
Abstract
Background
We aimed to update estimates of global vision loss due to age-related macular degeneration (AMD).
Methods
We did a systematic review and meta-analysis of population-based surveys of eye diseases from January, 1980, to October, 2018. We fitted hierarchical models to estimate the prevalence of moderate and severe vision impairment (MSVI; presenting visual acuity from <6/18 to 3/60) and blindness ( < 3/60) caused by AMD, stratified by age, region, and year.
Results
In 2020, 1.85 million (95%UI: 1.35 to 2.43 million) people were estimated to be blind due to AMD, and another 6.23 million (95%UI: 5.04 to 7.58) with MSVI globally. High-income countries had the highest number of individuals with AMD-related blindness (0.60 million people; 0.46 to 0.77). The crude prevalence of AMD-related blindness in 2020 (among those aged ≥ 50 years) was 0.10% (0.07 to 0.12) globally, and the region with the highest prevalence of AMD-related blindness was North Africa/Middle East (0.22%; 0.16 to 0.30). Age-standardized prevalence (using the GBD 2019 data) of AMD-related MSVI in people aged ≥ 50 years in 2020 was 0.34% (0.27 to 0.41) globally, and the region with the highest prevalence of AMD-related MSVI was also North Africa/Middle East (0.55%; 0.44 to 0.68). From 2000 to 2020, the estimated crude prevalence of AMD-related blindness decreased globally by 19.29%, while the prevalence of MSVI increased by 10.08%.
Conclusions
The estimated increase in the number of individuals with AMD-related blindness and MSVI globally urges the creation of novel treatment modalities and the expansion of rehabilitation services.
Similar content being viewed by others


Introduction
Age-related macular degeneration (AMD) is an acquired, degenerative disorder affecting the macula of older adults [1]. The disease is characterised by an array of features in the macular region, such as drusen (deposits that accumulate between the retinal pigment epithelium -RPE- and the Bruch’s membrane), RPE cell depigmentation and proliferation, detachment of the RPE, loss of RPE cells and subretinal choroidal neovascularization [1], is categorized into a non-exudative (or “dry”) stage and an exudative (or ‘wet’) stage. Older age, genetic background, family history, European ancestry, and smoking are considered risk factors for the development and progression of the disease [1].
Significant progress has been made in the treatment of the exudative stage of AMD over the last two decades due to the clinical introduction of intraocular injections of anti-vascular endothelial growth factor (VEGF) drugs [2]. Still, AMD has remained a challenge in global eye healthcare due to its relatively high prevalence in older adults and since most cases of the non-exudative stage, the most common form of AMD, cannot effectively be treated yet. AMD has a high importance as a cause of vision impairment and blindness [3], with sequels such as a reduction of the quality of life [4] and economic impact due to loss of productivity [5].
Although AMD-related blindness is a growing global problem due to population aging, its importance is not homogeneous across world regions. In countries with a higher cataract surgical coverage (usually high-income countries), chronic eye conditions such as AMD account for a relatively more significant proportion of blindness [6].
To contribute to the World Health Organization (WHO) World Report on Vision [7] and the implementation of the recommendations generated [8], The Vision Loss Expert Group (VLEG) of the Global Burden of Disease (GBD) Study calculated estimates of the leading causes of vision impairment and blindness, like AMD [3, 9,10,11]. Such estimates are essential for monitoring, action planning, and advocacy [6]. In this systematic review, we aimed to update estimates of the global vision loss burden due to AMD, presenting estimates for 2020, temporal changes, and distribution by sex and world region.
Methods
The data was arranged following a review of published population-focused studies on vision impairment and blindness by the VLEG. This review included studies published between Jan 1, 1980, and Oct 1, 2018, incorporating grey literature. After title and abstract screening, abstracts were sent to regional VLEG committees, where at least three ophthalmic epidemiologists independently scored studies for quality against inclusion criteria. They were asked to review and rate each study with a score of 1 (clearly a representative population-based study using a comprehensive methodology), 2 (questionable representativeness and/or inadequately described or low-quality methodology), or 3 (definitely neither, warranting exclusion). Reviewers were asked to give their rationale for a rating of 2 or 3. A threshold for inclusion/exclusion was decided based on the average score of each study. Relevant studies from this review were combined with data from Rapid Assessment of Avoidable Blindness (RAAB) studies by VLEG. Data was also sourced from the US National Health and Nutrition Examination Survey 2007-2008 and the WHO Study on Global Ageing and Adult Health (SAGE Wave 1 2007-2010), contributed by the GBD team. A total of 252 studies contributed data on age-related macular degeneration and are grouped by geographical region in the Appendix. More detailed methods are published elsewhere [3, 10] and discussed in brief as follows.
VLEG pinpointed 137 studies and pulled data from 70 studies in their 2010 review and 67 additional studies in their 2014–18 review. Most of these studies were national or subnational cross-sectional surveys. VLEG also arranged to produce 5-year age-segregated RAAB data from the RAAB repository (www.raab.world). To qualify, studies met specific criteria: vision acuity data must be gathered through a test chart compatible with the Snellen scale, and the sample must represent the population. Subjective reports of vision loss were not included. The criteria for vision loss was defined by the International Classification of Diseases 11th edition as employed by WHO. It was based on the vision in the better eye upon presentation. Moderate vision loss was defined as a visual acuity of 6/60 or better but less than 6/18, severe vision loss as a visual acuity of 3/60 or better but less than 6/60, and blindness as a visual acuity of less than 3/60 or less than 10° visual field around central fixation (although the visual field definition was rarely used in population-based eye surveys).
We split the original data into several datasets, creating separate envelopes for each degree of vision loss (mild, moderate, and severe) and blindness. This data was then fed into a meta-regression tool designed by the Institute for Health Metrics and Evaluation (IHME) known as MR-BRT (meta-regression; Bayesian; regularised; trimmed) [12]. The benchmark for each severity level was presenting vision impairment.
When possible, data about uncorrected refractive errors were pulled straight from the data sources. If not, they were calculated by subtracting the best-corrected vision impairment from presenting vision impairment prevalence at each severity level. Other causes were factored into the best-corrected estimates for each level of vision impairment.
Our models for distance vision impairment and blindness were based on the most commonly reported causes found in the literature, and the minimum age for inclusion of data on AMD was 45 years. We created estimates of MSVI and blindness specific to location, year, age, and sex using Disease Modelling Meta-Regression (Dismod-MR) 2.1 [13]. Its data processing steps have been outlined elsewhere [3]. Briefly, Dismod-MR 2.1 models were run for all vision impairment by severity (moderate, severe, blindness) regardless of cause and, separately, for MSVI and blindness due to each modelled cause of vision impairment. Then, models of MSVI due to specific causes were split into moderate and severe estimates using the ratio of overall prevalence in the all-cause moderate presenting vision impairment and severe presenting vision impairment models. Next, prevalence estimates for all causes by severity were scaled to the models of all-cause prevalence by severity. This produced final estimates by age, sex, year, and location for each cause of vision impairment by severity. We age-standardised our estimates using the GBD standard population [14]. Hierarchical logistic regressions with mixed effects were applied using the R package RStanArm to assess the prevalence of blindness independently and MSVI across various country-age groups, structured within a five-tiered hierarchy. The blindness model was based on 270 studies, while the MSVI model included 245 studies, acknowledging that a single study might span multiple countries or years. This framework spanned 187 countries, grouped into 21 subregions and further into seven broader regions, culminating in an analysis of global-level effects. Data on blindness and MSVI due to AMD were presented by seven super-regions (Southeast Asia/East Asia/Oceania, Central Europe/Eastern Europe/Central Asia, High-income, Latin America and Caribbean, North Africa, and the Middle East, South Asia, and Sub-Saharan Africa) and globally. Data on other causes of vision impairment and blindness will be presented in separate publications.
Results
In 2020, 1.85 million (all ages; 95% uncertainty interval (UI): 1.35 to 2.43 million) people were estimated to be blind due to AMD, with 664,000 (472,000 to 894,000) males and 1,185,000 (876,000 to 1,545,000) females affected (Tables 1, 2). AMD-related MSVI affected 6.23 million (95%UI: 5.04 to 7.58) individuals worldwide, among them 2,747,000 (2,207,000 to 3,377,000) males and 2,743,000 (2,202,000 to 3,371,000) females (Tables 1, 3).
High-income countries (0.60 million people; 0.46 to 0.77) accounted for the highest number of individuals with AMD-related blindness per world region, whereas the lowest number of individuals with presenting blindness due to AMD per world region was found in Central Europe / Eastern Europe / Central Asia combined (0.06 million people; 0.04 to 0.08) and Latin America and the Caribbean (0.07 million people; 0.50 to 0.1) (Table 1).
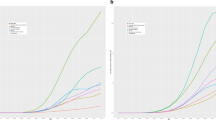
The crude prevalence of AMD-related blindness in those aged ≥ 50 years in 2020 was estimated as 0.10% (0.07 to 0.12) globally. The regions with the highest prevalence of blindness due to AMD were North Africa/Middle East, 0.22% (0.16 to 0.30) and Sub-Saharan Africa, 0.15% (0.11 to 0.20) (Supplementary Fig. 1). Age-standardized estimated prevalence of MSVI due to AMD in those aged ≥ 50 years in 2020 was 0.34% (0.27 to 0.41) globally, and the regions with the highest prevalence of MSVI due to AMD were also North Africa/Middle East (0.55%; 0.44 to 0.68) and Sub-Saharan Africa (0.50%; 0.40 to 0.61) (Table 1).
From 2000 to 2020, the estimated crude prevalence of blindness due to AMD decreased globally by 19.3% (19.6 to 19.0%), with a wide variety between regions, from -32.6% (-32.9 to -32.3%) in Southeast Asia, East Asia, and Oceania to +1.3% (0.9 to 1.7%) in Latin America and the Caribbean, the only region which showed an increase (Table 4). On the other hand, over the same period, the estimated crude prevalence of MSVI due to AMD increased globally by 10.1% (9.8 to 10.3%), with changes varying from −9.3% (−9.5 to −9.0%) in North Africa and Middle East to +7.2% (6.9 to 7.5%) in Southeast Asia, East Asia, and Oceania (Table 5). Figure 2 shows the estimated crude prevalence of MSVI due to AMD in 2020.
Discussion
In 2020, AMD ranked second among the causes of irreversible blindness globally [3]. From 2000 to 2020, there was an estimated decrease in the prevalence of AMD-related blindness in all regions except Latin America and the Caribbean and an increase in the prevalence of AMD-related MSVI in all regions except North Africa, Middle East, and Sub-Saharan Africa, with wide discrepancies between regions. The global population growth and increasing life expectancy can explain the increasing number of individuals with AMD-related vision loss. Yet, the divergences in AMD prevalence and vision impairment necessitate extensive research to unravel the complex interplay of genetic factors, lifestyle choices, and access to healthcare services.
The prevalence of blindness and MSVI due to AMD is higher in older age groups, and countries with a growing life expectancy should take this information into account for better health service planning. But considering the current barriers to accessing AMD treatment and rehabilitation services in many regions, even a minor increase in absolute numbers might put pressure on the already overloaded public health systems. The reduced availability of ophthalmic services during the Covid-19 pandemic [15] and the economic impact that might be seen during the post-pandemic years can increase barriers in managing chronic eye conditions like AMD.
Dealing with AMD from a public health perspective is a complex task. First, although a trained ophthalmologist efficiently performs diagnosis, the availability and distribution of eye care professionals remain an issue in many parts of the world [16]. If well connected to public health initiatives, the growing use of telemedicine and artificial intelligence in eye care will likely reduce the percentage of those with undiagnosed AMD. Second, its first-line treatment, intravitreal anti-VEGF injection, can be expensive; its effect lasts only a few months and is only indicated for the wet form and, more recently, geographic atrophy [17]. And finally, those with MSVI and blindness due to AMD would benefit from rehabilitation services, and their availability is also scarce [18]. The integration of education for those at a higher risk for developing AMD diagnosis, treatment, and rehabilitation, using a people-centred approach [7], could reduce the burden of AMD. Ideally, addressing AMD from a public health perspective demands a life course, people-centered approach recognizing the importance of early interventions and managing AMD co-morbidities. Preventative measures, such as anti-smoking campaigns targeted at adolescents and adults, could significantly impact the prevalence of AMD in the older population, given the well-established link between smoking and the progression of AMD.
In the healthcare continuum, involving primary care providers (PCPs) in AMD care could alleviate some current issues, especially in low-resource scenarios. They can serve as the initial touchpoint for patient education and promote awareness of AMD risk factors and early symptoms. For example, PCPs could play a crucial role in guiding patients through lifestyle changes that mitigate the risk of AMD, such as advocating smoking cessation, reinforcing the need for regular check-ups for those with diagnosed AMD or at a higher risk of having it, and potentially managing portable fundus cameras that could send images for remote ophthalmologists, or reinforcing the importance of compliance with follow-ups and treatment, and monitoring co-morbidities.
In addition to preventive care, there is a critical need to address the broader spectrum of challenges faced by individuals with AMD, particularly as they often experience other ocular and extraocular health issues. For instance, hearing impairment is a common co-morbidity that can compound the difficulties faced by those with vision loss, intensifying feelings of isolation and hindering effective communication. Moreover, individuals with vision impairment are at an increased risk of falls, which can lead to further physical injury and a decline in their quality of life [6]. Depression is another concern, with the loss of visual function significantly impacting mental health and the overall well-being of affected individuals [6].
The non-physician administration of anti-VEGF injections could be explored as a strategy to decentralize treatment, lowering costs and increasing access, while ensuring the safety and efficacy of such approaches through proper training and oversight [19]. Another option to be considered is conducting the injections within the same day of consultation, and same-day bilateral intravitreal injections to avoid multiple visits [20,21,22].
In the realm of age-related macular degeneration (AMD) treatments, emerging therapies like Pegcetacoplan and gene therapy offer renewed hope. Pegcetacoplan was recently the first drug approved by the Food and Drug Administration to treat geographic atrophy, the advanced stage of dry AMD known for its relentless progression of retinal cell degeneration and consequent permanent vision loss [17]. This novel drug specifically inhibits the C3 component of the immune system’s complement pathway, a system implicated in the exacerbation of GA. In a recently published clinical trial, intravitreal injections of Pegcetacoplan could successfully slow GA progression. However, no differences in visual acuity between eyes injected with either Pegcetacoplan or sham injections were found [17].
Gene therapy presents a frontier approach in AMD treatment by introducing genetic material into cells to correct abnormal genes, suppress harmful gene expression, or produce beneficial proteins. This can involve various strategies, from replacing defective genes with functional ones, silencing genes contributing to disease progression to introducing new genes that could stop disease progression or repair damaged retinal tissue. Initial clinical trials have shed light on gene therapy’s capacity for offering a sustained therapeutic effect, potentially simplifying treatment regimens by reducing the need for frequent injections, which are the current standard of care for wet AMD. Despite these promising developments, gene therapy for AMD remains in the experimental phase, and ongoing research is focused on overcoming hurdles related to precise delivery methods, ensuring lasting benefits, and establishing safety protocols [23].
Strengths of the present study included the number of population-based data accessed and used, analysis of trends in the causes of blindness and MSVI, incorporation of nonlinear age trends and accounting for data that were not reported by age, and systematic quantitative analysis and reporting of uncertainty. Among the limitations of the present study, we can cite the shortage of data in some countries/regions and information on the burden of AMD in ethnic minorities, such as indigenous people. In some countries, population-based data were either collected sub nationally or more than a decade ago, and estimates may not represent the current reality of a given country. Also, most analysed studies used the Rapid Assessment of Cataract Surgical Services or RAAB methodologies, which may underestimate posterior pole diseases, such as AMD. The evolution of population-based studies, especially those employing advanced imaging technologies like fundus photography, should be elaborated to reflect how these methodologies can refine the accuracy of AMD prevalence studies [24].
Policymakers and the academic community should consider that AMD’s social and economic impact is expected to increase substantially due to population growth and ageing [6]. Since population growth rates and life expectancies differ across regions, the burden of AMD will vary globally. Different from cataract and uncorrected refractive errors, the leading causes of blindness and vision impairment, respectively, the burden of AMD can only be alleviated if significant advances in research are made. Developing novel, cost-effective treatment modalities ideally restoring sight, and adopting a life course approach integrating all levels of care is paramount for managing AMD for the next decades.
Summary
What was known before:
-
Based on the Global Burden of Disease Study 2010, the Vision Loss Expert Group (VLEG) estimated that there were 2.1 million people blind due to macular diseases.
What this study adds:
-
In 2020, 1.85 million (95%UI: 1.35 to 2.43 million) people were blind due to AMD, and another 6.23 million (95%UI: 5.04 to 7.58) presented with MSVI globally.
-
From 2000 to 2020, there was a reduction in the crude prevalence of age-related macular degeneration (AMD)-related blindness globally and an increase in AMD-related moderate and severe vision impairment.
Data availability
The data that support the findings of this study are not openly available due to reasons of sensitivity and are available from the coordinator of the Vision Loss Expert Group (Professor Rupert Bourne; rb@rupertbourne.co.uk) upon reasonable request. Data are located in controlled access data storage at Anglia Ruskin University.
References
Mitchell P, Liew G, Gopinath B, Wong TY. Age-related macular degeneration. The Lancet. 2018;392:1147–59. https://doi.org/10.1016/S0140-6736(18)31550-2
Rosenfeld PJ, et al. Ranibizumab for neovascular age-related macular degeneration. N. Engl. J. Med. 2006;355:1419–31.
Bourne RRA, et al. Causes of blindness and vision impairment in 2020 and trends over 30 years, and prevalence of avoidable blindness in relation to VISION 2020: The Right to Sight: An analysis for the Global Burden of Disease Study. Lancet Glob. Heal. 2021;9:e144–e160.
Mitchell J, Bradley C. Quality of life in age-related macular degeneration: A review of the literature. Health Q. Life Outcomes. 2006;4:97.
Eckert, KA, Lansingh, VC, Carter, MJ & Frick, KD Update of a Simple Model to Calculate the Annual Global Productivity Loss Due to Blindness and Moderate and Severe Vision Impairment. Ophthalmic Epidemiol. 2013;30.
Burton MJ, et al. The Lancet Global Health Commission on Global Eye Health: vision beyond 2020. Lancet Glob. Heal. 2021;9:e489–e551.
WHO. World report on vision. WHO; 2019 https://www.who.int/publicatio%0D%0Ans/i/item/world-report-on-vision%0D%0A.
Keel S, et al. Strengthening the integration of eye care into the health system: Methodology for the development of the WHO package of eye care interventions. BMJ Open Ophthalmol. 2020;5:e000533.
Bourne RRA, et al. Magnitude, temporal trends, and projections of the global prevalence of blindness and distance and near vision impairment: a systematic review and meta-analysis. Lancet Glob. Heal. 2017;5:e888–e897.
Bourne RRA, et al. Trends in prevalence of blindness and distance and near vision impairment over 30 years: An analysis for the Global Burden of Disease Study. Lancet Glob. Heal. 2021;9:e130–e143.
Flaxman SR, et al. Global causes of blindness and distance vision impairment 1990–2020: a systematic review and meta-analysis. Lancet Glob. Heal. 2017;5:e1221–e1234.
Zheng P, et al. Trimmed constrained mixed effects models: formulations and algorithms. ArXiv190910700. Math Stat. 2019. http://arxiv.org/abs/1909.10700.
Vos T, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396:1204–22.
Vollset SE, et al. Fertility, mortality, migration, and population scenarios for 195 countries and territories from 2017 to 2100: a forecasting analysis for the Global Burden of Disease Study. Lancet. 2020;396:1285–306.
Muralikrishnan J, et al. Access to eye care during the COVID-19 pandemic, India. Bull. World Health Organ. 2022;100:135–43.
Hong, H. et al. The Challenge of Universal Eye Health in Latin America: Distributive inequality of ophthalmologists in 14 countries. BMJ Open 2016; 6.
Heier JS, et al. Pegcetacoplan for the treatment of geographic atrophy secondary to age-related macular degeneration (OAKS and DERBY): two multicentre, randomised, double-masked, sham-controlled, phase 3 trials. Lancet. 2023;402:1434–48.
Chiang PPC, O’Connor PM, Le Mesurier RT, Keeffe JE. A global survey of low vision service provision. Ophthalmic Epidemiol. 2011;18:109–21.
Austeng D, et al. Nurse-administered intravitreal injections of anti-VEGF: study protocol for noninferiority randomized controlled trial of safety, cost and patient satisfaction. BMC Ophthalmol. 2016;16:169.
Bolme S, Austeng D, Morken TS, Follestad T, Halsteinli V. Cost consequences of task-shifting intravitreal injections from physicians to nurses in a tertiary hospital in Norway. BMC Health Serv Res. 2023;23:229 https://doi.org/10.1186/s12913-023-09186-0.
Juncal VR, et al. Same-day bilateral intravitreal anti-vascular endothelial growth factor injections: Experience of a large Canadian retina center. Ophthalmologica. 2019;242:1–7. https://doi.org/10.1159/000499115.
Borkar DS, et al. Endophthalmitis rates after bilateral same-day intravitreal anti-vascular endothelial growth factor injections. Am J Ophthalmol. 2018;194:1–6. https://doi.org/10.1016/j.ajo.2018.06.022.
Kim K, et al. Genome surgery using Cas9 ribonucleoproteins for the treatment of age-related macular degeneration. Genome Res. 2017;27:419–26.
Mactaggart I, Limburg H, Bastawrous A, Burton MJ, Kuper H. Rapid assessment of avoidable blindness: Looking back, looking forward. Br J Ophthalmol. 2019;103:1549–52.
Acknowledgements
The Global Burden of Disease Study is primarily funded by the Bill & Melinda Gates Foundation (OPP1152504). The funder of this study had no role in the study design, data collection, data analysis, data interpretation, or writing of the publication.
Funding
This study was funded by Brien Holden Vision Institute, Fondation Thea, Fred Hollows Foundation, Bill & Melinda Gates Foundation, Lions Clubs International Foundation (LCIF), Sightsavers International, and University of Heidelberg.
Author information
Authors and Affiliations
Consortia
Contributions
Please see Appendix for more detailed information about individual author contributions to the research, divided into the following categories: managing the overall research enterprise; writing the first draft of the manuscript; primary responsibility for applying analytical methods to produce estimates; primary responsibility for seeking, cataloguing, extracting, or cleaning data; designing or coding figures and tables; providing data or critical feedback on data sources; developing methods or computational machinery; providing critical feedback on methods or results; drafting the manuscript or revising it critically for important intellectual content; and managing the estimation or publications process.
Corresponding author
Ethics declarations
Competing interests
GBD 2019 Blindness and Vision Impairment Collaborators T W Bärnighausen reports support for the present manuscript from Fondation Botnar and Harvard T.H. Chan School of Public Health; grants or contracts from National Institutes of Health (NIH), Wellcome, German National Science Foundation, German Ministry of Education and Research, Volkswagen Foundation, European Union Horizon Europe, German Ministry of the Environment, Alexander von Humboldt Foundation, Else-Kröner Fresenius Foundation, International Vaccine Institute for grants to Heidelberg Institute of Global Health, Heidelberg University, Germany; stock or stock options in EUR 5000 ownership stake in a consultancy on climate change and health research; all outside the submitted work. R Bai reports support for the present manuscript from Social Science Fund of Jiangsu Province (grant number 21GLD008) N Bayleyegn reports leadership or fiduciary roles in board, society, committee or advocacy groups, paid or unpaid with project HIPPO and GECKO as a hospital lead as well as Ethiopia as a member of a surgical society. S Bhaskar reports grants or contracts from Japan Society for the Promotion of Science (JSPS) Grant 2023-25 and Ministry of Education, Culture, Sports, Science and Technology (MEXT), Japan. T Braithwaite reports grants or contracts from Fight for Sight/Royal College of Ophthalmologists for Zakarian Award (RCOZAK2202). X Dai reports support for the present manuscript from IHME/UW for paid salary. A Dastiridou support for attending meetings and/or travel from THEA and ABBVIE. M Foschi reports consulting fees from Roche and Novartis as a scientific consultant; support for attending meetings and/or travel from Roche, Novartis, Biogen, Merck, and Sanofi; leadership or fiduciary roles in board, society, committee or advocacy groups, paid or unpaid with MSBase collaboration scientific leadership group as a member. J M Furtado reports consulting fees from Pan American Health Organization and Lions Club International Foundation. S Hallaj reports grants or contracts from National Institute of Health Bridge to Artificial Intelligence common fund, grant # OT2OD032644. I M Karaye support for attending meetings and/or travel from Hofstra University and National Academies of Sciences, Engineering, and Medicine. K Krishan reports other support from Kewal Krishan acknowledges non-financial support from the UGC Centre of Advanced Study, CAS II, awarded to the Department of Anthropology, Panjab University, Chandigarh, India, outside the submitted work. T Laksono reports support for attending meetings and/or travel outside the submitted work. V C Lansingh reports support for attending meetings and/or travel from HwelpMeSee. M Lee reports support from the Ministry of Education of the Republic of Korea and the National Research Foundation of Korea (NRF-2021R1I1A4A01057428) and Bio-convergence Technology Education Program through the Korea Institute for Advancement Technology (KIAT) funded by the Ministry of Trade, Industry and Energy (No. P0017805), all outside the submitted work. C McAlinden reports grants or contracts from the Welsh Government for a research grant related to diabetic eye disease (unpaid role)]; consulting fees from: Acufocus (Irvine, California, USA), Atia Vision (Campbell, California, USA), Bausch and Lomb (Bridgewater, New Jersey, USA), BVI (Liège, Belgium), Coopervision (Pleasanton, California, USA), Cutting Edge (Labége, France), Fudan University (Fudan, China), Hoya (Frankfurt, Germany), Knowledge Gate Group (Copenhagen, Denmark), Johnson & Johnson Surgical Vision (Santa Ana, California, USA), Keio University (Tokyo, Japan), Ludwig-Maximilians-University (München, Germany), Medevise Consulting SAS (Strasbourg, France), Ophtec BV (Groningen, The Netherlands), SightGlass vision (Menlo Park, California, USA), Science in Vision (Bend, Oregan, USA), Scope (Crawley, UK), SpyGlass (Aliso Viejo, California, USA), Sun Yat-sen University (Guangzhou, China), Targomed GmbH (Bruchsal, Germany), University of São Paulo (São Paulo, Brazil), Vold Vision (Arkansas, USA); payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Scope (Crawley, UK), and Thea pharmaceuticals (Clemont-Ferrand, France); support for attending meetings and/or travel from the following over the past thirty-six months: Bayer (Leverkusen, Germany), British Society of Refractive Surgery (Oxford, UK), Portuguese Society of Ophthalmology (Coimbra, Portugal), Royal College of Ophthalmologists (London, UK), Scope (Crawley, UK), Thea pharmaceuticals (Clemont-Ferrand, France); leadership or fiduciary roles in board, society, committee or advocacy groups, paid or unpaid with the British Society for Refractive Surgery as a council member (unpaid role), a PROM advisor to the Royal College of Ophthalmologists (unpaid role), an editorial board member for Graefe’s Archive for Clinical and Experimental Ophthalmology, Eye and Vision, Archives of Medical Science, Journal of Clinical Medicine, Journal of Ophthalmology, and Journal of Clinical and Experimental Ophthalmology as well as an Associate Editor for Frontiers in Medicine – Ophthalmology; and other support as a developer of the Quality of Vision (QoV) questionnaire and the Orthokeratology and Contact Lens Quality of Life Questionnaire (OCL-QoL) having a financial interest in these tools and consults on topics including Rasch analysis, questionnaires, statistical analyses, and clinical/surgical ophthalmology topics. Dr McAlinden has undertaken paid peer reviews for Research Square (Durham, North Carolina, USA); all outside the submitted work. Y L Samodra reports grants or contracts from Taipei Medical University for a Ph.D. Scholarship; leadership or fiduciary roles in board, society, committee or advocacy groups, paid or unpaid with Benang Merah Research Center as Co-founder, all outside the submitted work. J A Singh reports consulting fees from AstraZeneca, Crealta/Horizon, Medisys, Fidia, PK Med, Two labs Inc., Adept Field Solutions, Clinical Care options, Clearview healthcare partners, Putnam associates, Focus forward, Navigant consulting, Spherix, MedIQ, Jupiter Life Science, UBM LLC, Trio Health, Medscape, WebMD, and Practice Point communications; and the National Institutes of Health and the American College of Rheumatology; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from the speaker’s bureau of Simply Speaking; support for attending meetings and/or travel from OMERACT as a past steering committee for attending their meeting every 2 years; participation on a Data Safety Monitoring Board or Advisory Board with FDA Arthritis Advisory Committee as a member (No financial support); leadership or fiduciary roles in board, society, committee or advocacy groups, paid or unpaid as a past steering committee member of the OMERACT, an international organization that develops measures for clinical trials and receives arm’s length funding from 12 pharmaceutical companies, Co-Chair of the Veterans Affairs Rheumatology Field Advisory Committee (No financial support), and editor and the Director of the UAB Cochrane Musculoskeletal Group Satellite Center on Network Meta-analysis (No financial support); stock or stock options in Atai life sciences, Kintara therapeutics, Intelligent Biosolutions, Acumen pharmaceutical, TPT Global Tech, Vaxart pharmaceuticals, Atyu biopharma, Adaptimmune Therapeutics, GeoVax Labs, Pieris Pharmaceuticals, Enzolytics Inc., Seres Therapeutics, Tonix Pharmaceuticals Holding Corp., and Charlotte’s Web Holdings, Inc. as well as previous stock options in Amarin, Viking and Moderna pharmaceuticals, all outside the submitted work. E Skiadaresi reports consulting fees from Bayer (Leverkusen, Germany), Novartis (Basel, Switzerland), Roche (Basel, Switzerland), Medevise Consulting SAS (Strasbourg, France); payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Bayer (Leverkusen, Germany), Novartis (Basel, Switzerland), and Roche (Basel, Switzerland); support for attending meetings and/or travel from Bayer (Leverkusen, Germany), Novartis (Basel, Switzerland), and Roche ((Basel, Switzerland); leadership or fiduciary roles in board, society, committee or advocacy groups, paid or unpaid with Chair of ATHENA Trial Steering Committee, UK (unpaid); all outside the submitted work. B T Taye reports support for the present manuscript from Brien Holden Vision Institute, Fondation Thea, Fred Hollows Foundation, Bill & Melinda Gates Foundation, Lions Clubs International Foundation (LCIF), Sightsavers International, and University of Heidelber. The funder has no role in designing and preparing the manuscript. J H V Ticoalu leadership or fiduciary roles in board, society, committee or advocacy groups, paid or unpaid with Benang Merah Research Center as Co-founder. M Zielińska reports other support as an AstraZeneca employee; outside the submitted work. Vision Loss Expert Group of the Global Burden of Disease Study T Braithwaite reports grants or contracts from any entity from Zakarian Award Fight for Sight/Royal College of Ophthalmologists (RCOZAK2202). A Bron reports payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Théa. N Congdon reports grants or contracts from any entity from Welcome Trust and MRC; consulting fees from Belkin Vision; and support for attending meetings and/or travel from Singapore National Eye Center. M A Del Monte reports support for attending meetings and/or travel from the University of Michigan; and leadership or fiduciary roles in board, society, committee or advocacy groups, paid or unpaid as past president of Costenbader Society. T Fricke reports grants or contracts from any entity from Brien Holden Vision Institute, Victorian Lions Foundation, International Myopia Institute, and Australian government; and support for attending meetings and/or travel from International Myopia Institute. D Friedman reports grants or contracts from any entity from Perivison and Genentech (to the institution for research); consulting fees from Abbvie and Life Biosciences; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Thea Pharmaceuticals; support for attending meetings and/or travel from Thea Pharmaceuticals; and leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid, from Orbis International as member of board of governors. J M Furtado reports consulting fees from Pan American Health Organization and from Lions Club International Foundation. G Gazzard reports consulting fees from Alcon Laboratories, Inc; Allergan, Inc; BELKIN Vision LTD; Carl Zeiss Meditec; Elios; Genentech/Roche; Reichert; Théa and ViaLase; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Alcon Laboratories, Inc; BELKIN Vision Ltd; Carl Zeiss Meditec; Elios and Ellex; participation on a Data Safety Monitoring Board or Advisory Board with Alcon Laboratories, Inc; Allergan, Inc; BELKIN Vision Ltd; Carl Zeiss Meditec; Elios and Visufarma; and leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid with Glaucoma UK Medical Advisory Board and UK&Eire Glaucoma Society as president. M E Hartnett reports support for the present manuscript (e.g., funding, provision of study materials, medical writing, article processing charges, etc.) from Michael F. Marmor, M.D. Professor of Retinal Science and Disease as endowment to support salary; grants or contracts from any entity (from National Eye Institute R01 EY017011 and National Eye Institute R01 EY015130) as partial salary support; patents planned, issued or pending (WO2015123561A2 and WO2021062169A1); and leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid with Jack McGovern Coats’ Disease Foundation and as director of Women’s Eye Health and Macular Society Grant Review Chair. J H Kempen reports support for the present manuscript (e.g., funding, provision of study materials, medical writing, article processing charges, etc.) from Mass Eye and Ear Global Surgery Program (as support of salary); and grants or contracts from any entity from Sight for Souls (as support of salary). J E Kim reports consulting fees from Genentech/Roche, DORC, Notal Vision and Outlook Therapeutics (all as payment to J E Kim); participation on a Data Safety Monitoring Board or Advisory Board with Allergan, Amgen, Apellis, Bausch&Lomb, Clearside, Coherus, Novartis and Regeneron (all as participation on advisory board); leadership or fiduciary role in other borad, society, committee or advocacy group, paid or unpaid, with AAO, APRIS, ASRS, Macular Society and NAEVR/AEVR (all unpaid); and receipt of equipment, materials, drugs, medical writing, gifts or other services from Clearside and Genentech/Roche (both for medical writing). V C Lansingh reports consulting fees from HelpMeSee (as an employee); and support for attending meetings and/or travel from HelpMeSee (pay airfare and hotel). J Leasher reports leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid with National Eye Institute (as a member) and National Eye Health Education Program planning committee (unpaid). M Nowak reports participation on a Data Safety Monitoring Board or Advisory Board with Vision Express Co. Poland as the chairman of medical advisory board of Vision Express Co. Poland. P Ramulu reports grants or contracts from National Institute of Health and Perfuse Therapeutics; and consulting fees from Alcon and W. L. Gore. F Topouzis reports grants or contracts from Théa, Omikron, Pfizer, Alcon, Abbvie and Bayer (all paid to Institution); consulting fees from Omikron, Théa and Bausch & Lomb (all paid to Topouzis); payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Omikron (paid to Topouzis), Abbvie and Roche (both paid to Institute); and leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid with European Glaucoma Society (as president), Greek Glaucoma Society (as president) and Board of Governors, World Glaucoma Association (all unpaid).
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix: Contributions by Authors
GBD 2019 Blindness and Vision Impairment Collaborators
Providing data or critical feedback on data sources
Yohannes Habtegiorgis Abate, Tadele Girum Girum Adal, Kishor Adhikari, Antonella Agodi, Williams Agyemang-Duah, Fares Alahdab, Syed Shujait Shujait Ali, Louay Almidani, Sofia Androudi, Jalal Arabloo, Alessandro Arrigo, Seyyed Shamsadin Athari, Desta Debalkie Atnafu, Alok Atreya, Yared Asmare Aynalem, Zewdu Bishaw Aynalem, Ahmed Y Azzam, Sara Bagherieh, Martina Barchitta, Mainak Bardhan, Till Winfried Bärnighausen, Nebiyou Simegnew Bayileyegn, Ahmet Begde, Babak Behnam, Akshaya Srikanth Bhagavathula, Sonu Bhaskar, Gurjit Kaur Bhatti, Jasvinder Singh Bhatti, Bagas Suryo Bintoro, Rupert R. A. Bourne, Tasanee Braithwaite, Paul Svitil Briant, Florentino Luciano Caetano dos Santos, Muthia Cenderadewi, Vijay Kumar Chattu, Dinh-Toi Chu, Maria Vittoria Cicinelli, Natália Cruz-Martins, Xiaochen Dai, Maedeh Dastmardi, Nikolaos Dervenis, Vinoth Gnana Chellaiyan Devanbu, Joshua R Ehrlich, Michael Ekholuenetale, Temitope Cyrus Ekundayo, Iman El Sayed, Ambaw Abebaw Emrie, Adeniyi Francis Fagbamigbe, Hossein Farrokhpour, Ali Fatehizadeh, Alireza Feizkhah, Arthur G Fernandes, Lorenzo Ferro Desideri, Seth Flaxman, Kayode Raphael Fowobaje, João M Furtado, Tilaye Gebru Gebi, Brhane Gebremariam, Molalegn Mesele Gesese, Fariba Ghassemi, Sherief Ghozy, Mahaveer Golechha, Pouya Goleij, Sapna Gupta, Veer Bala Gupta, Vivek Kumar Gupta, Teklehaimanot Gereziher Haile, Arvin Haj-Mirzaian, Sung Hwi Hong, Praveen Hoogar, Mehdi Hosseinzadeh, Chengxi Hu, Hong-Han Huynh, Chidozie C D Iwu, Mihajlo Jakovljevic, Shubha Jayaram, Jost B Jonas, Charity Ehimwenma Joshua, Gebisa Guyasa Kabito, Laleh R Kalankesh, Himal Kandel, Gbenga A Kayode, Shemsu Kedir, Yousef Saleh Khader, Himanshu Khajuria, Mahalaqua Nazli Khatib, Yun Jin Kim, Adnan Kisa, Sezer Kisa, Soewarta Kosen, Kewal Krishan, Chandrakant Lahariya, Tri Laksono, Dharmesh Kumar Lal, Trang Diep Thanh Le, Munjae Lee, Seung Won Lee, Nicolas Leveziel, Stephen S Lim, Xuefeng Liu, Razzagh Mahmoudi, Kashish Malhotra, Roy Rillera Marzo, Andrea Maugeri, Tesfahun Mekene Meto, Soheil Mohammadi, Ali H Mokdad, Mohammad Ali Moni, Maryam Moradi, Admir Mulita, Kovin S Naidoo, Ganesh R Naik, Shumaila Nargus, Zuhair S Natto, Biswa Prakash Nayak, Dang H Nguyen, Hien Quang Nguyen, Phat Tuan Nguyen, Van Thanh Nguyen, Robina Khan Niazi, Ogochukwu Janet Nzoputam, Ismail A Odetokun, Andrew T Olagunju, Matthew Idowu Olatubi, Obinna E Onwujekwe, Uchechukwu Levi Osuagwu, Mayowa O Owolabi, Jagadish Rao Padubidri, Jay Patel, Shrikant Pawar, Arokiasamy Perianayagam, Hoang Tran Pham, Fakher Rahim, Vafa Rahimi-Movaghar, Ahmed Mustafa Rashid, Annisa Utami Rauf, Elrashdy Moustafa Mohamed Redwan, Serge Resnikoff, Zahra Saadatian, Siamak Sabour, Basema Saddik, Umar Saeed, Sare Safi, Sher Zaman Safi, Narjes Saheb Sharif-Askari, Joseph W Sakshaug, Vijaya Paul Samuel, Abdallah M Samy, Monika Sawhney, Mete Saylan, Sayed Mansoor Sediqi, Yashendra Sethi, Allen Seylani, Jaffer Shah, Masood Ali Shaikh, Muhammad Aaqib Shamim, Maryam Shayan, Aminu Shittu, Jasvinder A Singh, Paramdeep Singh, Chandrashekhar T Sreeramareddy, Jaimie D Steinmetz, Ian Tapply, Hugh R Taylor, Guesh Mebrahtom Tsegay, Saif Ullah, Muhammad Umair, Sahel Valadan Tahbaz, Theo Vos, Dong Keon Yon, Naohiro Yonemoto, Mikhail Sergeevich Zastrozhin, and Magdalena Zielińska.
Developing methods or computational machinery
Alessandro Arrigo, Desta Debalkie Atnafu, Ahmed Y Azzam, Akshaya Srikanth Bhagavathula, Rupert R. A. Bourne, Paul Svitil Briant, Kaleb Coberly, Xiaochen Dai, Maedeh Dastmardi, Michael Ekholuenetale, Mehdi Emamverdi, Ayesha Fahim, Ali Fatehizadeh, Arthur G Fernandes, Seth Flaxman, Sherief Ghozy, Mehdi Hosseinzadeh, Hong-Han Huynh, Jost B Jonas, Charity Ehimwenma Joshua, Mahalaqua Nazli Khatib, Adnan Kisa, Chandrakant Lahariya, Nicolas Leveziel, Razzagh Mahmoudi, Ali H Mokdad, Mohammad Ali Moni, Admir Mulita, Hien Quang Nguyen, Phat Tuan Nguyen, Van Thanh Nguyen, Michal Ordak, Jagadish Rao Padubidri, Hoang Tran Pham, Premkumar Ramasubramani, Umar Saeed, Abdallah M Samy, Monika Sawhney, Tabassom Sedighi, Jaimie D Steinmetz, Ian Tapply, Hugh R Taylor, Muhammad Umair, Theo Vos, and Peng Zheng.
Providing critical feedback on methods or results
Yohannes Habtegiorgis Abate, Mohammad Abdollahi, Tadele Girum Girum Adal, Isaac Yeboah Addo, Kishor Adhikari, Antonella Agodi, Aqeel Ahmad, Hamid Ahmadieh, Hooman Ahmadzadeh, Fares Alahdab, Ahmad Samir Alfaar, Robert Kaba Alhassan, Syed Shujait Shujait Ali, Louay Almidani, Sofia Androudi, Anayochukwu Edward Anyasodor, Jalal Arabloo, Alessandro Arrigo, Mubarek Yesse Ashemo, Seyyed Shamsadin Athari, Desta Debalkie Atnafu, Alok Atreya, Melese Kitu Ayalew, Yared Asmare Aynalem, Zewdu Bishaw Aynalem, Ahmed Y Azzam, Sara Bagherieh, Ruhai Bai, Martina Barchitta, Mainak Bardhan, Till Winfried Bärnighausen, Nebiyou Simegnew Bayileyegn, Fatemeh Bazvand, Ahmet Begde, Babak Behnam, Akshaya Srikanth Bhagavathula, Sonu Bhaskar, Gurjit Kaur Bhatti, Jasvinder Singh Bhatti, Bagas Suryo Bintoro, Rupert R. A. Bourne, Tasanee Braithwaite, Paul Svitil Briant, Katrin Burkart, Yasser Bustanji, Florentino Luciano Caetano dos Santos, Vera L A Carneiro, Muthia Cenderadewi, Vijay Kumar Chattu, Dinh-Toi Chu, Natália Cruz-Martins, Omid Dadras, Xiaochen Dai, Ana Maria Dascalu, Mohsen Dashti, Anna Dastiridou, Maedeh Dastmardi, Xinlei Deng, Nikolaos Dervenis, Vinoth Gnana Chellaiyan Devanbu, Mengistie Diress, Shirin Djalalinia, Michael Ekholuenetale, Temitope Cyrus Ekundayo, Iman El Sayed, Muhammed Elhadi, Mehdi Emamverdi, Ambaw Abebaw Emrie, Adeniyi Francis Fagbamigbe, Ayesha Fahim, Umar Farooq, Hossein Farrokhpour, Ali Fatehizadeh, Alireza Feizkhah, Arthur G Fernandes, Lorenzo Ferro Desideri, Getahun Fetensa, Bikila Regassa Feyisa, Florian Fischer, Seth Flaxman, Ali Forouhari, Matteo Foschi, Kayode Raphael Fowobaje, João M Furtado, Aravind P Gandhi, Tilaye Gebru Gebi, Miglas W Gebregergis, Mesfin Gebrehiwot, Brhane Gebremariam, Molalegn Mesele Gesese, Khalil Ghasemi Falavarjani, Fariba Ghassemi, Sherief Ghozy, Mahaveer Golechha, Sapna Gupta, Veer Bala Gupta, Vivek Kumar Gupta, Teklehaimanot Gereziher Haile, Semira Goitom Hailu, Arvin Haj-Mirzaian, Aram Halimi, Shahin Hallaj, Billy Randall Hammond, Ikramul Hasan, Hamidreza Hasani, Hossein Hassanian-Moghaddam, Mahsa Heidari-Foroozan, Sung Hwi Hong, Praveen Hoogar, Mehdi Hosseinzadeh, Chengxi Hu, Hong-Han Huynh, Mustapha Immurana, Chidozie C D Iwu, Louis Jacob, Mihajlo Jakovljevic, Shubha Jayaram, Mohammad Jokar, Jost B Jonas, Nitin Joseph, Charity Ehimwenma Joshua, Gebisa Guyasa Kabito, Laleh R Kalankesh, Sagarika Kamath, Himal Kandel, Ibraheem M Karaye, Gbenga A Kayode, Shemsu Kedir, Yousef Saleh Khader, Himanshu Khajuria, Moawiah Mohammad Khatatbeh, Mahalaqua Nazli Khatib, Zahra Khorrami, Yun Jin Kim, Adnan Kisa, Sezer Kisa, Ai Koyanagi, Kewal Krishan, Chandrakant Lahariya, Tri Laksono, Dharmesh Kumar Lal, Van Charles Lansingh, Trang Diep Thanh Le, Munjae Lee, Seung Won Lee, Wei-Chen Lee, Nicolas Leveziel, Stephen S Lim, Xuefeng Liu, Alireza Mahmoudi, Razzagh Mahmoudi, Kashish Malhotra, Vahid Mansouri, Roy Rillera Marzo, Andrea Maugeri, Colm McAlinden, Tesfahun Mekene Meto, Abera M Mersha, Tomislav Mestrovic, Ephrem Tesfaye Mihretie, Mehdi Mirzaei, Prasanna Mithra, Nouh Saad Mohamed, Soheil Mohammadi, Abdulwase Mohammed, Ali H Mokdad, Hossein Molavi Vardanjani, Mohammad Ali Moni, Fateme Montazeri, Maryam Moradi, Ahmed Nuru Muhamed, Admir Mulita, Ganesh R Naik, Shumaila Nargus, Zuhair S Natto, Biswa Prakash Nayak, Mohammad Negaresh, Hadush Negash, Seyed Aria Nejadghaderi, Dang H Nguyen, Hien Quang Nguyen, Phat Tuan Nguyen, Van Thanh Nguyen, Robina Khan Niazi, Ogochukwu Janet Nzoputam, Ismail A Odetokun, Andrew T Olagunju, Matthew Idowu Olatubi, Obinna E Onwujekwe, Michal Ordak, Uchechukwu Levi Osuagwu, Nikita Otstavnov, Mayowa O Owolabi, Jagadish Rao Padubidri, Parsa Panahi, Ashok Pandey, Shahina Pardhan, Jay Patel, Shrikant Pawar, Arokiasamy Perianayagam, Ionela-Roxana Petcu, Hoang Tran Pham, Ibrahim Qattea, Pankaja Raghav Raghav, Fakher Rahim, Vafa Rahimi-Movaghar, Mosiur Rahman, Premkumar Ramasubramani, Ahmed Mustafa Rashid, Annisa Utami Rauf, Elrashdy Moustafa Mohamed Redwan, Serge Resnikoff, Nazila Rezaei, Priyanka Roy, Zahra Saadatian, Siamak Sabour, Basema Saddik, Umar Saeed, Sare Safi, Sher Zaman Safi, Narjes Saheb Sharif-Askari, Joseph W Sakshaug, Mohamed A Saleh, Yoseph Leonardo Samodra, Vijaya Paul Samuel, Abdallah M Samy, Monika Sawhney, Mete Saylan, Sayed Mansoor Sediqi, Yashendra Sethi, Jaffer Shah, Samiah Shahid, Masood Ali Shaikh, Muhammad Aaqib Shamim, Maryam Shayan, Mika Shigematsu, Aminu Shittu, Seyed Afshin Shorofi, Emmanuel Edwar Siddig, Juan Carlos Silva, Jasvinder A Singh, Paramdeep Singh, Eirini Skiadaresi, Chandrashekhar T Sreeramareddy, Vladimir I Starodubov, Ian Tapply, Birhan Tsegaw Taye, Jansje Henny Vera Ticoalu, Guesh Mebrahtom Tsegay, Saif Ullah, Muhammad Umair, Sahel Valadan Tahbaz, Theo Vos, Nuwan Darshana Wickramasinghe, Guadie Sharew Wondimagegn, Arzu Yiğit, Dong Keon Yon, Naohiro Yonemoto, Yuyi You, Mikhail Sergeevich Zastrozhin, Hanqing Zhao, and Magdalena Zielińska.
Drafting the work or revising it critically for important intellectual content
Yohannes Habtegiorgis Abate, Mohammad Abdollahi, Tadele Girum Girum Adal, Isaac Yeboah Addo, Prerna Agarwal, Antonella Agodi, Hamid Ahmadieh, Hooman Ahmadzadeh, Fares Alahdab, Ahmad Samir Alfaar, Robert Kaba Alhassan, Syed Shujait Shujait Ali, Louay Almidani, Abhishek Anil, Anayochukwu Edward Anyasodor, Jalal Arabloo, Alessandro Arrigo, Seyyed Shamsadin Athari, Desta Debalkie Atnafu, Alok Atreya, Melese Kitu Ayalew, Ahmed Y Azzam, Sara Bagherieh, Martina Barchitta, Mainak Bardhan, Till Winfried Bärnighausen, Maurizio Battaglia Parodi, Ahmet Begde, Akshaya Srikanth Bhagavathula, Sonu Bhaskar, Gurjit Kaur Bhatti, Jasvinder Singh Bhatti, Marina G Birck, Rupert R. A. Bourne, Tasanee Braithwaite, Paul Svitil Briant, Yasser Bustanji, Florentino Luciano Caetano dos Santos, Muthia Cenderadewi, Vijay Kumar Chattu, Dinh-Toi Chu, Maria Vittoria Cicinelli, Natália Cruz-Martins, Ana Maria Dascalu, Anna Dastiridou, Maedeh Dastmardi, Nikolaos Dervenis, Joshua R Ehrlich, Michael Ekholuenetale, Iman El Sayed, Muhammed Elhadi, Mehdi Emamverdi, Ambaw Abebaw Emrie, Adeniyi Francis Fagbamigbe, Ayesha Fahim, Ali Fatehizadeh, Arthur G Fernandes, Getahun Fetensa, Florian Fischer, Seth Flaxman, Ali Forouhari, Matteo Foschi, João M Furtado, Aravind P Gandhi, Tilaye Gebru Gebi, Miglas W Gebregergis, Mesfin Gebrehiwot, Brhane Gebremariam, Gebreamlak Gebremedhn Gebremeskel, Yibeltal Yismaw Gela, Fariba Ghassemi, Sherief Ghozy, Sapna Gupta, Veer Bala Gupta, Vivek Kumar Gupta, Teklehaimanot Gereziher Haile, Aram Halimi, Shahin Hallaj, Billy Randall Hammond, Ikramul Hasan, Hamidreza Hasani, Hong-Han Huynh, Mustapha Immurana, Chidozie C D Iwu, Louis Jacob, Abdollah Jafarzadeh, Mihajlo Jakovljevic, Shubha Jayaram, Jost B Jonas, Nitin Joseph, Charity Ehimwenma Joshua, Gebisa Guyasa Kabito, Sagarika Kamath, Himal Kandel, Hengameh Kasraei, Gbenga A Kayode, Shemsu Kedir, Yousef Saleh Khader, Himanshu Khajuria, Moawiah Mohammad Khatatbeh, Mahalaqua Nazli Khatib, Adnan Kisa, Sezer Kisa, Ai Koyanagi, Kewal Krishan, Chandrakant Lahariya, Van Charles Lansingh, Janet L Leasher, Nicolas Leveziel, Xuefeng Liu, Razzagh Mahmoudi, Vahid Mansouri, Roy Rillera Marzo, Andrea Maugeri, Colm McAlinden, Tesfahun Mekene Meto, Tomislav Mestrovic, Ephrem Tesfaye Mihretie, Mehdi Mirzaei, Prasanna Mithra, Nouh Saad Mohamed, Soheil Mohammadi, Abdulwase Mohammed, Ali H Mokdad, Hossein Molavi Vardanjani, Mohammad Ali Moni, Fateme Montazeri, Maryam Moradi, Parsa Mousavi, Kovin S Naidoo, Shumaila Nargus, Zuhair S Natto, Biswa Prakash Nayak, Mohammad Negaresh, Hadush Negash, Seyed Aria Nejadghaderi, Dang H Nguyen, Hien Quang Nguyen, Phat Tuan Nguyen, Van Thanh Nguyen, Robina Khan Niazi, Mamoona Noreen, Ogochukwu Janet Nzoputam, Ismail A Odetokun, Andrew T Olagunju, Matthew Idowu Olatubi, Obinna E Onwujekwe, Michal Ordak, Uchechukwu Levi Osuagwu, Nikita Otstavnov, Mayowa O Owolabi, Jagadish Rao Padubidri, Shahina Pardhan, Jay Patel, Venkata Suresh Patthipati, Shrikant Pawar, Arokiasamy Perianayagam, Ionela-Roxana Petcu, Hoang Tran Pham, Ibrahim Qattea, Pankaja Raghav Raghav, Fakher Rahim, Vafa Rahimi-Movaghar, Mohammad Hifz Ur Rahman, Premkumar Ramasubramani, Ahmed Mustafa Rashid, Elrashdy Moustafa Mohamed Redwan, Serge Resnikoff, Nazila Rezaei, Priyanka Roy, Siamak Sabour, Basema Saddik, Umar Saeed, Amene Saghazadeh, Fatemeh Saheb Sharif-Askari, Amirhossein Sahebkar, Saina Salahi, Sarvenaz Salahi, Vijaya Paul Samuel, Abdallah M Samy, Aswini Saravanan, Monika Sawhney, Mete Saylan, Siddharthan Selvaraj, Yashendra Sethi, Allen Seylani, Jaffer Shah, Samiah Shahid, Moyad Jamal Shahwan, Muhammad Aaqib Shamim, Mika Shigematsu, Aminu Shittu, Seyed Afshin Shorofi, Emmanuel Edwar Siddig, Jasvinder A Singh, Paramdeep Singh, Eirini Skiadaresi, Raúl A R C Sousa, Chandrashekhar T Sreeramareddy, Vladimir I Starodubov, Birhan Tsegaw Taye, Miltiadis K Tsilimbaris, Saif Ullah, Muhammad Umair, Sahel Valadan Tahbaz, Theo Vos, Nuwan Darshana Wickramasinghe, Guadie Sharew Wondimagegn, Lin Yang, Arzu Yiğit, Dong Keon Yon, Naohiro Yonemoto, Mikhail Sergeevich Zastrozhin, Makan Ziafati, and Magdalena Zielińska.
Managing the estimation or publications process
Rupert R. A. Bourne, João M Furtado, Ali H Mokdad, and Theo Vos
Vision Loss Expert Group of the Global Burden of Disease Study
Providing data or critical feedback on data sources
Alessandro Arrigo, Maurizio Battaglia Parodi, Mukharram M Bikbov, Rupert R A Bourne, Tasanee Braithwaite, Alain Bron, Ching-Yu Cheng, Maria Vittoria Cicinelli, Nathan Congdon, Monte A Del Monte, Joshua R Ehrlich, Arthur Fernandes, Seth Flaxman, Tim Fricke, David Friedman, João M Furtado, Gus Gazzard, M Elizabeth Hartnett, Jost B Jonas, Rim Kahloun, John H Kempen, Moncef Khairallah, Rohit C Khanna, Judy E Kim, Van Charles Lansingh, Janet Leasher, Nicolas Leveziel, Kovin S Naidoo, Vinay Nangia, Michal Nowak, Konrad Pesudovs, Tunde Peto, Pradeep Ramulu, Serge Resnikoff, Tabassom Sedighi, Ian Tapply, Hugh Taylor, Fotis Topouzis, Miltiadis Tsilimbaris, Ya Xing Wang, Ningli Wang
Developing methods or computational machinery
Rupert R A Bourne, Jost B Jonas, Ian Tapply
Providing critical feedback on methods or results
Alessandro Arrigo, Mukharram M Bikbov, Rupert R A Bourne, Tasanee Braithwaite, Monte A Del Monte, David Friedman, João M Furtado, M Elizabeth Hartnett, Jost B Jonas, Rim Kahloun, John H Kempen, Konrad Pesudovs, Serge Resnikoff, Ian Tapply, Ningli Wang
Drafting the work or revising it critically for important intellectual content
Alessandro Arrigo, Mukharram M Bikbov, Rupert R A Bourne, Tasanee Braithwaite, Nathan Congdon, Monte A Del Monte, João M Furtado, M Elizabeth Hartnett, Jost B Jonas, Janet Leasher, Konrad Pesudovs
Managing the estimation or publications process
Rupert R A Bourne, João M Furtado, Jost B Jonas
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Vision Loss Expert Group of the Global Burden of Disease Study., the GBD 2019 Blindness and Vision Impairment Collaborators. Global estimates on the number of people blind or visually impaired by age-related macular degeneration: a meta-analysis from 2000 to 2020. Eye 38, 2070–2082 (2024). https://doi.org/10.1038/s41433-024-03050-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41433-024-03050-z
- Springer Nature Limited