
Abstract
The allele ε4 of the apolipoprotein E gene (APOE ε4) is the major genetic risk factor for non-dominantly inherited Alzheimer’s Disease (AD). Current techniques for APOE ε4 carriers identification show good accuracy but have several disadvantages that limit its implementation in a clinical laboratory. These include the need for sample preprocessing, poor automation, low throughput, requirement of additional equipment, and high cost. We followed ISO 13485 guidelines to validate the e4Risk test, a new latex-enhanced immunoturbidimetric blood assay for apolipoprotein E4 (ApoE4) determination in human plasma samples. The test showed high performance in terms of lot to lot variability, precision, interferences, reagents stability, prozone, and detectability. Furthermore, diagnostic accuracy is almost equal (99%) to the gold standard, APOE ε4 genotyping by polymerase chain reaction (PCR). Furthermore, we demonstrated that the e4Risk test can be adapted to any clinical chemistry analyzer, including the high throughput analyzers present in most hospitals and clinical laboratories. The e4Risk test versatility, low cost, and easiness provides an excellent solution for APOE ε4 carriers identification using the same blood sample drawn for biochemical diagnostic work-up of AD patients, which can have important advantages for patient stratification in clinical trials, preventative strategies for AD, and clinical assessment of risk for brain amyloidosis.
Similar content being viewed by others


Introduction
Apolipoprotein E (ApoE) is a glycoprotein involved in lipid metabolism. It is encoded by the APOE gene, which has three different alleles (ε2, ε3, ε4) that encode for three different ApoE isoforms (ApoE2, ApoE3, and ApoE4). These isoforms only differ at the amino acids 112 and 158. Isoform E2 has cysteine at both sites, E4 has arginine at both sites, while E3, the most common form, has a cysteine at position 112 and an arginine at position 1581,2. These minor sequence differences have profound consequences in protein function and ApoE isoforms have been associated with the predisposition to pathological conditions such as hyperlipoproteinemia3, hypercholesterolemia, coronary heart disease4 and Alzheimer’s disease (AD). The allele ε4 of APOE is the major genetic risk factor and the second most important risk factor after age for non-dominantly inherited AD (by far, the most common form). APOE ε4 is present in approximately 20% of the global population and in 40–60% of all patients with AD5,6. The presence of one allele ε4 of the APOE gene increases the risk of AD by 3–5 fold, while the presence in homozygosis increases the risk by 8–12 fold7. Furthermore, APOE ε4 carriers have an earlier onset of the disease8 and they progress faster from the prodromal stage of AD (mild cognitive impairment, MCI) to AD than APOE ε4 non-carriers9. Interestingly, ApoE4 appears to be closely related with brain amyloidosis, considered as one of the earliest events in AD pathophysiology10. Therefore, ApoE4 determination can provide meaningful information to physicians regarding the patient risk for brain amyloidosis and AD.
Several effective techniques are described for APOE genotyping, including gene-based analyses such as real-time PCR11 and biochemical (non-genetic) methods such as isoelectric focusing-immunoblotting12,13, ELISA14 or biochip arrays15. However, all of these techniques pose several limitations such as time-consuming, technically complex, need additional sample processing, require the investment on specific instrumentation, lack high-throughput capacity, or lack of fully automation. These technical disadvantages hampered in part the implementation of apoE4 analysis in the clinical routine of hospitals and laboratories.
We recently described an effective ELISA-based technique that could be adapted to immunoturbidimetry14 in order to eliminate these technical barriers. This assay represents a fast and cost-effective assay for ApoE4 determination (e4Risk test), that can be very easily implemented within the clinical routine, since it uses the same sample that other routine lab tests, without any further processing, and that can be run in any chemistry analyzer, including the high-throughput clinical chemistry analyzers present in hospitals and clinical laboratories.
Here we summarize the main experiments carried out to validate the test for scale-up and commercial distribution, under a formal Design Control for In vitro diagnostic (IVD) medical devices following ISO13485 guidelines. We also provide one example for its adaptation to one of the leading high-throughput chemistry analyzer Architect c16000 (Abbott).
Results
Lot to lot variability
A total of 40 plasma samples (8 APOE ε4 carriers) were analyzed with the three lots of Reagent 1(R1) and Reagent 2 (R2). Identical analytical result and 100% correlation with APOE genotyping by PCR were obtained with the three lots, demonstrating that the e4Risk test can be consistently produced using different lots of key raw material and that the three lots can be used indistinctly within the e4Risk test Validation.
Analytical performance
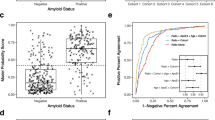
A total of 118 plasma samples (20 APOE ε4 carriers) were analyzed blinded to their APOE genotype. Real-time PCR showed the following genotypes (ε2/ε3, n = 11; ε2/ε4, n = 1; ε3/ε3, n = 87; ε3/ε4, n = 18; ε4/ε4, n = 1). The test showed a 100% sensitivity and 98.9% specificity. ApoE4 concentration (μg/mL) against the genotype is plotted in Fig. 1A. Receiver Operator Characteristics (ROC) curve for the APOE ε4 carriership analysis is shown in Fig. 1B. Analytical accuracy of the e4Risk test as measured as 1-misclassification rate was found to be 99% (only 1 false positive was found).

Analytical performance of the e4Risk test in a cohort of 118 plasma samples (20 APOE ε4 carriers). (A) ApoE4 concentration (μg/mL) against the genotype obtained by PCR. (B) Receiver Operator Characteristics (ROC) curve for the APOE ε4 carriership analysis. Analytical accuracy of the e4Risk test as measured as 1-misclassification rate was found to be 99%.
ApoE4 signal stability
ApoE4 signal stability was analyzed in fresh and frozen plasma samples under different storage conditions and at different times after blood extraction and plasma isolation. A total of 50 plasma samples (8 APOE ε4 carriers) were analyzed. Fresh samples were maintained either at room temperature (RT; 22 ± 3 °C) or refrigerated (5 ± 3 °C) and analyzed immediately (t0), 24 hours (for RT and refrigerated conditions) or 7 days (only for refrigerated conditions) after plasma isolation. Another set of samples were immediately frozen after plasma isolation at either −20 ± 5 °C or −70 ± 10 °C and analyzed 1 month and 3 months after freezing and after 1, 2 or 3 freeze/thaw cycles. ApoE4 signal was considered stable if the same analytical result of samples (i.e. sample was classified as APOE ε4 carrier or APOE ε4 non-carrier) at t0 was obtained. Results showed that ApoE4 signal was stable in plasma samples at least 24 h if kept at RT and at least 7 days if kept refrigerated after plasma isolation. Similarly, plasma ApoE4 is stable in frozen plasma samples for at least 3 months and at least after 3 freeze/thaw cycles at −20 ± 5 °C or −70 ± 5 °C.
Precision
The precision studies consisted on assaying two lots of positive controls with a theoretical concentration of 7.1 μg/mL (sample A) and 6.9 μg/mL (sample B), 2 runs per day during 20 days, every run for duplicate (a total of 80 replicates per sample). Precision data was evaluated in CV (%) of imprecision, according to guideline EP05A3E from Clinical & Laboratory Standards Institute (CLSI). Table 1 expresses the repeatability a well as the variability within laboratory, between run, within day and between days.
Results showed that CV for these parameters did not exceed 10%, with the exception of within-laboratory variability which was slightly above (11.6% and 10.6% for samples A and B, respectively).
Detectability (LoD and LoB)
Limit of Blank (LoB) and Limit of Detection (LoD) were evaluated according to guideline EP-17A2E from CLSI using the Classical Approach protocol with parametric data analysis previous normality test of raw data (Shapiro-Wilk and D’Agostino-Pearson tests).
Four different testing samples were prepared for LoB assays combining plasma from APOE ε4 non-carriers to achieve a final concentration of 0.44–0.77 µg/mL. Similarly, four different testing samples were prepared for LoD assays using the same plasmas used in LoB assays but spiked with recombinant ApoE4 (rApoE4) to achieve samples with low concentrations of ApoE4. LoD testing samples had a final concentration of 0.79–1.08 µg/mL. All samples were aliquoted and frozen at −70 °C until analysis. A total of 48 sample measurements per reagent lot were analyzed. (3 days × 4 samples × 4 replicates) for LoD and LoB determination.
LoB was found to be 0.87 μg/mL and LoD was 1.22 μg/mL.
Interferences
Evaluation of interferences was performed based on CLSI EP7-A2. Control (without interference) and test samples (with interference factor added) were prepared from each analytical group (APOE ε4 carrier and APOE ε4 non-carrier) and both samples were analyzed within one analytical run. The following concentrations of each interference were tested: Rheumatoid factor (450 UI/mL), intralipid (3 g/L), human hemoglobin (500 mg/dL), free bilirubin (18 mg/dL) and HAMA (human anti-mouse antibodies, 40 ng/mL). Due to the impossibility to obtain APOE genotype from commercial HAMA preparations and the common presence of other interferents in these preparations, HAMA interference was simulated using a goat anti-mouse antibody. An interference was considered to exist if the analytical result of the test sample was changed in the presence of the interference. If any interference was found, the minimum concentration at which the interference appeared was determined.
No significant interferences of rheumatoid factor (450 UI/mL), free bilirubin (18 mg/dL) or HAMA (40 ng/mL) were observed with the established cut-off value (4.62 μg/mL). Positive interference was observed in APOE ε4 non-carrier plasma sample with 3 g/L of Intralipid test and 500 mg/dL of hemoglobin. These interferences were no longer observed at 2.5 g/L and 300 mg/dL, respectively.
Prozone
Prozone was evaluated using plasma samples from APOE ε4 non-carriers spiked with increasing concentrations of rApoE4 (5, 10, 15, 20 and 30 times more concentrated than cut-off value (4.62 μg/mL)). Prozone effect was considered if the analytical result of a sample containing rApoE4 became negative. No prozone effect was found at any concentration, including the highest concentration tested (146 μg/mL).
Reagents stability
Three lots of R1 and R2 were evaluated at different times after production under the following conditions: onboard (reagents were left opened within the analyzer at 2–8 °C and were not mixed before analysis), shelf-life (reagents were stored at 2–8 °C and never used/opened before analysis) and opened (reagents were stored at 2–8 °C, analyzed and kept closed at 2–8 °C until following analysis). Similarly, two lots of calibrator and two positive and negative controls were produced, kept at 2–8 °C and analyzed under the following conditions: Freeze-dried (vials were stored at 2–8 °C and resuspended immediately before analysis) and reconstituted (vials were reconstituted and kept at 2–8 °C reconstituted until next analysis) and evaluated at different time points thereafter.
R1 and R2 stabilities were evaluated using one aliquot of calibrator and controls as well as one plasma sample from APOE ε4 carrier and one plasma sample from APOE ε4 carrier kept at −70 °C. R1 and R2 were considered stable if the analytical result of plasma samples were unchanged, positive and negative control were under specifications and calibrator concentration remained within ±20% of assigned concentration. On the other hand, calibrator and controls were considered stable if readings remained within the initial concentration ± 20%. The test was not considered failed until two consecutive time points did not meet the criteria.
R1 and R2 showed to be stable onboard at least for 4 weeks. R1 and R2 remained stable for at least 6 months (shelf-life) and at least 8 months (opened) (stability studies still ongoing). Calibrator and controls were stable after resuspension for 1 day and 7 days, respectively. Calibrator and controls shelf-life stability is still ongoing, and so far freeze-dried calibrator and controls are stable for at least 6 months.
Adaptability to different chemistry analyzers
The e4Risk test prototypes had shown prior to Validation its versatility for use in three different chemistry analyzers of different throughput capacity (Selectra Vital Junior, SpinReact, 110 tests/hour, LIDA 300 (Linear Chemicals, 300 tests/hour) and Architect c16000 (Abbott, 1600 tests/hour). Table 2 shows the optimal analytical performance of the e4Risk test prototype in these analyzers. Importantly, the e4Risk test final formulation maintained its adaptability to different chemistry analyzers such as SK-500 Biolis 50i (used during validation) and Architect c16000. Table 2 compares the analytical performance of the e4Risk test in both analyzers showing that the e4Risk test validated formulation maintained its adaptability and excellent performance among chemistry analyzers, including leading high throughput chemistry analyzers.
Discussion
We developed and validated a novel latex-enhanced immunoturbidimetric assay, the e4Risk test, which represents a fast, cost-effective and accurate method to identify APOE ε4 carriers within the clinical routine in a high-throughput and automated manner.
The e4Risk test is intended to be used for classifying individuals as APOE ε4 carrier (at-risk for AD) or APOE ε4 non-carrier. Identification of people at risk can be very valuable for stratification in clinical trials, prevention programs as well as providing valuable information to clinicians helping in the diagnostic process in selected cases16,17. The absolute concentration of ApoE4 is not informative for these intended uses and therefore, the e4Risk test was designed to report results qualitatively. Absolute concentrations values of ApoE4 provided by the e4Risk test should not be interpreted beyond its intended use. Individuals are binary classified either in APOE ε4 carrier or APOE ε4 non-carrier) depending if their apoE4 concentration is above or below the cut-off level, respectively. For example, absorbance values resulting in ApoE4 concentrations below the established cut-off value of 4.62 μg/mL are considered non-specific agglutination and will be reported as APOE ε4 non-carrier, despite being assigned with a positive absolute concentration of ApoE4.
We found that performance parameters regarding lot to lot variability, ApoE4 sample stability, precision, detectability, interferences, prozone, and reagents stability are good, comparable to similar routine lab tests and compatible with routine work in hospitals and clinical laboratories.
Diagnostic accuracy of the e4Risk test was found excellent (99%; sensitivity = 100% and specificity = 98.9%). One sample out of 118 was misclassified (false positive) in the validation set, which was also observed in the set of samples used for the adaptation to Architect c16000 (1 false positive out of 80 samples). The source of this misclassification is currently under investigation. As demonstrated during validation, high concentrations of triglycerides, cholesterol or hemoglobin, can affect the analytical results. Additionally, preliminary data from our lab suggest that the presence of anti-BSA antibodies in plasma can also interfere with the analytical results. Finally, since 90% of circulating ApoE4 is produced in the liver18, liver transplantation might induce some misclassification of patients if APOE ε4 genotype is not the same between donor and recipient. Therefore, our test should not be indicated for liver-transplanted individuals.
Higher signal was observed in APOE ε4 homozygous, but whether the test can differentiate by its own between heterozygous and homozygous cannot be ascertained since only 1 sample from homozygous could be recruited. Further experiments are underway in this regard. Nevertheless, the e4Risk test offers a sufficient level of information in order to fulfill its intended use of detecting the presence of ApoE4, independently of heterozygosis or homozygosis.
As opposed to currently available techniques for ApoE4 determination, the e4Risk test presents several advantages that allow its implementation within the clinical routine: First, the analysis can be performed in the same sample that other routine tests, without any preprocessing, which facilities its inclusion in routine laboratory test panels, such as the battery of tests performed in patients being evaluated for cognitive disorders (such as TSH, Vitamin B12, renal and hepatic function tests). Interestingly, these tests are not specific for AD but are used to rule out the so-called secondary dementias. The inclusion of the e4Risk test in this panel would provide clinicians with relevant information directly related to AD. Second, the e4Risk test does not require the laboratory to acquire specific instrumentation, since it can be run in the standard automated high-throughput chemistry analyzers present in most hospitals and clinical laboratories.
We believe that recent changes in scientific knowledge and AD health strategies created a demand for a fast, cost-effective and accurate method for detection of APOE ε4 carriers within the laboratory routine in a high-throughput and automated manner, without all the logistic problems of APOE genotyping by PCR.
On one hand, there is a growing literature showing that ApoE4 is directly related to extracellular amyloid beta (Aβ) accumulation (brain amyloidosis), considered one of the earliest events in AD pathophysiology10. ApoE4 stimulates the transcription of Amyloid Precursor Protein and Aβ secretion19 and also favors Aβ deposition and toxicity by several mechanisms20,21. All these findings obtained in animal and in vitro models find their correlation in humans, where it was demonstrated that the likelihood of having brain amyloidosis is significantly higher in APOE ε4 carriers within the entire AD continuum. Accordingly, abnormal Aβ brain accumulation occurs in more than 90% of APOE ε4 carriers diagnosed with AD22 and it was found that the probability of amyloid positivity of MCI patients is approximately twice as higher in APOE ε4 carriers than in APOE ε4 non-carriers23. Furthermore, even in healthy cognitively individuals, abnormal Aβ concentrations were found 10 years earlier in APOE ε4 carriers24. Therefore, ApoE4 detection provides clear information about the natural predisposition of APOE ε4 carriers for Aβ brain accumulation and their risk for brain amyloidosis, which is considered necessary for AD diagnosis by the latest guidelines for AD research25 and is has been recently proven to be a decisive information for AD diagnosis within clinical settings26.
On the other hand, prevention has become a major objective in the AD Health strategy. The failure during the last two decades of all investigational drugs led to the idea that treatments should be directed to very early stages of the disease27,28,29. Identification of people at risk is key for the effectiveness of preventative measures and consequently, APOE ε4 carriers were defined as a priority population for prevention30,31. Accordingly, several ongoing, prevention clinical trials describe APOE ε4 as an inclusion factor (NCT02565511, NCT03131453, NCT02569398) and large-scale screening programs are being established to identify APOE ε4 carriers for AD preventive clinical trials32. The e4Risk test, due to its ease of use and low cost can be very useful as a screening test for AD clinical trials, where APOE ε4 carriers can be selected in a fast and inexpensive manner.
Additionally, some evidence from clinical trials and clinical registries showed that the response to several investigational and prescription drugs to treat AD symptoms is different depending on APOE ε4 carriership33,34,35,36,37,38,39. Therefore, ApoE4 determination would not only provide clinicians with meaningful information about patient Aβ biology and risk to AD but also can eventually help to decide the optimal medical intervention.
Methods
Test description and reagents composition
The e4Risk test is a CE-marked and commercially available immunoturbidimetry test composed of two ready-to-use reagents (R1 and R2), one calibrator, and positive and negative controls, which are used as quality controls of the assay.
R1 is provided as a solution containing an anti-apoE4 antibody in a Bis-Tris buffer, BSA, and sodium azide. R2 is a suspension containing latex particles, in a Tris buffer with sodium azide. Calibrator and controls are provided as a lyophilized powder. Calibrator consists of a matrix composed of a pool of plasmas from APOE ε4 non-carriers and sucrose, spiked with human recombinant ApoE4. Positive and negative controls consist of a pool of plasmas from APOE ε4 carriers and APOE ε4 non-carriers.
Materials and reagents
The following key raw materials were used during the validation process:
Human recombinant ApoE4 (rApoE4, Peprotech; London, UK), mouse anti-apoE4 (4E4 clone, Novus Biologicals; Abingdon, UK), bovine serum albumin (BSA, Merck; Spain), human plasma (Diaserve Laboratories GmbH; Ifeldorf, Germany), latex particles (Ikerlat Polymers; Guipúzcoa, Spain), human hemoglobin, bilirubin, and intralipid were purchased from Sigma-Aldrich (Spain), rheumatoid factor (Access Biologicals, Spain), goat anti-mouse IgG (Novus Biologicals; Abingdon, UK).
Validation process
Three lots of R1 and R2 were produced for validation: lot A (250 mL of each reagent), lot B (500 mL), and lot C (750 mL), combining different lots of key raw material. The three lots were compared in the lot to lot variability assay as well as during reagent stability assays. The calibrator curve stability, prozone, and detectability assays were performed with two lots (B and C), while just one lot (B or C) was used for the correlation, calibrator and control stability assays, precision, interferences, and ApoE4 sample stability assays.
Two different lots of calibrator and controls were also produced for validation with the following ApoE4 concentration: Calibrators (6.44 and 6.65 μg/mL), positive controls (7.05 and 7.78 μg/mL) and negative controls (0.83 and 1.02 μg/mL). All assays were calibrated with a calibrator lot that was produced prior to validation at 7.1 μg/mL and that was aliquoted and stored at −70 °C.
Plasma samples and APOE Genotyping
Blood samples were centrifuged at 2280 g for 5 minutes to isolate plasma. Human plasma samples were collected from two different sources:
A set of 19 samples were acquired from Diaserve Laboratories GmbH (Iffeldorf, Germany). These samples were used for building the matrix of calibrator and controls and for the analytical performance study. Additionally, another set of samples were collected from 100 healthy volunteers (51 women and 49 men from 18 to 63 years old) within the context of the project entitled “Study for the development of a non-genetic test in blood for the identification of carriers of the ε4 allele of the APOE gene (APOE ε4)” (Code: BCR-2017-01). The study was approved by the Clinical Investigation Ethical Committee from the Santa Creu i Sant Pau Hospital (Barcelona, Spain). These samples were used in the analytical performance study as well as in the rest of the validation assays.
All samples were obtained after an informed consent form was signed by subjects. All the data were analyzed anonymously, and clinical investigations have been conducted according to the principles expressed in the Declaration of Helsinki. For logistic reasons, all plasma samples used during the e4Risk test validation were frozen and stored at −70 °C, with the exception of some samples used in the ApoE4 sample stability assay. Frozen samples had a maximum of 2 freeze/thaw cycles and were stored at −70 ± 10 °C for less than 1 year before analysis.
Paired samples of total blood were collected from each participant for APOE genotyping following the method described in Calero et al.40. APOE genotype obtained by Real-Time PCR was used as the reference technique for comparison of turbidimetric results.
Gold standard
The e4Risk test calibrators and controls are traceable to a gold standard produced prior to validation. The gold standard consisted on a lyophilized plasma from an APOE ε4 carrier (ε3/ε4), whose ApoE4 concentration (13.44 μg/mL) was determined by targeted mass spectrometry (multiple reaction monitoring, MRM) following a method developed ad hoc, based on the method described in Rezeli et al.41.
Sample analysis
Plasma samples used for validation were analyzed with the chemistry analyzer SK-500 Biolis 50i (Tokyo Boeki, Japan, 580 tests/hour). Shortly, the analyzer was calibrated with a two point-calibration curve, using purified water as the 0 μg/mL point and resuspended the e4Risk test calibrator as the 7.1 μg/mL point. Then, 5 μL of plasma were incubated with 110 μL of R1 and 110 μL of R2, gently mixed and absorbance at 546 nm was obtained immediately (A1). Then, the mixture was incubated at 37 °C for 5 minutes and the absorbance was read again (A2). ApoE4 concentration was calculated by interpolation of its (A2-A1) value in the calibration curve. Quality controls were included in each run. All samples and controls were run in duplicate, with the exception of calibrator which was run in triplicate. Results were expressed as the mean of replicates. All sample were evaluated using a cut-off of 4.62 μg/mL and were defined as APOE ε4 carrier or APOE ε4 non-carrier depending if its ApoE4 concentration was above or below this value, respectively. The cut-off point of 4.62 μg/mL was established based on the a priori criteria that the test should be able to detect all APOE ε4 carriers (sensitivity = 100%). This criteria was considered to be the most beneficial for its intended uses for identifying patients at risk of brain amyloidosis and as a screening test for clinical trials or preventive initiatives.
Sample analysis for the adaptation to the high-throughput Architect c16000 (Abbott) was identical, with the exception that sample (8 μL) and R1 (160 μL) were incubated for 5 minutes before adding R2 (160 μL), and that samples were run without replicas and analyzed at 548 nm.
Employment or leadership
MC is one of the cofounders of Biocross SL and owns stock options from the company. ARM and SV are employees of Biocross SL. M.C. and A.R.M participate in the European patent application EP 16 794 966.8-1111, entitled METHODS FOR APOLIPOPROTEIN DETECTION which is directly related to this work and was granted by the European patent Agency on 09th January 2019.
References
Emi, M. et al. Genotyping and sequence analysis of apolipoprotein E isoforms. Genomics 3, 373–379 (1988).
Utermann, G., Langenbeck, U., Beisiegel, U. & Weber, W. Genetics of the apolipoprotein E system in man. American journal of human genetics 32, 339–347 (1980).
Breslow, J. L. et al. Studies of familial type III hyperlipoproteinemia using as a genetic marker the apoE phenotype E2/2. Journal of lipid research 23, 1224–1235 (1982).
Lahoz, C. et al. Apolipoprotein E genotype and cardiovascular disease in the Framingham Heart Study. Atherosclerosis 154, 529–537 (2001).
Crean, S. et al. Apolipoprotein E epsilon4 prevalence in Alzheimer’s disease patients varies across global populations: a systematic literature review and meta-analysis. Dementia and geriatric cognitive disorders 31, 20–30, https://doi.org/10.1159/000321984 (2011).
van Duijn, C. M. et al. Apolipoprotein E4 allele in a population-based study of early-onset Alzheimer’s disease. Nature genetics 7, 74–78, https://doi.org/10.1038/ng0594-74 (1994).
Farrer, L. A. et al. Effects of age, sex, and ethnicity on the association between apolipoprotein E genotype and Alzheimer disease. A meta-analysis. APOE and Alzheimer Disease Meta Analysis Consortium. Jama 278, 1349–1356 (1997).
Corder, E. H. et al. Gene dose of apolipoprotein E type 4 allele and the risk of Alzheimer’s disease in late onset families. Science 261, 921–923 (1993).
Craft, S. et al. Accelerated decline in apolipoprotein E-epsilon4 homozygotes with Alzheimer’s disease. Neurology 51, 149–153 (1998).
Selkoe, D. J. & Hardy, J. The amyloid hypothesis of Alzheimer’s disease at 25 years. EMBO molecular medicine 8, 595–608, https://doi.org/10.15252/emmm.201606210 (2016).
Zivelin, A. et al. Improved method for genotyping apolipoprotein E polymorphisms by a PCR-based assay simultaneously utilizing two distinct restriction enzymes. Clinical chemistry 43, 1657–1659 (1997).
Kataoka, S., Paidi, M. & Howard, B. V. Simplified isoelectric focusing/immunoblotting determination of apoprotein E phenotype. Clinical chemistry 40, 11–13 (1994).
Steinmetz, A. Phenotyping of human apolipoprotein E from whole blood plasma by immunoblotting. Journal of lipid research 28, 1364–1370 (1987).
Calero, O., García-Albert, L., Rodríguez-Martín, A., Veiga, S. & Calero, M. A fast and cost-effective method for apolipoprotein E isotyping as an alternative to APOE genotyping for patient screening and stratification. Scientific reports 8, 5969, https://doi.org/10.1038/s41598-018-24320-3 (2018).
Badrnya, S. et al. Development of a new biochip array for APOE4 classification from plasma samples using immunoassay-based methods. Clinical chemistry and laboratory medicine 56, 796–802, https://doi.org/10.1515/cclm-2017-0618 (2018).
Sun, X., Nicholas, J., Walker, A., Wagner, M. T. & Bachman, D. APOE genotype in the diagnosis of Alzheimer’s disease in patients with cognitive impairment. American journal of Alzheimer’s disease and other dementias 27, 315–320, https://doi.org/10.1177/1533317512452037 (2012).
Sabbagh, M. N., Lue, L. F., Fayard, D. & Shi, J. Increasing Precision of Clinical Diagnosis of Alzheimer’s Disease Using a Combined Algorithm Incorporating Clinical and Novel Biomarker Data. Neurology and therapy 6, 83–95, https://doi.org/10.1007/s40120-017-0069-5 (2017).
Linton, M. F. et al. Phenotypes of apolipoprotein B and apolipoprotein E after liver transplantation. The Journal of clinical investigation 88, 270–281, https://doi.org/10.1172/JCI115288 (1991).
Huang, Y. A., Zhou, B., Wernig, M. & Sudhof, T. C. ApoE2, ApoE3, and ApoE4 Differentially Stimulate APP Transcription and Abeta Secretion. Cell. 168, 427–441 e421, https://doi.org/10.1016/j.cell.2016.12.044 (2017).
Kim, J., Basak, J. M. & Holtzman, D. M. The role of apolipoprotein E in Alzheimer’s disease. Neuron 63, 287–303, https://doi.org/10.1016/j.neuron.2009.06.026 (2009).
Hashimoto, T. et al. Apolipoprotein E, especially apolipoprotein E4, increases the oligomerization of amyloid beta peptide. The Journal of neuroscience: the official journal of the Society for Neuroscience 32, 15181–15192, https://doi.org/10.1523/JNEUROSCI.1542-12.2012 (2012).
Ossenkoppele, R. et al. Prevalence of amyloid PET positivity in dementia syndromes: a meta-analysis. Jama 313, 1939–1949, https://doi.org/10.1001/jama.2015.4669 (2015).
Jansen, W. J. et al. Prevalence of cerebral amyloid pathology in persons without dementia: a meta-analysis. Jama 313, 1924–1938, https://doi.org/10.1001/jama.2015.4668 (2015).
Lautner, R. et al. Preclinical effects of APOE epsilon4 on cerebrospinal fluid Abeta42 concentrations. Alzheimer’s research & therapy 9, 87, https://doi.org/10.1186/s13195-017-0313-3 (2017).
Jack, C. R. Jr. et al. NIA-AA Research Framework: Toward a biological definition of Alzheimer’s disease. Alzheimer’s & dementia: the journal of the Alzheimer’s Association 14, 535–562, https://doi.org/10.1016/j.jalz.2018.02.018 (2018).
Rabinovici, G. D. et al. Association of Amyloid Positron Emission Tomography With Subsequent Change in Clinical Management Among Medicare Beneficiaries With Mild Cognitive Impairment or Dementia. Jama 321, 1286–1294, https://doi.org/10.1001/jama.2019.2000 (2019).
Sperling, R. In 14th Annual Mild Cognitive Impairment Symposium (Miami Beach Resort, Miami. Florida, 2016).
Livingston, G. et al. Dementia prevention, intervention, and care. Lancet, https://doi.org/10.1016/S0140-6736(17)31363-6 (2017).
Crous-Bou, M., Minguillon, C., Gramunt, N. & Molinuevo, J. L. Alzheimer’s disease prevention: from risk factors to early intervention. Alzheimer’s research & therapy 9, 71, https://doi.org/10.1186/s13195-017-0297-z (2017).
Reiman, E. M. et al. Alzheimer’s Prevention Initiative: a plan to accelerate the evaluation of presymptomatic treatments. Journal of Alzheimer’s disease: JAD 26(Suppl 3), 321–329, https://doi.org/10.3233/JAD-2011-0059 (2011).
Solomon, A. et al. Effect of the Apolipoprotein E Genotype on Cognitive Change During a Multidomain Lifestyle Intervention: A Subgroup Analysis of a Randomized Clinical Trial. JAMA neurology, https://doi.org/10.1001/jamaneurol.2017.4365 (2018).
Langbaum, J. B. et al. GeneMatch: A novel recruitment registry using at-home APOE genotyping to enhance referrals to Alzheimer’s prevention studies. Alzheimer’s & dementia: the journal of the Alzheimer’s Association, https://doi.org/10.1016/j.jalz.2018.12.007 (2019).
Yassine, H. N. et al. Association of Docosahexaenoic Acid Supplementation With Alzheimer Disease Stage in Apolipoprotein E epsilon4 Carriers: A Review. JAMA neurology 74, 339–347, https://doi.org/10.1001/jamaneurol.2016.4899 (2017).
S. Abushakra, A. P. et al. Clinical Benefits Of Tramiprosate In Alzheimer’s Disease Are Associated With Higher Number Of Apoe4 Alleles: The “Apoe4 Gene-Dose Effect”. The Journal of Prevention of Alzheimer´s Disease 3, 219–228 (2016).
Henderson, S. T. et al. Study of the ketogenic agent AC-1202 in mild to moderate Alzheimer’s disease: a randomized, double-blind, placebo-controlled, multicenter trial. Nutrition & metabolism 6, 31, https://doi.org/10.1186/1743-7075-6-31 (2009).
Salloway, S. et al. Two phase 3 trials of bapineuzumab in mild-to-moderate Alzheimer’s disease. The New England journal of medicine 370, 322–333, https://doi.org/10.1056/NEJMoa1304839 (2014).
Sevigny, J. et al. The antibody aducanumab reduces Abeta plaques in Alzheimer’s disease. Nature 537, 50–56, https://doi.org/10.1038/nature19323 (2016).
Sokolow, S. et al. Deleterious Effect of Butyrylcholinesterase K-Variant in Donepezil Treatment of Mild Cognitive Impairment. Journal of Alzheimer’s disease: JAD 56, 229–237, https://doi.org/10.3233/JAD-160562 (2017).
Wang, L. et al. The effect of APOE epsilon4 allele on cholinesterase inhibitors in patients with Alzheimer disease: evaluation of the feasibility of resting state functional connectivity magnetic resonance imaging. Alzheimer disease and associated disorders 28, 122–127, https://doi.org/10.1097/WAD.0b013e318299d096 (2014).
Calero, O., Hortiguela, R., Bullido, M. J. & Calero, M. Apolipoprotein E genotyping method by real time PCR, a fast and cost-effective alternative to the TaqMan and FRET assays. Journal of neuroscience methods 183, 238–240, https://doi.org/10.1016/j.jneumeth.2009.06.033 (2009).
Rezeli, M. et al. Quantification of total apolipoprotein E and its specific isoforms incerebrospinal fluid and blood in Alzheimer’s disease and otherneurodegenerative diseases. EuPa Open Proteomics 8, 137–145 (2015).
Acknowledgements
The authors thank all the patients, hospitals, and institutions that made this study possible. We thank Pablo Cabello, Matt Mittino, Isabel Jiménez and Cristina Pérez for their decisive role throughout the course of this project, and Verónica Martínez, Montse Pérez and Lluis Cano from Linear Chemicals (Barcelona, Spain) for their work on the validation of the method. We also thank Dr. Alberto Paradela, Sergio Ciordia and Maria del Carmen Mena from Proteomics Facility, National Center for Biotechnology (CNB, Madrid, Spain) for their work on the development of a Targeted mass spectrometry (MRM)-based method for the quantification of ApoE4. Finally, we thank Montserrat Puntes (MD.) and Maria Teresa Garrido (MSc.) from the Centre for Drug Research (CIM) of the Hospital de la Santa Creu i Sant Pau for their collaboration on the project entitled “Study for the development of a non-genetic test in blood for the identification of carriers of the ε4 allele of the APOE gene (APOE ε4)” (Code: BCR-2017-01). This research was fully funded by Biocross and did not receive any other specific grant from funding agencies in the public, commercial, or not-for-profit sectors for this research.
Author information
Authors and Affiliations
Contributions
All the authors have accepted responsibility for the entire content of this submitted manuscript and approved submission. Conceived, design the experiments and analysis of data: S.V., A.R.M. and M.C.; Wrote the manuscript: S.V., A.R.M., G.G.R. and M.C.; Experiments adaptation to Architect: M.M.R.; Critical revision of the manuscript; I.A.
Corresponding authors
Ethics declarations
Competing interests
This work was supported by Biocross SL, which participated in the acquisition of data, study supervision, and approval of data generated by the outsourced company, Linear Chemicals. Biocross SL participated in the study design; in the collection, analysis, and interpretation of data; in the writing of the report and the decision to submit the report for publication.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Veiga, S., Rodríguez-Martín, A., Garcia-Ribas, G. et al. Validation of a novel and accurate ApoE4 assay for automated chemistry analyzers. Sci Rep 10, 2138 (2020). https://doi.org/10.1038/s41598-020-58841-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-58841-7
- Springer Nature Limited
This article is cited by
-
Perspectives and challenges in patient stratification in Alzheimer’s disease
Alzheimer's Research & Therapy (2022)