
Abstract
The aim of this systematic review (qualitative analysis) was to identify the variables of changes induced by extrinsic (sport specific training) and intrinsic (individual anatomical predispositions) compensatory mechanisms that impact on the physiological magnitude of spinal curvatures in the sagittal plane and their deviations in the frontal plane. Furthermore, the aim of the quantitative analysis was to verify and objectivize the impact of these variables on athlete’s body posture. A search of electronic database (PubMed, EBSCO, MEDLINE) was conducted to identify all studies on sports training and athlete’s spine and body posture from 2011 to 2021. In the sagittal plane, the pooled proportion accounted for 44.97% (95% CI 31.22–58.72%) for thoracic hyperkyphosis (TH), 4.98% (95% CI 1.60–8.36%) for lumbar hyperlordosis (hyperLL), and 12.35% (95% CI 1.60–8.36%) for lumbar hypolordosis (hypoLL). Furthermore, in the sagittal plane, the pooled mean of thoracic kyphosis angle was 37.59° (95% CI 34.45–40.73%), whereas lumbar lordosis angle was 29.79° (95% CI 26.46–33.12%). Professional athletes tend to have postural disturbances and/or spinal curvature disorders in the sagittal and frontal planes. The meta-analysis indicated which intrinsic and extrinsic components might induce spinal abnormalities.
Similar content being viewed by others


Introduction
Human posture changes during ontogeny and is affected by multiple factors including gender, age, somatic parameters, lifestyle, muscular strength, and balance1,2,3. Nevertheless, a crucial indicator of the proper body posture is the shape of the anteroposterior spinal curvatures i.e., kyphosis and lordosis, and the symmetry between each other in the sagittal and frontal planes3,4. Since it was acknowledged that physical activity impacts on the spinal shape, athlete’s body posture has been the subject of interest of sport scientists5,6,7,8. Despite the high level of athleticism, different postural disturbances are frequently observed in athletes9,10. The currently available scientific literature indicates that specialized athletic training contributes to inducing adaptations in physique and posture among athletes5. As a result of high training loads and a focus on repetition of specific movements, there is a tendency for muscular dystonia and spinal curvature disturbances11, which can cause musculoskeletal pain, increase the risk of injuries and traumas, decrease athletic performance, and affect the quality of life both during the competitive period and after the end of the athletic career12,13.
The human body always strives to maintain the state of equilibrium and, for this purpose, it activates compensatory yet not always beneficial mechanisms. There are two important and closely related adaptation strategies: intrinsic and extrinsic. The intrinsic compensatory mechanism is defined as self-activating changes in the musculoskeletal system that are related to the individual anatomical structure, whereas the extrinsic compensatory mechanism is responsible for the adaptation of the athlete's body to specific movements resulting from a given sport13. It should be noted that the athletes cannot influence individual genetic and anatomical predispositions14, thus the intrinsic adaptation strategy is one-sided. The opposite phenomenon is observed in relation to the mechanism of extrinsic compensation, which is the result of a process that is strictly defined, repeatable, and dependent on the athlete (athletic training). The extrinsic adaptation strategy affects the athlete's body in two ways, i.e. (a) it can induce new musculoskeletal adaptations, and (b) it can aggravate existing adaptations.
The analysis of the available scientific literature indicates a significant trend of postural disturbances in athletes5,6,7,8,10,11,12,15,16. Thus, there have been several theories and hypotheses concerning the factors that might cause disturbances in spinal curvatures, however, this problem remains unsolved. Some authors suggest that sport-specific training is the main factor that induces spinal disturbances in the athlete’s body10,11,12,15,16,17,18, whereas other scientists observed no relationship between those components9,10,19,20. At the same time, studies have identified different factors that might affect the athlete’s posture and indicated the need for deeper analyses.
Spinal curvatures have been the subject of the previous meta-analyses21,22, yet, to the best of the authors’ knowledge, no study has analysed the effects of extrinsic and intrinsic compensatory mechanisms on magnitude of spinal curvatures and athlete’s body posture. Given the abovementioned findings and the gap in the available scientific literature, there is a need for additional research to evaluate the effect of various variables on athlete’s spine that may help in the development of training programs and in the selection of the most appropriate training methods to prevent spinal disorders, postural disturbances, musculoskeletal complaints, and exclusion from the training process. Accordingly, the aim of this systematic review (qualitative analysis) was to identify the variables of changes induced by extrinsic (sport specific training) and intrinsic (individual anatomical predispositions) compensatory mechanisms that impact on the physiological magnitude of the spinal curvatures in the sagittal plane and theirs deviations in the frontal plane. Furthermore, the aim of the meta-analysis (quantitative analysis) was to verify and objectivize the impact of these variables on athlete’s body posture.
Methods
Study design
The methodology of this systematic review was planned according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines23.
Inclusion and exclusion criteria
In this systematic review, inclusion criteria for studies (a) cross-sectional study, (b) measurement of spinal curvatures in at least one plane, (c) well-trained or elite male and/or female athletes, (d) able-bodied athletes, and (e) symmetric or asymmetric sport. The exclusion criteria were as follows: (a) no data on the angle of thoracic kyphosis and/or lumbar lordosis and/or trunk rotation, (b) the assessment of the body posture and/or spinal curvatures performed with subjective methods e.g. specific test, (c) poor methodological design or measurement of parameters, and (d) full-text not in English.
Literature search
A search of electronic databases (PubMed, EBSCO, MEDLINE) was conducted by two authors (AZ, EG) to identify all studies on sport-specific training and athlete’s spine and body posture from 2011 to 2021. The following methods were used: (a) data mining, (b) data discovery and classification. As a prerequisite, all studies were performed in healthy populations including both adults and adolescents (> 11 years). Search terms were combined by Boolean logic (AND/OR) in PubMed, EBSCO and MEDLINE databases. The search was undertaken using the following 7 keyword combinations in English with the assumed hierarchy of their importance: ‘body posture’, ‘athletes’, ‘postural disorders’, ‘spinal deformities’, ‘kyphosis’, ‘lordosis’, ‘scoliosis’. Furthermore, two authors (AZ, EG) with expertise in the spinal curvatures and body posture reviewed the reference lists of the included studies and screened Google Scholar to find additional studies. The corresponding authors of the selected publications were also contacted directly if the crucial data were not available in the original articles.
Methodological quality of included studies (risk of bias)
The methodological quality of the included studies was evaluated by the Joanna Briggs Institute (JBI) Critical Appraisal Checklist for analytical cross-sectional study24. The JBI is known as the newest and the most preferred tool for assessing the methodological quality (risk of bias) of analytical cross-sectional studies24. The checklist consists of 8 questions (see Table 1). Each study was read and scored ‘Yes’, ‘No’, ‘Unsure’, or ‘Not applicable’. If the criterion was fulfilled, a ‘Yes’ was assigned to the article, which simultaneously received a score of one, whereas if the criterion was not fulfilled, a ‘No’, ‘Unclear’, or ‘Not applicable’ was assigned to the article, and the article received a zero score. Each study was read and ranked by two independent investigators (AZ, EG). Moreover, an independent co-author (AM) was designated to resolve all discrepancies that could occur among investigators during the assessment. The sum of the awarded points (out of a possible 8 points) indicated the methodological quality (risk of bias), with the higher values representing better quality in the included publications.

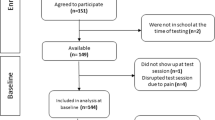
PRISMA flow diagram detailing the study inclusion process23.
Selection of articles for the meta-analysis
Based on the reports of other authors25 dealing with meta-analysis, the quality of the included studies was assessed using the Newcastle–Ottawa Scale (NOS) for cohort studies26. NOS assesses each study according to the following categories: selection of the study groups, comparability of the groups, and ascertainment of the outcome of interest. Selection of the study groups is performed by evaluating the representativeness of the exposed cohort, the selection of the non-exposed cohort, ascertainment of exposure, and demonstration that the outcome of interest was not present at the start of the study25. Comparability of the groups is assessed by evaluating the cohorts based on the design or analysis. Ascertainment of the outcome of interest includes evaluation of outcome parameters, and the length and adequacy of follow-up. A study can be awarded a maximum of one star for each item within the selection and outcome categories, and a maximum of two stars can be given for comparability26.
Statistical analysis
The statistical analysis was conducted on meta-analyses of proportions to combine data or meta-analyses of means to combine data. The studies were weighted by the inverse variance method for pooling. Between-study heterogeneity was explored using forest plots and was evaluated statistically using I2, which represents the percentage of between-study variation that is due to heterogeneity rather than to chance27. I2 of 0% indicates the absence of heterogeneity, while values of 50% or above suggest considerable heterogeneity28. We used a random-effects model since it is more conservative and the observed heterogeneity was > 50%. Statistical analysis was carried out using PQStat Software (2021, PQStat v.1.8.2.208). We did not use either funnel plots or formal statistical tests to explore publication bias as the number of articles used for analysis was not adequate for interpreting funnel plots. Moreover, funnel plots can be misleading for exploration of publication bias, particularly when the number of studies is relatively small29.
Results
Study selection and characteristics
Figure 1 presents the flow of the systematic review. Thirty three full-text articles were assessed to determine eligibility, while seventeen studies met the inclusion criteria and were subjected to detailed analysis and assessment of their methodological quality (see Table 1).
Over three-fourths of the reports that were assessed for their methodological quality were considered to have 8/8 points of eligibility to be included in the systematic review. Two publications6,9 were considered to have 6/8 points of eligibility and one25 scored 5/8 points of eligibility. The initial agreement of the two independent investigators (AZ, EG) was 90%. All discrepancies among the investigators were resolved by the expert evaluation by an independent co-author (AM).
Seventeen full-text articles were finally included in the systematic review (see Table 2), while ten publications were included in various meta-analyses.
Characteristics of the studies included in the meta-analysis
Quality assessment of the included studies using the NOS is shown in Tables 3 and 4. The studies included in the meta-analysis had an overall good quality for ascertainment of the outcome of interest and selection of the studies. Frequent causes of scoring low on the quality assessment were (a) studies derived from high-risk populations, and (b) lack of description of the outcome of individual cases.
Based on the analyzed data, several meta-analysis models were built (Figs. 2A–C, 3A,B). PQStat software (version PQStat V 1.8.4) was used to create all models.

Forest plot (random-effects model) showing the incidence of (A) hyper TH, (B) hyper LL, (C) hypo LL in the sagittal plane for each of the included studies and the pooled incidence for all studies (created with: PQStat software (version PQStat V 1.8.4).

Forest plot (random-effects model) showing mean (A) ThK Angle (°), (B) LL Angle(°) in the sagittal plane for each of oncluded studies and the pooled data for all studies (created with: PQStat software (version PQStat V 1.8.4).
In the first random model, they were used to classify the proportion of thoracic hyperkyphosis (TH) in the sagittal plane (Fig. 2A). Statistical analysis of the research results for hyper TH in the sagittal plane allowed for a significant heterogeneity between the 11 studies included in the analysis. The analysis found that I2 was above 50% for almost all analyzed results. Therefore, it was decided to use the model for random effects. Based on the acquired knowledge, in the present paper, a meta-analysis of proportions was used and forest plots were presented to illustrate the proportion of hyperTH in the sagittal plane. The results for each of the 11 studies included in the meta-analysis are presented as proportions and 95% CIs, together with pooled results for all studies, with the size of the boxes proportional to that of the study sample. Data were reported for 502 athletes. Of these athletes, 248 had hyperTH in the sagittal plane. The analysis led to the conclusion that the pooled proportion of hyperTH in the sagittal plane accounted for 44.97% (95% CI 31.22–58.72%) (Fig. 2A). It was found that for 6 reports (Rajabi et al.17, Muyor et al.19, Grabara11, and Gines-Diaz et al.7 (show jumping)), the incidence of hyperTH was higher than the pooled proportion of hyperTH in the sagittal plane, especially in the report by Rajabi et al.17.
The second random model classified the proportion of lumbar hyperlordosis (hyperLL) in the sagittal plane (Fig. 2B). Statistical analysis of the research results for hyperLL in the sagittal plane allowed for a significant heterogeneity between the 10 studies included in the analysis. The analysis found that I2 was above 50% for almost all analyzed results. Therefore, it was decided to use the model for random effects. Based on the acquired knowledge, in the present paper, a meta-analysis of proportions was used and forest plots were presented to illustrate the proportion of hyperLL in the sagittal plane. The results for each of the 10 studies included in the meta-analysis are presented as proportions and 95% CIs, together with pooled results for all studies, with the size of the boxes proportional to that of the study sample. Data were reported for 465 athletes. Of these athletes, 38 had hyperLL in the sagittal plane. The analysis led to the conclusion that the pooled proportion of hyperLL in the sagittal plane accounted for 4.98% (95% CI 1.60–8.36%) (Fig. 2B). It was found that for 5 reports (Muyor et al.9 (females), Grabara11, Sanz-Mengibar et al.6, and Gines-Diaz et al.7), the incidence of hyperLL was higher than the pooled proportion of hyperLL in the sagittal plane, especially in the report by Gines-Diaz et al.7.
The third random model classified the proportion of hypoLL in the sagittal plane (Fig. 2C). Statistical analysis of the research results for hypoLL in the sagittal plane allowed for a significant heterogeneity between the 10 studies included in the analysis. The analysis found that I2 was above 50% for almost all analyzed results. Therefore, it was decided to use the model for random effects. Based on the acquired knowledge, in the present article, a meta-analysis of proportions was used and forest plots were presented to illustrated the proportions of hypoLL in the sagittal plane. The results for each of the 10 studies included in the meta-analysis are presented as proportions and 95% CIs, together with pooled results for all studies, with the size of the boxes proportional to that of the study sample. Data were reported for 465 athletes. Of these athletes, 93 had hypoLL in the sagittal plane. The analysis led to the conclusion that the pooled proportion of hypoLL in the sagittal plane accounted for 12.35% (95% CI 1.60–8.36%) (Fig. 2C). It was found that for 3 reports (Mueor et al.19 (masters), Grabara,11 (males) and Sanz-Mengibar et al.6), the incidence of hypoLL was higher than the pooled proportion of hypoLL in the sagittal plane, especially in the report by Grabara11 (males).
The fourth random model classified means of thoracic kyphosis angle (ThK) (°) in the sagittal plane (Fig. 3A). Statistical analysis of the research results for mean ThK Angle (°) in the sagittal plane allowed for a significant heterogeneity between the 16 studies included in the analysis. The analysis found that I2 was above 50% for almost all analyzed results. Therefore, it was decided to use the model for random effects. Based on the acquired knowledge, in the present article, a meta-analysis of means was performed and forest plots were used to illustrate mean ThK Angle (°) in the sagittal plane. The results for each of the 16 studies included in the meta-analysis are presented as means and 95% CIs, together with pooled results for all studies, with the size of the boxes proportional to that of the study sample. Data were reported for 691 athletes. The analysis led to the conclusion that the pooled mean ThK Angle (°) in the sagittal plane accounted for 37.59 (°) (95% CI 34.45–40.73%) (Fig. 3A). It was found that in the case of 7 reports, the mean was higher than the pooled mean ThK Angle (°) in the sagittal plane, especially in the report by Muyor et al.19 (elite athlets).
The fifth random model classified mean LL Angle (°) in the sagittal plane (Fig. 3B). Statistical analysis of the research results for mean LL Angle (°) in the sagittal plane allowed for a significant heterogeneity between the 15 studies included in the analysis. The analysis found that I2 was above 50% for almost all analyzed results. Therefore, it was decided to use the model for random effects. Based on the acquired knowledge, in the present article, a meta-analysis of means was used and forest plots were presented to illustrate mean LL Angle (°) in the sagittal plane. The results for each of the 15 studies included in the meta-analysis are presented as means and 95% CIs, together with pooled results for all studies, with the size of the boxes proportional to that of the study sample. Data were reported for 601 athletes. The performed analysis led to the conclusion that the pooled mean LL Angle (°) in the sagittal plane accounted for 29.79 (°) (95% CI 26.46–33.12%) (Fig. 3B). It was found that in the case of 4 reports, the mean was higher than the pooled mean LL Angle (°) in the sagittal plane, especially in the report by Yang et al.20.
Discussion
A careful examination of the current scientific studies on the effect of sport-specific training on the magnitudes of spinal curvatures and athlete’s body posture has yielded partially inconsistent findings. However, this systematic review found athletic training to be the most frequent variable that impacts on the athlete’s spine and body posture.
The majority of the studies have found a directly proportional relationship between spinal curvature abnormalities or disorders and sport-specific training5,6,7,8,11,12,16,17,18. On the contrary, four investigations conducted by Muyor et al.9,19, Yang et al.20, and Grabara10 did not report any effect of athletic training on the magnitude of spinal curvatures. The inconsistences in the results of the cited studies can be explained mainly by differences in the characteristics of participants, which is presented in the qualitative analysis of this systematic review including (i) extrinsic compensatory mechanisms such (a) type of sport, (b) training experience, (c) duration and/or intensity of sports trainings, and (d) training loads, and (ii) intrinsic compensatory mechanisms, such as (a) gender, (b) age, and (c) joints mobility.
Numerous authors have suggested that sport-specific training contributes to the depth of the anteroposterior spinal curvatures. Most of the studies have indicated the deepening of the thoracic kyphosis6,7,8,11,16,17, whereas several investigations have found flattening of the thoracic and/or lumbar spine5,6,9,11. In the present meta-analysis, the conducted quantitative synthesis confirmed a general tendency for imbalances between thoracic and lumbar curvatures in professional athletes. Furthermore, it allowed for indicating which of the analyzed reports was closest to the statement about the effect of extrinsic compensatory mechanisms (athletic training). As reported in the studies by Grabara11, Gines-Diaz et al.7, Muyor et al.19, and Rajabi et al.17, extrinsic compensation might significantly contribute to disturbances in the athlete’s body posture i.e., thoracic hyperkyphosis11,17, lumbar hypolordosis7,11, as confirmed by the results of the meta-analysis (Figs. 2A–C, 3A,B].
Rajabi et al.17 and Bańkosz12 suggested that training experience and duration of a sports training impact on spinal imbalances, especially by deepening of the kyphosis in the thoracic segment of the spine. On the contrary, the studies by Yang et al.20, Sanz-Mengibar et al.6 and Gines-Díaz et al.7 did not report any relationships between the magnitude of spinal curvatures and duration and/or intensity of training sessions and suggested the need for further research. Muyor et al.19 indicated that it is higher weekly training loads (rather than the duration of training sessions) that impact on the depth of thoracic kyphosis. These results were also confirmed by Grabara5, who reported a significant correlation between the increase in the depth of thoracolumbar segment curvature and duration of training sessions. The conducted meta-analysis corresponds with the uncertainty of the cited studies6,7,20 and indicates the complexity of the phenomenon of body posture variability that seems to depend both on the kind of sport and training experience. At the same time, there is the need to indicate the importance of neurophysiological mechanisms to postural control in athletes, which were found to impact significantly on intrinsic postural regulation33. Furthermore, the findings of our meta-analysis directly indicate the sports in which athletes are characterized by greater values of thoracic kyphosis and/or lumbar lordosis angles (extrinsic adaptation mechanism).
The systematic review suggested that spinal curvatures imbalances could be induced by sports training during the somatic development18. Furthermore, anatomical differences in pelvic inclination between genders seem to significantly contribute to anteroposterior spinal curvatures9, what might be a result of result from the body’s intrinsic adaptation strategies. Garbara11 and Gines-Diaz7 reported a tendency for the increase in the magnitude of lumbar curvature in female athletes, whereas the studies of Muyor et al.9 and Grabara11 indicated that male adolescent athletes tend to show deepened thoracic curvature but at the same time, they stressed the need for deeper analyses. As regards the intrinsic adaptation strategies, joint mobility might contribute to spinal curvature disorders as its could impact on the pelvic inclination19. As was reported in the study by Muyor et al.19, athletes with greater hamstring flexibility had a significantly greater pelvic tilt and deepened lumbar lordosis, whereas those with lesser flexibility showed a lumbar hypolordotic spine19. Similar conclusions were presented by Yang et al.20, who suggested that the stiffness of the lower lumbar segments and limited spinal joint mobility contribute to the depth of the lumbar lordosis. The abovementioned findings indicate the prevalence of postural disturbances and spinal curvature disorders in professional athletes, which is consistent with the results of the conducted meta-analysis (Figs. 2A–C, 3A,B]. Furthermore, both intrinsic and extrinsic compensatory mechanisms seem to lead to disorders in the athlete’s spine.
Unfortunately, the currently available scientific studies that have examined athlete’s spinal curvatures in the frontal plane did not provide enough data to conduct a meta-analysis. Nevertheless, based on the detailed examination of the current scientific reports (Table 2) it is difficult to confirm the direct effect of sports training on the development of scolioses in athletes. For instance, Longworth et al.15 found a relationship between the incidence of scolioses and sport-specific training. On the contrary, other studies have indicated that scoliosis can be induced by other factors30,31,32.
The incompatible results of the presented reports can be explained mainly by differences in the characteristics of participants, including (1) extrinsic compensatory mechanisms, such as (a) type of sport, and (b) training loadsand (2) intrinsic compensatory mechanisms, such as (a) body mass, (b) joint mobility and function, (c) gender, and (d) age.
In should be noted that studies that have examined adolescent athletes reported a high prevalence of trunk asymmetries and adolescent idiopathic scolioses (AIS)5,10,15,16,30. As regards the cited reports, they might have been due to intrinsic (low body mass, joints hypermobility/hypomobility, muscle imbalance, sacroiliac joint dysfunction) and extrinsic (high training loads in sport-specific training, symmetric/asymmetric sports techniques) adaptation strategies5,10,15,16,30,32. These findings are consistent with the studies by Grabara5, Bańkosz et al.12, Zaina et al.16, who suggested that sport-specific training could be the major contributor to postural disturbances in the frontal plane because of the body’s extrinsic adaptation strategy.
Longworth et al.15 did not report any relationships between scoliosis and training loads in adolescent athletes but indicated that intrinsic factors might contribute to spinal aberrations in the frontal plane. Similar findings were reported by Park et al.32 who compared the prevalence of scoliosis and training period in female adolescent athletes and found no correlation between those components. However, the incidence of scoliosis was directly proportional to the intrinsic variables such as age, body height and body mass.
The study by Šarčević et al.31 found a strong relationship between sacroiliac joint dysfunction and the incidence of AIS in young athletes, whereas Sanz-Mengibar et al.6 and Bańkosz et al.12 indicated gender as a relevant variable to induce disorders in spinal curvatures of athletes. Based on the above studies, a tendency for trunk asymmetries and spinal curvature disturbances were found in female athletes. Furthermore, Longworth et al.15 suggested that joints hypermobility, low body mass, and delayed maturation could activate body’s intrinsic strategies, while Park et al.32 found that decreased total hip-joint flexibility and range of motion might induce AIS in females.
Limitations and strengths
While this systematic review and meta-analysis relevantly contributes to the current body of literature, there are some limitations that need to be acknowledged. The main limitation of the current study is the small number of studies that have investigated the athlete’s spinal curvatures in the frontal plane, which did not allow for conducting a quantitative analysis. Furthermore, diverse research tools were used to evaluate the magnitude of spinal curvatures in the sagittal plane, which makes generalization impossible. At the same time, the current body of research that has evaluated the athlete’s spinal curvatures in the frontal plane failed to provide enough data to conduct a quantitative analysis. The main strength of the presented paper is the qualitative and quantitative analysis and synthesis of the latest reports that have examined the athlete’s body posture. Moreover, three-fourths of the included reports were considered to be perfectly eligible for including in this study. In authors’ opinion, the novelty of the presented research problem and undertaking the aspects hitherto unexplored in the scientific literature will help improve scientific methodology and optimize training programs of professional athletes in terms of improved health, athletic development, and prevention of the exclusion form the training process.
Conclusions
The present meta-analysis of the results of published scientific literature provides evidence that professional athletes tend to have postural disturbances and/or spinal curvature disorders. At the same time, the study indicates which intrinsic and extrinsic components might lead to spinal aberrations and points to extrinsic adaptations as a primary compensatory mechanisms in well-trained able-bodied athletes.
To date, it remains unclear whether or not professional sport leads to the spinal curvature asymmetries and scoliosis. However, as they are common in athletes, this issue needs further and deeper analyses.
Practical implications
The presented results indicate the necessity of performing investigations with a protocol that assess athlete’s body posture both in the frontal and sagittal planes with the use of objective research tools, which will allow to refer to angular values. Furthermore, authors should employ control groups to reduce the risk of bias (Supplementary Information S1).
Data availability
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
References
Zwierzchowska, A., Rosołek, B., Celebańska, D., Gawlik, K. & Wójcik, M. The prevalence of injuries and traumas in elite goalball players. Int. J. Environ. Res. Public Health. 17(7), 2496. https://doi.org/10.3390/ijerph17072496 (2020).
Grabara, M. Spinal curvatures of yoga practitioners compared to control participants—a cross-sectional study. PeerJ 9, e12185. https://doi.org/10.7717/peerj.12185 (2021).
Tuz, J., Maszczyk, A. & Zwierzchowska, A. Variability of body build and physiological spinal curvatures of young people in an accelerated longitudinal study. Int. J. Environ. Res. Public Health. 18(14), 7590. https://doi.org/10.3390/ijerph18147590 (2021).
Zwierzchowska, A. & Tuz, J. Evaluation of the impact of sagittal spinal curvatures on musculoskeletal disorders in young people. Med. Pr. 69(1), 29–36. https://doi.org/10.13075/mp.5893.00558 (2018).
Grabara, M. A comparison of the posture between young female handball players and non-training peers. J. Back Musculoskelet. Rehabil. 27(1), 85–92. https://doi.org/10.3233/BMR-130423 (2014).
Sanz-Mengibar, J. Training intensity and sagittal curvature of the spine in male and female artistic gymnasts. J. Sports Med. Phys. Fitness. 58(4), 465–471. https://doi.org/10.23736/S0022-4707.17.06880-3 (2018).
Ginés-Díaz, A. & Martínez-Romero, M. Sagittal spinal morphotype assessment in dressage and show jumping riders. J. Sport Rehabil. 29(5), 533–540. https://doi.org/10.1123/jsr.2018-0247 (2019).
Sainz de Baranda, P. et al. Sagittal spinal morphotype assessment in 8 to 15 years old Inline Hockey players. PeerJ 8, e8229. https://doi.org/10.7717/peerj.8229 (2020).
Muyor, J. M., Sánchez-Sánchez, E., Sanz-Rivas, D. & López-Miñarro, P. A. Sagittal spinal morphology in highly trained adolescent tennis players. J. Sports Sci. Med. 12(3), 588–593 (2013).
Grabara, M. Comparison of posture among adolescent male volleyball players and non-athletes. Biol. Sport. 32(1), 79–85. https://doi.org/10.5604/20831862.1127286 (2015).
Grabara, M. Anteroposterior curvatures of the spine in adolescent athletes. J. Back Musculoskelet. Rehabil. 27(4), 513–519. https://doi.org/10.3233/BMR-140475 (2014).
Bańkosz, Z. & Barczyk-Pawelec, K. Habitual and ready positions in female table tennis players and their relation to the prevalence of back pain. PeerJ 8, e9170. https://doi.org/10.7717/peerj.9170 (2020).
Gaweł, E. & Zwierzchowska, A. Effect of compensatory mechanisms on postural disturbances and musculoskeletal pain in elite sitting volleyball players: Preparation of a compensatory intervention. Int. J. Environ. Res. Public Health. 18(19), 105. https://doi.org/10.3390/ijerph181910105 (2021).
Suchomel, T. J., Nimphius, S. & Stone, M. H. The importance of muscular strength in athletic performance. Sports Med. 46(10), 1419–1449. https://doi.org/10.1007/s40279-016-0486-0 (2016).
Longworth, B., Fary, R. & Hopper, D. Prevalence and predictors of adolescent idiopathic scoliosis in adolescent ballet dancers. Arch. Phys. Med. Rehabil. 95(9), 1725–1730. https://doi.org/10.1016/j.apmr.2014.02.027 (2014).
Zaina, F., Donzelli, S., Lusini, M., Minnella, S. & Negrini, S. Swimming and spinal deformities: A cross-sectional study. J. Pediatr. 166(1), 163–167. https://doi.org/10.1016/j.jpeds.2014.09.024 (2015).
Rajabi, R., Mobarakabadi, L., Alizadhen, H. M. & Hendrick, P. Thoracic kyphosis comparisons in adolescent female competitive field hockey players and untrained controls. J. Sports. Med. Phys. Fitness. 52(5), 545–550 (2012).
Grabara, M. The posture of adolescent male handball players: A two-year study. J. Back. Musculoskelet. Rehabil. 31(1), 183–189. https://doi.org/10.3233/BMR-170792 (2018).
Muyor, J. M., López-Miñarro, P. A. & Alacid, F. Spinal posture of thoracic and lumbar spine and pelvic tilt in highly trained cyclists. J. Sports Sci. Med. 10(2), 355–361 (2011).
Yang, J. H. et al. Changes in the spinopelvic parameters of elite weight lifters. Clin. J. Sport. Med. 24(4), 343–350. https://doi.org/10.1097/JSM.0000000000000094 (2014).
Chun, S. W., Lim, C. Y., Kim, K., Hwang, J. & Chung, S. G. The relationships between low back pain and lumbar lordosis: A systematic review and meta-analysis. Spine J. 17(8), 1180–1191. https://doi.org/10.1016/j.spinee.2017.04.034 (2017).
González-Gálvez, N., Gea-García, G. M. & Marcos-Pardo, P. J. Effects of exercise programs on kyphosis and lordosis angle: A systematic review and meta-analysis. PLoS ONE 14(4), 6180. https://doi.org/10.1371/journal.pone.0216180 (2019).
The PRISMA 2020 statement: An updated guideline for reporting systematic reviews | The EQUATOR Network (equator-network.org)
Ma, L.L. et al. Methodological quality (risk of bias) assessment tools for primary and secondary medical studies: what are they and which is better? Mil. Med. Res. 7(1), 7 (2020). https://doi.org/10.1186/s40779-020-00238-8.
Carta, S., Kaelin Agten, A., Belcaro, C. & Bhide, A. Outcome of fetuses with prenatal diagnosis of isolated severe bilateral ventriculomegaly: Systematic review and meta-analysis. Ultrasound Obstet. Gynecol. 52(2), 165–173. https://doi.org/10.1002/uog.19038 (2018).
Wells, G.A. et al. The Newcastle–Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. The Ottawa Hospital Research Institute: Ottawa, Canada, 1–4 (2013).
Coleman, S. R., Mazzola, R. F., Guyatt, G., Rennie, D. & Meade, M. Users’ guides to the medical literature: A manual for evidence-based clinical practice. Evid. Based Med. 62, 359 (2008).
Higgins, J. P., Thompson, S. G., Deeks, J. J. & Altman, D. G. Measuring inconsistency in meta-analyses. BMJ 327(7414), 557–560. https://doi.org/10.1136/bmj.327.7414.557 (2003).
Lau, J., Ioannidis, J. P., Terrin, N., Schmid, C. H. & Olkin, I. The case of the misleading funnel plot. BMJ 333(7568), 597–600. https://doi.org/10.1136/bmj.333.7568.597 (2006).
Trexler, E. T., Smith-Ryan, A. E., Roelofs, E. J. & Hirsch, K. R. Body composition, muscle quality and scoliosis in female collegiate gymnasts: A pilot study. Int. J. Sports Med. 36(13), 1087–1092. https://doi.org/10.1055/s-0035-1555781 (2015).
Šarčević, Z. & Tepavčević, A. Association between adolescent idiopathic scoliosis and sacroiliac joint dysfunction in young athletes: A case control study. Medicine 98(15), 5161. https://doi.org/10.1097/MD.0000000000015161 (2019).
Park, S., Cho, D. & Kim, L. Characteristics of elite rhythmic gymnasts with scoliosis in Korea. Int. J. Appl. Sports Sci. 33(2), 159–166 (2021).
Bieniek, K. & Wilczyński, J. Characteristics of the correlations between body posture and postural stability in boys aged 10–12 years. Balt. J. Health Phys. Activ. 11(2), 65–74. https://doi.org/10.29359/BJHPA.11.2.07 (2019).
Acknowledgements
Open access was funded by The Jerzy Kukuczka Academy of Physical Education in Katowice—Institute of Sport Sciences, grant number AWF/INS/ZB2/2022.
Author information
Authors and Affiliations
Contributions
A.Z. conceptualized the purposes of the study, reviewed the list of the included studies and scanned the reference lists to find additional studies, read and evaluated the methodological quality of the selected studies, analyzed and interpreted the results, supervised during the study and was a major contributor in writing the original article. EG screened the databases, contacted directly the corresponding author, if the crucial data were not available in the original articles, read and evaluated the methodological quality of the selected studies, prepared tables, figures and was responsible for formatting, writing the review and editing. AM and RR performed the quantitative analysis and wrote the methods and results sections (quantitative analysis). All authors read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Zwierzchowska, A., Gaweł, E., Maszczyk, A. et al. The importance of extrinsic and intrinsic compensatory mechanisms to body posture of competitive athletes a systematic review and meta-analysis. Sci Rep 12, 8808 (2022). https://doi.org/10.1038/s41598-022-12979-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-12979-8
- Springer Nature Limited
This article is cited by
-
Differentiation of the body build and posture in the population of people with intellectual disabilities and Down Syndrome: a systematic review
BMC Public Health (2024)
-
The effect of swimming on the body posture, range of motion and musculoskeletal pain in elite para and able-bodied swimmers
BMC Sports Science, Medicine and Rehabilitation (2023)
-
Prediction of injuries, traumas and musculoskeletal pain in elite Olympic and Paralympic volleyball players
Scientific Reports (2023)