
Abstract
Neuroprotective treatments in ischemic stroke are focused to reduce the pernicious effect of excitotoxicity, oxidative stress and inflammation. However, those cellular and molecular mechanisms may also have beneficial effects, especially during the late stages of the ischemic stroke. The objective of this study was to investigate the relationship between the clinical improvement of ischemic stroke patients and the time-dependent excitotoxicity and inflammation. We included 4295 ischemic stroke patients in a retrospective study. The main outcomes were intra and extra-hospital improvement. High glutamate and IL-6 levels at 24 hours were associated with a worse intra-hospital improvement (OR:0.993, 95%CI: 0.990–0.996 and OR:0.990, 95%CI: 0.985–0.995). High glutamate and IL-6 levels at 24 hours were associated with better extra-hospital improvement (OR:1.13 95%CI, 1.07–1.12 and OR:1.14, 95%CI, 1.09–1.18). Effective reperfusion after recanalization showed the best clinical outcome. However, the long term recovery is less marked in patients with an effective reperfusion. The variations of glutamate and IL6 levels in the first 24 hours clearly showed a relationship between the molecular components of the ischemic cascade and the clinical outcome of patients. Our findings suggest that the rapid reperfusion after recanalization treatment blocks the molecular response to ischemia that is associated with restorative processes.
Similar content being viewed by others


Introduction
The ischemic cascade is a complex molecular and cellular process that is triggered immediately after an ischemic stroke (IS). During this process, several mechanisms are developed sequentially as a consequence of the deprivation of blood and oxygen supply to the ischemic core1,2,3,4,5,6,7. Neuroprotective treatments in acute IS are mainly focused to reduce the pernicious effect of excitotoxicity, oxidative-nitrosative stress, and inflammation7,8, however, these cellular and molecular mechanisms could also have reparative and beneficial effects for the patients. The reduction of glutamate concentration in the synaptic cleft has been the target of several clinical trials using antagonists of glutamate N-methyl-D-aspartate receptors to alleviate excitotoxicity, however those trials have failed to show clinical efficacy8,9. Targeting glutamate receptors can also block the synaptic transmission, and even though it could protect from glutamate excitotoxicity, it could also hinder the promotion of neuronal survival and cerebral plasticity in the late phase of IS9. Inflammation can also amplify the ischemic lesion and a considerable number of clinical trials were designed to target the inflammatory response10. Nonetheless, it is now clear that inflammation also promotes critical events necessary for tissue repair during the late stages of the IS11.
Recanalization treatments aimed to achieve reperfusion, either with the tissue Plasminogen Activator (tPA) or by mechanical thrombectomy, are the only treatments that have shown clinical benefit in IS, with a better clinical outcome observed in patients treated with recanalization therapies compared with untreated patients, both at short and long term12,13,14,15. Preclinical studies have shown that reperfusion could also modify the molecular profile of the ischemic cascade1,16,17,18, although the clinical implications of these findings are yet to be proven. In addition, reperfusion is associated with detrimental side effects. For instance, the potential toxic effect of tPA has been demonstrated in patients who did not reperfuse after the recanalization treatment19,20. Reperfusion is also associated with secondary damage due to oxidative stress8,21, although its repercussion on the clinical evolution of patients has not been demonstrated.
The clinical benefits of reperfusion are limited by several factors, including its narrow therapeutic window, the topography of the vascular occlusion and the type of thrombus, as well as by other factors related to the patients, such as age and the hemodynamic situations. The risks associated with reperfusion therapies require the best possible selection of patients amenable to recanalization therapies. Since recanalization treatment is known to modify the patient’s outcome, in this work we studied the improvement of patients in relation with the success of the recanalization treatment, both at short term or intra-hospital improvement (patient improvement between admission and discharge) and at long term or extra-hospital improvement (patient improvement between discharge and 3 months afterwards). We also evaluated the relation between patient improvement with the time-dependent excitotoxic and/or inflammatory mechanisms. The aim of the present study was to evaluate whether the levels of glutamate, IL6 and the reperfusion have a direct influence in the intra-hospital and extra-hospital improvement, in patients with IS.
Results
The IS patients included in the analysis were classified into 3 groups: patients who did not receive recanalization treatment (PNR); patients with recanalization treatment and effective reperfusion (PER) and patients with recanalization treatment and uneffective reperfusion (PWER). The results are summarized in Table 1, including clinical and analytical variables.
The selection criteria of patients for recanalization partially determined the statistical differences between the groups. In this regard, PER showed the highest clinical improvement, and the benefit persists during the first three months after the treatment (mRS at 3 months: 0[0,1] for PER vs 2[1,3] for PNR and 1[0,3] for PWER. p < 0.0001).
The NIHSS at hospital discharge was significantly higher for PWER compared to PNR and PER (12[10,16], 6[3,12] and 1[0,4]. p < 0.0001). Regarding the intra-hospital improvement, it was much higher for PER compared with PNR and PWER (45.9 ± 12.8, 9.1 ± 10.1 and 3.9 ± 17.2, p < 0.0001). However, this trend was different for the extra-hospital improvement, with the highest values observed in PNR, followed by PWER and PER (11.7 ± 10.8, 5.0 ± 8.3 and 0.5 ± 2.9, p < 0.0001).
Intra-hospital improvement
Intra-hospital improvement was defined as a positive value of the NIHSS scale on admission minus the value of the NIHSS scale at discharge. Among the total sample (4295 patients), 1176 patients (27.4%) did not show any improvement during hospitalization, including 398 deaths, while 3119 patients (72.6%) showed an improvement of at least 1 point in the NIHSS between admission and discharge. It can be seen (Table 2) that intra-hospital improvement is a good marker for good outcome at 3 months, defined as mRS values ≤2 (59.6% for patients with intra-hospital improvement and 31.9% for patients without intra-hospital improvement, p < 0.0001). Intra-hospital improvement was also related with lower values of markers associated with acute inflammatory response, such as temperature (36.3 ± 0.6 °C vs 36.5 ± 0.7 °C, p < 0.0001), leukocytes (9.2 ± 3.1 × 103 mL vs 9.7 ± 3.1×103 mL, p < 0.0001), fibrinogen (444.7 ± 95.5 mg/dL vs 447.0 ± 104.2 mg/dL, p = 0.004), C-reactive protein (2.8 ± 3.5 mg/L vs 3.9 ± 4.5 mg/L, p < 0.0001) and sedimentation rate (25.4 ± 22.6 mm vs 25.7 ± 23.0 mm, p = 0.003).
The type of recanalization treatment did not influence the intra-hospital improvement (Table S1, p = 0.064), but intra-hospital improvement was more frequent in PER compared with PWER (10.9% vs 9.2%, p < 0.0001).
The data was also analyzed in a logistic regression model (Table S1), using the intra-hospital improvement as the dependent variable and the relationship of effective reperfusion therapy with intra-hospital improvement was confirmed (OR: 38.13, 95%CI: 5.26–276.64; p < 0.0001). Likewise, an ineffective reperfusion therapy was associated with a negative intra-hospital evolution (OR: 0.26, 95%CI: 0.19–0.35; p < 0.0001).
Extra-hospital improvement
Extra-hospital improvement was defined as a positive value of the NIHSS scale at discharge minus the value of the NIHSS scale at three months. Extra-hospital improvement was analyzed in 3853 patients (Table 3). Among those patients, 1326 (34.4%) did not show extra-hospital improvement while 2527 (65.6%) showed an improvement of at least 1 point in the NIHSS 3 ± 1 months after the hospital discharge. A bivariate analysis was carried out classifying the patients into two groups depending on the presence or absence of extra-hospital improvement (Table 3), and it was observed that the extra-hospital improvement was not related with a good outcome at 3 months, defined as mRS values ≤2 (64.9% vs 60.5%, p = 0.051). Extra-hospital improvement was associated with higher values of inflammatory markers (leukocytes 8.7 ± 3.1×103 mL vs 9.4 ± 3.1 × 103 mL, p = 0.001; fibrinogen 437.6 ± 94.9 mg/dL vs 445.3 ± 98.6 mg/dL, p = 0.002; and sedimentation rate 23.2 ± 23.6 mm vs 26.5 ± 22.8 mm, p < 0.0001). Also, extra-hospital improvement was higher in patients with more serious infarcts (infarct volume 40.8 ± 69.1 mL vs 11.2 ± 31.3 mL, p < 0.0001). The type of reperfusion treatment did not influence the extra-hospital improvement, however, it was less frequent in PER (2.7%) compared with PNR (79.7%) and with PWER (17.6%).
A logistic regression analysis was carried out using the extra-hospital improvement as a dependent variable (Table S2), showing that extra-hospital improvement is significantly negative in PER (OR:0.02, 95%CI: 0.01–0.03, p < 0.0001).
Molecular mechanisms (excitotoxicity and inflammation) associated with intra and extra-hospital improvement
In order to evaluate the influence of excitotoxicity and inflammation on the intra and extra-hospital improvement, an analysis of glutamate and IL6 levels was carried out in patients on admission and after 24 h (Table S3). Serum glutamate levels decreased significantly in the first 24 hours for the three groups of patients, although this decrease was more pronounced in PER (Fig. 1). The difference between the glutamate levels on admission in the three groups of patients is attributed to the selection criteria of patients for reperfusion treatments, the onset-inclusion time and the severity of the neurological deficit (both listed in Table S3), demonstrated by the correlations between the NIHSS and the glutamate levels on admission in the three groups of patients.

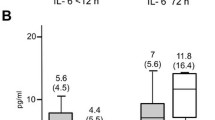
Mean concentrations of Glutamate (left) and IL6 (right) concentrations on admission and at 24 hours in PER, PNR and PWER.
Serum IL6 levels on admission were similar for the three groups of patients, however, IL6 levels were significantly higher in PNR and PWER at 24 hours compared with PER. Moreover, only PER showed a decrease in IL6 levels after 24 h.
Glutamate levels on admission were related with a worse intra-hospital evolution (OR:0.996, 95%CI: 0.995–0.998, p < 0.0001); however, this relationship was not demonstrated for basal IL-6 levels (OR:1.005, 95%CI: 0.996–1.0014, p = 0.292). After 24 hours, both glutamate and IL6 levels correlated with a worse intra-hospital evolution (OR:0.993, 95%CI: 0.990–0.996, p < 0.0001 and OR:0.990, 95%CI: 0.985–0.995, p < 0.0001 respectivelly) (Table S4). These results are consistent with a large number of publications that justify the use of drugs to reduce excessive excitotoxic and inflammatory response in IS22,23.
Surprisingly, and opposed to the trend observed for intra-hospital improvement, the extra-hospital improvement (Table S5) was associated with higher glutamate and IL6 levels determined at 24 h (OR:1.132, 95%CI, 1.072–1.196, p < 0.0001 and OR:1.137, 95%CI, 1.094–1.183, p < 0.0001).
The association of glutamate and IL6 levels with intra and extra-hospital improvement was further confirmed using a multiple linear regression analysis (Table S6). Glutamate levels on admission were correlated with positive intra and extrahospital improvement (β:0.025, p = 0.017 and β:0.019, p = 0.002 respectively), however, there was a negative correlation of high glutamate levels at 24 hours and intrahospital improvement (β −0.042, p = 0.046). Regarding IL6, high levels of this marker on admission had a negative correlation with extrahospital improvement (β −0.305, p < 0.0001), while high levels of IL6 at 24 hours correlates with a negative intrahospital improvement and a positive extrahospital improvement (β: −0.121, p < 0.0001 vs β: 0.131, p < 0.0001). These analyses showed the association between glutamate and IL6 and are further discussed below.
Discussion
To the best of our knowledge, this is the first study aimed to analyse the early (intra-hospital) and late (extra-hospital) evolutionary outcome of IS patients in relation to the recanalization treatment.
Recanalization treatments have demonstrated high survival rates and good outcome in clinical trials13,14,15. In our study, we also observed the best clinical outcome in patients with effective reperfusion as a response to the most appropriate recanalizing treatment, both at the time of hospital discharge and after 3 months. Indeed, the multivariate analysis demonstrates that early improvement is 38 times more frequent in patients with effective reperfusion compared with patients without recanalization treatment. Patients who received an uneffective recanalization treatment were the ones with the worst clinical situation. These results are in agreement with other clinical studies, as it is now recognized that effective reperfusion is an accurate indicator for clinical outcome in IS patients24,25.
The main factors independently associated with a negative intra-hospital evolution are hyperthermia, infarct volume and especially the uneffective reperfusion. However, effective reperfusion is related to worst extra-hospital improvement. Logically, the extra-hospital evolution is greater in patients who present a higher NIHSS at discharge, and therefore, the margin for improvement is lower for PER (Fig. 2). However, we hypothesize that the effective early reperfusion could also hinder neuroprotective molecular mechanisms. Although this hypothesis cannot be demonstrated in this study, the variations in glutamate and IL6 levels in the first 24 hours clearly show a relationship between the molecular components of the ischemic cascade and the clinical outcome of patients after 3 months, as discussed next.

Variation of the NIHSS on admission, at discharge and 3 months after hospitalization in PER, PNR and PWER.
Serum glutamate levels on admission are related to the stroke severity, and high levels of glutamate at and 24 h after admission were independently associated with a worse intra-hospital evolution. This is in agreement with previous studies26,27, although the clinical significance of these findings is rather low taking into account the nature of these variables and its units. Surprisingly, we observed an association between high glutamate levels at 24 hours and better extra-hospital evolution, and we determined that high glutamate levels at 24 hours are independently associated with an 11% better extra-hospital improvement, with both statistical and clinical significance. These observations suggested that the intense reduction of glutamate in the first 24 hours may be a factor that leads to a lower late recovery after an effective reperfusion (Fig. 3).

Correlation between the glutamate levels on admission and after 24 hours and the intra-hospital and extra-hospital improvement.
The inflammatory response has also been associated with early clinical deterioration28,29, and a worse prognosis after IS30. In our study, the inflammatory response was similar in the three groups of patients at admission; however we found significant differences on IL6 levels in serum at 24 h. IL6 levels significantly increased after 24 hours in PNR and PWER, but decreased in PER. Similar to the trend observed with glutamate, high levels of IL6 at 24 hours are independently associated with a worse intra-hospital evolution, but also with an 11% increase in extra-hospital improvement. A reduction in IL6 levels after 24 hours is another factor correlated with a worse extra-hospital improvement in IS patients (Fig. 4).

Correlation between the IL6 levels on admission and after 24 hours and the intra-hospital and extra-hospital improvement.
This is a retrospective and single-center study. However, the study comprises a large and unbiased sample (5306 patients) for the purposes of this analysis. The use of a clinical criterion to define effective reperfusion could lead to a bias in the classification in therapeutic response groups. The Doppler and MR angiography study after recanalization treatment was limited to a small group of patients. The narrow therapeutic margin available for patients with good therapeutic response could reduce the benefits in this group of patients; however, to avoid this effect we used the percentage deviation, not absolute, between the score of the NIHSS at discharge and at 3 months. The 3-month follow-up time is probably too short to evaluate the long-term effects. We have made an analysis in a subgroup of 287 patients that we have followed for a year, and the results were similar (data not shown).
Conclusions
Effective reperfusion after recanalization treatments provided the best clinical outcome for IS patients. However, this clinical improvement is usually achieved at an early stage, and long term recovery is less marked in PER. It is likely that the rapid reperfusion blocks the molecular response to ischemia, which is associated with restorative processes and cerebral plasticity, and some degree of excitatory and inflammatory mechanisms may be associated with the late recovery of patients.
The results of this work may involve the following practical suggestions: treatments targeting excitotoxicity may be optimal if administered in very short therapeutic windows and the inhibition of excitotoxicity after the first hours could block molecular responses for brain healing. The use of peripheral glutamate grabbers, which do not affect the mechanisms of the excitatory response in the brain, could be therefore an interesting therapeutic alternative22. The administration of anti-inflammatory drugs in large therapeutic windows could have negative effects. In this sense, the use of inflammatory markers like IL6 could be used not only for diagnosis but also as neuroprotectors in the management of IS31,32.
Methods and Patients
Study design
This is a retrospective analysis conducted on a prospective registry of patients with acute cerebrovascular disease consecutively admitted to the Stroke Unit of the University Clinical Hospital of Santiago de Compostela (Spain) from September 2007 to March 2018. We prospectively included all IS patients admitted to the Stroke Unit in the BICHUS registry. The study was carried out in accordance with the Declaration of Helsinki of the World Medical Association and approved by the Research Ethics Committee of Galicia. Written informed consent was obtained on admission from each patient or from their relatives after full explanation of the procedures.
The clinical questions addressed in this study expressed in PICO (Patient, Intervention, Comparison, Outcome) format were:
Among IS patients, do high levels of glutamate, IL6 and effective reperfusion compared with low levels of the mentioned makers and with uneffective reperfusion and non recanalization treatments improve the functional outcome at short and long term after hospitalization?
Clinical variables
All patients were handled by the same stroke team according to the Stroke Unit protocol. The variables of our registry included the date, onset-inclusion and wake-up strokes. Moreover, demographic data, previous modified Rankin scale score (mRS) and vascular risk factors were included. Data on previous carotid disease and processes of carotid revascularization were also collected, and in patients with a previous transient ischemic attack (TIA), the time between the TIA and stroke, as well as the coincidence or not with the topography. Medical history recording potential vascular risk factors, blood and coagulation test, 12-lead ECG and chest x-ray were collected. Carotid and transcranial Doppler were performed on admission; the transcranial Doppler study was repeated as a control of the recanalization treatment in 18% of the treated patients. Axillary temperature was obtained on admission and every 4 hours during the first 48 hours. The outcome clinical variables recorded were: National Institute of Health Stroke Scale (NIHSS), an internationally validated scale used to quantify the neurological impairment caused by a stroke, with values ranging from 0 (no stroke symptoms) to 42 (severe stroke), measured on admission, 24 hours, 48 hours, at discharge and at 3 ± 1 months; and the modified Ranking Scale (mRS), which is commonly used for measuring the degree of disability or dependence in the activities of stroke patients, ranging from 0 (no symptoms) to 6 (dead), measured at discharge and at 3 ± 1 months. Good outcome was considered for patients with a mRS value of 0,1 and 2. Both scales were performed by accredited neurologist.
On the other hand, IS stroke subtypes were classified according to the TOAST criteria and hemorrhagic strokes were classified as hypertensive, amyloid or related to antiplatelet/anticoagulant. The type of reperfusion treatment, its characteristics and complications were also recorded.
At discharge, 28.7% of the patients were institutionalized and the rest were reintegrated into their family environment. During hospitalization, candidate patients for rehabilitation were evaluated by the Rehabilitation Service according to a common protocol. The outpatient rehabilitation was coordinated by the primary care physician, but it was not protocolized in an even way.
Analytical determinations
Biochemistry, haematology and coagulation test were assessed in the central laboratory of the hospital. For the molecular determinations, venous blood samples were collected in Vacutainer tubes (Becton Dickinson, San Jose, CA, USA) on admission, and 24 ± 12 hours and/or 48 ± 12 hours from stroke onset. After clotting for 60 minutes, blood samples were centrifuged at 3000 × g for 10 minutes, and the serum was immediately aliquoted, frozen and stored at −80 °C until analysis.
Glucose levels, glycosylated hemoglobin, leukocytes, red blood cells, platelets, fibrinogen, C-reactive protein, total and fractionated cholesterol, triglycerides, proBNP, vitamin D and cholecalciferol were measured on admission. Serum levels of glutamate were determined on admission and after 24 hours by high performance liquid chromatography (HPLC) analysis (1260 Infinity II; Agilent Technologies) using the AccQ‐Tag derivatization method for amino acid analysis following the manufacturer´s technical specifications (Waters)33. Serum levels of interleukin 6 (IL6) were also measured on admission and after 24 hours using an immunodiagnostic IMMULITE 1000 System (Diagnostic Products Corporation, California, USA).
Neuroimaging studies
All patients underwent cerebral computed tomography (CT) on admission and between days 4 and 7 after IS. Multimodal magnetic resonance imaging (MRI) was also performed on admission in IS patients candidates to recanalization treatments. Lesion volumes were measured using ABC/2 method34 in DWI-MRI on admission and betwen the 4th and 7th day in IS patients. In 2012, recanalization by endovascular treatment was protocolized in our hospital. Since 2012, a MRI angiography is performed in all patients candidate for reperfusion treatments. Neuroradiologists blinded to clinical and analytical data performed all imaging studies.
Patients
We included 6565 stroke patients. Excluded patients were: ICH (1011), transient ischemic attack patients (512), patients transferred to other hospital during the acute phase (44), dead by other causes (40), no final stroke diagnosis (85), admitted outside the acute phase (97) and lacked follow-up at 3 months (480). Finally, 4295 patients were valid for the analysis.
Early neurological improvement (the reduction ≥8 points in the NIHSS in the first 24 hours35) was used as a clinical marker of effective reperfusion.
Outcome endpoints
We have defined the intra-hospital improvement as the normalized percentage difference between the basal and discharge NIHSS through the formula: [(NIHSS on admission-NIHSS at discharge)/42 × 100], and the extra-hospital improvement between the NIHSS at discharge and at 3 ± 1 months, using the formula [(NIHSS at discharge-NIHSS at 3 months)/42 × 100] (42 was used to normalize the values as the maximum variation of the NIHSS).
We categorized the intra-hospital and extra-hospital improvement as a decrease ≥1 in the NIHSS between admission and discharge and between discharge and at 3 months, respectively. The deceased patients were given the highest NIHSS value.
Statistical analysis
Firstly, an analysis was performed to describe the sample. Frequencies and percentages were calculated for categorical variables while mean and standard deviation [SD] or median and interquartile range were used for continuous variables depending on their adjustment to normality. Kolmogorov-Smirnov test with Lilliefors was applied to assess it. ANOVA and squared test were performed to determine differences in patients according with the reperfusion group (PNR, PER, PWER). The main objective of the study was to evaluate the intra and extra hospital improvement. In order to achieve it, multivariable models were built using a lineal regression analysis. The dependent variables were adjusted by clinical significant variables calculated in the bivariate analysis. Also, logistic regression analyses were carried out for patients with the same dependent variables but categorized. These results were shown as odds ratios (ORs) with 95% confidence intervals (CI 95%). P-value <0.05 was considered to be statistically significant. The statistical analyses were conducted in SPSS 21.0 (IBM, USA).
Data availability
All data are available within the text of the manuscript. Further anonymized data could be made available to qualified investigators upon reasonable request.
References
Bai, J. & Lyden, P. D. Revisiting cerebral postischemic reperfusion injury: new insights in understanding reperfusion failure, hemorrhage, and edema. International Journal of Stroke 10, 143–152 (2015).
Lakhan, S. E., Kirchgessner, A. & Hofer, M. Inflammatory mechanisms in ischemic stroke: therapeutic approaches. Journal of translational medicine 7, 97 (2009).
Iadecola, C. & Anrather, J. The immunology of stroke: from mechanisms to translation. Nature medicine 17, 796 (2011).
Khatri, R., McKinney, A. M., Swenson, B. & Janardhan, V. Blood–brain barrier, reperfusion injury, and hemorrhagic transformation in acute ischemic stroke. Neurology 79, S52–S57 (2012).
Xing, C., Arai, K., Lo, E. H. & Hommel, M. Pathophysiologic cascades in ischemic stroke. International Journal of Stroke 7, 378–385 (2012).
Savitz, S. I., Baron, J.-C., Yenari, M. A., Sanossian, N. & Fisher, M. Reconsidering neuroprotection in the reperfusion era. Stroke 48, 3413–3419 (2017).
Chamorro, Á. Neuroprotectants in the Era of Reperfusion Therapy. Journal of stroke 20, 197 (2018).
Chamorro, A., Dirnagl, U., Urra, X. & Planas, A. M. Neuroprotection in acute stroke: targeting excitotoxicity, oxidative and nitrosative stress, and infl ammation. Lancet Neurology 15, 869–881, https://doi.org/10.1016/s1474-4422(16)00114-9 (2016).
Ikonomidou, C. & Turski, L. Why did NMDA receptor antagonists fail clinical trials for stroke and traumatic brain injury? The Lancet Neurology 1, 383–386 (2002).
Sughrue, M. E., Mehra, A., Connolly, E. S. Jr. & D’Ambrosio, A. L. Anti-adhesion molecule strategies as potential neuroprotective agents in cerebral ischemia: a critical review of the literature. Inflammation research: official journal of the European Histamine Research Society… [et al.] 53, 497–508, https://doi.org/10.1007/s00011-004-1282-0 (2004).
Moskowitz, M. A., Lo, E. H. & Iadecola, C. The science of stroke: mechanisms in search of treatments. Neuron 67, 181–198, https://doi.org/10.1016/j.neuron.2010.07.002 (2010).
Zhao, W. B. et al. Long-term outcomes of acute ischemic stroke patients treated with endovascular thrombectomy: A real-world experience. Journal of the Neurological Sciences 390, 77–83, https://doi.org/10.1016/j.jns.2018.03.004 (2018).
Muruet, W., Rudd, A., Wolfe, C. D. & Douiri, A. Long-term survival after intravenous thrombolysis for ischemic stroke: a propensity score-matched cohort with up to 10-year follow-up. Stroke 49, 607–613 (2018).
Campbell, B. C. V. et al. Endovascular Thrombectomy for Ischemic Stroke Increases Disability-Free Survival, Quality of Life, and Life Expectancy and Reduces Cost. Frontiers in Neurology 8, https://doi.org/10.3389/fneur.2017.00657 (2017).
Budimkic, M. S. et al. Long-Term Prognosis in Ischemic Stroke Patients Treated with Intravenous Thrombolytic Therapy. Journal of Stroke & Cerebrovascular Diseases 26, 196–203, https://doi.org/10.1016/j.jstrokecerebrovasdis.2016.09.009 (2017).
Enzmann, G., Kargaran, S. & Engelhardt, B. Ischemia–reperfusion injury in stroke: impact of the brain barriers and brain immune privilege on neutrophil function. Therapeutic Advances in Neurological Disorders 11, 1756286418794184 (2018).
Eltzschig, H. K. & Eckle, T. Ischemia and reperfusion-from mechanism to translation. Nature Medicine 17, 1391–1401, https://doi.org/10.1038/nm.2507 (2011).
Kinouchi, H. et al. Attenuation of focal cerebral ischemic-injury in transgenic mice overexpressing CuZn superoxide-dismutase. Proceedings of the National Academy of Sciences of the United States of America 88, 11158–11162, https://doi.org/10.1073/pnas.88.24.11158 (1991).
Copin, J. C. et al. Recombinant tissue plasminogen activator induces blood–brain barrier breakdown by a matrix metalloproteinase‐9‐independent pathway after transient focal cerebral ischemia in mouse. European Journal of Neuroscience 34, 1085–1092 (2011).
Iglesias-Rey, R. et al. Worse Outcome in Stroke Patients Treated with rt-PA Without Early Reperfusion: Associated Factors. Translational Stroke Research 9, 347–355, https://doi.org/10.1007/s12975-017-0584-9 (2018).
Wu, J. et al. Neuroprotective effects of sulfiredoxin-1 during cerebral ischemia/reperfusion oxidative stress injury in rats. Brain research bulletin 132, 99–108 (2017).
Guldris, N. et al. Influence of of the separation procedure on the properties of magnetic nanoparticles: Gaining in vitro stability and T-1-T-2 magnetic resonance imaging performance. Journal of Colloid and Interface Science 472, 229–236, https://doi.org/10.1016/j.jcis.2016.03.040 (2016).
Chamorro, Á., Dirnagl, U., Urra, X. & Planas, A. M. Neuroprotection in acute stroke: targeting excitotoxicity, oxidative and nitrosative stress, and inflammation. The Lancet Neurology 15, 869–881 (2016).
Soares, B. P. et al. Reperfusion Is a More Accurate Predictor of Follow-Up Infarct Volume Than Recanalization A Proof of Concept Using CT in Acute Ischemic Stroke Patients. Stroke 41, E34–E40, https://doi.org/10.1161/strokeaha.109.568766 (2010).
Ribo, M. et al. Temporal profile of recanalization after intravenous tissue plasminogen activator - Selecting patients for rescue reperfusion techniques. Stroke 37, 1000–1004, https://doi.org/10.1161/01.STR.0000206443.96112.d9 (2006).
Castillo, J., Dávalos, A. & Noya, M. Progression of ischaemic stroke and excitotoxic aminoacids. The Lancet 349, 79–82 (1997).
Castillo, J., Dávalos, A., Naveiro, J. & Noya, M. Neuroexcitatory amino acids and their relation to infarct size and neurological deficit in ischemic stroke. Stroke 27, 1060–1065 (1996).
Vila, N., Castillo, J., Davalos, A. & Chamorro, A. Proinflammatory cytokines and early neurological worsening in ischemic stroke. Stroke 31, 2325–2329, https://doi.org/10.1161/01.str.31.10.2325 (2000).
Vila, N. et al. Levels of anti-inflammatory cytokines and neurological worsening in acute ischemic stroke. Stroke 34, 671–675, https://doi.org/10.1161/01.str.0000057976.53301.69 (2003).
Bustamante, A. et al. Prognostic value of blood interleukin-6 in the prediction of functional outcome after stroke: a systematic review and meta-analysis. J Neuroimmunol 274, 215–224, https://doi.org/10.1016/j.jneuroim.2014.07.015 (2014).
Ramiro, L., Simats, A., García-Berrocoso, T. & Montaner, J. Inflammatory molecules might become both biomarkers and therapeutic targets for stroke management. Therapeutic Advances in Neurological Disorders 11, 1756286418789340, https://doi.org/10.1177/1756286418789340 (2018).
Grønhøj, M. H., Clausen, B. H., Fenger, C. D., Lambertsen, K. L. & Finsen, B. Beneficial potential of intravenously administered IL-6 in improving outcome after murine experimental stroke. Brain, behavior, and immunity 65, 296–311 (2017).
White, J., Hart, R. & Fry, J. An evaluation of the Waters Pico-Tag system for the amino-acid analysis of food materials. Journal of Analytical Methods in Chemistry 8, 170–177 (1986).
Sims, J. R. et al. ABC/2 for rapid clinical estimate of infarct, perfusion, and mismatch volumes. Neurology 72, 2104–2110, https://doi.org/10.1212/WNL.0b013e3181aa5329 (2009).
Kharitonova, T. et al. Association of early National Institutes of Health Stroke Scale improvement with vessel recanalization and functional outcome after intravenous thrombolysis in ischemic stroke. Stroke 42, 1638–1643 (2011).
Acknowledgements
This study was partially suproted by the Spanish Ministry of Economy and Competitiveness (SAF2014-56336-R; SAF2017-84267-R), Xunta de Galicia (GRC2014/027, IN607A2018/3) and Instituto de Salud Carlos III (RD16/0019, PIE13/00024 and PI17/01103, Miguel Servet contracts CPII17/00027 and CP14/00154). The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
Conception and design of the study P.H, R.I-R, J.C. Data acquisition and analysis (P.H., E.M., I.L-L.). Clinical data acquisition and analysis (J.C., E.R-C., M.R-Y., S.A., M.S-C., I.L-D.). Handled funding and supervision (F.C., T.S., J.C.). Statistical analysis (A.E-G. and J.C.). Manuscript drafting (P.H., R.I-R. and J.C.). Critical revision for important intellectual content (F.C., T.S., J.C.). Supervision P.H, R.I-R, J.C., All authors reviewed and approved the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Hervella, P., Rodríguez-Castro, E., Rodríguez-Yáñez, M. et al. Intra- and extra-hospital improvement in ischemic stroke patients: influence of reperfusion therapy and molecular mechanisms. Sci Rep 10, 3513 (2020). https://doi.org/10.1038/s41598-020-60216-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-60216-x
- Springer Nature Limited
This article is cited by
-
Neurological Instability in Ischemic Stroke: Relation with Outcome, Latency Time, and Molecular Markers
Translational Stroke Research (2022)