
Abstract
This study was to investigate the correlation of vagal activity with coronary artery lesion (CAL) in Kawasaki disease (KD) children, and assess the predictive value of heart rate deceleration capacity (DC) for CAL in acute phase of KD.50 KD children with CAL, 130 KD children without CAL, 30 children with acute upper respiratory infection and 100 healthy children were recruited and indicators reflecting vagal activity including DC were measstuogram. KD children with CAL showed decreased vagal activity with significantly lower values of DC. DC was negatively correlated with levels of N-terminal pro-brain natriuretic peptide (NT-proBNP) and C-reactive protein (CRP) in KD children. DC was a usable cardiac electrophysiological index to predict CAL in children with KD, with an area under the receiver operating characteristic curve (AUC) of 0.741. The cut-off value of DC for predicting CAL in KD children was 4.37 ms. DC was an independent predictor of CAL in children with KD, evaluated by multiple logistic regression analysis, KD children with DC ≤ 4.37 ms had an increased risk of CAL, with odds ratios (OR) of 5.94. Our study illustrates DC could be used to predict CAL in acute phase of KD.
Similar content being viewed by others

Introduction
Kawasaki disease (KD) is an acute febrile systemic vasculitis syndrome, which is one of the most common acquired heart disease in children1. Coronary artery lesion (CAL) as one of the most serious complications, which could result in coronary artery aneurysm, even myocardial infarction and sudden death, that cause serious damage to children’s health, occurs in 25% of untreated children with KD2,3,4. Studies have shown that some biochemical indicators are associated with CAL in KD, but there are relatively few reliable indicators for predicting CAL in the acute phase of disease5,6,7,8.
Heart rate variability (HRV) reflects beat-to-beat changes in RR intervals, which is a traditional, non-invasive method detecting autonomic nervous function. Root mean squared successive difference (rMSSD), percentage of successive normal sinus RR intervals >50 ms (PNN50) belongs to the time–domain variables of HRV, high frequency (HF) belongs to the frequency domain variable of HRV, low values for these indicators indicate hypoactivity of the vagal nerve9,10,11. Decreased vagal activity has been found in patients with coronary artery disease in adults by HRV analysis, which is closely related to the prognosis and the severity of CAL12,13,14. Since HRV method cannot accurately distinguish between the vagal and sympathetic activities of the autonomic nervous system, Heart rate deceleration capacity (DC) as a new indicator, which reflects the general trend of sinus rhythm RR interval and its ability to decelerate, has been discovered that can more accurately and quantitatively evaluate vagal activity and has a better warning ability of adverse cardiac events than HRV15,16,17,18. In this study, we aimed to investigate the correlation of vagal activity with CAL in KD children, and assess the predictive value of DC for CAL in acute phase of KD.
Material and Methods
Study subjects
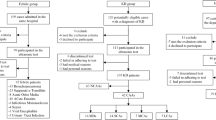
Between June 2017 and June 2019,180 children with KD treated at Chengdu Women’s and Children’s Central Hospital, School of Medicine, University of Electronic Science and Technology of China(UESTC) were recruited. 50 cases of KD children with CAL–30 boys and 20 girls, aged from 7 to 49 months old–were assigned into KD-CAL group, while 130 KD cases of KD children without CAL–80 boys and 50 girls, aged from 7 to 61 months old–were assigned into KD-NCAL group. The diagnosis of KD was established according to the American Heart Association guideline in 201719. The echocardiography was performed by a pediatric cardiologist to detect CAL within 30 days after onset of kawasaki disease, at the peak period for CAL20. CAL was defined as a coronary artery internal dimeter with a z score of ≥2.5 in at least one of the following coronary arteries: right, left anterior descending, and left main21. 100 healthy children– 65 boys and 35 girls, aged from 7 to 51 months old– were recruited as control group. 30 cases of children with fever due to acute upper respiratory tract infection (AURI) –16 boys and 14 girls, aged from 10 to 52 months old–were recruited into AURI group.
Excluded from this study were children with the following conditions: presence of non-sinus rhythm (eg, atrial fibrillation, atrial flutter, sick sinus syndrome or atrioventricular block); complicated with other diseases affecting the autonomic nerve function (eg, hyperthyroidism, anemia, or suffocation); using medications that may affect HRV(eg, cardiotonic, antagonists of the renin-angiotensin system, vasodilators, beta-adrenergic antagonists, neuroleptics, antidepressants, antihistamines, anaesthetic, hormones); other organic heart disease.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Ethics Committee of Chengdu Women’s and Children’s Central Hospital, School of Medicine, UESTC and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from guardians of all individual participants included in the study.
Dynamic electrocardiogram examination
Children with KD received a 24-hour dynamic electrocardiogram examination after the diagnosis and before intravenous immunoglobulins (IVIG) therapy. Other children were examined within 24 hours after enrollment. The recorded data were analyzed using an offline DMS dynamic electrocardiogram analysis system (DM Software, Stateline, NV, USA). DC and indicators of heart rate variability associated with vagal activity PNN50, rMSSD and HF were calculated automatically.
Plasma NT-proBNP, CRP detection
Fasting peripheral venous blood 3 ml was drawn in all children except the healthy controls on the next morning after enrollment. The blood samples were collected in EDTA anti-coagulant tubes, then the plasma was segregated for detection. The N-terminal pro-brain natriuretic peptide (NT-proBNP) was detected using Nano-Checker 710 immunochromatographic detector (Nano-Ditech Corporation, USA). The normal value of NT-proBNP is 0~500 pg/ml. The C-reactive protein (CRP) was detected using QuikRead CRP quantitative analyzer (Orion Diagnostica company, Finland). The normal value of CRP is 0~1 mg/dL.
Statistical analysis
Data was analyzed using SPSS version 19.0 software (IBM Corporation, Armonk, NY, USA). We used the Shapiro-Wilks test to check the distribution of variables and the Levene test to check homogeneity of variances. Because of the non-normal distribution and heterogeneity of variance of some measures, data were presented as the median with the interquartile range for continuous variables. Comparisons among groups were evaluated using the Kruskal-Wallis test, while the two groups were compared by the Mann-Whitney U test. χ2 tests were performed to compare categorical variables. All tests were performed as two-sided, the value of P < 0.05 was considered to indicate statistical significance. Spearman’s partial correlation was used to assess correlations between variables. To evaluate the performance of different indicators in discriminating CAL in KD, KD children with and without CAL were pooled, the area under the receiver operating characteristic curve (AUC) analysis was performed. The sensitivity and specificity were calculated, and the cutoff value was determined by the Youden index. Multivariate logistic regression was used to identify the independent predictor of CAL in KD children.
Results
Comparison of baseline characteristics among groups
Table 1 shows the differences of baseline characteristics among different groups. There were no significant differences in age (P = 0.250) and gender ratio (P = 0.703) among the groups. The values of DC, PNN50, RMSSD and HF were significantly lower in KD-NCAL group compared with the control group (all P < 0.001). The values of DC (P = 0.021), PNN50 (P = 0.016), and HF (P < 0.001) were also lower in AURI group than the control group, while rMSSD was not different. There were no significant differences on the values of DC (P = 0.683), PNN50 (P = 0.268), RMSSD (P = 0.169) and HF (P = 0.188) between AURI group and KD-NCAL group. However, The values of DC (P < 0.001), PNN50 (P = 0.001), RMSSD (P = 0.027) and HF (P = 0.008) were lower in KD-CAL group compared with AURI group, and were also significantly lower than the control group and (all P < 0.001). The values of DC (P < 0.001), PNN50 (P = 0.001) in KD-CAL group were lower than KD-NCAL group, but RMSSD (P = 0.120), HF (P = 0.056) were not different between the two groups. The levels of plasma NT-proBNP and CRP were significantly different across different groups with the following rank order: KD-CAL group> KD-NCAL group > AURI group (all P < 0.001). Spearman’s partial correlation showed that both DC and PNN50 negatively correlated with NT-proBNP (r = −0.883, −0.430, P < 0.001), and CRP (r = −0.846, −0.377, P < 0.001).
ROC analysis of using different indicators to predict CAL in children with KD
The ROC curves of using DC, PNN50, NT-proBNP and CRP to predict CAL in children with KD were analyzed (Fig. 1; Table 2). AUCs corresponding to DC and NT-proBNP, which may be used to predict CAL in children with KD, were demonstrated to be relatively higher (0.741 and 0.744, respectively) compared with PNN50 and CRP. By contrast, the sensitivities of NT-proBNP were revealed to be higher, with values of 82.00% at its cutoff points at 684 pg/ml, compared with that of 66.00, 44.00 and 66.00% for DC, PNN50, and CRP at their classical cutoff points at 4.37 ms, 1%, 5.3 mg/dl, respectively. In comparison, the specificity of DC was determined to be high, with a value of 83.08% at its classical cutoff point, compared with that of 78.46%, 64.62%, 77.69% for PNN50, NT-proBNP, and CRP respectively.

Receiver operating characteristic curves using DC, PNN50, NT-proBNP and CRP to predict CAL in children with KD. CAL, coronary artery lesion; KD, kawasaki disease DC, heart rate deceleration capacity; PNN50, percentage of successive normal sinus RR intervals >50 ms; NT-proBNP, N-terminal pro-brain natriuretic peptide; CRP, C-reactive protein.
Logistic regression analysis of Kawasaki disease with CAL
Using DC ≤ 4.37 ms, PNN50 ≤ 1%, NT-proBNP > 684 pg/ml and CRP > 5.3 mg/dl as binary independent variable, multivariate Logistic regression for CAL in acute phase of Kawasaki disease was analyzed is presented in Table 3.The results showed that DC ≤ 4.37 ms (P = 0.024) and NT-proBNP > 684 pg/ml (P = 0.032) are independent predictors of CAL in KD children.
Discussion
Previous studies have found that decreased vagal activity assessed by HRV analysis is associated with myocardial infarction developed from giant coronary artery aneurysm in KD22. However, there are few studies on the relationship between vagal activity and CAL in KD. In our study, the recruited KD children were in the acute phase and had fever. Studies have shown that fever can cause a decrease in vagal activity23,24, so in addition to the healthy control, children with fever due to AURI were set as the febrile control. In this study, we observed that DC, PNN50 and HF in AURI children and KD children with or without CAL were significantly reduced compared with the healthy children, indicating that vagal activity was decreased in febrile children. Besides, we found DC, PNN50, RMSSD and HF were not significantly different between AURI children and KD children without CAL, indicating that there was no difference in vagal activity between children with different febrile illness. Vagal activity measurements may not be applicable to the discrimination of febrile diseases such as AURI and KD. Nevertheless, we still found that DC, PNN50, rMSSD and HF were lower in KD children with CAL compared with AURI children. DC and PNN50 in KD children with CAL were also lower than those without CAL, though no statistical differences were found in RMSSD and HF between the two groups. It suggests that decreased vagal activity may be associated with CAL in KD children, DC and PNN50 may be more reliable in KD children for the assessment of vagal activity compared with RMSSD, HF.
Exaggerated inflammation in the acute phase that leads to dysfunction of vascular endothelial cells is an important mechanism for the occurrence of CAL25. NT-proBNP is an important cardiac biomarker that associated with ventricular myocyte ischemia and hypoxia26. CRP is a pentameric protein that is present in the bloodstream during inflammatory events, can reflect the severity of inflammation27. Studies have confirmed that levels of NT-proBNP and CRP exist a positive correlation with CAL in KD5,6. Recent studies have found that increased vagal activity can reduce the levels of inflammatory factors by activating the “cholinergic anti-inflammatory pathway”, so as to improve endothelial dysfunction28,29. In animal and human studies, levels of NT-proBNP and CRP were decreased in response to vagus nerve stimulation30,31,32,33. In our study, compared to KD-CAL group, relatively higher values of DC and PNN50, lower levels of NT-proBNP and CRP were found in KD-NCAL group. This indicated that KD children without CAL had higher vagal activity and a relatively lower level of inflammation compared with KD children with CAL. At the same time, correlation study showed that DC and PNN50 were negatively correlated with levels of plasma NT-proBNP and CRP in KD children. It is speculated that increasing vagal activity in KD children could be a way of protection of the coronary artery by reducing the production of inflammatory factors.
In the present study, DC cutoff value of 4.37 ms yielded sensitivity of 66.00% and specificity of 83.08% for predicting CAL, KD children with DC ≤ 4.37 ms (OR = 3.275) had an increased risk of CAL. In adults, it has been demonstrated that DC < 2.5 ms is significantly related to a higher risk of death after myocardial infarction, while DC > 4.5 ms is related to a lower risk16,34. Wei Hu’s research found that DC was an independent risk factor for heart failure, with cutoff values of 4.55 ms in males and 4.85 ms in females35. Although the cutoff values of DC are varied from study to study in different prediction events, these studies suggest that DC is a useful prognostic tool for risk stratification in cardiovascular diseases. NT-proBNP is also a strong predictor of CAL in KD children. Kaneko et al. reported that the NT-proBNP cutoff value of 1000 pg/ml yielded sensitivity of 68% and specificity of 83% for predicting CAL8. Yoshimura et al. indicated that a cutoff value of 1300 pg/ml to predict CAL produced specificity of 95% and sensitivity of 85%36. In our study, the cutoff value was 684 pg/ml, which yielded sensitivity of 82.00% and specificity of 64.62%. The relatively lower value of NT-proBNP in our study may have occurred because we performed the test during the acute phase of KD. KD children with NT-proBNP >684 pg/ml (OR = 2.968) had a higher risk of CAL. The odds ratio of NT-proBNP is lower compared with that of DC. It is suggested that the relevance of DC and CAL is stronger compared with NT-proBNP.
This study has some limitations. First, the sample size of this study is small. Large-scale, multicenter prospective studies are needed to confirm our findings. Second, we excluded patients with non-sinus rhythm in this study. Therefore, our findings may not be directly generalized to these patients. Third, temperature fluctuations have an effect on vagal activity. HRV and DC after body core temperature correction were more reliable in studying the correlation between vagal activity and CAL in KD. Unfortunately, we did not have the equipment for continuous monitoring of body temperature and dynamic electrocardiogram at the same time.
In conclusion, decreased vagal activity may be associated with CAL in KD children, the DC would provide an insight into the disease severity and could be used as an independent predictor for the risk of CAL in acute phase of KD.
References
Wood, L. E. & Tulloh, R. M. R. Kawasaki disease in children. Heart 95, 787–92 (2009).
Kuo, H. C. Preventing coronary artery lesions in kawasaki disease. Biomed J. 40, 141–46 (2017).
Duan, C., Du, Z. D., Wang, Y. & Jia, L. Q. Effect of pravastatin on endothelial dysfunction in children with medium to giant coronary aneurysms due to kawasaki disease. World J Pediatr 10, 232–237 (2014).
Holve, T. J. et al. Long-term cardiovascular outcomes in survivors of kawasaki disease. Pediatrics 133, e305–11 (2014).
Min, K. K., Min, S. S. & Gi, B. K. F. Factors predicting resistance to intravenous immunoglobulin treatment and coronary artery lesion in patients with kawasaki disease: analysis of the korean nationwide multicenter survey from 2012 to 2014. Korean Circ J 48, 71–9 (2018).
Jun, H. et al. Age-adjusted plasma N-terminal pro-brain natriuretic peptide level in kawasaki disease. Korean J Pediatr 59, 298–302 (2016).
Kobayashi, T. et al. Prediction of intravenous immunoglobulin unresponsiveness in patients with kawasaki disease. Circulation 113, 2606–12 (2006).
Kaneko, K. et al. Prediction of the risk of coronary arterial lesions in kawasaki disease by brain natriuretic peptide. Pediatr Cardiol 32, 1106–9 (2011).
Ewing, D. J., Borsey, D. Q., Bellavere, F. & Clarke, B. F. Cardiac autonomic neuropathy in diabetes: comparison of measures of R-R interval variation. Diabetologia 21, 18–24 (1981).
Paiva, V. C. et al. Comparison of assessment methods of cardiac vagal modulation. Arq Bras Cardiol 97, 493–501 (2011).
Bigger, J. T., Fleiss, J. L., Rolnitzky, L. M. & Steinman, R. C. Frequency domain measures of heart period variability to assess risk late after myocardial infarction. J Am Coll Cardiol 21, 729–36 (1993).
Yıldız, B. S. et al. Evaluation of heart rate variability in patients with coronary artery ectasia and coronary artery disease. Turk Kardiyol Dern Ars 44, 306–314 (2016).
Wennerblom, B., Lurje, L., Tygesen, H., Vahisalo, R. & Hjalmarson, A. Patients with uncomplicated coronary artery disease have reduced heart rate variability mainly affecting vagal tone. Heart 83, 290–4 (2000).
Li, H. R. et al. Additive value of heart rate variability in predicting obstructive coronary artery disease beyond framingham risk. Circ J 80, 494–501 (2016).
Hamm, W. et al. Deceleration capacity of heart rate after acute altitude exposure. High Alt Med Biol 19, 299–302 (2018).
Bauer, A. et al. Deceleration capacity of heart rate as a predictor of mortality after myocardial infarction: cohort study. Lancet 367, 1674–81 (2006).
Pan, Q. et al. The degree of heart rate asymmetry is crucial for the validity of the deceleration and acceleration capacity indices of heart rate: a model-based study. Comput Biol Med 76, 39–49 (2016).
Guzik, P. et al. Heart rate deceleration runs for postinfarction risk prediction. J Electrocardiol 45, 70–6 (2012).
McCrindle, B. W. et al. Diagnosis, treatment, and long-term management of kawasaki disease: a scientific statement for health professionals from the american heart association. Circulation 135, e927–99 (2017).
Burns, J. C. & Matsubara, T. New insights into cardiovascular disease in patients with kawasaki disease. Curr Opin Pediatr 30, 623–27 (2018).
McCrindle, B. W. et al. Coronary artery involvement in children with kawasaki disease: risk factors from analysis of serial normalized measurements. Circulation 116, 174–9 (2007).
Kikuchi, Y., Sato, Y., Ichihashi, K., Shiraishi, H. & Momoi, M. Y. Autonomic function in kawasaki disease with myocardial infarction: usefulness of monitoring heart rate variability. Pediatr Int 45, 407–9 (2003).
Kinugasa, H. & Hirayanagi, K. Effects of skin surface cooling and heating on autonomic nervous activity and baroreflex sensitivity in humans. Exp Physiol 84, 369–77 (1999).
Massaro, A. N. et al. Effect of temperature on heart rate variability in neonatal ICU patients with hypoxic-ischemic encephalopathy. Pediatr Crit Care Med 18, 349–54 (2017).
Agarwal, S. & Agrawal, D. K. Kawasaki disease: etiopathogenesis and novel treatment strategies. Expert Rev Clin Immunol 13, 247–258 (2017).
Heck, P. B., Müller, J., Weber, R. & Hager, A. Value of N-terminal pro-brain natriuretic peptide levels in different types of fontan circulation. Eur J Heart Fail 15, 644–49 (2013).
Hwang, J., Seo, Y., Jo, Y., Son, J. & Choi, J. Aptamer-conjugated live human immune cell based biosensors for the accurate detection of c-reactive protein. Sci Rep 6, 34778 (2016).
Zhao, M. et al. Vagal stimulation triggers peripheral vascular protection through the cholinergic anti-inflammatory pathway in a rat model of myocardial ischemia/reperfusion. Basic Res Cardiol 108, 345 (2013).
Moser, M. et al. Investigation of a micro-test for circulatory autonomic nervous aystem responses. Front Physiol 21, 448 (2017).
Lorgis, L. et al. High N-terminal pro-B-type natriuretic peptide levels are associated with reduced heart rate variability in acute myocardial infarction. PLoS ONE 7, e44677 (2012).
Rauchenzauner, M. et al. N-terminal pro-brain natriuretic peptide (NT-proBNP) release in children with vagus nerve stimulation. A prospective case series. J Neurol 255, 980–5 (2008).
Yu, H. et al. Chronic vagus nerve stimulation improves left ventricular function in a canine model of chronic mitral regurgitation. J Transl Med 12, 302 (2014).
Sloan, R. P. et al. RR interval variability is inversely related to inflammatory markers: the CARDIA study. Mol Med Camb Mass 13, 178–84 (2007).
Rizas, K. D. et al. Bedside autonomic risk stratification after myocardial infarction by means of short-term deceleration capacity of heart rate. Europace 20, f129–36 (2018).
Hu, W. et al. Deceleration and acceleration capacities of heart rate associated with heart failure with high discriminating performance. Sci Rep 6, 23617 (2016).
Yoshimura, K. et al. N-terminal pro-brain natriuretic peptide and risk of coronary artery lesions and resistance to intravenous immunoglobulin in kawasaki disease. J Pediatr 162, 1205–9 (2013).
Acknowledgements
This study was funded by the Municipal Planning Commission of Science and Research Fund in Sichuan, China (17PJ270). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
Yaheng Lu and Xianmin Wang. designed the research. Mei Jin performed Echocardiography. Tingting Chen, Yonghong Guo and Yizhou Wen collected the data, Yaheng Lu analyzed the data. Yaheng Lu, Feifei Si, Xianmin Wang wrote and edited the paper. All authors approved the final version.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Lu, Y., Guo, Y., Si, F. et al. Predictive value of heart rate deceleration capacity on coronary artery lesion in acute phase of Kawasaki disease. Sci Rep 10, 10211 (2020). https://doi.org/10.1038/s41598-020-67121-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-67121-3
- Springer Nature Limited