conventional impressions, and all manufacturers’ instructions were followed. Materials were cleaned with an immersion disinfection (Eurosept Plus Impression Disinfection Liquid; Henry Schein, Langen, Germany) and subsequent rinced with water. The conventional impressions with Impregum Penta Soft and Affinis were air-dried and poured after 24 h with type IV dental stone (Fujirock EP-Classic; GC Corporation, Bad Homburg, Germany). To obtain a highly accurate reference model for each participant, the gypsum casts of the polyether impressions were digitized using a high-resolution industrial 3D-scanner (Atos Professional; GOM, ZEISS company, Braunschweig, Germany) and standard tessellation language (STL) files were created. This three-layer scanning technology has an average measurement error of 3 μm39. All gypsum casts (Polyether and Affinis) were additionally digitized (IM, AF) using an extraoral laboratory scanner (D900; 3shape, Düsseldorf, Germany) to generate STL-files for analyses. Thus, the casts of the Impregum impressions were scanned twice to detect the reliability and possible error sources of the employed laboratory scanner.
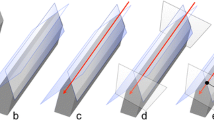
Direct digital full-arch models were obtained using two powder-free intraoral scanners: CEREC Omnicam v. 5.0.2 (Dentsply Sirona; Bensheim, Germany) and Trios 3 v. 1.6.10.1 (3shape; Düsseldorf, Germany). The manufacturers’ scanning strategies were also followed, which can be found in the user manuals of each system. The operator had previous training with the utilized scanners. For the comparisons, the data from the digital models were converted into standard tessellation language files (STL) (Fig. 1).

Flowchart illustrating the experimental design of the study based on an example of a test person. In the first step, the digital (1a) TRIOS 3 [TR1], (b) Cerec Omnicam [CO2]) and conventional, (1c) Impregum [IM3], (d) Affinis [AF4]) impressions were taken. Then, the reference gypsum cast of the IM-impression was provided with reference points and scanned with ATOS (GOM, ZEISS company) (2). Subsequently, the STL files of the different impression techniques were virtually superimposed on the STL reference model (3) so that the deviations were represented in the form of color-coded distance maps (4).
Analysis
All data were stored in STL files for analyses. For three-dimensional difference analysis, surface matching software (Atos Professional; GOM, ZEISS company, Braunschweig, Germany) was used to superimpose the scans according to the best-fit-alignment method. The mean deviation values (mean distance in mm) were obtained by superimposing the respective model for each participant with the associated reference model. This method allows determination of the trueness of different impression methods.
First, the reference model was imported as an STL file, and subsequently trimmed to the tooth shape. The file for comparison was also imported as an STL file. Then, a rough, manual 3-point alignment of the two relevant models had to be implemented via prominent points on the tooth surfaces of the canines and molars for all study participants. Subsequently, the precise adjustment in form of a best-fit alignment could be performed by manual selection of the entire tooth surfaces, enabling the surface matching software to superimpose the models for variance analyses. Surface discrepancies between the two images were represented using color-mapping methods, and numbers. The color maps show a tolerance range of ± 10 µm (green) and a specified range of ± 100 µm (20 color segments). The analysis included all tooth surfaces. The complete arch was considered for evaluation, and a division into anterior and posterior segments was also realised. The total arch included teeth 17 to 27, the anterior segment teeth 13 to 23, and the posterior segment teeth 14 to 17, and 24 to 27. Thereby, the two segments were not scanned separately but were selected from the full-arch dataset of the digitized reference casts.
A statistician performed the evaluation. The level of significance was set at α = 0.05. Statistically significant discrepancies were calculated using the Wilcoxon signed-rank test. Statistical analysis was performed using the statistical software R V3.6.3, R Core Team 2020.
Ethical approval and informed consent
The experimental procedures were approved by the Medical Ethics Committee of Friedrich-Alexander University Erlangen-Nuremberg (approval number: 416_18B). Before starting the data acquisition, all participants signed an informed consent. Before starting the data acquisition, all participants signed an informed consent. All persons gave their informed consent prior to their inclusion in the study. Details that might disclose the identity of the subjects under study were omitted. All methods were carried out in accordance with relevant guidelines and regulations in the declaration section.
Results
The mean distance values (± standard deviation) for the complete arch ranged from 0.005 mm (± 0.025 mm) for Trios 3 (TR) to 0.023 mm (± 0.010 mm) for lab scans of the gypsum casts obtained using Impregum (IM). The mean values for the anterior segment ranged from 0.001 mm (± 0.016 mm) for CEREC Omnicam (CO) to 0.068 mm (± 0.146 mm) for IM, and those for the posterior segment ranged from 0.019 mm (± 0.036 mm) for lab scans of the gypsum casts obtained using Affinis (AF) to 0.042 mm (± 0.076 mm) for IM (Table 1). The mean distances from the reference models were generally similar between the conventional impression method using the silicone material AF and the two intraoral digital scanners. The impressions made using the polyether material IM exhibited the highest discrepancies for all compared areas (Table 1; Fig. 2, 3).

Mean distance for complete-arch (n = 31) and significant p-values.

Mean distance for the anterior and posterior segment of dental arch (n = 31) and significant p-values.
Full-arch comparisons between all impression methods (AF vs. IM, AF vs. CO, AF vs. TR, IM vs. CO, IM vs. TR, and CO vs. TR) revealed significant differences between AF vs. IM (p = 0.014), IM vs. CO (p = 0.002), and IM vs. TR (p = 0.001) (Fig. 2). Specifically, the lab scans of gypsum casts obtained using the polyether impression material (IM) were significantly less precise compared to the silicone impression material (AF) or to both utilized intraoral scanners (CO and TR).
Comparative analysis between the anterior and posterior segment of the dental arch within the same impression group revealed significantly higher values for the posterior segment when using the intraoral digital scanner Omnicam (p < 0.001) or Trios 3 (p < 0.001) (Figs. 3, 4). Thus, with both scanners, the scans of the anterior segment showed significantly less deviations compared to the scans of the posterior segment. The conventional impressions were continuously accurate, with no significant differences between the anterior and posterior areas (p > 0.05).

Color coded, 3D superimposition showing deviations of the Trios 3 scan to the reference cast between the anterior and posterior segments based on the example of one proband.
Discussion
In the present study, the trueness of conventional and digital impression methods for the complete arch was evaluated in vivo. In 31 participants, impressions of the upper jaw were taken with two routinely used conventional impression materials—a polyether and a vinylpolysiloxane material—and two intraoral scanners.
The two most routinely materials for high precision impressions were used for conventional impressions40,41,42,43. Polyether even gave more accurate impressions than polyvinylsiloxane. It is assumed that this is due to the hydrophilic nature of polyether and its use in the moist intraoral environment44,45,46. Assuming that polyether is the most accurate conventional impression material, Impregum Penta Soft was selected for obtaining the reference models. Clinical experience, and previous investigations by other authors, indicate that polyether is a highly accurate material46,47,48. Comparison studies have usually used the gypsum cast of a conventional impression as the reference model12,29,36. Similar to the study design of Ender et al., the anterior and posterior segments were considered separately for analysis after being digitally cut out of the complete arch12. The intention was to test in vivo whether there are differences in the detection of the dental arch between the anterior and posterior areas due to certain influencing factors. The posterior area was previously described as most prone to deviation in the case of intraoral scanning49,50,51,52. The method of best-fit alignment was used, as this is the most common direct concept for accuracy evaluations12,23,24.
The present results disproved the null hypothesis that there were no statistically significant differences between the conventional and the digital impression techniques for full-arch and partial-arch comparisons.
The accuracy of the impression indisputably determines the fit of the produced prosthetics. There is still no clear evidence how much discrepancy of a dental prosthesis is clinically acceptable. However, many authors propose a clinically acceptable marginal gap of up to 120 µm (incl. 25–50 µm for a cement layer)53,54,55. In the present study highly satisfactory mean distance values from 1 µm to 68 µm were obtained (full arch: 5 µm with TR to 23 µm with IM, anterior segment: 1 µm with CO to 68 µm with IM, and posterior segment: 19 µm with AF to 42 µm with IM)12,29. The in vitro investigation of Ender et al. showed similar mean deviation values of 16 µm to 93 µm for the complete arch (polyvinylsiloxane vs. Cerec Omnicam v. 4.6.1), 14 µm to 69 µm for the anterior part, and 10 µm to 47 µm for the posterior part (both polyvinylsiloxane vs. Medit i500 v. 1.2.1). They also compared the maxilla, in which they applied various intraoral scanners, and one conventional impression material. The impression with polyvinylsiloxane showed a significant better match with the custom complete-arch reference cast12. In contrast, in the present study, the values obtained with AF were generally very similar to those obtained with the digital scanners. Other investigations have reported similar results for conventional impression material and digital devices30,56. Especially regarding the complete arch, authors have mainly focused on in vitro studies using representative dental models. Ender et al. concluded that digital impressions could compete with conventional impressions in cases of partial arch capturing12,30. However, they and other authors have reported that conventional impression methods still showed higher accuracy when capturing the complete arch12,27,29,57,58. This may be largely because digital intraoral scanners only record sections of the dental arch and then match them to a whole image. The software identifies overlapping areas and superimposes them electronically, which may result in inaccuracies12,28,59. Nevertheless, some authors have reported that certain devices can keep up with conventional methods for the full arch30,34,35,60.
Concerning the fabrication of dental prosthesis, many authors have described intraoral scanning devices as being more precise than conventional impressions when producing single crowns or short-span restorations6,16,18,21,22,23,36,58,61. However, limited data are available regarding the survival of these restorations. Therefore, a meta-analysis concluded that these results should be interpreted with caution62. On the other hand, conventional methods are reported to be more precise when producing large or full-arch restorations58. To date, there is no general agreement on which impression method is most suitable.
The significance analysis revealed that the laboratory scans of gypsum casts made with Impregum (IM) significantly differed from the dental models obtained from impressions made with Affinis (AF) or from the two digital intraoral scanners, CEREC Omnicam (CO) and Trios 3 (TR). Specifically, IM showed significantly less trueness in full-arch comparisons when superimposed with the corresponding digitized reference casts. Better values for IM were expected, since prior studies showed similar accuracy from a polyether and a silicone impression material63. However, it can be assumed that the method used to make the reference casts was reliable as the polyether impressions were poured and directly scanned using the high-resolution industrial 3D-scanner Atos Professional. These casts, together with the gypsum casts of the silicone impressions, were digitized using an extraoral laboratory scanner. This could lead to errors, since the casts obtained using the impressions with polyether were transported and scanned twice. It appears that the indirect digitization of stone casts is fraught with errors and may provide inaccurate results14,23,34,64. Moreover, by scanning the polyether plaster model with both the high-resolution reference scanner and the extraoral laboratory scanner, the measurement accuracy of the latter scanner should be checked. The superimposition of the two digital models obtained should show maximum match for superimposition. Regarding Fig. 3 statistical outliers in case of IM can be seen at once. Thus, this is due to a measurement inaccuracy of the lab scanner.
The two utilized intraoral scanners showed significant differences when comparing the anterior segment versus posterior segment within the full arch of the same impression group. Superimposition of the anterior segments of the digital intraoral scans with the same fields of the relevant reference models indicated significantly higher trueness compared to the posterior segments. This can be explained by the more difficult conditions for scanning in the posterior area of the jaw, due to the limited oral space for the scan head and the higher condensation from breath or saliva. This finding is in accordance with the observations of Zhang et al., Ender et al., and Patzelt et al., who all found that higher local deviations within the full arch are possible when using a digital intraoral scanner35,36,57,65.
Only few clinical studies have compared digital versus conventional impressions of the complete arch. A thorough search revealed only four such studies. Zhang et al. had the largest number of participants (n = 20), and performed the only study approaching the number of participants in the present study36. Zhang et al. and Sfondrini et al. only used the conventional impression material Alginate for comparisons, and each only used one digital intraoral scanner36,64. Zhang et al. found no significant differences between the gypsum casts and the digital models generated by the scanner iTero, and concluded that digital impression methods are clinically acceptable, and could replace dental stones36. Sfondrini et al. examined 14 participants and determined that the gyspsum casts were not significantly different from the scans using Trios 3. Their conclusions emphasized that intraoral scanning seems to be more time efficient and more comfortable for orthodontic applications, and is on track to replace conventional methods64. However, it must be noted that both of these studies used Alginate, which is not a highly precise conventional material36,64. Moreover, the poured gypsum casts were not scanned using a high-precision industrial scanner to obtain the reference models, but rather were scanned using the same scanner that was employed for the intraoral scans64. Ender et al. applied various conventional materials, including polyether, vinylsiloxanether, and Alginate, and employed seven digital scanners on a total of five participants. They found higher precision when using conventional impressions, except for the alginate group. In contrast to the two previously mentioned studies, they found that the scans were more accurate than the alginate impressions57. This result was more likely to be expected. Keul and Guth examined the upper jaw of only one participant, using an addition curing silicone as a conventional impression material, and using iTero Element for intraoral scans. A unique aspect of their study was the implementation of an in vivo and an in vitro comparison. For the in vitro part, the silicone impression of the patient was casted with a model resin. Their results from both parts of the study indicated that iTero yielded the same or even higher accuracy for single parameters34. Other clinical investigations have focused on single teeth up to segments of the dental arch7,56,66.
The limitations of the present study were that no repetitions were conducted. This was due to the in vivo nature of this study, the relatively large number of participants and their compliance, and the associated exposure time. Similarly, impressions are not repeated in the clinical routine if all therapeutically relevant structures have been represented. Thus, in line with the everyday practice, only trueness and not precision was investigated. Some authors have likewise used only one component to describe accuracy49,67,68,69,70. Moreover, to enable an in vivo comparison, an impression method had to be selected for processing the reference models. This was previously established56. Therefore, no standardized independent model could be applied, as could be done in an in vitro study. Additionally, the anterior and posterior segments were not scanned separately but were rather generated from the data of the complete-arch scan, as was previously described in another study12.
Conclusion
Within the limitations of this in vivo study, scanning the complete dental arch with the tested digital impression systems yielded clinically acceptable results, and represents a suitable and reliable alternative to conventional impressions. The trueness was similar between Affinis and the two intraoral scanners, CEREC Omnicam and Trios 3. Digital impression devices can show higher local deviations within the complete arch. More precise results were obtained for the anterior segment compared to the posterior area. Depending on the clinical problem, the conventional impression can be replaced by the digital impression. Taking into consideration that digital devices should be used with caution in the posterior region.
These results should be verified in additional clinical studies, which should preferably include both jaws and more digital intraoral scanners.
Data availability
The datasets generated and/or analysed during the current study are not publicly available due part of this data from the study will also be used in the upcoming dissertation by Maria Paulig, and it includes patient data but are available from the corresponding author on reasonable request.
References
van Noort, R. The future of dental devices is digital. Dent. Mater. 28(1), 3–12 (2012).
Birnbaum, N. S. & Aaronson, H. B. Dental impressions using 3D digital scanners: Virtual becomes reality. Compend. Contin. Educ. Dent. 29(8), 494, 496, 498–505 (2008).
Beuer, F., Schweiger, J. & Edelhoff, D. Digital dentistry: An overview of recent developments for CAD/CAM generated restorations. Br. Dent. J. 204(9), 505–511 (2008).
Hategan, S. I. et al. Powder and powder-free intra-oral scanners: Digital impression accuracy. Prim. Dent. J. 7(2), 40–43 (2018).
Yuzbasioglu, E. et al. Comparison of digital and conventional impression techniques: Evaluation of patients’ perception, treatment comfort, effectiveness and clinical outcomes. BMC Oral Health 14, 10 (2014).
Gjelvold, B. et al. Intraoral digital impression technique compared to conventional impression technique. A randomized clinical trial. J. Prosthodont. 25(4), 282–287 (2016).
Kamimura, E. et al. In vivo evaluation of inter-operator reproducibility of digital dental and conventional impression techniques. PLoS ONE 12(6), e0179188 (2017).
Yilmaz, H. & Aydin, M. N. Digital versus conventional impression method in children: Comfort, preference and time. Int. J. Paediatr. Dent. 29(6), 728–735 (2019).
Gallardo, Y. R. et al. Patient outcomes and procedure working time for digital versus conventional impressions: A systematic review. J. Prosthet. Dent. 119(2), 214–219 (2018).
Skramstad, M. J. Welcome to Cerec Primescan AC. Int. J. Comput. Dent. 22(1), 69–78 (2019).
Kurbad, A. Inhouse workflow for single-stage, indirect restorations. Int. J. Comput. Dent. 22(1), 99–112 (2019).
Ender, A., Zimmermann, M. & Mehl, A. Accuracy of complete- and partial-arch impressions of actual intraoral scanning systems in vitro. Int. J. Comput. Dent. 22(1), 11–19 (2019).
Ng, J., Ruse, D. & Wyatt, C. A comparison of the marginal fit of crowns fabricated with digital and conventional methods. J. Prosthet. Dent. 112(3), 555–560 (2014).
Chochlidakis, K. M. et al. Digital versus conventional impressions for fixed prosthodontics: A systematic review and meta-analysis. J. Prosthet. Dent. 116(2), 184-190.e12 (2016).
Moustapha, G. et al. Marginal and internal fit of CAD/CAM fiber post and cores. Int. J. Comput. Dent. 22(1), 45–53 (2019).
Berrendero, S. et al. Influence of conventional and digital intraoral impressions on the fit of CAD/CAM-fabricated all-ceramic crowns. Clin. Oral Investig. 20(9), 2403–2410 (2016).
Cetik, S. et al. Adaptation of zirconia crowns created by conventional versus optical impression: In vitro study. J. Adv. Prosthodont. 9(3), 208–216 (2017).
Su, T. S. & Sun, J. Comparison of marginal and internal fit of 3-unit ceramic fixed dental prostheses made with either a conventional or digital impression. J. Prosthet. Dent. 116(3), 362–367 (2016).
Güth, J. et al. 3D-Druck in der Zahnheilkunde-zwischen Hype und Produktivitätssteigerung. Bayerisches Zahnärzte Blatt BZB 55, 46–55 (2018).
Wang, S. M. et al. Preliminary clinical application of complete digital workflow of design and manufacturing occlusal splint for sleep bruxism. Beijing Da Xue Xue Bao Yi Xue Ban 51(1), 105–110 (2019).
Abdel-Azim, T. et al. Comparison of the marginal fit of lithium disilicate crowns fabricated with CAD/CAM technology by using conventional impressions and two intraoral digital scanners. J. Prosthet. Dent. 114(4), 554–559 (2015).
Seelbach, P., Brueckel, C. & Wostmann, B. Accuracy of digital and conventional impression techniques and workflow. Clin. Oral Investig. 17(7), 1759–1764 (2013).
Tomita, Y. et al. Accuracy of digital models generated by conventional impression/plaster-model methods and intraoral scanning. Dent. Mater. J. 37(4), 628–633 (2018).
Ender, A. & Mehl, A. Accuracy of complete-arch dental impressions: A new method of measuring trueness and precision. J. Prosthet. Dent. 109(2), 121–128 (2013).
Iturrate, M., Eguiraun, H. & Solaberrieta, E. Accuracy of digital impressions for implant-supported complete-arch prosthesis, using an auxiliary geometry part—An in vitro study. Clin. Oral Implants Res. 30(12), 1250–1258 (2019).
Bonnet, G. et al. A new digital denture procedure: A first practitioners appraisal. BMC Oral Health 17(1), 155 (2017).
Cho, S. H. et al. Comparison of accuracy and reproducibility of casts made by digital and conventional methods. J. Prosthet. Dent. 113(4), 310–315 (2015).
Ender, A. & Mehl, A. In-vitro evaluation of the accuracy of conventional and digital methods of obtaining full-arch dental impressions. Quintessence Int. 46(1), 9–17 (2015).
Malik, J. et al. Comparison of accuracy between a conventional and two digital intraoral impression techniques. Int. J. Prosthodont. 31(2), 107–113 (2018).
Ender, A. & Mehl, A. Full arch scans: Conventional versus digital impressions—An in-vitro study. Int. J. Comput. Dent. 14(1), 11–21 (2011).
Abduo, J. & Elseyoufi, M. Accuracy of intraoral scanners: A systematic review of influencing factors. Eur. J. Prosthodont. Restor. Dent. 26(3), 101–121 (2018).
Osnes, C. et al. Sources of error in maximum intercuspation from complete dentate full-arch intraoral scans in vitro. Int. J. Comput. Dent. 24(3), 283–291 (2021).
Waldecker, M. et al. In vitro accuracy of digital and conventional impressions in the partially edentulous maxilla. Clin. Oral. Investig. 26(11), 6491–6502 (2022).
Keul, C. & Guth, J. F. Accuracy of full-arch digital impressions: An in vitro and in vivo comparison. Clin. Oral Investig. 24(2), 735–745 (2020).
Patzelt, S. B. et al. Accuracy of full-arch scans using intraoral scanners. Clin. Oral Investig. 18(6), 1687–1694 (2014).
Zhang, F., Suh, K. J. & Lee, K. M. Validity of intraoral scans compared with plaster models: An in-vivo comparison of dental measurements and 3D surface analysis. PLoS ONE 11(6), e0157713 (2016).
Caputi, S. & Varvara, G. Dimensional accuracy of resultant casts made by a monophase, one-step and two-step, and a novel two-step putty/light-body impression technique: An in vitro study. J. Prosthet. Dent. 99(4), 274–281 (2008).
Levartovsky, S. et al. The effect of one-step vs two-step impression techniques on long-term accuracy and dimensional stability when the finish line is within the gingival sulcular area. J. Prosthodont. 23(2), 124–133 (2014).
Holst, S. et al. A new triple-scan protocol for 3D fit assessment of dental restorations. Quintessence Int. 42(8), 651–657 (2011).
Theocharidou, A. et al. Evaluation of elastomeric impression materials’ hydrophilicity: An in vitro study. Acta Stomatol. Croat. 55(3), 256–263 (2021).
Naidu, D. et al. Validity, reliability and reproducibility of three methods used to measure tooth widths for bolton analyses. Aust. Orthod. J. 25(2), 97–103 (2009).
Santoro, M. et al. Comparison of measurements made on digital and plaster models. Am. J. Orthod. Dentofacial Orthop. 124(1), 101–105 (2003).
Joda, T., Zarone, F. & Ferrari, M. The complete digital workflow in fixed prosthodontics: A systematic review. BMC Oral Health 17(1), 124 (2017).
Menees, T. S. et al. Contact angle of unset elastomeric impression materials. J. Prosthet Dent. 114(4), 536–542 (2015).
Kugel, G. et al. Investigation of a new approach to measuring contact angles for hydrophilic impression materials. J. Prosthodont. 16(2), 84–92 (2007).
Walker, M. P. et al. Moisture effect on polyether and polyvinylsiloxane dimensional accuracy and detail reproduction. J. Prosthodont. 14(3), 158–163 (2005).
Rubel, B. S. Impression materials: A comparative review of impression materials most commonly used in restorative dentistry. Dent. Clin. North Am. 51(3), 629-642,vi (2007).
Faria, A. C. et al. Accuracy of stone casts obtained by different impression materials. Braz. Oral Res. 22(4), 293–298 (2008).
Koseoglu, M., Kahramanoglu, E. & Akin, H. Evaluating the effect of ambient and scanning lights on the trueness of the intraoral scanner. J. Prosthodont. 30(9), 811–816 (2021).
Revilla-León, M. et al. Does the available interocclusal space influence the accuracy of the maxillomandibular relationship captured with an intraoral scanner? J. Prosthet. Dent. https://doi.org/10.1016/j.prosdent.2022.09.004 (2022).
Chen, Y. et al. Influence of liquid on the tooth surface on the accuracy of intraoral scanners: An in vitro study. J. Prosthodont. 31(1), 59–64 (2022).
Kernen, F. et al. Accuracy of intraoral scans: An in vivo study of different scanning devices. J. Prosthet. Dent. 128(6), 1303–1309 (2022).
McLean, J. W. The estimation of cement film thickness by an in vivo technique. Br. Dent. J. 131(3), 107–111 (1971).
Ferrini, F. et al. Influence of intra-oral scanner (I.O.S.) on the marginal accuracy of CAD/CAM single crowns. Int. J. Environ. Res. Public Health 16(4), 544 (2019).
Martinez-Rus, F. et al. Marginal discrepancy of monolithic and veneered all-ceramic crowns on titanium and zirconia implant abutments before and after adhesive cementation: A scanning electron microscopy analysis. Int. J. Oral Maxillofac. Implants 28(2), 480–487 (2013).
Xie, Y. L. & Shen, G. Accuracy and reproducibility of intraoral scanning in vivo. Shanghai Kou Qiang Yi Xue 25(5), 593–599 (2016).
Ender, A., Attin, T. & Mehl, A. In vivo precision of conventional and digital methods of obtaining complete-arch dental impressions. J. Prosthet. Dent. 115(3), 313–320 (2016).
Ahlholm, P. et al. Digital versus conventional impressions in fixed prosthodontics: A review. J. Prosthodont. 27(1), 35–41 (2018).
Zimmermann, M. Die digitale Abformung mit dem Intraoralscanner: mehr als nur eine Abformung, in ZMK (Spitta-Verlag, 2016).
Serag, M. et al. A comparative study of the accuracy of dies made from digital intraoral scanning vs. elastic impressions: An in vitro study. J. Prosthodont. 27(1), 88–93 (2018).
Haddadi, Y., Bahrami, G. & Isidor, F. Accuracy of crowns based on digital intraoral scanning compared to conventional impression—A split-mouth randomised clinical study. Clin. Oral Investig. 23(11), 4043–4050 (2019).
Nagarkar, S. R. et al. Digital versus conventional impressions for full-coverage restorations: A systematic review and meta-analysis. J. Am. Dent. Assoc. 149(2), 139-147.e1 (2018).
Reddy, S. et al. Accuracy of impressions with different impression materials in angulated implants. Niger. J. Clin. Pract. 16(3), 279–284 (2013).
Sfondrini, M. F. et al. Computerized casts for orthodontic purpose using powder-free intraoral scanners: Accuracy, execution time, and patient feedback. Biomed. Res. Int. 2018, 4103232 (2018).
Patzelt, S. B. et al. Accuracy of computer-aided design/computer-aided manufacturing-generated dental casts based on intraoral scanner data. J. Am. Dent. Assoc. 145(11), 1133–1140 (2014).
Nedelcu, R. et al. Accuracy and precision of 3 intraoral scanners and accuracy of conventional impressions: A novel in vivo analysis method. J. Dent. 69, 110–118 (2018).
Michelinakis, G. et al. A comparison of accuracy of 3 intraoral scanners: A single-blinded in vitro study. J. Prosthet. Dent. 124(5), 581–588 (2020).
Albdour, E. A. et al. A novel in vivo method to evaluate trueness of digital impressions. BMC Oral Health 18(1), 117 (2018).
Yatmaz, B. B., Raith, S. & Reich, S. Trueness evaluation of digital impression: The impact of the selection of reference and test object. J. Dent. 111, 103706 (2021).
Mangano, F. G. et al. Trueness of 12 intraoral scanners in the full-arch implant impression: A comparative in vitro study. BMC Oral Health 20(1), 263 (2020).
Acknowledgements
The authors thank PD Dr. Werner Adler (Department of Medical Informatics, Biometry and Epidemiology Friedrich-Alexander-University of Erlangen-Nuremberg, Germany) for the statistic evaluation and the company GOM, ZEISS (Braunschweig, Germany) for the permission to use the Atos Industrial Scanner and Atos Professional Software. A part of this study will also be discussed in the upcoming dissertation of Maria Paulig (Friedrich-Alexander-University Erlangen-Nuremberg, Germany).
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
All authors contributed to and co-authored the submitted manuscript. Y.O. performed the clinical examinations and was instrumental in the preparation of the manuscript and in the literature search. She compared the results from the current literature with those obtained in our study. S.A-H. performed the clinical examinations and participated in the design of the manuscript and interpretation of the results. M.P. performed the documentation of the clinical examination and the three-dimensional evaluation. L.B. helped with the conduction of the study and wrote part of the material and methods and also part of the results. M.W. is the head of the prosthetic department in Erlangen. His experience and knowledge in the field of prosthodontics and science as well as constant corrections helped the authors in shaping the manuscript. R.E.M., project leader and developer of the three-dimensional examination method, helped interpret the three-dimensional results. He also made ongoing corrections to the manuscript. All authors involved agree with the publication.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Onbasi, Y., Abu-Hossin, S., Paulig, M. et al. Trueness of full-arch dental models obtained by digital and conventional impression techniques: an in vivo study. Sci Rep 12, 22509 (2022). https://doi.org/10.1038/s41598-022-26983-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-26983-5
- Springer Nature Limited