
Abstract
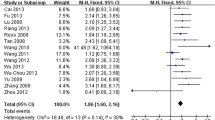
Co-existence of Parkinson’s disease (PD) and essential tremor (ET) may reflect overlapping pathophysiology underlying both conditions. Furthermore, PD patients with leucine-rich repeat kinase-2 (LRRK2) mutations may present with ET-like features, suggesting the possibility of common genetic underpinnings. Two common LRRK2 variants, R1398H and N551K, have been shown to be protective in multiple PD cohorts. We hypothesized that R1398H and N551K may show a similar effect in ET. In a case-control study involving 3198 subjects (2680 controls and 518 ET cases), R1398H was detected in 16.6% of ET cases compared to 18.0% in controls (OR = 0.91, 95% CI = 0.71–1.17, p = 0.46); while N551K was detected in 16.5% of ET cases compared to 18.0% of controls (OR = 0.89, 95% CI = 0.69–1.15, p = 0.37). While these results suggest that LRRK2 R1398H or N551K do not appear to modulate the risk of ET, it remains possible that a protective trend for both variants may be present in ET and a much larger sample size is required to identify this.
Similar content being viewed by others

Introduction
Essential tremor (ET) is a common movement disorder characterized mainly by postural and kinetic tremor of the upper extremities. ET and Parkinson’s disease (PD) are two of the most common movement disorders with overlapping clinical features1. Even though twin and family history studies show a high heritability for ET suggesting a strong genetic component for its pathophysiology, efforts to elucidate the genetic underpinnings of ET have only been moderately successful and the genetic determinants of ET remain unclear2,3. Mutations in the leucine-rich repeat kinase-2 (LRRK2) gene are the most common cause of familial PD, and PD patients with LRRK2 mutations have been reported to present initially with an ET-like phenotype4, raising the possibility of a genetic link between PD and ET. Two polymorphic LRRK2 variants rs7133914 (R1398H) and rs7308720 (N551K), both in linkage disequilibrium, were previously reported to confer up to 20% reduction in risk of PD in Chinese patients5, the protective effect of which has been replicated in other Asian cohorts5,6. Furthermore, the LRRK2 N551K-R1398H-K1423K protective haplotype was also reported to have a frequency of >5% in a large Caucasian and Asian series7, with R1398H being the most likely functional variant and its protective effect appearing independent of other SNCA and microtubule-associated tau (MAPT) variants8. Given the possibility of shared genetic links between ET and PD, we conducted a case-control analysis to investigate if the apparent protective effect of the LRRK2 R1398H and N551K variants would similarly be seen in our cohort of patients with ET.
Results
DNA samples from a total of 3198 subjects comprising of 518 ET subjects and 2680 age- and race-matched controls were analysed. Overall, 90.4% were ethnic Chinese, while the rest were of mixed Asian ethnicity. The mean ± SD age of cases and controls was 51.4 ± 20.2 and 52.5 ± 11.5 years respectively, comprising approximately 54.8% men and 45.2% women altogether. The genotype frequencies of both LRRK2 R1398H and N551K in ET and controls is summarized in Table 1. The genotype frequencies of heterozygous R1398H and N551K carriers was not significantly different in ET compared to controls. Five out of 518 ET cases and 21 out of 2680 controls were homozygous for the R1398H variant, while 6 out of 518 ET cases and 22 out of 2680 controls were homozygous for the N551K variant. Genotype frequencies did not vary according to age at onset in ET cases.
Discussion
An association between ET and PD beyond chance co-existence has been widely recognized. Patients with asymmetric, childhood-onset ET who later developed PD, had their PD-related rest tremor typically starting ipsilateral to the side of the more severe ET tremor9. Other overlapping clinical features between ET and PD include bradykinesia, rigidity, and gait disorders along with other non-motor features, making differentiating between both disorders clinically challenging early in the disease course10. Furthermore, several epidemiological studies have demonstrated an association between ET and PD greater than expected in the general population11,12, suggesting the possibility of overlapping molecular and/or genetic links underpinning both diseases.
Despite strong evidence for genetic links in ET with more than half of affected individuals having a positive family history, identifying genes in both monogenic and complex forms of ET has been challenging. Difficulties encountered by ET genetic studies may result from relatively lax diagnostic criteria, lack of biomarkers for ET with high phenocopy rates, and high locus heterogeneity2. Linkage studies conducted in families with ET have reported mutations in ETM2 (essential tremor monogenetic locus 2) and (fused in sarcoma) FUS, while other studies have linked (leucine-rich repeat and Ig domain containing 1) LINGO1, FUS and teneurin transmembrane protein 4 (TENM4) with ET3. Two genome-wide association studies demonstrated association between ET and variants in LINGO1 and (solute carrier family 1 member 2) SLC1A2, with a meta-analysis confirming the association of rs9652490 in LINGO1 with ET2.
Since the discovery of LRRK2 mutations as a major cause of autosomal dominant parkinsonism13, multiple studies have attempted to investigate the role of both rare and common LRRK2 variants in the pathophysiology of PD and other neurodegenerative disorders14,15,16,17. Genetic studies investigating the link between ET and LRRK2 have yielded conflicting results: the LRKK2 I2012T, G2019S and I2020T variants have been found to be rare in Caucasians with ET18, while a comprehensive analysis of the LRRK2 gene found no association of common and rarer LRRK2 mutations or LRRK2 single nucleotide polymorphisms (SNPs) in ET cases or autopsy brain samples19. The common LRRK2 G2385R variant widely shown to be associated with a two-fold increased risk of PD in various Asian populations was not found to be a significant risk factor for ET in our population20. While conversely, a novel LRRK2 Val2390Met mutation was reported in a group of patients with tremor-dominant parkinsonism (TDP) who underwent sequencing of the entire LRRK2 coding region, a notable finding as some patients displayed a clinical phenotype resembling ET converting to PD21. Furthermore, our group previously demonstrated an association between the known PD risk variant LRRK2 R1628P with ET, where R1628P carriers had a two-fold risk of developing ET (OR = 2.20, 95% CI = 1.30–3.73, p = 0.0035)22.
Our group was the first to report the apparent protective effect of LRRK2 variants N551K and R1398H in PD, which has since been replicated in other Asian PD cohorts5,6. Multivariate regression analysis suggest that R1398H and N551K confer a 20% reduction in PD risk independent of the Asian LRRK2 risk variants G2385R and R1628P5. In non-PD cohorts, a non-significant protective trend was also observed for the LRRK2 N551K-R1398H-K1423K haplotype in a clinical Lewy body dementia (DLB) series (OR 0.76, p = 0.061)23. Functional evidence for the protective effect of both variants come from in vitro studies using dopaminergic neuronal lines that revealed both G2385R and R1628P to display increased kinase activity in a toxic gain-of-function manner consistent with dominant missense LRRK2 mutations, while the protective R1398H variant, on the other hand, displayed reduced extrinsic kinase activity5. Furthermore, LRRK2 R1398H has been shown to increase GTPase domain dimerization and GTP hydrolysis, reduce active GTP-bound LRRK2, increase axon length of primary cortical neurones and enhance LRRK2′s stimulatory effect on the canonical Wnt signalling pathway, all in opposition to the effects seen with the LRRK2 G2385R risk variant24. As N551K is in linkage disequilibrium with R1398H, it is possible that its protective effect is driven primarily by R1398H.
The results from this study show that the odds ratios (OR) for both variants appear to be higher in ET (R1398H OR = 0.91, 95% CI = 0.71–1.17, p = 0.46; N551K OR = 0.89, 95% CI = 0.69–1.15, p = 0.37) compared to PD5 (R1398H OR = 0.86, 95% CI = 0.77–0.97; N551K OR = 0.80, 95% CI = 0.69–0.93), suggesting that a protective trend for both LRRK2 variants may be present in ET, but not high enough to reach statistical significance. It remains possible that these LRRK2 variants exert a weaker effect in ET compared to PD, and a much larger sample size may be required to identify this. Nonetheless, to our knowledge, the size of our ET cohort in this study is one of the largest in current literature. Additionally, there remains a possibility that ET patients with R1398H or N551K variants may not develop PD (known as ET-onset PD, or ET-PD) due to the protective effect of both variants. Longer-term data on these ET carriers are needed to clarify this possibility.
While the results from this study do not preclude an effect of LRRK2 in ET, we conclude that the LRRK2 protective variants R1398H and N551K may not play a major role in modulating the risk of ET in our population. Further identification and study of rare LRRK2 variants in ET is important, and would ideally be carried out in large multi-centre studies with sufficient power. Nevertheless, our current findings will potentially contribute to future pooled or meta-analyses of the role of LRRK2 in ET.
Methods
Consecutive ET cases recruited from the movement disorder clinics at the National Neuroscience Institute, and age-, gender- and race-matched controls were included this study. Some of the control subjects had participated in earlier studies5,25. ET was diagnosed clinically using the consensus statement of the Movement Disorder Society (MDS) on tremor26. The controls were not known to have any neurodegenerative diseases. The study received approval from the SingHealth Institutional Review Board ethics committee and all study subjects gave their informed consent. Genotyping of the LRRK2 R1398H and N551K variants was carried out as previously described5. For a 20% effect size difference, our sample size has >80% power at alpha = 0.05. All methods were performed in accordance with the relevant guidelines and regulations. The authors agree to make materials, data and associated protocols promptly available to readers without undue qualifications in material transfer agreements.
References
Thenganatt, M. A. & Jankovic, J. The relationship between essential tremor and Parkinson’s disease. Parkinsonism Relat. Disord. 22(1), S162–165 (2016).
Kuhlenbäumer, G., Hopfner, F. & Deuschl, G. Genetics of essential tremor: meta-analysis and review. Neurology 82, 1000–1007 (2014).
Tio, M. & Tan, E.-K. Genetics of essential tremor. Parkinsonism Relat. Disord. 22(1), S176–178 (2016).
Skipper, L. et al. Analysis of LRRK2 functional domains in nondominant Parkinson disease. Neurology 65, 1319–1321 (2005).
Tan, E.-K. et al. Multiple LRRK2 variants modulate risk of Parkinson disease: a Chinese multicenter study. Hum. Mutat. 31, 561–568 (2010).
Chen, L. et al. LRRK2 R1398H polymorphism is associated with decreased risk of Parkinson’s disease in a Han Chinese population. Parkinsonism Relat. Disord. 17, 291–292 (2011).
Ross, O. A. et al. Association of LRRK2 exonic variants with susceptibility to Parkinson’s disease: a case-control study. Lancet Neurol. 10, 898–908 (2011).
Heckman, M. G. et al. Protective effect of LRRK2p.R1398H on risk of Parkinson’s disease is independent of MAPT and SNCA variants. Neurobiol. Aging 35, 266.e5–14 (2014).
Minen, M. T. & Louis, E. D. Emergence of Parkinson’s disease in essential tremor: a study of the clinical correlates in 53 patients. Mov. Disord. Off. J. Mov. Disord. Soc. 23, 1602–1605 (2008).
Jiménez-Jiménez, F. J., Alonso-Navarro, H., García-Martín, E. & Agúndez, J. A. G. The relationship between Parkinson’s disease and essential tremor: review of clinical, epidemiologic, genetic, neuroimaging and neuropathological data, and data on the presence of cardinal signs of parkinsonism in essential tremor. Tremor Hyperkinetic Mov. N. Y. N 2 (2012).
Tan, E.-K., Lee, S.-S., S., F.-C. & Lum, S.-Y. Evidence of increased odds of essential tremor in Parkinson’s disease. Mov. Disord. Off. J. Mov. Disord. Soc. 23, 993–997 (2008).
Benito-León, J., Louis, E. D. & Bermejo-Pareja, F. & Neurological Disorders in Central Spain Study Group. Risk of incident Parkinson’s disease and parkinsonism in essential tremor: a population based study. J. Neurol. Neurosurg. Psychiatry 80, 423–425 (2009).
Zimprich, A. et al. Mutations in LRRK2 cause autosomal-dominant parkinsonism with pleomorphic pathology. Neuron 44, 601–607 (2004).
Kachergus, J. et al. Identification of a novel LRRK2 mutation linked to autosomal dominant parkinsonism: evidence of a common founder across European populations. Am. J. Hum. Genet. 76, 672–680 (2005).
Paisán-Ruíz, C. et al. LRRK2 gene in Parkinson disease: mutation analysis and case control association study. Neurology 65, 696–700 (2005).
Di Fonzo, A. et al. A common missense variant in the LRRK2 gene, Gly2385Arg, associated with Parkinson’s disease risk in Taiwan. Neurogenetics 7, 133–138 (2006).
Tan, E. K. et al. The LRRK2 Gly2385Arg variant is associated with Parkinson’s disease: genetic and functional evidence. Hum. Genet. 120, 857–863 (2007).
Deng, H., Le, W., Davidson, A. L., Xie, W. & Jankovic, J. The LRRK2 I2012T, G2019S and I2020T mutations are not common in patients with essential tremor. Neurosci. Lett. 407, 97–100 (2006).
Clark, L. N. et al. Mutations in the Parkinson’s disease genes, Leucine Rich Repeat Kinase 2 (LRRK2) and Glucocerebrosidase (GBA), are not associated with essential tremor. Parkinsonism Relat. Disord. 16, 132–135 (2010).
Tan, E.-K., Lee, J., Lim, H.-Q., Yuen, Y. & Zhao, Y. Essential tremor and the common LRRK2 G2385R variant. Parkinsonism Relat. Disord. 14, 569–571 (2008).
Clarimón, J. et al. Tremor dominant parkinsonism: Clinical description and LRRK2 mutation screening. Mov. Disord. 23, 518–523 (2008).
Chao, Y. X. et al. Lrrk2 R1628P variant is a risk factor for essential tremor. Sci. Rep. 5, 9029 (2015).
Heckman, M. G. et al. LRRK2 variation and dementia with Lewy bodies. Parkinsonism Relat. Disord. 31, 98–103 (2016).
Nixon-Abell, J. et al. Protective LRRK2 R1398H Variant Enhances GTPase and Wnt Signaling Activity. Front. Mol. Neurosci. 9, 18 (2016).
Foo, J. N. et al. Analysis of non-synonymous-coding variants of Parkinson’s disease-related pathogenic and susceptibility genes in East Asian populations. Hum. Mol. Genet. 23, 3891–3897 (2014).
Deuschl, G., Bain, P. & Brin, M. Consensus statement of the Movement Disorder Society on Tremor. Ad Hoc Scientific Committee. Mov. Disord. Off. J. Mov. Disord. Soc. 13(3), 2–23 (1998).
Acknowledgements
ASLN is supported by the Singapore Ministry of Health’s National Medical Research Council (NIG grant) and the SingHealth Foundation (PRISM grant). EKT is supported by the Singapore Ministry of Health’s National Medical Research Council (STaR and Parkinson’s disease TCR grants).
Author information
Authors and Affiliations
Contributions
A.S.L.N. contributed to the drafting of the manuscript and analysis of data. E.N. contributed to the genetic analysis and analysis of data. Y.J.T. contributed to data analysis and drafting of the manuscript. P.K., W.L.A., L.C.S.T. and E.K.T. contributed to patient recruitment and sample collection. E.K.T. contributed to revision of the manuscript for intellectual content.
Corresponding authors
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ng, A.S.L., Ng, E.Y.L., Tan, Y.J. et al. Case-control analysis of LRRK2 protective variants in Essential Tremor. Sci Rep 8, 5346 (2018). https://doi.org/10.1038/s41598-018-23711-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-018-23711-w
- Springer Nature Limited