
Abstract
The objective of the present study was to explore past and future primary health care use in preadolescents reporting frequent non-specific health complaints or a low self-rated health compared to that of preadolescents with no frequent health complaints or with good self-rated health. The study was conducted as a cohort study based within the Danish National Birth Cohort (1996–2002). Information on non-specific health complaints and self-rated health was obtained by an 11-year follow-up questionnaire. Information about number of general practitioner (GP) contacts was obtained from the Health Insurance Service Register. A total of 44,877 pre-adolescents gave complete exposure information. Pre-adolescents who reported frequent non-specific health complaints had a higher use of GP compared to pre-adolescents without complaints across the five years following the index date (somatic complaints: IRR = (1.46 [1.38; 1.55], mental complaints: IRR = 1.16 [1.12; 1.19], both complaints: IRR = 1.58 [1.47; 1.69]). The same pattern was found for the association between low self-rated health and number of GP contacts (IRR = 1.41 (1.36; 1.46)). Non-specific health complaints and a poor self-rated health in pre-adolescents was associated with a higher past and future use of GP, indicating a need for development of early interventions with help for symptom management.
Similar content being viewed by others


Explore related subjects
Find the latest articles, discoveries, and news in related topics.Introduction
An increasing number of children and adolescents across nations in Europe and North America report non-specific health complaints such as headache, abdominal pain and back-pain1,2,3,4. In 2013–14, on average 27% of 11-year-old and 39% of 15-year-old European pre-adolescents and adolescents reported at least two non-specific health complaints on a weekly basis3. The prevalence varied widely between countries and was generally higher in girls.
The experience of frequent non-specific health complaints is an indicator of a low wellbeing. Hence, the symptoms may be viewed as different expressions of (bodily) distress, i.e. various responses to prolonged mental or physical stress in susceptible individuals5. For some children and adolescents, the non-specific health complaints can be very disabling and may affect every day functioning and result in excessive school absence6. In addition, the complaints have consistently been found to be associated with emotional problems such as anxiety and/or depression in cross sectional studies and to have implication for the future health of children with an increased risk of developing both somatic and psychiatric illness in adulthood7,8,9,10,11,12,13.
In both adults and adolescents, multiple non-specific health complaints have been shown to be associated with a lower self-rated health14,15. A low self-rated health in adults is predictive of higher health expenditures as well as a higher mortality rate compared to individuals reporting an excellent general health16,17. Self-rated health in adolescents has been found to be relatively stable through an 11-year period and a poor self-rated health in this age group has been shown to predict later health problems and use of medication in adulthood18,19.
Thus, preadolescents with frequent non-specific health complaints and poor self-rated health seem to constitute a growing and clinically relevant group of individuals who may acquire a maladaptive symptom-related behavior with increased use of health care and medication early in life20. Given that health behavior is established in childhood and adolescence, it seems relevant to investigate how self-rated health and the experience of frequent non-specific health complaints in youth affect the contact pattern to primary health care over time21,22,23,24. The few existing studies in this area have mainly been cross-sectional7,25,26,27,28,29.
The aim of the present study was to describe both past and future primary health care use in preadolescents reporting frequent non-specific health complaints or a low self-rated health compared to that of preadolescents who do not report these non-specific health complaints frequently or who rate their health as good.
Method
Study population and design
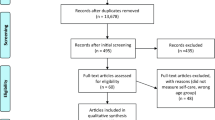
The study was based on longitudinal data on children from the Danish National Birth Cohort (DNBC)30. In short, women were recruited at their first pregnancy visit between 1996 and 2002. A total of 100,415 pregnancies were recruited resulting in 92,689 live born children after excluding live-born twins and triplets. In addition to multiple interviews during pregnancy and infancy, the children themselves and a parent were asked to fill in separate web-based questionnaires concerning health and lifestyle when the child turned 11 years. A total of 44,877 children gave complete information about non-specific health complaints and self-rated health at the 11-year follow-up.
Data from the 11-year follow-up was linked to information from the National Health Insurance Service Register (NHISR) using the unique personal identification number assigned to every citizen in Denmark31. The register holds information on services provided by health professionals in primary care contracted with the tax-funded public healthcare system. Since primary health care is free of charge in Denmark, private primary health care services not contracted by the tax-funded public health care system are considered negligible. Healthcare professionals must register all services provided with specific service codes to receive reimbursement for their services. From the NHISR it is possible to get information about type of contacts to the general practitioner (GP) (e.g. face-to-face consultation, e-mail and phone contacts) as well as the week and year of contact. The register also holds information on specific services provided by the GP, but no information on reason for the contacts.
Measures
Exposure
Information about non-specific health complaints and self-rated health was obtained from the 11-year follow-up questionnaire. The presence of frequent non-specific health complaints was determined from questions concerning the frequency of experienced somatic and mental health complaints during the past 6 months. Somatic health complaints included headache, abdominal pain, dizziness and constipation, whereas mental health complaints included feeling sad, irritability or bad mood, nervousness and trouble falling asleep. The symptom checklist has previously been shown to have a high validity and reliability32,33. The children were asked to fill in how often they experienced the different health complaints (daily, more than once a week, almost every week, more than once a month, almost every month, “more seldom or never”). In this study, frequent experience of complaints was defined as experiencing at least one of the health complaints on a daily basis (yes/no)4. This was further categorized in four subgroups: (1) no health complaints, (2) only mental health complaints, (3) only somatic health complaints or (4) both somatic and mental health complaints. Furthermore, in order to investigate if the total burden of somatic and/or mental health complaints was associated with increased health care use, we also calculated a total mental and somatic complaints sum-score. I.e. for each symptom, a score depending on the frequency was given (6 for daily health complaints decreasing to 1 for more seldom or never) and finally summed for all somatic or mental complaints, respectively. Finally, the sum-scores were categorized into tertiles (for somatic sum scores: low ( = 4), medium (5–6), high (7–24) and for mental sum-scores: low (4–6), medium (7–10), high (11–24).
Self-rated health was defined according to the question: How would you rate your own health? The answer-categories excellent, good, reasonable and bad were dichotomized into good (excellent or good) and poor (reasonable or bad).
Outcome
The main outcome was defined as total number of “all contacts” to the GP per year, which was defined as the sum of face-to-face contacts, telephone contacts and home visits in both day-time and out of hours, and E-mail contacts. E-mail contacts were included in the NHISR from 2004. Contacts related to routine well-child visits and to the Danish childhood vaccination program were excluded.
In further sub-analyses, the contacts were separated into total daytime contacts (sum of home visits, face to face, telephone, and e-mail contacts), daytime face-to-face, telephone, and finally total out of hour contacts (sum of home visits, face to face and telephone contacts). In addition, specific commonly performed paraclinical tests (urine analysis, blood samples, C-reactive protein, Streptococcal antigen and spirometry) were included as separate outcomes.
Covariates
Covariates were all selected a-priori. Information about sex and date of birth was obtained from the civil registration system. Information about year of filling out the questionnaire, number of siblings (both full and half) and parental cohabitation was obtained from the 11 year follow-up questionnaire and information about maternal education and family income was obtained from Statistics Denmark (the year prior to the date for filling out the 11 year questionnaire). Somatic and mental morbidity in the child prior to filling out the questionnaire was identified from answers to the 11-year questionnaire to the parents as well as from the Danish National Patient Registry and the Danish Register of Medicinal Product Statistics from a predefined checklist (Supplementary methods).
Statistical analyses
Negative binomial regression analysis estimating incidence rate ratios (IRR) was used to investigate the association between self-reported frequent non-specific health complaints as well as poor self-rated health and both past and future primary health care use. The date for filling out the 11-year questionnaire was defined as the index date. IRRs were estimated for each year prior to the index date back until birth and for every year following the index date until 31/12/2014. Mean follow-up time after filling out the questionnaire was 1068 days. Cluster robust variance was applied to account for repeated measurements in the individual child. The IRRs were adjusted for sex, age at index date (10, 11, 12, 13 and 14 years), year at index date (2010, 2011, 2012, 2013 and 2014), number of full-siblings (0, 1, 2, 3+), number of half-siblings (0, 1, 2, 3+), parental cohabitation (yes, no), known somatic morbidity (yes, no), known mental morbidity (yes, no), maternal education (lower secondary, upper secondary, tertiary, unknown) and family income (in quartiles).
Sub-analyses were conducted to investigate the association between self-reported nonspecific health complaints and self-rated health respectively and type of GP contact (daytime contacts, out of hour contacts, face-to-face contacts, telephone contact and E-mail contacts). In addition, the association with specific services provided by the GP were investigated (urine stix, blood sampling, c-reactive protein, streptococcal antigen and spirometry). Finally, the main analyses were stratified on sex.
All statistical analyses were performed in Stata 13 (StataCorp LP, TX, USA).
Ethics
The study was approved by the Danish Data protection Agency under the Aarhus University comment agreement (j. number 2015-57-0002) and Aarhus University j. number 2016-051-000001, sequential number 528. According to the Committee on Health Research Ethics in the Central Denmark Region, no ethical approval was required for this study. The DNBC was approved by the Committee on Health Research Ethics in the Capital Region of Denmark j. number (KF) 01-471/94 and by the Danish Data protection Agency under the common agreement for Statens Serum Institut, j. number 2015-57-0102. Written informed consents to use the self-reported information with linkage to register information was obtained from all mothers on behalf of themselves and their child and all methods were carried out in accordance with relevant guidelines and regulations including the General Data Protection Regulation (GDPR).
Results
Description of study population
Children participating in the 11-year follow-up were similar to those lost to follow-up with regard to year of birth and primary health care use in their 11th year of life. However, participants tended more often to be girls and to have mothers with longer educations and higher family income (Table 1).
The mean age of the children included was 11·4 years at index, 52% were girls, 10·7% reported experiencing at least one of the non-specific health complaints daily and 5·2% reported a poor self-rated health.
Children who reported frequent non-specific health complaints tended to have fewer full siblings and more half-siblings and more often to have non-cohabitating parents compared to children who did not report frequent complaints. In addition, they were more likely to suffer from concurrent somatic and mental conditions and to have a lower family income and a mother with a lower education. This was particularly evident for children who experienced both frequent mental and somatic complaints (Table 2).
Non-specific complaints and GP contacts
Children suffering from daily non-specific complaints had more frequent contacts to the GP compared to children without daily complaints. This was particularly evident from 1 year prior to the index date and onwards, but the consultation rate ratio (IRR) was above 1 for several years prior to the index date (Fig. 1). The associations appeared strongest for pre-adolescents experiencing either daily somatic or both somatic and mental complaints. On average, these groups had 46% and 57% more GP contacts (IRR = 1·46 (1·38; 1·55) and 1·57 (1·47; 1·69, respectively) during the first 5 years following the index date. However, also pre-adolescents reporting frequent mental health complaints had a higher health care use compared to children who did not report frequent complaints (IRR = 1·16 (1·12; 1·19)). The associations were similar when split into the different types of GP contacts and for specific services provided (Supplementary efigure 1a–d and efigure 2a–e). Also, the associations were similar for boys and girls (data not shown).

Mean number of yearly GP contacts by years before/since filling out the 11-year questionnaire according to the experience of frequent health complaints (non, somatic, mental or both somatic and mental) in top-panel and adjusted IRR (95%-CI) in bottom panel. IRRs and 95% CIs were estimated using negative binomial regression. Adjusted for sex, age, year, number of siblings, income and parental cohabitation.
The total burden of both non-specific somatic and mental complaints, i.e. the mental and somatic sum-scores, were also associated with primary health care use both prior to and following the index date, with an increase in IRR from early childhood and a leveling off around the index date (Fig. 2). Hence, children belonging to the second or third tertile for either the mental or somatic sum-scores had more GP contacts compared to children in the lowest tertile. The strongest associations were found for children in the third tertile.

Mean number of yearly GP contacts by years before/since filling out the 11-year questionnaire according to burden of somatic (left panel) and mental (right panel) health complaints in top-panel and adjusted IRR (95%-CI) in bottom panel. The burden of somatic and mental health complaints was calculated as sum-scores depending on the frequency of symptoms reported and categorized into tertiles. IRRs and 95% CIs were estimated using negative binomial regression. Adjusted for sex, age, year, number of siblings, income and parental cohabitation.
Self-rated health and GP contacts
Having a poor self-rated health was associated with a higher use of primary health care (Fig. 3). Again, the association was present several years prior to the index date and increased up until the index date before leveling off. Across the five years following the index date, pre-adolescents reporting a poor self-rated health had 41% more contacts on average compared to those who rated their health as good (IRR = 1·41 (1·36; 1·46)).The associations were similar when split into the different types of GP contacts and for specific services provided (supplementary efigure 3a–d and efigure 4a–e). Also, the association was similar for boys and girls (data not shown).

Mean number of yearly GP contacts by years before/since filling out the 11-year questionnaire according to self-rated health (good or bad) in top-panel and adjusted IRR (95%-CI) in bottom panel. IRRs and 95% CIs were estimated using negative binomial regression. Adjusted for sex, age, year, number of siblings, income and parental cohabitation.
Discussion
In summary, the study found that children experiencing frequent non-specific health complaints in pre-adolescence had higher past and future primary health care use compared to children who did not experience frequent health complaints. The association appeared strongest for children with a high burden of non-specific health complaints. Likewise, children with poor self-rated health had a higher past and future health care use compared to children reporting a good self-rated health.
Most previous studies on the association between non-specific health complaints and health care use have been cross sectional7,25,26,27,28. They have consistently found that children reporting non-specific health complaints have a higher use of health care services. To our knowledge, only one previous study has investigated the association between non-specific health complaints and future health care use. This study found higher healthcare use in Danish children with functional somatic symptoms at the age of 5–7 years29. Functional somatic symptoms are comparable to non-specific health complaint, except that the former primarily refers to medically unexplained somatic complaints. In another study using the same cohort, health care use in early childhood was a predictor of consulting the GP with respect to functional somatic symptoms34. Together these findings are in accordance with results from the present study showing higher both past and future primary health care use in children reporting non-specific health complaints. This tendency was evident for all types of contact to the general practitioner and for most types of specific services provided, indicating that the reasons for contacts are heterogenic and of both urgent and non-urgent character.
To our knowledge, no prospective study has previously investigated the association between self-rated health in children and primary health care use. However, one study based in the Norwegian YOUNG-HUNT-study did report an association between self-reported health service attendance in adolescents and self-rated health 4 years later15. This is in line with the finding from the present study with more contacts to the GP many years prior to the index date in children with a poor self-rated health. Also, longer follow up of the YOUNG-HUNT study revealed that a poor self-rated health at the age of 16 was associated with both allostatic load 11 years later and redemption of prescribed medication 18 years later18,19. In summary, these studies indicate that a poor self-rated health is established in early life and that it remains a strong predictor of problematic health issues even into adulthood21.
Primary health care use in younger children is to a large degree predicted by maternal illness behavior35,36. This is the case for both health care use in general and for non-specific health complaints24,37. Since the young children rely on parents when seeking help, the higher use of primary health care services in children with non-specific health complaints in early childhood could be the result of a maladaptive illness behavior by the parents10,21,22,38,39,40. This may affect the child’s self-rated health and experience of non-specific health complaints later in life and this again may affect the child’s health care seeking21. Whether this is the explanation for the associations seen in this study or whether these children always have had objective health problems, is however not possible to conclude from the present study.
The strengths of the study include the large study population as well as the registry-based information about health care use over a long period of time. The registry-based information excludes the risk of recall bias and the long observation time gives a detailed picture of the temporal development in health care use. The findings are believed to be generalizable to countries with a similar primary health care service where the GP act as a gatekeeper, but reservation should be taken when generalizing to countries without tax-payed health care services.
There are however also limitations in the study. The attrition of potential study participants is relatively large (51·8%). Children who were lost to follow-up were more likely to be boys, to have mothers with a lower degree of education, to have lower household income and to have parents with mental illness. Also, although not directly comparable, the relatively large difference in the prevalence of daily non-specific health complaints between the present study and the Danish Health Behavior in School-aged children (HBSC) Study (approx. 12% vs 25%), could indicate that the children suffering from frequent non-specific health complaints were less likely to participate in the study. Participation however appeared to be independent of primary health care use in the 11th year of life and selection bias is therefore expected to be limited. Another limitation of the study is that we do not know the reason for the health care contact. We also do not know whether the reported complaints and the poor self-rated health are due to known somatic or mental disorders. We did, however attempt to adjust for known concurrent morbidity according to both self-reported and registry-based information. This only changed the estimates marginally. Also, whereas the questions concerning non-specific health complaints have been validated among children in the relevant age-group, this is not the case for the question concerning self-rated health32,33. In adults, a poor self-rated health has been shown to be associated with an increased risk of becoming ill and die early and in adolescents it has been shown to be associated with health issues in adulthood. We therefore hypothesize that self-rated health also in 11-year-old children is an indicator of quality of life and future health.
In conclusion, children reporting frequent non-specific health complaints and poor self-rated health in pre-adolescence, have a higher both past and future health care use compared to children without such complaints and children who rate their health as good. With a general increase in the prevalence of non-specific health complains and poor self-rated health among children and adolescents, this is a group that needs special attention4. Development of early interventions are needed to prevent future morbidity and financial costs. These could be inspired by existing interventions, for medically unexplained symptoms in adults and should engage not only the young person but also the family as a whole41,42,43,44.
Data availability
Due to restrictions related to Danish law and protecting patient privacy, the combined set of data as used in this study can only be made available through a trusted third party, Statistics Denmark. This state organisation holds the data used for this study. University-based Danish scientific organisations can be authorized to work with data within Statistics Denmark and such organisations can provide access to individual scientists inside and outside of Denmark. Requests for data may be sent to Statistics Denmark: http://www.dst.dk/en/OmDS/organisation/TelefonbogOrg.aspx?kontor=13&tlfbogsort=sektion or the Danish Data Protection Agency: https://www.datatilsynet.dk/english/the-danish-data-protection-agency/contact/.
References
Berntsson, L. T. & Kohler, L. Long-term illness and psychosomatic complaints in children aged 2–17 years in the five Nordic countries. Comparison between 1984 and 1996. Eur. J. Public. Health 11, 35–42 (2001).
Dey, M., Jorm, A. F. & Mackinnon, A. J. Cross-sectional time trends in psychological and somatic health complaints among adolescents: a structural equation modelling analysis of ‘Health Behaviour in School-aged Children’ data from Switzerland. Soc. Psychiatry Psychiatr. Epidemiol. 50, 1189–1198 (2015).
Inchley, J., et al. Health policy for children and adolescents, no. 7. Growing up unequal: gender and socioeconomic differences in young people’s health and well-being. Health behaviour in school-aged children (HBSC) Study: International report from the 2013/2014 survey. (World Health Organization, Regional office for Europe, 2016).
Rasmussen, M.K. et al. 2018. (Syddansk Universitet, Statens Institut for Folkesundhed, 2019). (Danish)
Lievesley, K., Rimes, K. A. & Chalder, T. A review of the predisposing, precipitating and perpetuating factors in Chronic Fatigue Syndrome in children and adolescents. Clin. Psychol. Rev. 34, 233–248 (2014).
Hoftun, G. B., Romundstad, P. R., Zwart, J. A. & Rygg, M. Chronic idiopathic pain in adolescence–high prevalence and disability: the young HUNT Study 2008. Pain. 152, 2259–2266 (2011).
Campo, J. V., Comer, D. M., Jansen-Mcwilliams, L., Gardner, W. & Kelleher, K. J. Recurrent pain, emotional distress, and health service use in childhood. J. pediatrics 141, 76–83 (2002).
Jellesma, F. C., Rieffe, C., Terwogt, M. M. & Kneepkens, C. M. Somatic complaints and health care use in children: Mood, emotion awareness and sense of coherence. Soc. Sci. Med. 63, 2640–2648 (2006).
Hyams, J. S., Burke, G., Davis, P. M., Rzepski, B. & Andrulonis, P. A. Abdominal pain and irritable bowel syndrome in adolescents: a community-based study. J. pediatrics 129, 220–226 (1996).
Hotopf, M., Carr, S., Mayou, R., Wadsworth, M. & Wessely, S. Why do children have chronic abdominal pain, and what happens to them when they grow up? Population based cohort study. Bmj 316, 1196–1200 (1998).
Campo, J. V. et al. Adult outcomes of pediatric recurrent abdominal pain: do they just grow out of it? Pediatrics 108, E1 (2001).
Fearon, P. & Hotopf, M. Relation between headache in childhood and physical and psychiatric symptoms in adulthood: national birth cohort study. Bmj 322, 1145 (2001).
Homlong, L., et al. A prospective population-based study of health complaints in adolescence and use of social welfare benefits in young adulthood. Scandinavian journal of public health (2015).
Creed, F. H. et al. The epidemiology of multiple somatic symptoms. J. Psychosom. Res. 72, 311–317 (2012).
Breidablik, H. J., Meland, E. & Lydersen, S. Self-rated health during adolescence: stability and predictors of change (Young-HUNT study, Norway). Eur. J. Public. Health 19, 73–78 (2009).
DeSalvo, K. B., Bloser, N., Reynolds, K., He, J. & Muntner, P. Mortality prediction with a single general self-rated health question. A meta-analysis. J. Gen. Intern. Med. 21, 267–275 (2006).
DeSalvo, K. B. et al. Health care expenditure prediction with a single item, self-rated health measure. Med. care 47, 440–447 (2009).
Vie, T. L., Hufthammer, K. O., Holmen, T. L., Meland, E. & Breidablik, H. J. Is self-rated health a stable and predictive factor for allostatic load in early adulthood? Findings from the Nord Trondelag Health Study (HUNT). Soc. Sci. Med. 117, 1–9 (2014).
Vie, T. L., Hufthammer, K. O., Holmen, T. L., Meland, E. & Breidablik, H. J. Is self-rated health in adolescence a predictor of prescribed medication in adulthood? Findings from the Nord Trondelag Health Study and the Norwegian Prescription Database. SSM Popul. Health 4, 144–152 (2018).
Holstein, B. E. et al. Adolescents’ medicine use for headache: secular trends in 20 countries from 1986 to 2010. Eur. J. Public. Health 25(Suppl 2), 76–79 (2015).
Cardol, M. et al. All in the family: headaches and abdominal pain as indicators for consultation patterns in families. Ann. Fam. Med. 4, 506–511 (2006).
Levy, R. L., Whitehead, W. E., Von Korff, M. R. & Feld, A. D. Intergenerational transmission of gastrointestinal illness behavior. Am. J. Gastroenterol. 95, 451–456 (2000).
Craig, T. K., Cox, A. D. & Klein, K. Intergenerational transmission of somatization behaviour: a study of chronic somatizers and their children. Psychol. Med. 32, 805–816 (2002).
Shraim, M., Mallen, C. D. & Dunn, K. M. GP consultations for medically unexplained physical symptoms in parents and their children: a systematic review. Br. J. Gen. Pract. 63, e318–325 (2013).
Little, P. et al. Family influences in a cross-sectional survey of higher child attendance. Br. J. Gen. Pract. 51(977–981), 984 (2001).
Berra, S. et al. Correlates of use of health care services by children and adolescents from 11 European countries. Med. care 47, 161–167 (2009).
Vila, M., Kramer, T., Obiols, J. E. & Garralda, M. E. Abdominal pain in British young people: associations, impairment and health care use. J. Psychosom. Res. 73, 437–442 (2012).
Gieteling, M. J., Lisman-van Leeuwen, Y., van der Wouden, J. C., Schellevis, F. G. & Berger, M. Y. Childhood nonspecific abdominal pain in family practice: incidence, associated factors, and management. Ann. Fam. Med. 9, 337–343 (2011).
Graesholt-Knudsen, T., Skovgaard, A. M., Jensen, J. S. & Rask, C. U. Impact of functional somatic symptoms on 5–7-year-olds’ healthcare use and costs. Arch. Dis. Child. 102, 617–623 (2017).
Olsen, J. et al. The Danish National Birth Cohort–its background, structure and aim. Scand. J. public. health 29, 300–307 (2001).
Andersen, J. S., Olivarius Nde, F. & Krasnik, A. The Danish National Health Service Register. Scand. J. public. health 39, 34–37 (2011).
Haugland, S. & Wold, B. Subjective health complaints in adolescence–reliability and validity of survey methods. J. Adolesc. 24, 611–624 (2001).
Ravens-Sieberer, U. et al. An international scoring system for self-reported health complaints in adolescents. Eur. J. Public. Health 18, 294–299 (2008).
Rask, C. U., Ornbol, E., Fink, P. K. & Skovgaard, A. M. Functional somatic symptoms and consultation patterns in 5- to 7-year-olds. Pediatrics 132, e459–467 (2013).
Moran, T. E. & O’Hara, M. W. Maternal psychosocial predictors of pediatric health care use: Use of the common sense model of health and illness behaviors to extend beyond the usual suspects. Clin. Eff. Nurs. 9, e171–e180 (2006).
Minkovitz, C. S., O’Campo, P. J., Chen, Y. H. & Grason, H. A. Associations between maternal and child health status and patterns of medical care use. Ambul. Pediatr. 2, 85–92 (2002).
Shraim, M., Blagojevic-Bucknall, M., Mallen, C. D. & Dunn, K. M. Repeated primary care consultations for non-specific physical symptoms in children in UK: a cohort study. BMC Fam. Pract. 15, 195 (2014).
Barsky, A. J., Goodson, J. D., Lane, R. S. & Cleary, P. D. The amplification of somatic symptoms. Psychosom. Med. 50, 510–519 (1988).
Starfield, B. et al. Psychosocial and psychosomatic diagnoses in primary care of children. Pediatrics 66, 159–167 (1980).
Campo, J. V. et al. Physical and emotional health of mothers of youth with functional abdominal pain. Arch. Pediatr. Adolesc. Med. 161, 131–137 (2007).
van Gils, A. et al. Self-Help for Medically Unexplained Symptoms: A Systematic Review and Meta-Analysis. Psychosom. Med. 78, 728–739 (2016).
van Gils, A., Janssens, K. A. & Rosmalen, J. G. Family disruption increases functional somatic symptoms in late adolescence: the TRAILS study. Health Psychol. 33, 1354–1361 (2014).
Hulgaard, D., Dehlholm-Lambertsen, G. & Rask, C. U. Family-based interventions for children and adolescents with functional somatic symptoms: a systematic review. J. Fam. Ther. 41, 4–28 (2017).
Edwards, T. M., Cisneros, W. M. & Huth, A. A. Children and Adolescents with Medically Unexplained Symptoms: A Systematic Review of the Literature. Am. J. Family Ther. 47, 183–197 (2019).
Acknowledgements
The study was supported by the Program for Clinical Research Infrastructure (PROCRIN), which was established by the Lundbeck Foundation and the Novo Nordisk Foundation and is administered by Danish Regions. The Danish National Birth Cohort was established with a significant grant from the Danish National Research Foundation. Additional support was obtained from the Danish Regional Committees, the Pharmacy Foundation, the Egmont Foundation, the March of Dimes Birth Defects Foundation, the Health Foundation and other minor grants. The DNBC Biobank has been supported by the Novo Nordisk Foundation and the Lundbeck Foundation. Follow-up of mothers and children have been supported by the Danish Medical Research Council (SSVF 0646, 271-08-0839/06-066023, O602-01042B, 0602-02738B), the Lundbeck Foundation (195/04, R100-A9193), The Innovation Fund Denmark 0603-00294B (09-067124), the Nordea Foundation (02-2013-2014), Aarhus Ideas (AU R9-A959-13-S804), University of Copenhagen Strategic Grant (IFSV 2012), and the Danish Council for Independent Research (DFF – 4183-00594 and DFF - 4183-00152).
Author information
Authors and Affiliations
Contributions
D. Rytter conceptualized and designed the study, drafted the initial manuscript, and reviewed and revised the manuscript. B.H. Bech and C.U. Rask conceptualized and designed the study, and reviewed and revised the manuscript. C.H. Vestergaard carried out the analyses and reviewed and revised the manuscript. A.M. Nybo Andersen designed the data collection and reviewed and revised the manuscript. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Rytter, D., Rask, C.U., Vestergaard, C.H. et al. Non-specific Health complaints and self-rated health in pre-adolescents; impact on primary health care use. Sci Rep 10, 3292 (2020). https://doi.org/10.1038/s41598-020-60125-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-60125-z
- Springer Nature Limited
This article is cited by
-
Secular trends in risk factors for adolescent anxiety and depression symptoms: the Young-HUNT studies 1995–2019, Norway
European Child & Adolescent Psychiatry (2024)
-
Multiple health complaints in preadolescence and hospital contacts during adolescence: a prospective cohort study
Scientific Reports (2022)