
Abstract
Ocular toxoplasmosis is the leading cause of posterior uveitis worldwide. We conducted an observational study of 262 consecutive individuals (n = 344 eyes) with ocular toxoplasmosis who were followed over a 34-month period. Most subjects were T. gondii IgG + /IgM- (n = 242; 92.4%; 317 eyes), and 140 eyes (40.7%) had active lesions. For eyes in which retinal lesions were active at recruitment and best-corrected visual acuity (BCVA) could be measured (n = 133), 21.0% (n = 28) remained blind (BCVA below 20/400) after inflammation resolved. In these eyes, atypical ocular toxoplasmosis (OR 4.99; 95% CI 1.14–22.85; p = 0.0330), macular lesion (OR 9.95; 95% CI 2.45–47.15; p = 0.0019) and any complication (OR 10.26; 95% CI 3.82–30.67; p < 0.0001) were associated with BCVA below 20/200. For eyes with only inactive lesions at recruitment and BCVA measured (n = 178), 28.1% (n = 50) were blind. In these eyes, having at least one lesion larger than one disc-diameter (OR 6.30; 95% CI 2.28–22.46; p = 0.0013) and macular lesion (OR 5.69; 95% CI 2.53–13.54; p < 0.0001) were associated with BCVA below 20/200. Older age (OR 1.02; 95% CI 1.00–1.05; p = 0.0493) and active disease at presentation (OR 4.74; 95% CI 1.95–12.91; p = 0.0011) were associated with recurrences. Additional clinical attention should be directed towards patients with risk factors for poor visual outcome.
Similar content being viewed by others


Introduction
The Apicomplexan protozoan, Toxoplasma gondii, infects an estimated 25% to 30% of the human population1. Although the infection is usually asymptomatic in otherwise healthy humans, multiple clinical manifestations of acute and chronic infection are widely described, and ocular toxoplasmosis is the most common manifestation in chronically infected subjects2, 3. Ocular toxoplasmosis almost always presents as necrotizing retinitis that is associated with inflammation in adjacent ocular tissues3, and the condition is one of the leading causes of posterior uveitis worldwide4. In Latin America, where the prevalence of T. gondii infection is relatively high5, ocular toxoplasmosis is the most common form of uveitis6, 7, and also a major cause of childhood blindness8.
While many individuals presenting ocular toxoplasmosis have normal visual acuity and a satisfactory vision-related quality of life9, ocular toxoplasmosis is frequently a sight-threatening condition. Several hospital-based studies describe visual impairment in up to one in four affected eyes, most often associated with central retinal lesions10, 11. Since the retinal tissue does not regenerate, even individuals who receive appropriate antimicrobial and anti-inflammatory drug treatment may suffer irreversible blindness (best-corrected visual acuity less than 20/400). Human hosts cannot eliminate T. gondii, and therefore persons with ocular toxoplasmosis remain at risk of reactivation of the disease, and ocular complications may occur years after the initial infection2, 3.
The majority of data that describe risk factors for the development of recurrent ocular toxoplasmosis and visual impairment caused by the disease come from retrospective studies conducted on European and North America populations10. In these regions of the world, ocular toxoplasmosis is believed to be less severe than in South and Central America4. Understanding which individuals have an increased risk of developing recurrent disease and vision loss is important for the ophthalmologist. In describing a large and prospectively studied Brazilian patient group, we aimed to determine the clinical manifestations and risk factors for poor visual outcomes of ocular toxoplasmosis in Latin America.
Results
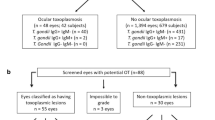
Clinical data were collected for 262 individuals (n = 344 eyes), who presented to the Ribeirão Preto General Hospital Uveitis Clinic with active or inactive ocular toxoplasmosis during the 34-month study period commencing January 14th, 2015 (Table 1). Mean follow-up was 12.9 months (standard deviation, 8.4 months; median, 11.9 months; range, 0–30.1 months). The study included 139 women (53.1%) and 123 men (46.9%). Within the group, 47.3% individuals (n = 124) considered themselves multiracial, 38.2% (n = 100) reported Caucasian ethnicity, 13.4% (n = 35) reported African-Brazilian ethnicity, and 1.1% (n = 3) did not report their ethnic background (Table 1). Age at inclusion was under 18 years in 11.1% of the persons (n = 29), 18–64 years in 79.8% (n = 209) and over 64 years in 9.2% (n = 24). Within the group of 262 persons, 3.8% (n = 10) were infected with human immunodeficiency virus (HIV).
For 50.7% (n = 133; 167 eyes) of the participants, ocular toxoplasmosis was active, and most often recurrent (n = 85; 115 eyes); and in 49.3% (n = 129; 177 eyes) of the participants, ocular toxoplasmosis was inactive (Table 1). Disease had a typical clinical appearance in most individuals (96.6%, n = 253; 330 eyes), and the mode of infection usually could not be determined in 85.9% (n = 225; 286 eyes). Just 7.6% of subjects (n = 20; 27 eyes) had serological evidence of acute infection (serum T. gondii IgG-positive and IgM-positive).
At presentation, 48.0% (n = 165) of the 344 affected eyes had a single retinal lesion, while 147 eyes (42.7%) had two to four lesions, and 32 eyes (9.3%) had five or more lesions (Table 2). Approximately half of the eyes had only peripheral retinal lesions (50.9%, n = 175), while the other half (49.1%, n = 169) had at least one lesion at the posterior pole. Most retinal lesions were measured greater than one disc-diameter (81.7%, n = 281). The lesions were active in 41.1% of eyes (n = 141), and 83.7% of eyes (n = 288) contained scars.
For the eyes in which retinal lesions were active at recruitment and best-corrected visual acuity could be measured (n = 133), 35.3% (n = 47) had normal acuity, 12.8% (n = 17) had acuities from 20/50 to 20/63, 18.1% (n = 24) had acuities from 20/63 to 20/160, 3.0% (n = 4) had acuities from 20/200 to 20/400, and 30.8% (n = 41) had visual acuities below 20/400 (Table 3). After the activity resolved in the 133 eyes, 56.4% (n = 75) had normal vision, and 21.0% (n = 28) were blind. Among these eyes, atypical ocular toxoplasmosis (odds ratio [OR]: 4.99; 95% confidence intervals [CI]: 1.14–22.85; p = 0.0330), macular lesion (OR 9.95; 95% CI 2.45–47.15; p = 0.0019) and development of any complication (OR 10.26; 95% CI 3.82–30.67; p < 0.0001) were associated with poor visual prognosis (Table 4). Best-corrected visual acuity could not be measured in 25 eyes (1 with an active lesion and 24 with inactive lesions) of 15 preverbal children.
For the eyes in which there were only inactive lesions at recruitment and best-corrected visual acuity could be measured (n = 178), 45.5% (n = 81) had normal acuity, while 28.1% (n = 50) had visual acuities below 20/400 (Table 3). In these 178 eyes, the presence of at least one lesion that measured greater than one disc-diameter in size (OR 6.30; 95% CI 2.28–22.46; p = 0.0013) and macular lesion (OR 5.69; 95% CI 2.53–13.54; p < 0.0001) were associated with a poor visual prognosis (Table 5).
Considering the visual acuity of the better-seeing eye in those with bilateral retinal lesions (either active or inactive ocular toxoplasmosis) and with final best-corrected visual acuity measured (n = 71 subjects), 73.2% (n = 52) had normal acuity, 9.9% (n = 7) had acuities from 20/50 to 20/63, 2.8% (n = 2) had acuities from 20/63 to 20/160, 5.6% (n = 4) had acuities from 20/200 to 20/400, and 8.5% (n = 6) had acuities below 20/400, rendering the individual bilaterally blind.
Older age (OR 1.02; 95% CI 1.00–1.05; p = 0.0493) and active ocular toxoplasmosis at presentation (OR 4.74; 95% CI 1.95–12.91; p = 0.0011) were the only risk factors associated with recurrence during follow-up (Table 6). Considering just the eyes that were followed over time (n = 292), we observed 28 episodes of reactivation during the follow-up period, with 21 of these reactivations occurring in eyes with active retinal lesions at enrollment. This equated to 0.091 (0.060 – 0.131, 95% CI) reactivations per eye-year across eyes presenting with either active or inactive lesions, and 0.172 (0.106 – 0.262, 95% CI) reactivations per eye-year for those eyes with active lesions at presentation.
Discussion
In this study of a large series of 262 Brazilian women and men who were followed prospectively for ocular toxoplasmosis, we observed permanent vision loss in approximately one-half of the eyes, with one in four eyes blind, and with six patients bilaterally blind. Among those eyes with active retinitis at presentation, we identified three clinical features that were associated with a final best-corrected visual acuity equal to or below 20/200: atypical ocular toxoplasmosis, the presence of a macula lesion, and the development of any ocular complication during follow up. For eyes that presented with inactive retinal scars, we found lesions in the macula and lesions measuring over one disc-diameter to be associated with this severe level of vision impairment. Older age and the presence of an active retinal lesion at presentation were associated with higher risk of disease recurrence, which may progress any vision loss.
Several other investigator teams have reported associations between characteristics of active ocular toxoplasmosis and severe vision impairment that are largely consistent with our findings in this larger group that also includes patients with inactive disease. One team, also from Brazil, prospectively studied a group of 230 subjects, and linked the same level of vision loss with location of the retinal lesion, presence of posterior eye complications and recurrence during follow-up11. Another team, based in The Netherlands, retrospectively evaluated a group of 154 consecutive patients, and associated size and location of the retinal lesion, as well as primary ocular toxoplasmosis and congenital toxoplasmosis, with visual acuity of 20/200 or worse. We did not assess the patient group for an association with the mode of infection (congenital or postnatally acquired), since the mode is seldom known with certainty.
Our study revealed that those individuals with active toxoplasmic retinal lesions at recruitment were at a higher risk of recurrence when compared to persons with inactive lesions (p = 0.001). This is in keeping with previous work describing recurrence patterns of ocular toxoplasmosis in a group of Dutch patients, which showed that recurrence risk was highest immediately after an episode of active disease and reduced with an increasing disease-free interval12. The alternate daily use of trimethoprim and sulfamethoxazole for one year after an active episode of ocular toxoplasmosis was first described by Brazilian ophthalmologists in 2002 as an option to reduce the risk of recurrences13. Subsequent studies that were also conducted in Brazil supported the preventive effect of the approach14, and showed that this effect was sustained over multiple years of follow-up15, 16.
Although the prophylactic use of trimethoprim and sulfamethoxazole in patients with ocular toxoplasmosis has become popular in Brazil17, the value of this therapy in non-endemic areas is less clear. While our study and previous reports suggest that patients at a higher risk of recurrence are those with a recent episode of active ocular toxoplasmosis, most of these people do not develop ocular recurrences within a short time frame. For this reason, we recommend preventive treatment be considered only for those patients with an increased risk of vision loss if their disease recurs. Recognizing that macular lesions are associated with a poor visual prognosis, and that active lesions frequently develop adjacent to retinochoroidal scars, an individualized approach may be taken to prophylactic drug therapy following recently active ocular toxoplasmosis.
Strengths of our study include the substantial number of prospectively enrolled subjects in an endemic area, the standardized process of data collection by a small number of specialized researchers, and the use of polymerase chain reaction (PCR) on intraocular fluid samples to confirm those cases of atypical toxoplasmosis. One limitation of our work, which is common to all studies on ocular toxoplasmosis, is the need to rely on clinical assessment and serological testing to make the diagnosis, since retinal biopsy poses an unacceptable risk to vision. Another limitation relates to selection bias: this study was conducted at a tertiary referral hospital clinic, and thus the percentage of patients who experienced severe visual impairment was probably higher than in the total population with ocular toxoplasmosis, since people with mild or no ocular symptoms would be unlikely to seek medical evaluation.
Our findings in this large patient group indicate that a significant percentage of eyes with ocular toxoplasmosis suffer vision loss, and suggest that particular clinical attention should be given to those with atypical manifestations of active disease, macular lesions and/or ocular complications, due to the increased risk of poor visual outcomes.
Materials and methods
All persons with the diagnosis of active or inactive ocular toxoplasmosis, who attended the Uveitis Clinic at Ribeirão Preto General Hospital (Ribeirão Preto, São Paulo, Brazil) consecutively from January 14th, 2015 to November 16th, 2017 were enrolled in this observational study. The research protocol followed the principles of the Declaration of Helsinki, and was approved by the Ethics Committee in Human Research at Ribeirão Preto General Hospital (approval number: 46015415.2.0000.5440). All subjects agreed to participate in the study and signed a consent form approved by the Committee; children were only included with the consent of their legal guardian.
Study subjects had a comprehensive ophthalmic examination, including measurement of best-corrected visual acuity, Goldmann applanation tonometry and dilated fundoscopy. Retinal lesions were photographed with either the Canon CR-2 non-mydriatic retinal camera (Melville, NY) or the Topcon TRC-50DX mydriatic retinal camera (Oakland, NJ), unless the ocular media were too densely opacified for clear imaging. Ocular toxoplasmosis was diagnosed by a uveitis-specialized ophthalmologist (JMF) based on the observation of active or inactive toxoplasmic retinal lesions, and the presence of serum immunoglobulin (Ig)M and/or IgG directed against T. gondii. In atypical presentations, intraocular fluid was tested for T. gondii DNA by PCR, and selected other investigations were ordered depending on the differential diagnosis. Serological testing for HIV was routinely performed.
Patients with active retinal lesions were treated with an oral course of either trimethoprim and sulfamethoxazole, or sulfadiazine and pyrimethamine, plus oral prednisone. In a small number of cases, when individuals were unable to use sulfamethoxazole and sulfadiazine, oral or intravitreal clindamycin was used. The patients were re-evaluated 14 days and 45–60 days after presentation, unless the clinical situation required more frequent assessment. Patients with inactive retinal lesions were followed on a case-by-case analysis.
Ocular toxoplasmosis was classified according to the form of presentation (primary active, recurrent active or inactive) and the mode of infection (congenital, acquired or unknown)10. Clinical information that was collected in addition to the descriptors of ocular toxoplasmosis included patient sex, age at recruitment and self-reported ethnicity.
Toxoplasmic retinal lesions were designated “active” when characterized by fluffy white retinitis and vitritis, with or without with retinal scars, and “inactive”, when characterized by well-defined atrophic retinochoroidal scar(s) without retinitis or vitritis2, 3. The lesions were described according to location (central retina [macular and non-macular, posterior pole] and peripheral retina), number and size, which was estimated by comparison to the optic disc (in disc-diameters). A presentation was considered “atypical” if there were multiple or extensive (greater than 10 disc-diameters in size) retinal lesions2. Ocular complications were recorded, including persistent vitreous opacities (present 3 months after resolution of active lesion(s)), raised intraocular pressure, glaucoma, posterior synechiae, cataract, epiretinal membrane, macular edema, macular hole, retinal tear, retinal detachment, retinal vascular occlusion, retinal and choroidal neovascularization, vitreous hemorrhage, optic atrophy and phthisis bulbi.
The descriptive results were presented as frequencies and percentages. The 95% CI were calculated for the estimated incidence rate of reactivation. Multivariate logistic regression was used to assess the risk factors associated with poor visual prognosis and reactivation of ocular toxoplasmosis. Statistical analyses were performed using R software (version 3.6.3; The R Foundation for Statistical Computing). A p-value of less than 0.05 was taken to indicate a significant difference.
References
Robert-Gangneux, F. & Dardé, M. L. Epidemiology of and diagnostic strategies for toxoplasmosis. Clin. Microbiol. Rev. 25, 264–296 (2012).
Holland, G. N. Ocular toxoplasmosis: A global reassessment. Part II: Disease manifestations and management. Am. J. Ophthalmol. 137, 1 (2004).
Butler, N. J., Furtado, J. M., Winthrop, K. L. & Smith, J. R. Ocular toxoplasmosis II: Clinical features, pathology and management. Clin. Exp. Ophthalmol. 41, 95–108 (2013).
Furtado, J. M., Winthrop, K. L., Butler, N. J. & Smith, J. R. Ocular toxoplasmosis I: Parasitology, epidemiology and public health. Clin. Exp. Ophthalmol. 41, 82–94 (2013).
Dubey, J. P., Lago, E. G., Gennari, S. M., Su, C. & Jones, J. L. Toxoplasmosis in humans and animals in Brazil: High prevalence, high burden of disease, and epidemiology. Parasitology 139, 1375–1424 (2012).
Gonzalez-Fernandez, D., Nascimento, H., Nascimento, C., Muccioli, C. & Belfort, R. Jr. Uveitis in Sao Paulo, Brazil: 1053 new patients in 15 months. Ocul. Immunol. Inflamm. 25, 382–387 (2017).
Schlaen, A. et al. Regional differences in the clinical manifestation of ocular toxoplasmosis between the center and northeast of Argentina. Ocul. Immunol. Inflamm. 27, 722–730 (2019).
Furtado, J. M. et al. Causes of blindness and visual impairment in Latin America. Surv. Ophthalmol. 57, 149–177 (2012).
de-la-Torre, A., González-López, G., Montoya-Gutiérrez, J. M., Marín-Arango, V. & Gómez-Marín, J. E. Quality of life assessment in ocular toxoplasmosis in a Colombian population. Ocul. Immunol. Inflamm. 19, 262–266 (2011).
Bosch-Driessen, L. E., Berendschot, T. T., Ongkosuwito, J. V. & Rothova, A. Ocular toxoplasmosis: Clinical features and prognosis of 154 patients. Ophthalmology 109, 869–878 (2002).
Aleixo, A. L., Curi, A. L., Benchimol, E. I. & Amendoeira, M. R. Toxoplasmic retinochoroiditis: Clinical characteristics and visual outcome in a prospective study. PLoS Negl. Trop. Dis. 10, e0004685 (2016).
Holland, G. N. et al. Analysis of recurrence patterns associated with toxoplasmic retinochoroiditis. Am. J. Ophthalmol. 145, 1007–1013 (2008).
Silveira, C. et al. The effect of long-term intermittent trimethoprim/sulfamethoxazole treatment on recurrences of toxoplasmic retinochoroiditis. Am. J. Ophthalmol. 134, 41–46 (2002).
Felix, J. P. et al. Trimethoprim-sulfamethoxazole versus placebo to reduce the risk of recurrences of Toxoplasma gondii retinochoroiditis: Randomized controlled clinical trial. Am. J. Ophthalmol. 157, 762-766.e761 (2014).
Felix, J. P. et al. Trimethoprim-sulfamethoxazole versus placebo in reducing the risk of toxoplasmic retinochoroiditis recurrences: A three-year follow-up. Am. J. Ophthalmol. 170, 176–182 (2016).
Felix, J. P. et al. Long-term results of trimethoprim-sulfamethoxazole versus placebo to reduce the risk of recurrent Toxoplasma gondii retinochoroiditis. Am. J. Ophthalmol. 213, 195–202 (2020).
Morais, F. B., Arantes, T. & Muccioli, C. Current practices in ocular toxoplasmosis: A survey of Brazilian uveitis specialists. Ocul. Immunol. Inflamm. 26, 317–323 (2018).
Acknowledgments
The authors wish to thank Ms. Janet Matthews for administrative support in the preparation of this manuscript.
Funding
This work was supported in part by grants from: São Paulo Research Foundation (FAPESP: 2017/06680–4 to MA); Australian Research Council (FT130101648 to JRS); National Council for Scientific and Technological Development (CNPq: 400167/2016–6 to JMF); and Foundation for Support of Teaching, Research & Assistance of the Clinical Hospital, Faculty of Medicine of Ribeirão Preto—University of São Paulo (FAEPA: 1901/2017 to JMF).
Author information
Authors and Affiliations
Contributions
J.R.S. and J.M.F. designed the research, performed the analysis, drafted and revised the manuscript. R.B.Jr. designed the research and revised the manuscript. DMG performed the statistical analysis and revised the manuscript. SA, BRV, MWR, RM, MA and MS collected and collated the data and revised the manuscript. All authors have given approval to the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Arruda, S., Vieira, B.R., Garcia, D.M. et al. Clinical manifestations and visual outcomes associated with ocular toxoplasmosis in a Brazilian population. Sci Rep 11, 3137 (2021). https://doi.org/10.1038/s41598-021-82830-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-82830-z
- Springer Nature Limited
This article is cited by
-
Outcomes of trimethoprim/ sulfamethoxazole treatment for ocular toxoplasmosis in Congolese patients
BMC Ophthalmology (2023)
-
Modulation of CXCL10 activity as a therapeutic target of ocular toxoplasmosis in diabetic mice
Journal of Parasitic Diseases (2023)
-
Posterior segment findings by spectral-domain optical coherence tomography and clinical associations in active toxoplasmic retinochoroiditis
Scientific Reports (2022)