
Abstract
Cytomegalovirus (CMV) is a widely prevalent herpesvirus that reaches seroprevalence rates of up to 95% in several parts of the world. The majority of CMV infections are asymptomatic, albeit they have severe detrimental effects on immunocompromised individuals. Congenital CMV infection is a leading cause of developmental abnormalities in the USA. CMV infection is a significant risk factor for cardiovascular diseases in individuals of all ages. Like other herpesviruses, CMV regulates cell death for its replication and establishes and maintains a latent state in the host. Although CMV-mediated regulation of cell death is reported by several groups, it is unknown how CMV infection affects necroptosis and apoptosis in cardiac cells. Here, we infected primary cardiomyocytes, the contractile cells in the heart, and primary cardiac fibroblasts with wild-type and cell-death suppressor deficient mutant CMVs to determine how CMV regulates necroptosis and apoptosis in cardiac cells. Our results reveal that CMV infection prevents TNF-induced necroptosis in cardiomyocytes; however, the opposite phenotype is observed in cardiac fibroblasts. CMV infection also suppresses inflammation, reactive oxygen species (ROS) generation, and apoptosis in cardiomyocytes. Furthermore, CMV infection improves mitochondrial biogenesis and viability in cardiomyocytes. We conclude that CMV infection differentially affects the viability of cardiac cells.
Similar content being viewed by others


Introduction
Cytomegalovirus (CMV) is a double-stranded DNA virus that belongs to the beta-herpesviridae family [1]. The serological prevalence of CMV infection ranges from 40–95% of the population worldwide, and approximately 1/3rd of children in the USA are infected with CMV by the age of five [2,3,4]. CMV infection is subclinical in immunocompetent individuals whereas reactivation of the virus in immunocompromised individuals leads to multi-organ disease and death [5, 6]. In vivo studies on cell tropism have suggested that endothelial, epithelial, fibroblast, and smooth muscle cells are the major targets of CMV lytic infection, whereas myeloid cells of hematopoietic origin including monocytes and polymorphonuclear leukocytes are permissive to infection but do not support lytic replication [7,8,9,10]. CMV infection is linked to an increased risk of cardiovascular disease (CVD), and a meta-analysis of community-based prospective studies showed that CMV infection attributes to 13.4% of CVD incidence [11]. CMV infection is involved in allograft rejection in pediatric heart transplant recipients [12]. Also, CMV infection mismatch in donor and recipient patients causes complications impairing outcomes in heart transplantation [13]. The inflammatory status of chronic heart failure (CHF) patients is directly related to CMV infection. CMV infection promotes the production of pro-inflammatory cytokines, and the concentrations of cytokines (tumor necrosis factor-alpha (TNFα), Interleukin-6 (IL-6), IL-17A, and IL-1β) are positively correlated to the production of antibodies against CMV in CHF patients [14]. Cytokines are released from the dying cardiac cells, and they induce adverse cardiac remodeling [15]. Long-term CMV infection is linked to the instigation of adverse cardiac remodeling by inducing cardiac hypertrophy and fibrosis [16]. However, the direct effect of CMV infection on cardiac cell death remains unclear.
Human CMV (HCMV) and mouse CMV (MCMV) have similar pathogenesis on the heart, and both promote inflammation to induce myocarditis [16,17,18]. In the present study, we have used MCMV, and determined its effects on cardiac cell death. At least six forms of cell death have been reported in the heart, namely apoptosis, necroptosis, mitochondrial-mediated necrosis, pyroptosis, ferroptosis, and autophagic cell death [19]. In the present study, we focused on apoptosis and necroptosis cell death mechanisms in cardiomyocytes and fibroblast cells. MCMV replicates and establishes latency in host cells by synthesizing viral suppressors of necroptosis and apoptosis signaling molecules [20,21,22]. Apoptosis is a well-characterized caspase-dependent cell death mechanism, which is triggered by both caspase-9-mediated intrinsic (mitochondrial-dependent) and caspase-8-mediated extrinsic signaling pathways [23, 24]. Extrinsic cell death signaling involves the activation of different death receptors, including TNF receptor-1 (TNFR1) [25]. In the presence of a caspase-8 inhibitor, extrinsic signaling can shift from apoptosis to a form of programmed necrosis termed necroptosis [26]. Necroptotic cell death is mediated by the interaction of Receptor Interacting Protein Kinase-3 (RIPK3) with adaptor proteins, such as RIPK1, Z-DNA binding protein-1 (ZBP1, also termed DAI) - a virus-induced nucleic acid sensor protein, and TIR-domain-containing adaptor-inducing interferon-β (TRIF), which is involved in response to activation of Toll-Like Receptors (TLRs) [27,28,29]. These interactions occur through a small protein-protein interaction motif known as RIP homotypic interaction motif (RHIM). Activation of different receptors and interaction of adapter proteins with RIPK3 lead to RIPK3 phosphorylation and activation [30]. The activated RIPK3 phosphorylates Mixed Lineage Kinase-Like (MLKL), a downstream effector molecule in the necroptosis pathway, which undergoes oligomerization and subsequently cell membrane insertion leading to cell swelling, disruption of plasma membrane integrity, and cell lysis [31, 32].
MCMV encodes the M45 gene, which is the first identified Viral Inhibitor of Receptor- interacting protein Activation (vIRA) that inhibits necroptosis [29]. M45 contains a RHIM and inhibits RIPK3 through RHIM-dependent interaction during infection to suppress the ZBP1‐RIPK3‐dependent necroptosis [33]. Increased necroptosis is an important innate anti-viral response by host cells [34]. Furthermore, MCMV suppresses apoptosis by encoding a Viral Inhibitor of Caspase-8-dependent apoptosis (vICA) - a product of the M36 gene, and loss of this gene product (∆M36) promotes caspase-8-mediated apoptosis [35,36,37]. Notably, caspase-8 is also involved in necroptosis and inflammatory signaling. Caspase-8 negatively regulates RIPK3 to inhibit necroptosis and restricts RIPK3-dependent proinflammatory IL-1β production [38, 39]. MCMV also employs two inhibitors of intrinsic apoptosis, the Viral Mitochondria-localized Inhibitor of Apoptosis (vMIA) encoded by m38.5, and the Viral Inhibitor of Bak Oligomerization (vIBO) encoded by m41.1, which suppresses the pro-apoptotic Bcl2-family members Bax and Bak, respectively. The loss of m38.5 and m41.1 gene products leads to apoptosis during MCMV infection [40,41,42,43]. Although MCMV infection is reported to inhibit non-cardiac cell death, how MCMV infection affects necroptosis and apoptosis in cardiac cells remains unclear. Here, we used primary cardiomyocytes and cardiac fibroblasts to investigate MCMV infection-induced regulation of necroptosis and apoptosis.
Results
MCMV infection prevents TNFα-induced necroptosis in cardiomyocytes possibly by suppressing inflammation
To determine the effect of MCMV infection on necroptosis in cardiomyocytes, we standardized the multiplicity and duration of MCMV infection using HL1 cell line, which has murine origin and exhibits several features of cardiomyocytes [44]. After time course and dose optimization studies (Fig. S1), we decided to use 5 MOI of MCMV and 24 h treatment duration for all studies with cardiac cells. We infected primary (neonatal) cardiomyocytes with WT MCMV (K181-bac) in the presence of necroptosis inducer TSZ, where T stands for TNFα, S stands for smac-mimetic compound SM-164, and Z stands for a pan-caspase inhibitor zVAD [45]. Since infection of susceptible cells with a virus mutated in the RHIM domain of M45 (M45mutRHIM) induces ZBP1-RIPK3-dependent necroptosis [33], we also infected primary cardiomyocytes with M45mutRHIM MCMV, treated them with TSZ, and evaluated their cell viability. We found that MCMV infection prevents TSZ-induced necroptosis in cardiomyocytes, which is independent of the DAI/ZBP1-RIPK3-mediated necroptosis pathway (Fig. 1A).

A Viability of neonatal cardiomyocytes obtained from C57BL/6 J mice were treated with necroptosis inducing agents TSZ in the presence and absence of MCMV (WT or M45mutRHIM mutant MCMV) infection. B Viability of neonatal cardiomyocytes treated with TSZ in the presence and absence of necroptosis inhibitor GSK872 (RIPK3 inhibitor) or Nec-1 (RIPK1 inhibitor). C Phase-contrast image and viability assessed by ATP levels in WT and M45mutRHIM mutant CMV-infected of neonatal cardiomyocytes. D Inflammatory cytokine Interleukin-1 beta (IL-1β) was measured in the culture medium of neonatal cardiomyocytes infected with WT or M45mutRHIM mutant MCMV. WT CMV = K-181-bac. One-way ANOVA followed by Tukey’s multiple comparison test was performed. Values are mean ± SE. Each point represents one sample. n = 4–6. ***P < 0.001; ****P < 0.0001.
To determine the role of RIPK3 and RIPK1 in necroptosis of cardiomyocytes (without MCMV infection), we treated primary cardiomyocytes with GSK872 (a RIPK3 inhibitor) and Nec-1 (a RIPK1 inhibitor) in the presence of TSZ and evaluated cell viability. We observed that inhibition of both RIPK3 and RIPK1 blunts the detrimental effects of TSZ on cardiomyocyte viability (Fig. 1B). This finding demonstrates that the RIPK1 and RIPK3-mediated necroptosis contributes to decreased cell viability in cardiomyocytes. Furthermore, the RIPK3-mediated necroptosis has a more pronounced effect on cell viability than the RIPK1-mediated necroptosis in cardiomyocytes.
To evaluate if MCMV infection improves the viability of cardiomyocytes independent of necroptosis (in the absence of chemical inducer TSZ), we measured cell viability in uninfected (MOCK), and WT and M45mutRHIM MCMV infected primary cardiomyocytes. We observed that WT MCMV infection increased the viability of primary cardiomyocytes, which was further enhanced by M45mutRHIM mutation in MCMV (Fig. 1C). We also observed a similar effect of WT and M45mutRHIM CMV infection on the improvement of cell viability and attenuation of cytotoxicity in HL1 cells (Fig. S2). Altogether, these findings suggest that MCMV infection promotes the viability of cardiomyocytes irrespective of necroptosis, and that cardiomyocytes are resistant to MCMV-induced necroptosis.
To confirm that the improvement in cell viability of cardiomyocytes is mainly due to MCMV infection, we measured viral proteins required for successful MCMV infection (Immediate Early-1 or IE1, Early protein-1 or E1) and replication (MCMV envelope glycoprotein or gB) in uninfected (MOCK), and WT and M45mutRHIM MCMV-infected HL1 cells. We found that these three virus proteins were expressed to comparable levels in the WT and M45mutRHIM MCMV-infected HL1 cells and not in the uninfected cells (Fig. S3). These findings corroborate MCMV infection and demonstrate that improvement in the viability of HL1 cells was due to MCMV infection.
Inflammation is an upstream signal for necroptosis since inflammation induces TNFα, which in turn instigates necroptosis. In mice, MCMV infection in the heart promotes TNFα expression [18]. Furthermore, circulating levels of inflammatory cytokine IL-1β are positively associated with anti-HCMV titer in CHF patients [14]. Therefore, we measured the secreted IL-1β in the culture medium of uninfected, WT and M45mutRHIM MCMV-infected cardiomyocytes. We found a remarkable decrease in IL-1β in WT MCMV-infected cardiomyocytes, which was further decreased in M45mutRHIM MCMV-infected cardiomyocytes (Fig. 1D). These findings suggest that suppression of upstream inflammation could be a potential mechanism by which MCMV infection prevents initiation of necroptosis and presumably cell death in cardiomyocytes. In addition, our results suggest that the necroptosis-specific mutation (M45mutRHIM) in MCMV contributes to the attenuation of inflammation in cardiomyocytes.
MCMV infection inhibits apoptosis in cardiomyocytes by reducing ROS
Apoptosis is triggered either by caspase-8 signaling that directly activates caspase-3/7 by cleaving pro-caspase-3/7 or by truncating Bcl-2 homology (BH)-3interacting-domain death agonist (BID) that induces mitochondrial-mediated caspase-3 activation through cytochrome c release [19]. We used two mutant MCMVs, one lacking caspase-8 inhibition (∆M36) and another lacking mitochondrial-mediated apoptosis inhibition (∆M38.5/41.1). To determine the effects of caspase-8 on cardiomyocyte viability, we infected primary cardiomyocytes with MOCK, WT, and three mutant MCMVs (M45mutRHIM, ∆M36, and ∆M38.5/41.1) and measured caspase-3/7 and caspase-8 activity. We found only mitochondrial-mediated apoptotic mutant MCMV (∆M38.5/41.1) infection was able to increase caspase-3/7 and caspase-8 activity (Fig. 2A, B). These findings suggest that MCMV infection inhibits mitochondrial-mediated apoptosis in cardiomyocytes independent of the necroptosis pathway.

A–B. Caspase-3/7 and caspase-8 activity in uninfected (MOCK), and WT, M45mutRHIM, ∆M36, and ∆M38.5/41.1 MCMV infected neonatal cardiomyocytes. C Staining of cellular oxidative stress (ROS) by CellROX and its quantification in neonatal cardiomyocytes infected with WT MCMV and M45mutRHIM MCMV. D Staining of mitochondrial ROS by MitoSOX and its quantification (n = 3 samples in each group). WT CMV = K-181-bac, ∆M36 = mutant CMV mutant promotes caspase-8-mediated apoptosis, ∆M38.5/41.1 CMV = mutant CMV promotes mitochondria-mediated (Bax/Bak) apoptosis. One-way ANOVA followed by Tukey’s multiple comparison test was performed. Values are mean ± SE. Each point represents one sample. n = 5–6 in (A–B) and n = 3 in (C–D). *P < 0.05; **P < 0.01; ***P < 0.001; ****P < 0.0001.
Mitochondrial-mediated apoptosis is triggered by intrinsic stimuli such as reactive oxygen species (ROS). Notably, the necroptosis pathway may regulate ROS to influence mitochondrial-mediated apoptosis [46]. Thus, we measured cytosolic and mitochondrial ROS levels in MOCK, WT, and necroptosis mutant (M45mutRHIM) MCMV-infected primary cardiomyocytes. We observed that both WT and M45mutRHIM MCMV infections reduced the cytosolic and mitochondrial levels of ROS (Fig. 2C, D). Similar findings were also observed in HL1 cells (Fig. S4). These results suggest that CMV may inhibit mitochondrial-mediated apoptosis by decreasing ROS levels in cardiomyocytes.
MCMV infection promotes mitochondrial biogenesis to increase the viability of cardiomyocytes
Impaired mitochondrial biogenesis may contribute to increases in ROS levels [47]. Thus, we measured mitochondria biogenesis (mitochondrial DNA copy number) and the number of mitochondria (using mitotracker green) in the uninfected (MOCK), WT MCMV, and M45mutRHIM MCMV-infected primary cardiomyocytes. Both WT and M45mutRHIM MCMV infection increased mitochondrial biogenesis and the number of mitochondria in cardiomyocytes (Fig. 3A, B). We also measured different mitochondrial biogenesis markers (PGC1α, TFAM, and mitotracker) in HL1 cells and observed increased mitochondrial biogenesis, complementing the results from primary cardiomyocytes (Fig. S5). The improved mitochondrial biogenesis may reduce ROS and subsequent ROS-induced apoptosis to improve cell viability. Thus, we determined cell viability in WT and M45mutRHIM MCMV-infected cardiomyocytes after 24 h treatment with apoptosis inducer TS, where T stands for TNFα and S stands for smac-mimetic compound SM-164. Both WT and M45mutRHIM MCMV infections blunt the detrimental effects of TS on cell viability in cardiomyocytes (Fig. 3C). These findings suggest that MCMV infection increased cell viability, potentially by improving mitochondrial biogenesis in cardiomyocytes.

A Mitochondrial DNA copy number assessed by D-loop in uninfected (MOCK), WT MCMV, and M45mutRHIM MCMV infected neonatal cardiomyocytes. B Morphology and cell viability of uninfected and WT and M45mutRHIM MCMV infected neonatal primary cardiomyocytes. C Effect of apoptosis inducer TS on viability of uninfected, WT MCMV, and M45mutRHIM MCMV infected neonatal cardiomyocytes. WT CMV = K-181- bac. One-way ANOVA followed by Tukey’s multiple comparison test was performed. Values are mean ± SE. Each point represents one sample. n = 4–6 in each group. *P < 0.05; **P < 0.01; ***P < 0.001.
MCMV infection induces cell death in cardiac fibroblasts
Since fibroblasts play a crucial role in cardiac fibrosis and dysfunction, we next evaluated how MCMV infection influences cardiac fibroblasts [48]. We first characterized cardiac fibroblasts isolated from the four to five-week-old murine heart and then evaluated their cell cytotoxicity and viability. The presence of vimentin, a marker of fibroblast, validated the isolation of uncontaminated primary cardiac fibroblasts (Fig. 4A). MCMV infection increased cytotoxicity (increased LDH levels) and impaired viability (decreased ATP levels) in cardiac fibroblasts (Fig. 4B, C). These results demonstrate that MCMV infection promotes cytotoxicity and decreases cell viability in primary cardiac fibroblasts. Moreover, the MCMV infection-induced cell death in cardiac fibroblasts was associated with an increase in TNFα levels (Fig. S6). Since TNFα promotes cell death via necroptosis, we evaluated necroptosis in cardiac fibroblasts after infection with WT and M45mutRHIM CMV. We observed that necroptosis markers (RIPK3 and ZBP1) were upregulated by WT MCMV infection and further enhanced by M45mutRHIM CMV infection in cardiac fibroblasts (Fig. 4D–E). Altogether, these findings demonstrate that MCMV infection promotes cell death via necroptosis in cardiac fibroblasts.

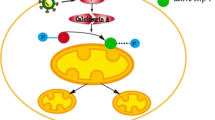
A Imaging cardiac fibroblasts immunofluorescence by Phase-contrast and vimentin. B Cell toxicity measurement by lactate dehydrogenase (LDH) release in uninfected (MOCK), WT MCMV, and M45mutRHIM MCMV infected cardiac fibroblasts. C Cell viability evaluation by ATP levels in uninfected (MOCK), WT MCMV, and M45mutRHIM MCMV infected cardiac fibroblasts. D Immunoblot and quantification of pRIPK3/RIPK3 in cardiac fibroblasts infected with WT and M45mutRHIM MCMV. E Immunoblot and quantification of ZBP1 in cardiac fibroblasts infected with WT and M45mutRHIM MCMV. F ZBP1 and RIP3 protein-protein-interactions in RHIM 1 and RHIM 2 domain. RHIM motif sequences for ZBP1 and RIPK3 were obtained from Uniprot database Q9QY24, Q9QZL0, respectively. Sequences were aligned using SnapGene software using global alignment tool (Needleman–Wunsch), identical amino acids are highlighted in black, similar amino acids in blue, and different amino acids in red. In 3 predicted models for ZBP1 binding to RIPK3, both ZBP1 and RIPK3 structures were obtained from alpha-fold database Q9QY24, Q9QZL0, respectively. Structural docking was performed using ClusPro for Protein-Protein docking. All models were analyzed for interaction sites, and only models with interactions through RHIM domains were considered in the analysis. Pymol and ChimeraX were used for analysis. Protein affinity binding was measured using prodigy webtool to calculate ∆G and Kd between the two proteins. G Schematic illustration of MCMV-mediated suppression of cell death in cardiomyocytes and induction of cell death in cardiac fibroblasts. BioRender was used to create this figure. WT CMV = K-181- bac. One-way ANOVA followed by Tukey’s multiple comparison test was performed. Values are mean ± SE. Each point represents one sample. n = 4–6 in each group. *P < 0.05; **P < 0.01; ***P < 0.001; ****P < 0.0001.
Notably, the molecular weight of ZBP1 varies between cardiomyocytes (42 kDa) and fibroblasts (55 kDa), pointing to a possibility of different ZBP1 variants in cardiomyocytes versus other cardiac cells (Figs. S7 and 4E). Our search in NCBI showed two validated splice variants (molecular weights 44 kDa and 20 kDa) of mouse ZBP1 where the second variant lacks both RHIMs (Fig. S8). ZBP1 interacts with RIPK3 via RHIM1 suggesting that splice variants without a RHIM (20 kDa) are unlikely to interact with RIPK3. ZBP1 is known to interact with several proteins, which are involved in inflammation and other cell signaling pathways, including the cell death pathway via RIPK1 and RIPK3 (Fig. S9). There is no defined or validated motif of ZBP1. To determine a predicted protein-protein interaction of ZBP1 and RIPK3, we acquired predicted ZBP1 protein structure using the AlphaFold protein structure database. We used both PyMOL and ChimeraX programs for predicted ZBP1 structural analysis and ClusPro web server for the predicted molecular docking of ZBP1 on RIPK3. Based on the high binding affinity analyzed by prodigy software, we propose three structural models for the predicted ZBP1 motif binding to RIPK3 through RHIM motifs, where each model represents a different docking position between the two proteins (Fig. 4F). However, these predicted models warrant further validation.
Altogether, these findings suggest that MCMV infection affects cell death differentially in cardiomyocytes and cardiac fibroblasts. In cardiomyocytes, MCMV infection promotes cell viability by inhibiting necroptosis and apoptosis, and by promoting mitochondrial biogenesis, whereas in cardiac fibroblasts, MCMV infection promotes cell death by inducing inflammation and necroptosis (Fig. 4G).
Discussion
Several clinical studies have demonstrated that CMV infection promotes CVD; however, the impact of CMV infection on cardiac cell viability remains unclear. Our studies reveal that CMV infection differentially influences cardiac cell viability in the murine heart by promoting the viability of cardiomyocytes while decreasing the viability of cardiac fibroblasts. One of the potential mechanisms of improved viability in MCMV-infected cardiomyocytes is the inhibition of both necroptosis and apoptosis.
Host cells eliminate viruses by inducing programmed cell death, such as necroptosis. However, programming death of terminally differentiated cardiomyocytes is an irreparable loss that could lead to heart failure. Thus, limiting programmed cell death in cardiomyocytes at the expense of carrying out CMV infection is potentially a critical adaptive mechanism that prevents heart failure. Improving the viability of cardiomyocytes is also affordable to CMV infection, which could provide an opportunity for the virus to replicate in these cells. Thus, cardiomyocytes are in a unique position where it is advantageous for both the host and CMV to save the cell from death. In other cardiac cells, such as fibroblasts, which are not as indispensable as myocytes, virus-infected cells are programmed to die to eliminate virus infection. Thus, cardiomyocytes and other cardiac cells may have developed different strategies to adapt to virus infection. This is the first report that shows that the same virus differentially regulates the fate of two different cell types in the same tissue.
Herpesvirus is known to induce and block apoptosis at multiple steps during infection, and protect cells from the extrinsic cell death in a cell-type-dependent manner [49]. Our results show that MCMV infection promotes the viability of cardiomyocytes by increasing mitochondrial biogenesis, reducing ROS accumulation and inflammation, and inhibiting necroptotic and apoptotic signaling pathways. MCMV is known to use multiple strategies to evade the host cell’s programmed cell death mechanisms [50]. In cardiomyocytes, MCMV utilizes these established mechanisms to promote the survival of cardiomyocytes, although other unrecognized mechanisms may play additional roles. This is also the first report demonstrating that MCMV infection induces mitochondrial biogenesis and suppresses inflammation in cardiomyocytes.
DNA of CMV is detected in the atherosclerotic plaques, and CMV is involved in the development of atherosclerosis [51, 52]. However, there are inconsistent reports on the relationship of serum CMV seropositivity with the incidence of CVD [53, 54]. A recent meta-analysis on multiple studies that were performed to assess the effect of CMV infection on relative risk of CVD - ischemic heart disease, stroke, and cardiovascular death - revealed that CMV infection is associated with an increased risk of CVD [11]. However, none of these studies investigated the effect of CMV infection on cardiac cells. The present study reveals how MCMV infection differentially regulates cell viability in cardiomyocytes and cardiac fibroblasts, and their underlying molecular mechanisms. MCMV infection prevents the host cell death by modulating necroptosis [29]. In cardiomyocytes, both RIPK1 and RIPK3 inhibitors mitigate cytokine-induced cell death and thereby improve cell viability, which supports the previous report that necroptosis contributes to myocardial cell death [19]. MCMV requires the RHIM-containing vIRA to prevent the RIPK3-mediated necroptosis, and mutation in the RHIM (M45mutRHIM) augments TNFα-induced necroptosis [33]. In cardiomyocytes, M45mutRHIM does not sensitize cells to the TNFα-induced necroptosis, as cell viability after TSZ treatment remains unchanged between WT and M45mutRHIM MCMV-infected cardiomyocytes. Notably, MCMV infection decreases inflammation (IL-1β) in cardiomyocytes, which was enhanced by the M45mutRHIM mutation, pointing to a potential role of attenuated inflammation in the viability of cardiomyocytes. Based on these findings, we posit that the RHIM of MCMV vIRA may regulate inflammation but not TNFα-induced necroptosis in cardiomyocytes. How the RHIM regulates inflammation in cardiomyocytes remains unclear and requires further investigation.
RIPK3 domain needs adaptor protein ZBP1, a nucleic acid sensor, for necroptosis and IL-1β release [55]. We observed that IL-1β was decreased by the WT MCMV infection in cardiomyocytes, and the decrease was enhanced by the M45mutRHIM mutation. Thus, there is a possibility that RIPK3 and ZBP1 may have differential interactions in cardiomyocytes leading to the attenuation of inflammation and inhibition of necroptosis. ZBP1 also binds to the Z-nucleic acid-binding domain (ZBD) of the RNA-editing enzyme ADAR1, which is a negative regulator of ZBP1 [56]. We observed different molecular weights of ZBP1 in cardiomyocytes (42 kDa) and fibroblasts (55 kDa). At least two validated splice variants of mouse ZBP1 have been reported: (1) a full-length ZBP1 containing two RHIMs (RHIM1 and RHIM 2) and (2) a shorter variant with a predicted molecular weight of 20 kDa lacking any RHIMs. There is potentially more cell type or tissue-specific splice variants of mouse ZBP1, although that remains to be validated. Our observed 42 kDa splice variant could be a novel cardiomyocyte-specific splice variant, which warrants further studies. It is germane to report that human ZBP1 has more validated splice variants than mouse, and the human ZBP1 structure differs from the mouse ZBP1. Thus, the new mouse variants require further validation for their presence or absence in humans. Altogether, our findings suggest a possibility of a new cardiomyocyte-specific variant of ZBP1 (hereafter termed cZBP1), which is different from the cardiac fibroblast variant and contributes to an increase in the viability of cardiomyocytes after MCMV infection.
ZBP1 promotes IL-1β release via the RHIM-mediated interactions with RIPK1 [55]. Thus, there is a possibility that cZBP1 in cardiomyocytes may compromise IL-1β release causing a decrease in inflammation. We observed that attenuation of IL-1β level was comparatively higher in the M45mutRHIM MCMV-infected than the WT MCMV-infected cardiomyocytes. This points to a potential interaction of the MCMV vRIA with the cZBP1 to reduce IL-1β released during infection. As inflammation is an upstream regulator of necroptosis and potentially other forms of cell death, we posit that cZBP1 in cardiomyocytes reduces inflammation, downstream necroptosis, and possibly other cell death signaling resulting in increased viability after MCMV infection. Future studies focusing on interactions of cZBP1 with RIPK3 to regulate IL-1β are warranted.
Like all studies, ours has a few limitations. The first limitation is that we have used only in vitro models. Although we have used primary cardiomyocytes and cardiac fibroblasts in our studies to delineate the specific effects of MCMV infection on specific cardiac cells (cardiomyocytes versus cardiac fibroblasts), a cardiomyocyte-specific or fibroblast-specific loss and gain-of-function mouse model would provide a whole-body effect of MCMV infection. It could also delineate cardiac-specific versus the central mechanism-mediated effects of MCMV infection on the heart. The second limitation is the use of neonatal cardiomyocytes rather than the adult cardiomyocytes. This limitation is due to technical challenges in the culture and treatment of adult cardiomyocytes. We know that the gene expression of neonatal cardiomyocytes is not identical to that of the adult cardiomyocytes. However, despite these limitations, we have uncovered an unexpected difference in the way cardiomyocytes and cardiac fibroblasts respond to viral infection.
In summary, our results reveal that MCMV infection differentially regulates cell death in different cardiac cells. It promotes cell viability in cardiomyocytes while cell death in cardiac fibroblasts. We identify the potential regulatory mechanism by which MCMV infection increased cell viability in cardiomyocytes and cell death in cardiac fibroblasts. We predict a new splice variant of ZBP1 - cZBP1 - in cardiomyocytes, which potentially decreases inflammation and improves viability after MCMV infection. Furthermore, we demonstrate that necroptosis inhibition in cardiomyocytes was independent of RHIM-domain-dependent RIPK3 activation, and concomitant with reduced ROS and inflammation, and increased mitochondrial mass. In contrast to cardiomyocytes, MCMV infection promotes necroptosis and cellular toxicity to decrease viability in cardiac fibroblasts. These are novel and unique features of different cardiac cells to adapt to CMV infection.
Materials and methods
Generation of MCMV mutants
MCMV mutants M45mutRHIM, ∆M36, and ∆M38.5/41.1 have been previously described [29, 50, 57]. Wild type (K181-bac) and mutant viral stocks were generated, clarified, concentrated, and tittered by plaque assay as previously described using NIH 3T3 fibroblasts (ATCC CRL-1658) [58].
Isolation and culture of neonatal cardiomyocytes
For Isolation of neonatal cardiomyocytes, one to two-day old pups from C57BL/6 J mice were decapitated and hearts were dissected out. Primary cardiomyocytes were isolated using Pierce Primary Cardiomyocyte Isolation Kit (Cat # 88281).
Isolation and culture of neonatal cardiac fibroblast
Four to five-week-old C57BL/6 J mice hearts were extracted, washed in ice-cold PBS and HBSS, and minced in 1–3 mm3 pieces. The minced tissue was mixed with 0.1% collagenase II and incubated at 37 °C for an hour in a shaker incubator. Dulbecco’s Modified Eagle Medium (DMEM) medium was added to stop the enzymatic tissue lysis, and lysed tissue was washed in ice-cold HBSS. Cells were counted and cultured in complete DMEM medium containing 5 ng/ml fibroblast growth factor and used for further treatments.
Viral infection
Primary neonatal cardiomyocytes, 0.5 × 106 cells, were seeded in a 24-well plate at the time of isolation. After two days of culture, the cells were infected with the WT MCMV and the mutant MCMV at MOI = 5 for 24 h in the incomplete medium. After 24 h of incubation, the culture medium and cells were collected separately. Cell lysates were prepared by lysis of the cell pellet in the RIPA lysis buffer containing protease and phosphatase buffer. The culture medium was used for measuring Lactate Dehydrogenase (LDH) release and cytokine levels.
Protein isolation and Western blotting
We used a standard method for Western blotting [59]. The primary antibodies used were pRIPK3 (Cat # 91702), RIPK3 (Cat # ab56164), ZBP1 (Cat # NBP1-76854), IE1 (anti-m123/IE1- clone IE1.01, Cat # R-MCMV-12), E1 (anti- M112-113/E1- clone- chroma-103, Cat # HR-MCMV-07), gB (anti- M55/gB- clone-M55.01, Cat # HR-MCMV-05), and β-actin (1:5000, ab56164). The secondary antibodies used were anti-rabbit IgG-HRP (7074 S) and anti-antibody-mouse IgG-HRP (7076). Blots were developed using Clarity™ Western ECL Substrate (Bio-Rad Laboratories, 1705061) and Chemidoc (Bio-Rad Laboratories) instrument, and band intensity was analyzed by ChemiDoc software (Bio-Rad Laboratories).
Immunocytochemistry
We used vimentin (cat # ab92547) and followed our previously described immunocytochemistry protocol [59].
Cell viability measurement by ATP assay
The luminescence levels of Adeno-Tri-Phosphate (ATP) was measured in primary cardiomyocytes and cardiac fibroblasts using CellTiter-Glo Luminescence Cell viability Assay kit (Promega, Cat # G7571) following our previously described protocol [59].
Cell death measurement by LDH assay
Absorbance-based LDH assay was used following our previously described protocol [59].
Treatment strategies for induction of necroptosis and inhibition
To induce necroptosis, we treated cells with TS: TNFα (T, 30 ng/ml) + Smac mimetic (S, 10 µM), and TSZ: TNFα (T, 30 ng/ml) + Smac mimetic (S, 5 µM) + Z-VAD-FMK (Z, 10 mM). To inhibit necroptosis, we pretreated cells one hour before necroptosis induction with RIPK3 inhibitor GSK872 (5 µM) and RIPK1 inhibitor Nec1 (10 µM).
Caspase-3 activity assay
We used Caspase-Glo 3/7 Assay Promega kit and followed the kit protocol for measuring caspase-3 activity (cat #G8091).
Caspase-8 activity assay
We used Caspase-Glo 8 Assay Promega kit and followed the kit protocol for measuring caspase-8 activity (cat # 8201).
Enzyme-linked immuno-sorbent assay (ELISA)
We used mouse IL-1β ELISA kit (Cat # ab100705) and performws ELISA on a 100 µl of cell culture supernatant following the kit protocol. To determine the concentration of IL-1β, we measured absorbance at 450 nm using a spectrophotometer.
MitoSOX staining
We used MitoSOX Red from Invitrogen (Cat # M36008) and followed the kit protocol to measure MitoSOX levels in the treated cells. Hoechst 33342 stain was used to counterstain the nucleus.
Cell ROS staining
We used CellROX Green from Invitrogen (Cat # C10444) and followed the kit protocol to measure cellular ROS levels. Hoechst 33342 stain solution was used for staining the nucleus.
Statistical analysis
All the experimental values are expressed as mean ± SEM. To compare the two groups, we used student’s t- test. For more than two groups, we used one-way analysis of variance (ANOVA) followed by Tukey’s multiple comparison test. We used Graph Pad Prism 9 software for statistical analyses. A P value <0.05 was considered statistically significant.
Data availability
All the experimental data are safely stored in the one drive and Box drive of the University of Nebraska Medical Center. Materials described in the manuscript, including all relevant raw data, will be freely available to any researcher wishing to use them for con-commercial purposes, without breaching participants confidentiality.
References
Griffiths P, Reeves M. Pathogenesis of human cytomegalovirus in the immunocompromised host. Nat Rev Microbiol. 2021;19:759–73.
Al Mana H, Yassine HM, Younes NN, Al-Mohannadi A, Al-Sadeq DW, Alhababi D, et al. The current status of cytomegalovirus (CMV) prevalence in the MENA region: a systematic review. Pathogens. 2019;8:213.
Lachmann R, Loenenbach A, Waterboer T, Brenner N, Pawlita M, Michel A, et al. Cytomegalovirus (CMV) seroprevalence in the adult population of Germany. PLoS One. 2018;13:e0200267.
Lanzieri TM, Dollard SC, Bialek SR, Grosse SD. Systematic review of the birth prevalence of congenital cytomegalovirus infection in developing countries. Int J Infect Dis. 2014;22:44–8.
Leeaphorn N, Garg N, Thamcharoen N, Khankin EV, Cardarelli F, Pavlakis M. Cytomegalovirus mismatch still negatively affects patient and graft survival in the era of routine prophylactic and preemptive therapy: a paired kidney analysis. Am J Transpl. 2019;19:573–84.
Kaminski H, Fishman JA. The cell biology of cytomegalovirus: implications for transplantation. Am J Transpl. 2016;16:2254–69.
Sinzger C, Digel M, Jahn G. Cytomegalovirus cell tropism. Curr Top Microbiol Immunol. 2008;325:63–83.
Grefte A, Harmsen MC, van der Giessen M, Knollema S, van Son WJ. The TH. Presence of human cytomegalovirus (HCMV) immediate early mRNA but not ppUL83 (lower matrix protein pp65) mRNA in polymorphonuclear and mononuclear leukocytes during active HCMV infection. J Gen Virol. 1994;75:1989–98.
Stevenson EV, Collins-McMillen D, Kim JH, Cieply SJ, Bentz GL, Yurochko AD. HCMV reprogramming of infected monocyte survival and differentiation: a Goldilocks phenomenon. Viruses 2014;6:782–807.
Xiaofei E, Meraner P, Lu P, Perreira JM, Aker AM, McDougall WM, et al. OR14I1 is a receptor for the human cytomegalovirus pentameric complex and defines viral epithelial cell tropism. Proc Natl Acad Sci USA. 2019;116:7043–52.
Wang H, Peng G, Bai J, He B, Huang K, Hu X. et al.Cytomegalovirus infection and relative risk of cardiovascular disease (ischemic heart disease, stroke, and cardiovascular death): a meta-analysis of prospective studies up to 2016.J Am Heart Assoc. 2017;6:e005025.
Das BB, Prusty BK, Niu J, Sue PK. Cytomegalovirus infection and allograft rejection among pediatric heart transplant recipients in the era of valganciclovir prophylaxis. Pediatr Transpl. 2020;24:e13750.
Immohr MB, Akhyari P, Bottger C, Mehdiani A, Dalyanoglu H, Westenfeld R, et al. Cytomegalovirus mismatch after heart transplantation: Impact of antiviral prophylaxis and intravenous hyperimmune globulin. Immun Inflamm Dis. 2021;9:1554–62.
Garcia-Torre A, Bueno-Garcia E, Lopez-Martinez R, Rioseras B, Diaz-Molina B, Lambert JL, et al. CMV infection is directly related to the inflammatory status in chronic heart failure patients. Front Immunol. 2021;12:687582.
Nian M, Lee P, Khaper N, Liu P. Inflammatory cytokines and postmyocardial infarction remodeling. Circ Res. 2004;94:1543–53.
Bonavita CM, White TM, Francis J, Cardin RD. Heart dysfunction following long-term murine cytomegalovirus infection: fibrosis, hypertrophy, and tachycardia. Viral Immunol. 2020;33:237–45.
Kyto V, Vuorinen T, Saukko P, Lautenschlager I, Lignitz E, Saraste A, et al. Cytomegalovirus infection of the heart is common in patients with fatal myocarditis. Clin Infect Dis. 2005;40:683–8.
Ritter JT, Tang-Feldman YJ, Lochhead GR, Estrada M, Lochhead S, Yu C, et al. In vivo characterization of cytokine profiles and viral load during murine cytomegalovirus-induced acute myocarditis. Cardiovasc Pathol. 2010;19:83–93.
Mishra PK, Adameova A, Hill JA, Baines CP, Kang PM, Downey JM, et al. Guidelines for evaluating myocardial cell death. Am J Physiol Heart Circ Physiol. 2019;317:H891–H922.
Chaudhry MZ, Casalegno-Garduno R, Sitnik KM, Kasmapour B, Pulm A-K, Brizic I, et al. Cytomegalovirus inhibition of extrinsic apoptosis determines fitness and resistance to cytotoxic CD8 T cells. Proc Natl Acad Sci. 2020;117:12961–8.
Terhune S, Torigoi E, Moorman N, Silva M, Qian Z, Shenk T, et al. Human Cytomegalovirus UL38 Protein Blocks Apoptosis. J Virol. 2007;81:3109–23.
Fiddian-Green RG, Silen W. Mechanisms of disposal of acid and alkali in rabbit duodenum. Am J Physiol. 1975;229:1641–8.
Hengartner MO. The biochemistry of apoptosis. Nature .2000;407:770–6.
Fulda S, Debatin KM. Extrinsic versus intrinsic apoptosis pathways in anticancer chemotherapy. Oncogene .2006;25:4798–811.
Taylor RC, Cullen SP, Martin SJ. Apoptosis: controlled demolition at the cellular level. Nat Rev Mol Cell Biol. 2008;9:231–41.
Galluzzi L, Kroemer G. Necroptosis: a specialized pathway of programmed necrosis. Cell 2008;135:1161–3.
Kaiser WJ, Sridharan H, Huang C, Mandal P, Upton JW, Gough PJ, et al. Toll-like receptor 3-mediated necrosis via TRIF, RIP3, and MLKL. J Biol Chem. 2013;288:31268–79.
Zhang DW, Shao J, Lin J, Zhang N, Lu BJ, Lin SC, et al. RIP3, an energy metabolism regulator that switches TNF-induced cell death from apoptosis to necrosis. Science . 2009;325:332–6.
Upton JW, Kaiser WJ, Mocarski ES. Virus inhibition of RIP3-dependent necrosis. Cell Host Microbe. 2010;7:302–13.
Cho YS, Challa S, Moquin D, Genga R, Ray TD, Guildford M, et al. Phosphorylation-driven assembly of the RIP1-RIP3 complex regulates programmed necrosis and virus-induced inflammation. Cell 2009;137:1112–23.
Petrie EJ, Czabotar PE, Murphy JM. The structural basis of necroptotic cell death signaling. Trends Biochem Sci. 2019;44:53–63.
Chen X, Li W, Ren J, Huang D, He WT, Song Y, et al. Translocation of mixed lineage kinase domain-like protein to plasma membrane leads to necrotic cell death. Cell Res. 2014;24:105–21.
Upton JW, Kaiser WJ, Mocarski ES. DAI/ZBP1/DLM-1 complexes with RIP3 to mediate virus-induced programmed necrosis that is targeted by murine cytomegalovirus vIRA. Cell Host Microbe. 2012;11:290–7.
Nailwal H, Chan FK. Necroptosis in anti-viral inflammation. Cell Death Differ. 2019;26:4–13.
McCormick AL, Skaletskaya A, Barry PA, Mocarski ES, Goldmacher VS. Differential function and expression of the viral inhibitor of caspase 8-induced apoptosis (vICA) and the viral mitochondria-localized inhibitor of apoptosis (vMIA) cell death suppressors conserved in primate and rodent cytomegaloviruses. Virology .2003;316:221–33.
Feng Y, Daley-Bauer LP, Roback L, Guo H, Koehler HS, Potempa M, et al. Caspase-8 restricts antiviral CD8 T cell hyperaccumulation. Proc Natl Acad Sci. 2019;116:15170–7.
Fletcher-Etherington A, Nobre L, Nightingale K, Antrobus R, Nichols J, Davison AJ, et al. Human cytomegalovirus protein pUL36: A dual cell death pathway inhibitor. Proc Natl Acad Sci. 2020;117:18771–9.
Kim S, Lu HC, Steelman AJ, Li J. Myeloid caspase-8 restricts RIPK3-dependent proinflammatory IL-1beta production and CD4 T cell activation in autoimmune demyelination. Proc Natl Acad Sci USA. 2022;119:e2117636119.
Moriwaki K, Bertin J, Gough PJ, Chan FK. A RIPK3-caspase 8 complex mediates atypical pro-IL-1beta processing. J Immunol. 2015;194:1938–44.
Handke W, Luig C, Popovic B, Krmpotic A, Jonjic S, Brune W. Viral inhibition of BAK promotes murine cytomegalovirus dissemination to salivary glands. J Virol. 2013;87:3592–6.
Jurak I, Schumacher U, Simic H, Voigt S, Brune W. Murine cytomegalovirus m38.5 protein inhibits bax-mediated cell death. J Virol. 2008;82:4812–22.
Cam M, Handke W, Picard-Maureau M, Brune W. Cytomegaloviruses inhibit Bak- and Bax-mediated apoptosis with two separate viral proteins. Cell Death Differ. 2010;17:655–65.
Crosby LN, McCormick AL, Mocarski ES. Gene products of the embedded m41/m41.1 locus of murine cytomegalovirus differentially influence replication and pathogenesis. Virology .2013;436:274–83.
Claycomb WC, Lanson NA Jr, Stallworth BS, Egeland DB, Delcarpio JB, Bahinski A, et al. HL-1 cells: a cardiac muscle cell line that contracts and retains phenotypic characteristics of the adult cardiomyocyte. Proc Natl Acad Sci USA. 1998;95:2979–84.
Zhu K, Liang W, Ma Z, Xu D, Cao S, Lu X, et al. Necroptosis promotes cell-autonomous activation of proinflammatory cytokine gene expression. Cell Death Dis. 2018;9:500.
Deragon MA, McCaig WD, Patel PS, Haluska RJ, Hodges AL, Sosunov SA, et al. Mitochondrial ROS prime the hyperglycemic shift from apoptosis to necroptosis. Cell Death Disco. 2020;6:132.
Chan SHH, Chan JYH. Mitochondria and reactive oxygen species contribute to neurogenic hypertension. Physiol (Bethesda). 2017;32:308–21.
Piccoli MT, Gupta SK, Viereck J, Foinquinos A, Samolovac S, Kramer FL, et al. Inhibition of the cardiac fibroblast-enriched lncRNA Meg3 prevents cardiac fibrosis and diastolic dysfunction. Circ Res. 2017;121:575–83.
Galvan V, Roizman B. Herpes simplex virus 1 induces and blocks apoptosis at multiple steps during infection and protects cells from exogenous inducers in a cell-type-dependent manner. Proc Natl Acad Sci USA. 1998;95:3931–6.
Mandal P, Nagrani LN, Hernandez L, McCormick AL, Dillon CP, Koehler HS. et al. Multiple autonomous cell death suppression strategies ensure cytomegalovirus fitness. Viruses. 2021;13:1707.
Xenaki E, Hassoulas J, Apostolakis S, Sourvinos G, Spandidos DA. Detection of cytomegalovirus in atherosclerotic plaques and nonatherosclerotic arteries. Angiology .2009;60:504–8.
Cristescu CV, Alain S, Ruta SM. The role of CMV infection in primary lesions, development and clinical expression of atherosclerosis. J Clin Med. 2022;11:13.
Nikitskaya E, Lebedeva A, Ivanova O, Maryukhnich E, Shpektor A, Grivel JC. et al. Cytomegalovirus-productive infection is associated with acute coronary syndrome. J Am Heart Assoc. 2016;5:e003759.
Haider AW, Wilson PW, Larson MG, Evans JC, Michelson EL, Wolf PA, et al. The association of seropositivity to Helicobacter pylori, Chlamydia pneumoniae, and cytomegalovirus with risk of cardiovascular disease: a prospective study. J Am Coll Cardiol. 2002;40:1408–13.
Muendlein HI, Connolly WM, Magri Z, Smirnova I, Ilyukha V, Gautam A, et al. ZBP1 promotes LPS-induced cell death and IL-1beta release via RHIM-mediated interactions with RIPK1. Nat Commun. 2021;12:86.
Hubbard NW, Ames JM, Maurano M, Chu LH, Somfleth KY, Gokhale NS, et al. ADAR1 mutation causes ZBP1-dependent immunopathology. Nature .2022;607:769–75.
Daley-Bauer LP, Roback L, Crosby LN, McCormick AL, Feng Y, Kaiser WJ, et al. Mouse cytomegalovirus M36 and M45 death suppressors cooperate to prevent inflammation resulting from antiviral programmed cell death pathways. Proc Natl Acad Sci USA. 2017;114:E2786–E95.
Gopal S, Perez E Jr, Xia AY, Knowlton JJ, Cerqueira F, Dermody TS, et al. Murine cytomegalovirus M72 promotes acute virus replication in vivo and is a substrate of the TRiC/CCT complex. Virology .2018;522:92–105.
Yadav SK, Kambis TN, Kar S, Park SY, Mishra PK. MMP9 mediates acute hyperglycemia-induced human cardiac stem cell death by upregulating apoptosis and pyroptosis in vitro. Cell Death Dis. 2020;11:186.
Acknowledgements
We would like to thank Dr. Mocarski ES for proving mutant strains of CMV. We thank Mr. Shahshahan HR for animal-related work.
Funding
This work was supported in part by the National Institutes of Health (NIH) Grant HL-113281, 1U54GM115458, P20GM104320, and R56HL156806 and the University of Nebraska Collaboration Initiative Grant to PKM. The work at the University of Mississippi Medical Center was supported by NASA award # 80 NSSC19K1603 to RT.
Author information
Authors and Affiliations
Contributions
SKY has performed most experiments and data analysis. FIG prepared splice variants and predicted structural images of ZBP1 interacting proteins. MHH contributed to standardization of dose and time course experiment of MCMV. SKY drafted the manuscript and RT and JWU contributed to manuscript drafts. PKM has supervised the study and wrote the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Yadav, S.K., Gawargi, F.I., Hasan, M.H. et al. Differential effects of CMV infection on the viability of cardiac cells. Cell Death Discov. 9, 111 (2023). https://doi.org/10.1038/s41420-023-01408-y
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41420-023-01408-y
- Springer Nature Limited