
Abstract
The study aimed to evaluate the treatment outcome of bimaxillary surgery for class II asymmetry and find the influencing factors for residual asymmetry. Cone-beam computed tomographic images of 30 adults who had bimaxillary surgery were acquired, and midline and contour landmarks of soft tissue and teeth were identified to assess treatment changes and outcome of facial asymmetry. The postoperative positional asymmetry of each osteotomy segment was also measured. After surgery, the facial midline asymmetry of the mandible, chin, and lower incisors improved significantly (all p < 0.01). However, the residual chin deviation remained as high as 2.64 ± 1.80 mm, and the influencing factors were residual shift asymmetry of the mandible (p < 0.001), chin (p < 0.001), and ramus (p = 0.001). The facial contour asymmetry was not significantly improved after surgery, and the influencing factors were the initial contour asymmetry (p < 0.001), and the residual ramus roll (p < 0.001) or yaw (p < 0.01) asymmetry. The results showed that bimaxillary surgery significantly improved midline but not contour symmetry. The postoperative midline and contour asymmetry was mainly affected by the residual shift and rotational jaw asymmetry respectively.
Similar content being viewed by others
Introduction
Facial asymmetry is commonly seen in adults. The causes of facial asymmetry include skeletal asymmetry, soft tissue asymmetry, functional asymmetry or a combination1. Of these, skeletal asymmetry involving deviations in the maxillofacial region is predominant. In instances of jaw asymmetry, distinctions in type of asymmetry can be further divided into positional, size, and shape asymmetry2,3. Positional asymmetry of the jaw can be further described into shift (translation), roll or yaw (rotation) asymmetry4.
Positional asymmetry of the jaw must be addressed before size and shape asymmetry can be efficiently diagnosed and corrected and the only procedure for centering jaws in adult patients is orthognathic surgery (OGS). Many studies on correcting facial asymmetry with OGS have been conducted, however most corrections were on patients with class III deformity5,6,7,8,9,10,11,12,13,14 due to the lower incidence and extent of facial asymmetry in class II deformity15,16,17. Furthermore, the focus of most of these studies was on improvement of midline asymmetry. Symmetry of gonial width improved after OGS in a study by Ko et al. and frontal ramal symmetry improved for many patients in a study by Chen et al.; however, their investigation of the change of contour asymmetry was limited to skeletal structures8,14. Despite Blockhaus et al. and Hajeer et al. studying outcomes of OGS on patients with class II asymmetry, there was a lack of information regarding contour asymmetry16,18. Importantly, none of the above studies analyzed the impact of positional jaw asymmetry on residual asymmetry with regards to soft tissue and dental aspects.
The introduction and development of cone-beam computed tomography (CBCT) makes the accurate evaluation of the 3-dimensional (3D) complexity of facial asymmetry possible. Therefore, this study aimed to evaluate the asymmetry outcome (midline and contour symmetry) of bimaxillary OGS for class II asymmetry and find the influencing factors for residual asymmetry.
Results
Thirty patients with class II asymmetry (9 men and 21 women; mean age, 29.3 ± 5.6 years; range, 19.0 to 47.0 years) fulfilled the inclusion criteria and were analyzed. The postoperative CBCT was taken 20.6 ± 7.2 months after surgery, on average (range, 12.0 to 34.6 months). The bimaxillary surgery was highly effective for class II deformity with significant improvement in the ANB angle (from 7.2 ± 2.0 degrees to 3.7 ± 1.5 degrees, p < 0.001) and overjet (from 4.8 ± 3.0 mm to 2.7 ± 0.6 mm, p < 0.01).
Asymmetry outcome
The bimaxillary surgery significantly improved the midline deviation of the mandible (p < 0.01), chin (p < 0.001), and lower incisors (p < 0.01). Nevertheless, the midline deviation of the nose deteriorated after surgery (p < 0.001). There was no significant improvement in the lip cant, upper, middle, or lower contour asymmetry (p > 0.01) (Table 1).
Influencing factors for residual asymmetry
Stepwise multiple linear regression analysis demonstrated the residual midline deviation of the nose and upper lip was associated with the initial deviation and the residual maxillary shift asymmetry (all p ≤ 0.001). The residual midline deviation of the lower lip was associated with the residual mandibular shift asymmetry (p = 0.001). The residual midline deviation of the mandible was affected by the residual shift and yaw asymmetry of the mandible (both p < 0.001). The residual midline deviation of the chin was affected by the residual shift asymmetry of the mandible (p < 0.001), chin (p < 0.001), and ramus (p = 0.001). The residual lip cant was affected by the residual mandibular roll asymmetry (p < 0.001) (Table 2).
The residual upper contour asymmetry was associated with its initial asymmetry and the residual ramus roll asymmetry (both p < 0.001). The residual middle and lower contour asymmetry was associated with their initial asymmetry (both p < 0.001) and the residual ramus roll (both p < 0.001) and yaw asymmetry (both p < 0.01) (Table 2).
The residual upper dental midline deviation was affected by the residual mandibular yaw asymmetry (p < 0.001) and maxillary shift asymmetry (p < 0.01). The residual lower dental midline deviation was affected by the residual yaw (p = 0.001) and shift (p < 0.01) asymmetry of the mandible (Table 2).
Discussion
Patient satisfaction for correction of sagittal deformity and malocclusion via OGS requires improvement of facial asymmetry. Improvement of midline asymmetry of soft tissue and incisors shown in the frontal view, including midline deviation and lip cant, are of primary importance for patients to assess an asymmetry outcome positively6,7,19. Nevertheless, the frontal contour asymmetry, which is indeed altered by OGS and is of great clinical relevance20, has long been overlooked. Thus, the facial landmarks chosen in the present study covered midline and contour regions, intending to provide a measuring technique which is easily applicable and practical for clinicians to assess facial symmetry during and after operation.
This study also evaluated the underlying jaw characteristics contributing to the residual asymmetry after surgery. After bimaxillary surgery, the extent of residual facial asymmetry was highest in the lower contour region, and decreased in the order of middle and upper contour, chin, mandible, lower and upper incisors, lower lip, lip commissures, upper lip, and nose. The trend was almost the same as preoperative asymmetry (Table 1). For the contour region, the asymmetry was improved via surgery but not well enough to reach significance, which was correlated with the initial asymmetry and the roll or yaw asymmetry of the ramus (Table 2).
Although the mandibular body is the underlying skeletal support corresponding to the soft tissue envelope of the lower contour region, there was no significant correlation in between. Residual lower contour asymmetry was directly affected by the ramus, rather than the underlying mandibular body. One possible explanation is the modified Hunsuck technique, which extends the anterior cut of the osteotomy to the first molar. Another explanation is the limitation of the roll rotation of the proximal segment during surgery14. This speculation is supported by the significant correlation between the postoperative ramus roll asymmetry and the postoperative mandibular yaw asymmetry (r = −0.61, p < 0.001).
The threshold of clinical acceptance for midline asymmetry has been reported to be approximately 2 mm, including the upper dental midline21,22, lower dental midline21, and chin midline2,21,23. Thus, the results in Table 1 showing the treatment outcome of soft tissue midline asymmetry, with the exception of the chin, was favorable when the mean value was ≤2 mm. Although the soft tissue chin midline deviation in skeletal class II showed the greatest improvement (2.97 mm, 52.9%, p < 0.001), noticeable asymmetry (2.64 ± 1.80 mm) was still observed after surgery. This finding of residual chin deviation is consistent with previous OGS studies on different types of malocclusion7,8,9,12,16, suggesting the difficulty in the recognition of facial midline intra-operatively or relapse post-operatively. The present study provided further evidence that the residual chin asymmetry is correlated with the residual shift asymmetry of the mandible, chin, and ramus (Table 2).
The lip cant was insignificantly improved after bimaxillary OGS (0.64 mm, 37.0%, p = 0.013). We found that the mandibular roll asymmetry, rather than the maxillary roll asymmetry, affected the lip cant postoperatively (Table 2). In addition, postoperative mandibular roll asymmetry was not necessarily correlated with postoperative maxillary roll asymmetry (r = 0.35, p = 0.055). In the study by Suzuki-Okumara et al., the preoperative measurements showed the same correlation, in which the preoperative lip cant was correlated with the preoperative mandibular roll asymmetry rather than the maxillary roll asymmetry12. Interestingly, Suzuki-Okumara et al., also reported that the change of lip cant was correlated with the change of the maxillary roll asymmetry, rather than the change of the mandibular roll asymmetry12. Although the present study did not measure the change in roll asymmetry of the maxilla or mandible, many of the OGS studies on lip cant consistently found a significant correlation between the change of lip cant and the change of the maxillary occlusal cant6,10,19. The study by Kim et al. demonstrated the average amount of lip cant correction was approximately 50% of the maxillary occlusal cant correction19. Therefore, in addition to correction of maxillary occlusal cant, correction of mandibular roll asymmetry might also play a role in further restoring lip symmetry.
Residual maxillary and mandibular shift asymmetry were found to be the most important factors influencing the postoperative upper and lower dental midline deviation, respectively. Residual mandibular yaw asymmetry also affected the upper and lower dental midline deviation postoperatively. Residual maxillary yaw asymmetry was found to have no significant influence on residual upper dental midline asymmetry, although mandibular yaw asymmetry was significantly correlated with maxillary yaw asymmetry (r = 0.63, p < 0.001). Song et al. analyzed pre-treatment variables and found that maxillary yaw asymmetry was the primary contributing factor for upper dental midline deviation in patients with upper dental midline deviation greater than 2 mm; however, analysis of mandibular variables was not shown22. Ryu et al. also analyzed pre-treatment variables and found that upper dental midline deviation was not significantly correlated with mandibular roll or yaw asymmetry, and lower dental midline deviation was significantly correlated with mandibular yaw asymmetry24. The possible reasons for the discordant findings about influencing factors for upper dental midline deviation include heterogeneity of samples (class III asymmetry vs. class II asymmetry), different variables for positional jaw asymmetry (line vs. plane), and the intervention of surgical-orthodontic treatment (no vs. yes).
The midline deviation of the nose became more severe after surgery (Table 1). This could be explained by the shift asymmetry of the maxilla after surgery (Table 2). Sacrifice of the nasal and maxillary symmetry has also been shown to achieve favorable mandibular and overall facial symmetry25. Despite the deterioration, the mean residual midline deviation of the nose was less than 1 mm, which is usually clinically acceptable2,21,22.
This study has some limitations. First, the degree of facial asymmetry in patients with class II deformities is usually modestly remarkable and consequently the sample size of this study was small. Studies with larger sample size are needed to draw more robust conclusions. Second, the occlusal plane cant, which might play an important role on mandibular shift and chin deviation, was not measured. Finally, no size influence of soft tissue or jaws was analyzed. Future studies are needed to explore the impact of occlusal cant, soft and hard tissue volume on the treatment outcome of facial asymmetry.
Conclusions
The findings of the present study showed bimaxillary OGS for patients with class II asymmetry significantly improved the midline asymmetry of the chin, mandible, and lower incisors. However, noticeable chin deviation was still observed after surgery, which was affected by the residual shift asymmetry of the mandible, chin, and ramus. The contour asymmetry was not significantly improved after surgery, which was affected by the initial severity of contour asymmetry, and the residual roll or yaw asymmetry of the ramus. Maxillary shift asymmetry was the primary factor influencing the postoperative midline deviation of the nose, upper lip, and upper incisors. Mandibular shift asymmetry was the primary factor influencing the postoperative midline deviation of the lower lip, mandible, chin, and lower incisors.
Material and Methods
Patients
The retrospective study was conducted in accordance with the World Medical Association Declaration of Helsinki on medical research ethics. The approval of the study was granted by the Ethics Committee for Human Research at the Chang Gung Memorial Hospital in Taoyuan, Taiwan. The need for informed consent was waived by the Ethics Committee that approved the study due to the retrospective design of the study. Thirty Taiwanese adults (age ≥18 years) with class II deformity (A point–nasion–B point angle >4 degrees) and significant facial asymmetry (skeletal menton deviation >2 mm or lip cant >2 mm or significant contour asymmetry) were selected based on the following criteria: (1) consecutive Le Fort I osteotomy and bilateral sagittal split osteotomy (BSSO) advancement surgery by the attending surgeons supervised by one senior surgeon with more than 40 years of experience at the Chang Gung Craniofacial Center during a 3-year period, (2) completion of postsurgical orthodontic treatment, (3) no progressive or chronic temporomandibular joint disorder, (4) no other craniofacial deformities or genetic syndromes, (5) no history of craniofacial surgery or trauma, and (6) available CBCT taken at two time points, before surgery and at least 12 months after surgery, on the day of orthodontic debonding. The informed consent for publication of identifying information/images in an online open-access publication was obtained from the patient whose images were displayed.
Surgical technique
The BSSO was modified from Hunsuck26 by extending the anterior cut of the osteotomy to the first molar27,28. The Le Fort I osteotomy was performed with a technique similar to that popularized by Bell29. No additional surgical intervention other than genioplasty was performed. Rigid fixation was performed with bone plates or screws. On average, the anterior maxilla (incisive foramen) moved backward (1.16 mm), upward (2.36 mm), and toward the opposite side (opposite to menton-deviated side, 0.23 mm). The posterior maxilla (greater palatine foramen) moved forward (0.49 mm and 0.61 mm, respectively for the deviated and opposite sides), upward (0.74 mm and 1.93 mm, respectively for the deviated and opposite sides), and toward the opposite side (0.11 mm and 0.25 mm, respectively for the deviated and opposite sides). The anterior mandible (genial tubercle) moved forward (3.87 mm) and toward the opposite side (2.13 mm). The posterior mandible (mental foramen) moved forward (2.86 mm and 3.04 mm, respectively for the deviated and opposite sides), downward (2.31 mm and 0.95 mm, respectively for the deviated and opposite sides), and toward the opposite side (2.23 mm and 1.28 mm, respectively for the deviated and opposite sides).
CBCT
CBCT of the head and neck was performed using an i-CAT 3D Dental Imaging System (Imaging Sciences International, Hatfield, PA, USA) with the following parameters: 120 kVp, 0.4 mm × 0.4 mm × 0.4 mm voxel size, 40 second scan time, and 16 cm × 16 cm field of view. The patient’s head was positioned with the Frankfort horizontal plane parallel to the ground. Throughout the scan, patients were asked not to swallow.
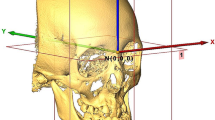
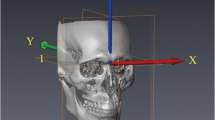
Images were stored in the Digital Imaging and Communications in Medicine (DICOM) format and then transferred to a workstation (Avizo v7.0.0 software, FEI, Mérignac, France) where they were rendered into volumetric images, segmented and analyzed by one single investigator (CYF) blinded to the patients’ treatment histories. Before analysis, six skeletal landmarks were selected for registration of the 3D images in a 3D coordinate system (x, y, z) given in millimeters with nasion as the zero point: nasion, bilateral porion, bilateral orbitale, and basion. The horizontal reference plane was parallel with the FH plane (the best-fit plane passing through bilateral porion and orbitale) and passing through nasion. The midsagittal plane was perpendicular to the horizontal reference plane and passing through nasion and basion. The coronal reference plane was perpendicular to the horizontal and midsagittal reference planes and passing through nasion. A positive value indicates the left, posterior and superior side of the face. After registration of the 3D images, landmarks30,31,32 and planes used for measurement (Tables 3 and 4, and Figs. 1 and 2) were located on the 3D surface models by the same investigator. Multiplanar reconstruction views were also used to identify the landmarks when necessary.

Landmarks used for asymmetry outcome analysis. (a) Soft tissue landmarks: Sn, subnasale; Ls, labiale superius; Li, labiale inferius; B’, soft tissue B point; Me’, soft tissue menton; ChR, cheilion right; ChL, cheilion left; cSnR, contour Sn point right; cSnL, contour Sn point left; cLsR, contour Ls point right; cLsL, contour Ls point left; cStoR, contour Sto point right; cStoL, contour Sto point left; cLiR, contour Li point right; cLiL, contour Li point left; cB’R, contour B’ point right; cB’L, contour B’ point left; cPg’R, contour Pg’ point right; cPg’L, contour Pg’ point left. (b) Dental landmarks: UIE, upper incisal embrasure; LIE, lower incisal embrasure.

Landmarks and planes used for positional jaw asymmetry analysis. (a) Maxillary central plane: ANS, anterior nasal spine; IF, incisive foramen; PNS, posterior nasal spine. (b) Mandibular central plane: mGT, genial tubercle midpoint; sGT, genial tubercle superius; LBs, lower border points. (c) Chin central plane: Me, menton; lCR, lateral chin point right; lCL, lateral chin point left. (d) Ramal plane right: SPR, sigmoid point right; ARPR, anterior ramal point right; PRPR, posterior ramal point right. Ramal plane left: SPL, sigmoid point left; ARPL, anterior ramal point left; PRPL, posterior ramal point left. The inscribed circle (red) within the ramus was used to define the tangents of SPR, ARPR and PRPR.
Asymmetry outcome
To demonstrate the extent of asymmetry before and after surgery, absolute values of the following measurements for soft tissue and dental asymmetry were used. Real values were used for regression analysis.
Soft tissue asymmetry: midline and contour asymmetry
-
(1)
Midline asymmetry:
- (a)
Midline deviation: the transverse distances between midline landmarks of Sn, Ls, Li, B’, Me’ and the midsagittal plane (MSP) were measured as the midline deviation of the nose, upper lip, lower lip, mandible, and chin, respectively (Table 3).
- (b)
Lip cant: the vertical distance between bilateral landmarks of Ch was measured as the lip cant.
- (a)
-
(2)
Contour asymmetry: the discrepancy in transverse distances of bilateral contour landmarks at the same level from the MSP
- (a)
Upper contour asymmetry: the summation of contour asymmetry at Sn level and Ls level.
- (b)
Middle contour asymmetry: the summation of contour asymmetry at Sto level and Li level.
- (c)
Lower contour asymmetry: the summation of contour asymmetry at B’ level and Pg’ level.
- (a)
Dental asymmetry: midline asymmetry
-
(1)
Midline asymmetry:
- (a)
Midline deviation: the transverse distances between the midline landmarks of UIE and LIE and the MSP were measured as the midline deviation of the upper incisors and lower incisors (Table 3).
- (a)
Influencing factors
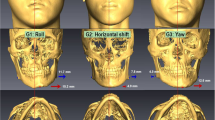
The possible influencing factors for residual asymmetry included preoperative asymmetry and postoperative positional jaw asymmetry in terms of shift, roll or yaw asymmetry. To evaluate the positional jaw asymmetry, we first defined five planes (maxillary central plane, mandibular central plane, chin central plane, and bilateral ramal planes) for each osteotomy segment (Table 4). Then, the discrepancy of the five planes from the reference planes was calculated to quantify the shift, roll or yaw asymmetry of the maxilla, mandible, chin and ramus (Table 5). Figure 3 is an example of a patient showing positional jaw asymmetry after bimaxillary surgery: (a) Maxilla: shift asymmetry (ANS deviation) of −0.96 mm, roll asymmetry of −2.99 degrees, and yaw asymmetry of +1.59 degrees. (b) Mandible: shift asymmetry (mGT deviation) of +2.74 mm, roll asymmetry of +2.53 degrees, and yaw asymmetry of +0.44 degrees. (c) Chin: shift asymmetry (Me deviation) of +2.57 mm, roll asymmetry of +5.41 degrees, and yaw asymmetry of −1.34 degrees. (d) Ramus: shift asymmetry (discrepancy in transverse distances of SPR and SPL from the MSP) of −0.44 mm, roll asymmetry of +2.51 degrees, and yaw asymmetry of −1.21 degrees.

Example of a patient showing positional jaw asymmetry after bimaxillary surgery. (a) Maxilla: ANS, anterior nasal spine (b) Mandible: mGT, genial tubercle midpoint. (c) Chin: Me, menton. (d) Ramus: SPR, sigmoid point right; SPL, sigmoid point left.
Reliability
To assess intra-examiner reliability, all CBCT measurements were repeated by the same investigator for 10 randomly chosen patients one month after the initial session. Intra-examiner reliability, analyzed by the intraclass correlation coefficient (ICC), was excellent (mean ICC, 0.962; 95 percent confidence interval, 0.938 to 0.978).
Statistical analysis
Statistical analyses were performed using the statistical software package SPSS version 19.0 for Windows (SPSS Inc, Chicago, USA). All descriptive statistics are presented as mean ± standard deviation (SD). Paired t test was used to compare the difference in facial asymmetry before and after surgery. To identify the influencing factors for residual asymmetry, stepwise multiple linear regression analysis was used with the postoperative soft tissue and dental asymmetry as the dependent variables and the preoperative soft tissue and dental asymmetry and the postoperative positional asymmetry of the osteotomy segments as the independent variables. To account for multiple comparison, p ≤ 0.01 was considered statistically significant.
Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Cheong, Y. W. & Lo, L. J. Facial asymmetry: Etiology, evaluation, and management. Chang Gung Med J 34, 341–351 (2011).
Cevidanes, L. H. et al. Three-dimensional quantification of mandibular asymmetry through cone-beam computerized tomography. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 111, 757–770, https://doi.org/10.1016/j.tripleo.2011.02.002 (2011).
Baek, C., Paeng, J. Y., Lee, J. S. & Hong, J. Morphologic evaluation and classification of facial asymmetry using 3-dimensional computed tomography. J Oral Maxillofac Surg 70, 1161–1169, https://doi.org/10.1016/j.joms.2011.02.135 (2012).
Ackerman, J. L., Proffit, W. R., Sarver, D. M., Ackerman, M. B. & Kean, M. R. Pitch, roll, and yaw: Describing the spatial orientation of dentofacial traits. Am J Orthod Dentofacial Orthop 131, 305–310, https://doi.org/10.1016/j.ajodo.2006.05.032 (2007).
Ferrario, V. F., Sforza, C., Schmitz, J. H. & Santoro, F. Three-dimensional facial morphometric assessment of soft tissue changes after orthognathic surgery. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 88, 549–556 (1999).
Bergeron, L., Yu, C. C. & Chen, Y. R. Single-splint technique for correction of severe facial asymmetry: Correlation between intraoperative maxillomandibular complex roll and restoration of mouth symmetry. Plast Reconstr Surg 122, 1535–1541, https://doi.org/10.1097/PRS.0b013e31818820d8 (2008).
Yu, C. C., Bergeron, L., Lin, C. H., Chu, Y. M. & Chen, Y. R. Single-splint technique in orthognathic surgery: Intraoperative checkpoints to control facial symmetry. Plast Reconstr Surg 124, 879–886, https://doi.org/10.1097/PRS.0b013e3181b03842 (2009).
Ko, E. W., Huang, C. S. & Chen, Y. R. Characteristics and corrective outcome of face asymmetry by orthognathic surgery. J Oral Maxillofac Surg 67, 2201–2209, https://doi.org/10.1016/j.joms.2009.04.039 (2009).
Verze, L., Bianchi, F. A., Schellino, E. & Ramieri, G. Soft tissue changes after orthodontic surgical correction of jaws asymmetry evaluated by three-dimensional surface laser scanner. J Craniofac Surg 23, 1448–1452, https://doi.org/10.1097/SCS.0b013e31824e25fc (2012).
Kim, S. J., Choi, J. Y. & Baek, S. H. Evaluation of canting correction of the maxillary transverse occlusal plane and change of the lip canting in Class III two-jaw orthognathic surgery. Angle Orthod 82, 1092–1097, https://doi.org/10.2319/011512-36.1 (2012).
Hagensli, N., Stenvik, A. & Espeland, L. Asymmetric mandibular prognathism: Outcome, stability and patient satisfaction after BSSO surgery. A retrospective study. J Craniomaxillofac Surg 42, 1735–1741, https://doi.org/10.1016/j.jcms.2014.06.008 (2014).
Suzuki-Okamura, E., Higashihori, N., Kawamoto, T. & Moriyama, K. Three-dimensional analysis of hard and soft tissue changes in patients with facial asymmetry undergoing 2-jaw surgery. Oral Surg Oral Med Oral Pathol Oral Radiol 120, 299–306, https://doi.org/10.1016/j.oooo.2015.05.020 (2015).
Lee, G. C., Yoo, J. K., Kim, S. H. & Moon, C. H. Lip line changes in Class III facial asymmetry patients after orthodontic camouflage treatment, one-jaw surgery, and two-jaw surgery: A preliminary study. Angle Orthod 87, 239–245, https://doi.org/10.2319/033016-254.1 (2017).
Chen, Y. J. et al. A new classification of mandibular asymmetry and evaluation of surgical-orthodontic treatment outcomes in Class III malocclusion. J Craniomaxillofac Surg 44, 676–683, https://doi.org/10.1016/j.jcms.2016.03.011 (2016).
Chew, M. T. Spectrum and management of dentofacial deformities in a multiethnic Asian population. Angle Orthod 76, 806–809, https://doi.org/10.1043/0003-3219(2006)076[0806:Samodd]2.0.Co;2 (2006).
Hajeer, M. Y., Ayoub, A. F. & Millett, D. T. Three-dimensional assessment of facial soft-tissue asymmetry before and after orthognathic surgery. Br J Oral Maxillofac Surg 42, 396–404, https://doi.org/10.1016/j.bjoms.2004.05.006 (2004).
Thiesen, G., Gribel, B. F., Freitas, M. P. M., Oliver, D. R. & Kim, K. B. Mandibular asymmetries and associated factors in orthodontic and orthognathic surgery patients. The Angle Orthodontist 88, 545–551, https://doi.org/10.2319/111517-785.1 (2018).
Blockhaus, M., Kochel, J., Hartmann, J., Stellzig-Eisenhauer, A. & Meyer-Marcotty, P. Three-dimensional investigation of facial surface asymmetries in skeletal malocclusion patients before and after orthodontic treatment combined with orthognathic surgery. J Orofac Orthop 75, 85–95, https://doi.org/10.1007/s00056-013-0200-x (2014).
Kim, Y. H., Jeon, J., Rhee, J. T. & Hong, J. Change of lip cant after bimaxillary orthognathic surgery. J Oral Maxillofac Surg 68, 1106–1111, https://doi.org/10.1016/j.joms.2009.07.030 (2010).
Choi, J. W. et al. Frontal soft tissue analysis using a 3 dimensional camera following two-jaw rotational orthognathic surgery in skeletal class III patients. J Craniomaxillofac Surg 42, 220–226, https://doi.org/10.1016/j.jcms.2013.05.004 (2014).
Haraguchi, S., Takada, K. & Yasuda, Y. Facial asymmetry in subjects with skeletal Class III deformity. Angle Orthod 72, 28–35, 10.1043/0003-3219(2002)072<0028:Faisws>2.0.Co;2 (2002).
Song, W. W., Kim, S. S., Sandor, G. K. & Kim, Y. D. Maxillary yaw as the primary predictor of maxillary dental midline deviation: 3D analysis using cone-beam computed tomography. J Oral Maxillofac Surg 71, 752–762, https://doi.org/10.1016/j.joms.2012.07.043 (2013).
Kim, J. Y., Jung, H. D., Jung, Y. S., Hwang, C. J. & Park, H. S. A simple classification of facial asymmetry by TML system. J Craniomaxillofac Surg 42, 313–320, https://doi.org/10.1016/j.jcms.2013.05.019 (2014).
Ryu, H. S., An, K. Y. & Kang, K. H. Cone-beam computed tomography based evaluation of rotational patterns of dentofacial structures in skeletal Class III deformity with mandibular asymmetry. Korean J Orthod 45, 153–163, https://doi.org/10.4041/kjod.2015.45.4.153 (2015).
Chen, Y. F., Liao, Y. F., Chen, Y. A. & Chen, Y. R. Treatment outcome of bimaxillary surgery for asymmetric skeletal class II deformity. Clin Oral Investig 23, 623–632, https://doi.org/10.1007/s00784-018-2462-6 (2019).
Hunsuck, E. E. A modified intraoral sagittal splitting technic for correction of mandibular prognathism. J Oral Surg 26, 250–253 (1968).
Honda, T., Lin, C. H., Yu, C. C., Heller, F. & Chen, Y. R. The medial surface of the mandible as an alternative source of bone grafts in orthognathic surgery. J Craniofac Surg 16, 123–128; discussion 128 (2005).
Chen, Y. A., Ng, L. S., Ko, E. W. & Chen, Y. R. Mandibular contouring during orthognathic surgery using the modified Hunsuck technique. J Craniofac Surg 28, 239–240, https://doi.org/10.1097/scs.0000000000003165 (2017).
Bell, W. H. Modern Practice in Orthognathic and Reconstructive Surgery. (Saunders 1992).
Swennen, G. R. J., Schutyser, F. A. C. & Hausamen, J. E. Three-Dimensional Cephalometry: A Color Atlas and Manual. (Springer, 2005).
Kim, T. Y. et al. Determination of midsagittal plane for evaluation of facial asymmetry using three-dimensional computed tomography. Imaging Sci Dent 41, 79–84, https://doi.org/10.5624/isd.2011.41.2.79 (2011).
Lee, S. Y., Choi, D. S., Jang, I., Song, G. S. & Cha, B. K. The genial tubercle: A prospective novel landmark for the diagnosis of mandibular asymmetry. Korean J Orthod 47, 50–58, https://doi.org/10.4041/kjod.2017.47.1.50 (2017).
Acknowledgements
The work was supported by the Chang Gung Memorial Hospital, Taiwan (CMRPG5F0052, CMRPG5F0062).
Author information
Authors and Affiliations
Contributions
Y.-F. Chen: collection, analysis of data, and drafting manuscript submissions. Y.-F. Liao: conception, analysis, interpretation of data, and revision of manuscript submissions. Y.-A. Chen: collection of data and revision of manuscript submissions. Y.-R. Chen: collection of data and revision of manuscript submissions
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Chen, YF., Liao, YF., Chen, YA. et al. Surgical-orthodontic treatment for class II asymmetry: outcome and influencing factors. Sci Rep 9, 17956 (2019). https://doi.org/10.1038/s41598-019-54317-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-019-54317-5
- Springer Nature Limited
This article is cited by
-
Site and severity of facial asymmetry after bimaxillary surgery for class III deformity: a case-control study
Clinical Oral Investigations (2024)
-
Is the pattern of mandibular asymmetry in mild craniofacial microsomia comparable to non-syndromic class II asymmetry?
Clinical Oral Investigations (2022)