
Abstract
Factors associated with infections after spinal cord surgery were not fully understood. This study aimed to evaluate whether preoperative pressure ulcers was a risk factor of infections after spinal cord operation. A 1:1 matched follow-up study was performed in a tertiary referral center in southwest China between 2010 and 2015. Risk ratios (RRs) and 95% confidence intervals (CIs) were calculated using unconditional logistic regression analysis. A total of 334 patients with spinal cord surgery were recruited (167 patients with preoperative pressure ulcers and 167 patients without preoperative pressure ulcers). Participants previously exposed to pressure ulcers had an elevated risk of infections post spinal cord operation including surgical site infection (RR: 2.3, 95% CI: 1.1, 4.7), pneumonia (RR: 2.4, 95% CI: 1.1,5.3), urinary tract infection (RR: 2.8, 95% CI: 1.1, 7.3), any kinds of postoperative infections (RR: 3.4, 95% CI: 2.1, 5.6) and 30-day postoperative hospitalization for infections (RR: 2.6, 95% CI: 1.1, 6.0). The associations between preoperative pressure ulcers in stage III to IV and postoperative infections were also pronounced, but towards null in stage I to II. The study showed an increased risk of infections after spinal cord surgery in patients with preoperative pressure ulcers, indicative of an urgent need for monitoring postoperative infections and medical treatment for patients with pressure sores.
Similar content being viewed by others


Introduction
Spinal cord injury (SCI) remains a devastatingly neurologic disease worldwide1,2. Factors affecting infections after spinal cord surgery might include old age, operation time, preoperative infection, malnutrition and etc.3. Infections after spinal cord surgery may increase hospital stay length, mortality rates and poor quality of life, which added health-care costs and financial burden to families and societies4. Due to antibiotic resistant pathogens in hospital-associated infections, it highlights the importance of preventing risk factors of infection in patients with spinal cord operation5.
Pressure ulcer is a set of complications which are featured with damage and defect of skin tissue4. In United States, there were 1.3–3 million patients suffering from pressure ulcer in 2003 and 20136,7. Patients with pressure sores were considered to have an elevated risk of inflammation, infection and mortality8,9. Recently, a retrospective cohort study revealed that patients with preoperative pressure sores were considered to have an increased risk of adverse outcomes (including postoperative infection) after major surgery (including spinal cord operation)10, indicative of a potential risk factor to infections after spinal cord surgery. The retrospective cohort study, however, did not illustrate specific effect of preoperative pressure sores on patients who underwent spinal cord operation, making the association inconclusive.
Thus, we performed a 1:1 matched follow-up study to evaluate the association between preoperative pressure sores and infections after spinal cord surgery. A total of 334 participants were recruited and impact of preoperative pressure sores on various postoperative infections of spinal cord in patients was analyzed.
Results
Selection and characteristics of participants
A total of 1276 patients who were newly diagnosed SCI within 3 months had operation treatments during January 1, 2010 and December 31, 2015 at the Affiliated Hospital of Guizhou Medical University in China. A total of 334 individuals were recruited, among which 167 patients with decubitus ulcers were the exposures and 167 patients free to decubitus ulcers were the controls (Fig. 1). Data regarding 161 pairs of the exposures and the controls were used for the final analysis since 4 individuals in case group and 2 in control group were lost to follow-up. Among the eligible participants, the mean age was 53.4 ± 7.8 years. There were 55.3% male participants in both groups. Other main characteristics including SCI level, operation procedure and cause for SCI of eligible participants are summarized in Table 1.

Flowchart exhibiting the selection of eligible individuals in the follow-up study.
Potential causes for pressure ulcers and its location
We comprehensively reviewed the potential causes for pressure ulcers in participants. Fracture, as the primary cause for pressure ulcers, was accounting for 84.5% (136/161), in particular hip fracture (97/161). Other potential causes for pressure sores included arthritis, cerebral trauma and etc. (Table 2). As for location of pressure ulcers in human body, there were 60.2% (97/161) reports in sacrococcygeal region, 8.7% (14/161) in heel, 7.4% (12/161) in iliac crest, 6.3%(10/161) in greater trochanter, 4.9% (8/161) in ankle, 3.0%(5/161) in ischial tuberosity and 6.3%(10/161) in other regions.
Infections risk in relation to preoperative pressure ulcers
Compared with control group, a 3.4-fold (95%CI, 2.1–5.6) increased risk of any kinds of postoperative infections within 14 days was observed in patients with preoperative pressure ulcers (Table 3). The positive association was also pronounced with regard to the specific kinds of infections. RRs for surgical site infection, pneumonia, urinary tract infection were 2.3 (95%CI, 1.1–4.7), 2.4 (95%CI, 1.1–5.3), and 2.8 (95%CI, 1.1–7.3), respectively. After adjusted for possible confounding risk factors, the RR values remained to be statistically significant. Pressure ulcers were also associated with an elevated risk of 30-day postoperative hospitalization for infection (RR, 2.6, 95%CI, 1.1–6.0). However, such positive effects disappeared in septicemia or deep vein infection.
Infections risk in relation to different stages of preoperative pressure ulcers
In terms of various severity degrees of pressure sores, associations between pressure ulcer in either stage III or stage IV and infections post spinal cord surgery were statistically significant but non-significant in stage I or stage II. The highest RR was observed in pressure ulcers of stage IV. In respect to pressure sores of stage IV, RR for 14-day postoperative infection was 4.2 (95%CI, 2.3–6.7) and RR for 30-day postoperative hospitalization for infection was 3.2 (95%CI, 2.0–6.4). The associations were also pronounced after adjusting for the aforementioned specific parameters (Table 4).
Discussion
To our best understanding, this is the first study suggesting an elevated infection risk after spinal cord surgery in patients with preoperative pressure ulcers in mainland China. Compared to controls, patients with preoperative pressure sores had a 3.4-fold increased risk of postoperative infections within 14 days and a 2.6-fold increased risk of 30-day postoperative hospitalization for infection. The higher risk of postoperative infections in pressure sore of stage III to IV was identified. The current study suggests a warning to give medical treatment for patients with pressure sores before spinal cord surgery, in particular those with pressure sore of stage III to IV. What is more, it should pay attention to make measures to control postoperative infections.
Several plausible mechanisms might be accounting for increasing risk of infections post spinal cord infections in relation to prior pressure sore exposures. To start with, pressure sores were perceived to induce impairment of skin protection function by destroying integrity of erythematous skin and prompting reproduction and growth of pathogenic bacteria11. Several species of pathogenic bacteria including Staphylococcus, Pseudomonas, Peptoniphilus, Enterobacter, Stenotrophomonas, Finegoldia, and Serratia were detected in collected samples from pressure sores12. Pressure ulcers might introduce possible resources and entrances of pathogens to human body, which was possible to result in local infections in human body. Secondly, chronic pressure ulcers were supposed to persist chronic inflammation, which might lead to stimulation of cytokines and inflammation factors12,13,14. An expansive literature suggest that long-term and excessive consumption of cytokines and inflammation factors might be accounting for immune suppression, and in turns led to a weaken ability to prevent invasions and attacks of pathogens15,16. Thirdly, immobilization, as a primary risk factor for the occurrence and development of pressure sores17,18, was considered to be associated with pneumonia. Immobilization might have destructive effects on removing function of bronchial secretions, which was conductive to reproduction of pathogen and help to result in pneumonia. However, mechanisms about association between preoperative pressure sores and infections post spinal cord surgery are still not conclusive.
This study demonstrates an increased risk of several specific infections (surgical incision infection, pneumonia, urinary tract infection) within 14-day after spinal cord operation in patient with pressure sores preoperatively. Our finding is in line with a retrospective cohort study which showed an increased risk of pneumonia and urinary tract infections after several major operative treatments including skin, breast, spinal cord surgery and etc. in relation to preoperative pressure sores10. However, pressure ulcer was neither associated with septicemia nor deep vein infection. What the aforementioned hints that pressure sore might be more easily introduce superficial infections to human body. The possible mechanisms might be involved in migration of pathogen from pressure ulcer to superficial areas.
Patients with different stages of pressure ulcer showed various risk of infections post spinal cord operation. Our finding indicates an elevated risk of either 14-day postoperative infections or 30-day postoperative hospitalization for infection in patient with preoperative pressure ulcers of stage III to IV, however, the elevated risk was towards to null in pressure ulcer of stage I to II. Based on the integrity of erythematous skin and the involved depth of wound, pressure sore of stage I present with intact epidermis, while stage II to IV with skin defect at different levels19. Among the four stages of pressure ulcer, stage IV has the highest risk of postoperative infections (Table 4). What the aforementioned suggest a possible dose-response relationship between degree stages of postoperative pressure sores and risk of infections after spinal cord operation. Previous studies showed that there were open wounds, endothelial cell dysfunction, abscess and cellulitis in pressure sores from stage II to IV, which made colony, invasion and infection of bacteria more easily20,21.
Even though our analysis was on basis of a follow-up study and results were relatively robust, there were some potential limitations which should be discussed. First of all, specific species of bacteria in wounds of pressure sores or postoperative infections were not detected. Whether postoperative infection resources came from pressure sores was not verified. What is more, the impact of pressure sores occurrence post spinal cord surgery on postoperative infections was not evaluated. According to statistics, morbidity of pressure sore was high among patients post surgical procedures of spinal cord22, while occurrences of pressure sores were inconsistent in disease course. Owing to the limited participants, such analysis was failed to conduct. In addition, the study might not avoid affecting by confounding bias. Some factors such as lifestyle, family support, nutrition and etc. have involvement in development of infections23. Although we have adjusted several factors for analysis, potential effect of other confounders might remain.
Conclusions
This follow-up study based on 167 pair of cases and controls demonstrated a positive association between preoperative pressure sores and infections after spinal cord surgery. Preoperative pressure sores might be a risk factor for infections after spinal cord surgery, especially in patients with pressure sore in stage III to IV. In consideration of limited number of participants in this study, additional studies, in particular perspective cohort studies based on population are needed to confirm the impact of preoperative pressure sores on postoperative infections.
Methods
Study design
A 1:1 matched follow-up study was conducted. Patients with pressure ulcers were consecutively recruited as the exposures according to inclusion criteria as follow: (1) ≥18 years and capable of communicating and providing information; (2) new diagnosis for SCI within 3 months; (3) diagnosis for pressure sores at least two weeks before SCI; (4) without severe medical co-morbidities including cancer, cardiovascular disease, mental disorder or severe infection over the last two months. For each exposures, control was selected among the clinic patients who were free of pressure ulcers and matched by sex, age (±3 years) with the specific case. Both case and control group underwent operation of spinal cord. The protocol was performed in accordance with the research ethics principles of the Committee of Guizhou Medical University. Written informed consents of this study were obtained from all participants.
Exposures
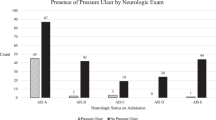
Patients with SCI were identified according to the ninth revision of the International Classification Diseases (ICD) for SCI (ICD-9-CM 806). Afterwards, spinal cord impairments were quantified into four levels (A, B, C, D) by the American Spinal Injury Association Impairment Scale (AIS)24. Patients received various surgical procedures including anterior cervical surgery, posterior cervical surgery and combined cervical surgery according to their injured sites and severity. Cases with pressure ulcers were initially classified on basis of ICD-9-CM 707.0 and severity levels of pressure sores were graded into four stages (stage I to IV) using the National Pressure Ulcer Advisory Panel18. Characteristic information of participants was collected with a designed questionnaire. Causes of pressure sores in the exposure group were comprehensively studied.
Outcomes
Postoperative infections within 14 days, including surgical site infection (ICD-9-CM E878), pneumonia (ICD-9-CM 480-486), urinary tract infection (ICD-9-CM 599.0), deep vein infection (ICD-9-CM 958.3), septicemia (ICD-9-CM 038, 998.5), were regarded as primary outcomes. Secondary outcome was 30-day postoperative hospitalization for infection.
Statistical analysis
Risk ratios (RRs) and their corresponding 95% confidence intervals (CIs) for associations between pressure ulcers and risk of infections after spinal cord operation were calculated by unconditional logistic regression analysis after adjusting for sex, age. Additionally, Subgroup analysis was conducted, which stratified by pressure ulcer degree (stage I to IV). All statistical analysis was conducted using SPSS 13.0 software (SPSS Inc., Chicago, IL, USA). Statistical tests in this study were 2-sided and a P value < 0.05 for statistically significance was used.
References
Zakrasek, E. C., Creasey, G. & Crew, J. D. Pressure ulcers in people with spinal cord injury in developing nations. Spinal Cord 53, 7–13 (2015).
Kruger, E. A., Pires, M., Ngann, Y., Sterling, M. & Rubayi, S. Comprehensive management of pressure ulcers in spinal cord injury: current concepts and future trends. J Spinal Cord Med 36, 572–585 (2013).
Guihan, M. & Bombardier, C. H. Potentially modifiable risk factors among veterans with spinal cord injury hospitalized for severe pressure ulcers: a descriptive study. J Spinal Cord Med 35, 240–250 (2012).
Shahin, E. S., Dassen, T. & Halfens, R. J. Pressure ulcer prevalence and incidence in intensive care patients: a literature review. Nurs Crit Care 13, 71–79 (2008).
Martin, E. T. et al. Diabetes and Risk of Surgical Site Infection: A Systematic Review and Meta-analysis. Infect Control Hosp Epidemiol 37, 88–99 (2016).
Chou, R. et al. Pressure ulcer risk assessment and prevention: a systematic comparative effectiveness review. Ann Intern Med 159, 28–38 (2013).
Lyder, C. H. Pressure ulcer prevention and management. JAMA 289, 223–226 (2003).
Flattau, A. & Blank, A. E. Risk factors for 90-day and 180-day mortality in hospitalized patients with pressure ulcers. Int Wound J 11, 14–20 (2014).
Ammons, M. C. et al. Biochemical association of metabolic profile and microbiome in chronic pressure ulcer wounds. PLOS One 10, e0126735 (2015).
Chou, C. L. et al. Adverse outcomes after major surgery in patients with pressure ulcer: a nationwide population-based retrospective cohort study. PLOS One 10, e0127731 (2015).
Schario, M. et al. Effects of two different fabrics on skin barrier function under real pressure conditions. J Tissue Viability 26, 150–155 (2017).
Rahim, K. et al. Bacterial Contribution in Chronicity of Wounds. Microb Ecol 73, 710–721 (2017).
Romana-Souza, B., Santos, J. S., Bandeira, L. G. & Monte-Alto-Costa, A. Selective inhibition of COX-2 improves cutaneous wound healing of pressure ulcers in mice through reduction of iNOS expression. Life Sci 153, 82–92 (2016).
Kurose, T., Hashimoto, M., Ozawa, J. & Kawamata, S. Analysis of Gene Expression in Experimental Pressure Ulcers in the Rat with Special Reference to Inflammatory Cytokines. PLOS One 10, e0132622 (2015).
Jiang, L. et al. Expression of cytokines, growth factors and apoptosis-related signal molecules in chronic pressure ulcer wounds healing. Spinal Cord 52, 145–151 (2014).
Bonnefoy, M., Coulon, L., Bienvenu, J., Boisson, R. C. & Rys, L. Implication of cytokines in the aggravation of malnutrition and hypercatabolism in elderly patients with severe pressure sores. Age Ageing 24, 37–42 (1995).
Nemunaitis, G. et al. The Effect of a Liner on the Dispersion of Sacral Interface Pressures during Spinal Immobilization. Assist Technol 27, 9–17 (2015).
Coleman, S. et al. Patient risk factors for pressure ulcer development: systematic review. Int J Nurs Stud 50, 974–1003 (2013).
Pressure ulcers prevalence, cost and risk assessment: consensus development conference statement–The National Pressure Ulcer Advisory Panel. Decubitus 2, 24–28 (1989).
Lee, S. Y. et al. Outcomes after Stroke in Patients with Previous Pressure Ulcer: A Nationwide Matched Retrospective Cohort Study. J Stroke Cerebrovasc Dis 25, 220–227 (2016).
Ortiz, B. J. et al. Microbiology of pressure and vascular ulcer infections. Rev Esp Geriatr Gerontol 50, 5–8 (2015).
Singh, R. et al. Surgery for pressure ulcers improves general health and quality of life in patients with spinal cord injury. J Spinal Cord Med 33, 396–400 (2010).
Meng, F., Cao, J. & Meng, X. Risk factors for surgical site infections following spinal surgery. J Cline Neurosci 22, 1862–1866 (2015).
Marino, R. J., Ditunno, J. J., Donovan, W. H. & Maynard, F. J. Neurologic recovery after traumatic spinal cord injury: data from the Model Spinal Cord Injury Systems. Arch Phys Med Rehabil 80, 1391–1396 (1999).
Acknowledgements
This study was funded by the Guizhou provincial Science & Technology Cooperation Program (grant no. 2016LH7234).
Author information
Authors and Affiliations
Contributions
Q.L. and L.L.Y. conceptualised the study; L.L.Y. compiled the figures and wrote the manuscript; L.L.Y., W.X.P. analysed and interpreted the raw data. Q.L. and C.Q.W. reviewed and edited the final manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Yang, Ll., Peng, Wx., Wang, Cq. et al. Elevated Risk of Infections after Spinal Cord Surgery in Relation to Preoperative Pressure Ulcers: a Follow-up Study. Sci Rep 8, 14027 (2018). https://doi.org/10.1038/s41598-018-32157-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-018-32157-z
- Springer Nature Limited