
Abstract
Background
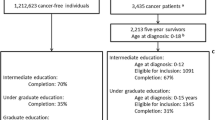
Survivors of childhood cancer may face difficulties at school. We investigated whether childhood cancer affects attainment of upper secondary education, in a register-based cohort study from Denmark, Finland, and Sweden, where we limit bias from selection and participation.
Methods
From the national cancer registers, we identified all long-term survivors of childhood cancer diagnosed aged 0–14 years in 1971–2005 (n = 7629), compared them to matched population comparisons (n = 35,411) and siblings (n = 6114), using odds ratios (OR) and 95% confidence intervals (CI).
Results
Overall, 6127 survivors (80%) had attained upper secondary education by age 25, compared to 84% among comparison groups. Elevated OR for not attaining this level were mainly confined to survivors of central nervous system (CNS) tumours (ORSurv_PopComp2.05, 95%CI: 1.83–2.29). Other risk groups were survivors who had spent more time in hospital around cancer diagnosis and those who had hospital contacts in early adulthood, particularly psychiatric. Survivors of all cancer types were less likely to have attained upper secondary education without delay.
Conclusions
Although survivors of childhood cancer experienced delays in their education, many had caught up by age 25. Except for survivors of CNS tumours, survivors attained upper secondary education to almost the same extent as their peers.
Similar content being viewed by others

Introduction
Advances in the diagnosis and treatment of childhood cancer have led to remarkable improvements in survival and a steadily increasing population of survivors [1, 2]. Attention has therefore been paid to better understand the somatic late effects and adverse socioeconomic consequences of a childhood cancer diagnosis [3, 4]. Educational attainment, such as completion of upper secondary education, are important milestones for future work-life opportunities. Survivors of childhood cancer may experience educational difficulties due to absence from school while undergoing treatment, the disease itself, or the toxicity of cancer treatment, which can affect cognition [5]. In previous studies, survivors of central nervous system (CNS) tumours and those treated with CNS-directed therapy were shown consistently to have lower educational attainment than their peers [4,5,6,7]. The picture is less conclusive for survivors of other cancer types, previous studies having reported that survivors of this heterogeneous group of malignancies have worse, equal, or better educational outcomes than comparison groups [4,5,6,7]. A recent review of the literature, including guidelines for surveillance, concluded that childhood and young adult cancer survivors are at increased risk for lower educational achievement overall, but the evidence level was graded as very low [8]. Most previous studies had methodological limitations such as use of self-reported outcomes from questionnaires, risk of selection bias due to non-participation, limited follow-up time, and assessment of educational attainment at only one time. The existing literature does not, therefore, clearly show whether survivors experience only delays in educational attainment [9], or whether they continue to lag behind their peers in adulthood.
In many previous studies, subgroup analyses were lacking owing to the rarity of childhood cancer. Diagnosis-specific analyses are, however, clinically relevant and important for potential interventions. The risk factors for lower educational attainment include not only the diagnostic group [4,5,6,7] but also the age at diagnosis [4, 10]. The severity of disease and somatic and psychiatric late effects [3, 11] have rarely been considered in previous work on educational attainment, although these factors can substantially affect both school attendance and the ability to benefit from teaching. Parental education is another factor that is likely to influence educational attainment also among childhood cancer survivors [9, 12, 13], and may confound the association. Moreover, highly educated parents may be in a better position to support their children during and after cancer treatment and thus compensate for the negative effects of childhood cancer on education, however, such effect modification has rarely been studied [10, 12, 14].
In this comprehensive population-based register study, we sought to examine the educational attainment of childhood cancer survivors in Denmark, Finland, and Sweden, in comparison with that of matched individuals from the general population and of survivors’ siblings, focusing on attainment of upper secondary education in young adulthood. We also aimed to identify vulnerable groups of survivors and to assess educational delay.
Material and methods
Design, study population, and data sources
This study is part of the SALiCCS (Socioeconomic Consequences in Adult Life after Childhood Cancer in Scandinavia) research programme, details of which have been published elsewhere [15]. We used a register-based matched cohort design and linked individual information for our study population across various nationwide registries with the unique personal identification number assigned to the residents of all Nordic countries. Denmark, Finland, and Sweden have nationwide registers covering health and social characteristics of the population. The three countries also have similar health care systems and to a large extent common treatment protocols within paediatric oncology, which makes it reasonable to combine data from these countries [15, 16].
We focused on long-term survivors of childhood cancer. All survivors of a first childhood cancer (including non-malignant CNS tumours) in Denmark, Finland, and Sweden born in 1960–1990 (1960–1989 in Finland), diagnosed at ages 0–14 during 1971–2005 (1971–2003 in Finland) who were alive and had not emigrated by the end of the year they turned 25 were eligible (Supplementary Fig. 1). We identified the survivors from the national cancer registers [17] and classified the diagnoses into groups according to the International Classification of Childhood Cancer [18]; we grouped acute lymphoid leukaemia (ALL, defined as group Ia), other leukaemias (Ib-Ie), lymphomas (II), CNS tumours (III), and non-CNS solid tumours (IV-XI) separately.
For each survivor, five individuals, referred to as population comparisons, were randomly sampled from the national population registries and individually matched by sex, year of birth and country of residence (region in Sweden). All biological and adopted siblings with an age difference of ≤5 years from the corresponding survivor were identified as a second comparison group to account for unmeasured genetic and familial background. Individuals in both comparison groups had to be cancer-free up to the age of 20 years (Supplementary Fig. 1).
As a cancer predisposition syndrome may confound associations with educational outcomes, we excluded individuals with Down syndrome, neurofibromatosis, or tuberous sclerosis. For survivors and population comparisons, the reference date was defined as the date of cancer diagnosis of the survivor. For siblings, the reference date was defined as the date on which the sibling was of the same age as the corresponding survivor at cancer diagnosis.
Outcome assessment
Annual individual information on highest attained educational level was retrieved from national registers administrated by statistical institutes [19,20,21] for the period 1985–2015 (1985, 1987–2014 in Finland). Educational level was categorised according to the International Standard Classification of Education (ISCED) as no education registered, lower secondary education or less (ISCED ≤ 2), upper secondary and non-tertiary post-secondary education (ISCED 3–4) and tertiary education (ISCED ≥ 5) [22]. In Finland, education levels below ISCED 3 are not registered; as virtually all Finnish children attend comprehensive school, missing information from Finland was considered to be lower secondary education or less.
We defined our main outcome as attainment of upper secondary education (ISCED 3) by age 25. We also assessed attainment of upper secondary education without delay, defined as having attained ISCED 3 or higher by age 19 in Finland and Sweden, and by age 20 in Denmark. Although the education systems in the three countries are overall similar, the difference in age reflects some diversity and different traditions [23].
Covariates
Age at the reference date was categorised similarly to Nordic school ages as preschool and younger (ages 0–6), lower stage of comprehensive school (ages 7–11), and higher stage of comprehensive school (ages 12–14). The highest attained parental educational level was considered that obtained by biological parents the year before the reference year and grouped as attainment of upper secondary education (ISCED 3) or not.
We collected information from the national patient registers on in- and outpatient hospital care. Time spent in hospital during and after diagnosis (defined as inpatient care within 5 years after the reference date) was used as an indicator of length of treatment and occurrence of complications. The variable was dichotomized (short, long) by the median value in each group of cancer diagnoses, country, and calendar period. We also assessed whether the individual had any hospital contacts for specified somatic disorders (Supplementary Table 1) at ages 20–24 years, categorised as none, cancer-related (i.e., main diagnosis is cancer), and other diagnoses. These categories have been used in previous studies of childhood cancer survivors as conditions related to somatic late effects [3]. Additionally, we assessed hospital contacts for psychiatric diagnoses at ages 20–24 (none, any).
Statistical analysis
We fitted logistic regression models to estimate odds ratios (ORs) and 95% confidence intervals (CIs) for the risk of not having attained upper secondary education by age 25. For the comparison of survivors with population comparisons, we used unconditional logistic regression models, crude and adjusted for the matching factors (country, sex, age (0–6, 7–11, 12–15) and reference year (10-year intervals)). Survivors and siblings were compared in conditional logistic regression models, crude and adjusted for sex and reference year, to enable comparisons within each sibling set. All the main analyses were also conducted separately for ALL, other leukaemias, lymphomas, CNS tumours, and non-CNS solid tumours. Stratified analyses were conducted by sex, age (0–6, 7–11, 12–15), reference period (1971–1989, 1990–2005), country, time spent in hospital (short, long), and somatic and psychiatric hospital contacts, performed separately for all cancers combined, ALL, CNS, and non-CNS solid tumours. As an additional analysis, we simultaneously stratified by age and reference year among children with ALL.
In comparing the educational attainment of survivors and population comparisons, we assessed the role of parental education by adjusting for it as a potential confounder and conducted stratified analyses. We also assessed potential interaction on the additive scale between cancer survivorship and parental education on the effect of educational attainment, by calculating the relative excess risk due to the interaction (RERI) with 95%CI [24]. RERI is an estimate of the joint effect of survivorship and having parents with a low level of education (hereinafter “low education”), i.e., the effect that is additional to the sum of the two individual factors on educational attainment.
Among individuals who had attained upper secondary education by age 25, we compared the probability of attainment without delay in logistic regression analysis, modelled in the same way as for the main analyses.
Analyses were conducted with SAS 9.4 and Stata 14. The level of statistical significance was set to <0.05.
Results
Our study population comprised 7629 survivors (4085 males and 3544 females), 35,411 population comparisons and 6114 siblings (Table 1 and Supplementary Fig. 1). Of the survivors, 47.5% were diagnosed with cancer before school age (0–6 years, Table 1).
In total, 6127 (80.3%) survivors, 29,880 (84.4%) population comparisons, and 5135 (84.0%) siblings had attained upper secondary education by age 25 (Table 2, Fig. 1). The overall adjusted ORs of the risk of not having attained upper secondary education by age 25, comparing survivors with population comparisons and siblings were 1.32 (95% CI: 1.23–1.40) and 1.57 (95% CI: 1.40–1.77), respectively. The associations differed substantially by diagnostic group and were strongest among survivors of CNS tumours (ORSurv vs PopComp 2.05 (95% CI: 1.83–2.29); ORSurv vs Sib 2.72 (95% CI: 2.19–3.39)) and less pronounced among survivors of ALL (ORSurv vs PopComp 1.15 (95% CI: 1.00–1.33); ORSurv vs Sib 1.27 (95% CI: 0.98–1.65)), while no associations were apparent for survivors of other leukaemias, lymphomas, or non-CNS solid tumours when compared with population comparisons (Table 2). In general, the point estimates were somewhat more elevated when survivors were compared with their siblings but also less precise. As the estimates from the crude and adjusted analyses were similar, only adjusted estimates are shown.

Proportion of survivors, population comparisons and siblings having attained upper secondary education by the respective ages 19–25, stratified by cancer type.
The OR of not having attained upper secondary education by age 25, comparing survivors with population comparisons, differed by sex, age, reference year, time spent in hospital, and hospital contacts (Table 3 and Supplementary Table 2). After stratification by age at diagnosis, the association for survivors of CNS tumours was strongest among those diagnosed before school age, while for survivors of ALL the most pronounced association was seen in the age group 12–14 (Table 3). The lower educational attainment of survivors of ALL than of population comparisons was confined to survivors of cancers diagnosed in 1971–1989, except for ALL diagnosed after age 12: in this age group, lower education attainment among survivors was observed in both periods (Supplementary Table 3). Stronger associations were found for survivors who had spent more time in hospital during and after diagnosis (ORSurv vs PopComp 1.61, 95% CI: 1.48–1.76), or had hospital contacts in early adulthood; this pattern was consistent across diagnostic groups and was particularly pronounced among survivors who had psychiatric hospital contacts in young adulthood (ORSurv vs PopComp 4.00, 95% CI: 3.26–4.90, Table 3). Survivors of leukaemia (Table 3) and non-CNS solid tumours (Supplementary Table 2) who had spent less time in hospital during and after diagnosis or had no hospital contacts for specified conditions in early adulthood had similar odds of attaining upper secondary education at age 25 as population comparisons.
Both survivors and population comparisons with parents who had achieved high education were more likely to attain upper secondary education; however, the difference between survivors and population comparisons was more pronounced for individuals with parents who had a higher education level than among those with parents who had low education (Table 3). Among individuals whose parents had low education, survivors of leukaemia and non-CNS tumours completed upper secondary education to at least the same extent as population comparisons (Table 4). There was no statistically significant additive interaction. Adjustment for parental education as a potential confounder did not appreciably change the effect estimates from those of the main analysis (Supplementary Table 4).
Among individuals who had attained upper secondary education by age 25, survivors were less likely to have completed this without delay; completion of upper secondary education without delay was achieved by 4361 (71.3%) survivors, 18,801 (77.2%) population comparisons and 3326 (77.7%) siblings. The overall adjusted ORs comparing the probability of completing upper secondary education without delay were 0.75 (95% CI: 0.70–0.80) and 0.72 (95% CI: 0.64–0.81) when survivors were compared to population comparisons and siblings, respectively. This pattern was seen in all diagnostic groups (Table 2 and Fig. 1) and in all three countries (Supplementary Table 5 and Supplementary Fig. 2).
Table 5 shows the distribution of educational level among individuals for whom follow-up information was available until age 30. A smaller proportion of the survivors had attained tertiary education by age 30, but the difference was smaller when restricting to individuals who had attained upper secondary education by age 25. For survivors of non-CNS solid tumours, similar proportions of tertiary education were observed compared with population comparisons and siblings (Supplementary Table 6).
Discussion
In this large register-based cohort study nested in the entire populations of three Nordic countries, we observed that, overall, a smaller proportion of childhood cancer survivors had attained upper secondary education by age 25 than population comparisons and siblings. The differences were, however, largely confined to survivors of CNS tumours, while smaller differences were seen for survivors of ALL diagnosed in 1971–1989 or at ages 12–14 years. Survivors of all cancer types experienced delays in education, but survivors of leukaemias other than ALL, lymphomas, and non-CNS solid tumours had caught up with their peers with regard to upper secondary education by age 25. Survivors who had spent more time in hospital during and after their cancer diagnosis or had hospital contacts in early adulthood were at particular risk of not attaining upper secondary education by age 25, especially survivors who had psychiatric hospital contacts. Parental education had a considerable impact on educational attainment in general, however, stratification by parental education showed the largest differences between survivors and population comparisons among those with parents with high education.
The pronounced educational disadvantage of survivors of CNS tumours is well recognised in the literature [4,5,6,7], seen even at younger ages [12, 13]. Our study suggests that this group of survivors does not catch up over time as do survivors of other types of cancer, in accordance with previous findings in Switzerland [9]. We found that survivors of CNS tumours diagnosed before school age were particularly vulnerable, with a somewhat stronger association among females and individuals diagnosed in the early calendar period, similar to previous studies [12, 13, 25]. However, survivors of CNS tumours were less likely to attain upper secondary education by age 25 than their peers in all the strata investigated, highlighting the need to support this group.
Survivors of ALL diagnosed in 1971–1989 also had a lower level of education than their peers at the age of 25. This is probably due to the use of cranial radiotherapy during that period [26]; previous studies also found lower educational attainment among survivors of leukaemia who were treated with irradiation [10, 27,28,29]. The difference between calendar periods was seen mainly among younger children, who are more sensitive to irradiation [30]. We also found that survivors of ALL diagnosed at ages 12–14 were at risk of poorer educational outcomes in both calendar periods. This finding is somewhat unexpected, although some other studies suggested that also older children with leukaemia are at risk of lower educational attainment [9, 10].
We found that survivors who had spent more time in hospital during and after diagnosis and survivors with more hospital contacts in early adulthood, i.e., after the original cancer treatment, were at higher risk of not attaining upper secondary education by age 25. This is in line with previous research of more specific health problems. For example, in the British Childhood Cancer Survivor Study, epilepsy influenced education negatively [27]. A German study of survivors of adolescent cancer suggested that visual or hearing late effects as well as neuropsychological late effects were risk factors for poorer educational attainment at different levels, while increasing length of treatment was borderline significant [31]. This result may also reflect that survivors experiencing a relapse or a second primary malignancy, who therefore have more contacts with hospitals, is a vulnerable group with regard to educational achievements. However, such specific conclusions require further investigation. In our study, the risk of poorer educational outcomes was particularly pronounced among survivors with psychiatric hospital contacts; this finding is important with regard to potential targeted interventions, although this is a small group of survivors as seen in the current study as well as in previous research from our group [11].
It has been shown previously that survivors with parents who had low education had worse educational outcomes than survivors with parents with high education [9, 12, 13], which reflects the pattern in the general population and is also seen in our study population. In addition to existing literature, we observed that the difference between survivors and comparisons was largest among children of parents with high education. This finding runs contrary to sociological theories of “compensatory advantage”, which argue that highly educated parents have more resources to counteract negative childhood circumstances [14], and suggests that childhood cancer is more disruptive for the educational trajectories of children of highly educated parents. Also, as it is less common that children with higher educated parents do not complete upper secondary education, the relative and absolute differences in this group become more pronounced. Indeed, survivors of ALL and non-CNS solid tumours whose parents had low education completed upper secondary education to the same extent or even more frequently than the corresponding population comparisons, which suggests that these groups of survivors gained from provided support. For survivors of CNS tumours, however, the combination of experiencing a cancer diagnosis as a child and having parents with lower education was associated with a particularly high risk of not completing upper secondary education before age 25.
Survivors of non-CNS solid tumours who had attained an upper secondary education attained tertiary education to a similar extent as their peers. A previous meta-analysis showed that survivors without CNS involvement had no disadvantage in achieving tertiary education but highlighted the risk of bias from non-participation [7]. This bias was not a concern in the present study, which strengthens the conclusion that, for this group, childhood cancer can disrupt education primarily in the early stages but has no further impact on later educational transitions. However, for other groups of survivors there seem to be a difference in achievement of tertiary education.
Our study is unique in that it combined high-quality register data from three Nordic countries and included comparisons with both the general population and siblings. Use of siblings as a second reference group controlled for confounding from shared familial and social backgrounds and strengthens the validity of our findings, although these analyses had less statistical power, as only data of siblings discordant for the outcome contributed to the estimates. The large population allowed subgroup analyses, which is important for identifying survivors who would benefit most from targeted support. However, although the whole population of survivors in Denmark, Finland, and Sweden were included, statistical power limited analyses of, for example, more defined cancer types (e.g., specific types of non-CNS solid tumours). As information on educational attainment was obtained from national population-based registers, there was no risk of bias due to self-reporting, non-participation, or selection. Further, the longitudinal information was obtained in the same way for the survivor and comparison groups.
The register-based design and the three-country wide inclusion have many advantages but also some limitations. We had no information on the reasons for delayed graduation, which are not necessarily related to educational problems. We also lacked information on treatment, especially cranial radiation therapy, an established risk factor for poorer educational achievement [4]. Inclusion in future studies of more clinical information would improve understanding of the underlying mechanisms and help to identify vulnerable survivors. Our study population came from three Nordic countries which have remarkably comparable, although not identical, health-, social- and educational systems. The matched design took differences between countries into consideration. Country specific analyses showed similar results, although effect estimates differed somewhat in magnitude. This could reflect true differences across countries but may also be a result of random variation. It is important to acknowledge differences between countries when interpreting the findings, but also the overall Nordic context. Support in school as well as the overall social- and educational systems will impact survivors’ opportunities after a cancer diagnosis, and it is therefore challenging to directly generalise our findings to other countries. We included survivors diagnosed over a long period of time during which treatment regimens have changed, and our results may not be applicable to children undergoing cancer treatment at present. Our findings highlight the importance of continued follow-up of late effects and socioeconomic consequences also among more recently treated survivors.
In this three-country wide register-based cohort study, we demonstrate that, although survivors of childhood cancer are more likely than their peers to experience delays in upper secondary education, many had caught up by the age of 25. Except for survivors of CNS tumours, survivors attained upper secondary education to almost the same extent as their peers. Parental education played an important role also in survivors’ educational attainment and modified the associations. In addition to the vulnerable group of survivors of CNS tumours, we identified survivors who had spent more time in hospital during and after diagnosis and survivors with hospital contacts, particularly for psychiatric diseases, in early adulthood as risk groups for educational difficulties. These findings add to the existing literature and recently published guidelines for surveillance [8] and enhance a possibility of identifying survivors who need additional educational support, both close to the diagnosis and at later follow-up visits.
Data availability
The data that support the information of this manuscript were accessed remotely on a secure platform at Statistics Denmark. Pseudonymized individual-level data were obtained from national registry holders after ethical approval (where applicable) and secrecy assessment. According to Danish, Finnish and Swedish laws and regulations, individual-level sensitive data can only be made available for researchers who fulfil legal requirements for access to personal sensitive data. Please contact Jeanette Falck Winther (jeanette@cancer.dk), the Principal Investigator of the SALiCCS research programme, for further questions about data access.
References
Gatta G, Botta L, Rossi S, Aareleid T, Bielska-Lasota M, Clavel J, et al. Childhood cancer survival in Europe 1999–2007: results of EUROCARE-5—a population-based study. Lancet Oncol. 2014;15:35–47.
Pritchard-Jones K, Pieters R, Reaman GH, Hjorth L, Downie P, Calaminus G, et al. Sustaining innovation and improvement in the treatment of childhood cancer: lessons from high-income countries. Lancet Oncol. 2013;14:e95–103.
de Fine Licht S, Rugbjerg K, Gudmundsdottir T, Bonnesen TG, Asdahl PH, Holmqvist AS, et al. Long-term inpatient disease burden in the Adult Life after Childhood Cancer in Scandinavia (ALiCCS) study: a cohort study of 21,297 childhood cancer survivors. PLoS Med. 2017;14:e1002296.
Frederiksen LE, Mader L, Feychting M, Mogensen H, Madanat-Harjuoja L, Malila N, et al. Surviving childhood cancer: a systematic review of studies on risk and determinants of adverse socioeconomic outcomes. Int J Cancer. 2019;144:1796–823.
Molcho M, D’Eath M, Alforque Thomas A, Sharp L. Educational attainment of childhood cancer survivors: a systematic review. Cancer Med. 2019;8:3182–95.
Gummersall T, Skaczkowski G, Wilson C. Childhood cancer, age at diagnosis and educational attainment: a meta-analysis. Crit Rev Oncol Hematol. 2020;145:102838.
Saatci D, Thomas A, Botting B, Sutcliffe AG. Educational attainment in childhood cancer survivors: a meta-analysis. Arch Dis Child. 2020;105:339–46.
Devine KA, Christen S, Mulder RL, Brown MC, Ingerski LM, Mader L, et al. Recommendations for the surveillance of education and employment outcomes in survivors of childhood, adolescent, and young adult cancer: a report from the International Late Effects of Childhood Cancer Guideline Harmonization Group. Cancer. 2022;128:2405–19.
Kuehni CE, Strippoli MP, Rueegg CS, Rebholz CE, Bergstraesser E, Grotzer M, et al. Educational achievement in Swiss childhood cancer survivors compared with the general population. Cancer. 2012;118:1439–49.
Holmqvist AS, Wiebe T, Hjorth L, Lindgren A, Ora I, Moell C. Young age at diagnosis is a risk factor for negative late socio-economic effects after acute lymphoblastic leukemia in childhood. Pediatr Blood Cancer. 2010;55:698–707.
Frederiksen LE, Erdmann F, Mader L, Mogensen H, Pedersen C, Kenborg L, et al. Psychiatric disorders in childhood cancer survivors in Denmark, Finland, and Sweden: a register-based cohort study from the SALiCCS research programme. Lancet Psychiatry. 2022;9:35–45.
Koch SV, Kejs AM, Engholm G, Johansen C, Schmiegelow K. Educational attainment among survivors of childhood cancer: a population-based cohort study in Denmark. Br J Cancer. 2004;91:923–8.
Lönnerblad M, Van’t Hooft I, Blomgren K, Berglund E. A nationwide, population-based study of school grades, delayed graduation, and qualification for school years 10-12, in children with brain tumors in Sweden. Pediatr Blood Cancer. 2020;67:e28014.
Bernardi F. Compensatory advantage as a mechanism of educational inequality: a regression discontinuity based on month of birth. Sociol Educ. 2014;87:74–88.
Erdmann F, Frederiksen L, Mogensen H, Pedersen C, Mader L, Talbäck M, et al. Cohort profile: the socioeconomic consequences in adult life after childhood cancer in scandinavia (SALiCCS) research programme. Front Oncol. 2021;11:752948.
Laugesen K, Ludvigsson JF, Schmidt M, Gissler M, Valdimarsdottir UA, Lunde A, et al. Nordic health registry-based research: a review of health care systems and key registries. Clin Epidemiol. 2021;13:533–54.
Pukkala E, Engholm G, Højsgaard Schmidt LK, Storm H, Khan S, Lambe M, et al. Nordic Cancer Registries—an overview of their procedures and data comparability. Acta Oncol. 2018;57:440–55.
Steliarova-Foucher E, Stiller C, Lacour B, Kaatsch P. International Classification of Childhood Cancer, third edition. Cancer. 2005;103:1457–67.
Ludvigsson JF, Svedberg P, Olén O, Bruze G, Neovius M. The longitudinal integrated database for health insurance and labour market studies (LISA) and its use in medical research. Eur J Epidemiol. 2019;34:423–37.
Statitics Finland. Educational structure of population 2018 (04.03.2022; date accessed). Available from: https://www.stat.fi/meta/til/vkour_en.html.
Jensen VM, Rasmussen AW. Danish education registers. Scand J Public Health. 2011;39:91–4.
Eurostat. International Standard Classification of Education (ISCED) 2020 (04.03.2022; date accessed). Available from: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=International_Standard_Classification_of_Education_(ISCED).
Jorgensen CH, Jarvinen T, Lundahl L. A Nordic transition regime? Policies for school-to-work transitions in Sweden, Denmark and Finland. Eur Educ Res J. 2019;18:278–97.
Andersson T, Alfredsson L, Källberg H, Zdravkovic S, Ahlbom A. Calculating measures of biological interaction. Eur J Epidemiol. 2005;20:575–9.
Ghaderi S, Engeland A, Gunnes MW, Moster D, Ruud E, Syse A, et al. Educational attainment among long-term survivors of cancer in childhood and adolescence: a Norwegian population-based cohort study. J Cancer Surviv. 2016;10:87–95.
Gustafsson G, Schmiegelow K, Forestier E, Clausen N, Glomstein A, Jonmundsson G, et al. Improving outcome through two decades in childhood ALL in the Nordic countries: the impact of high-dose methotrexate in the reduction of CNS irradiation. Nordic Society of Pediatric Haematology and Oncology (NOPHO). Leukemia. 2000;14:2267–75.
Lancashire ER, Frobisher C, Reulen RC, Winter DL, Glaser A, Hawkins MM. Educational attainment among adult survivors of childhood cancer in Great Britain: a population-based cohort study. J Natl Cancer Inst. 2010;102:254–70.
Harila-Saari AH, Lähteenmäki PM, Pukkala E, Kyyrönen P, Lanning M, Sankila R. Scholastic achievements of childhood leukemia patients: a nationwide, register-based study. J Clin Oncol. 2007;25:3518–24.
Jacola LM, Edelstein K, Liu W, Pui CH, Hayashi R, Kadan-Lottick NS, et al. Cognitive, behaviour, and academic functioning in adolescent and young adult survivors of childhood acute lymphoblastic leukaemia: a report from the Childhood Cancer Survivor Study. Lancet Psychiatry. 2016;3:965–72.
Duffner PK. Long-term effects of radiation therapy on cognitive and endocrine function in children with leukemia and brain tumors. Neurologist. 2004;10:293–310.
Dieluweit U, Debatin KM, Grabow D, Kaatsch P, Peter R, Seitz DC, et al. Educational and vocational achievement among long-term survivors of adolescent cancer in Germany. Pediatr Blood Cancer. 2011;56:432–8.
Acknowledgements
The authors want to thank Thomas Tjørnelund Nielsen (Danish Cancer Institute, Childhood Cancer Research Group) for technical support with data acquisition and preparation. Prior presentations: Parts of this work was presented at the International Society of Paediatric Oncology annual conference 2021 (Online) and the Brain Tumour Epidemiology Consortium annual conference 2021 (Online). This manuscript was a part of a PhD-thesis (H. Mogensen) that was defended in public on the 12th of May 2022.
Funding
This work was supported by NordForsk under grant 76111, and the Swedish Childhood Cancer Foundation under grant PR2020-0130 and PR2022-0155. The funding sources had no role in the design of the study, collection, analysis, and interpretation of the data, writing of the manuscript, or the decision to submit the manuscript for publication. Open access funding provided by Karolinska Institute.
Author information
Authors and Affiliations
Contributions
HM, FE, MF, and JFW were responsible for the conceptualisation and study design. HM, JFW, MF, FE, LMH, NM, MT, EH, AKy, LEF, AKr, CP, and HH contributed to the acquisition and preparation of data. HM conducted the statistical analyses with supervision from FE, GT, and MF. HM drafted the original manuscript with input from FE, MF, GT, LEF, JH, and KM. All authors contributed to interpretation of the results, critically reviewed the manuscript for important intellectual content and provided feedback. HM and MF take responsibility for the integrity of the data and the accuracy of the data analysis. All authors approved the final version of the manuscript. The work reported in the paper has been performed by the authors, unless clearly specified in the text.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
The SALiCCS research programme has been approved by the Regional Ethical Review Board in Stockholm, Sweden (dnr 2016/25-31/5, 2016/1561-32, 2017/1656-32, 2017/1990-32, 2017/2340-32, 2018/1165-32), Findata (Dnro THL/5543/14.06.00/2020) prolonging the former approvals by the National Institute for Health and Welfare and Social Insurance (KELA) and Statistics Finland (TK-53-394-17). The SALiCCS research programme is listed in a local archive (2018-DCRC-0044) at the Danish Cancer Institute, which replaces the former approval from the Danish Data Protection Agency, and all data has been approved by, and stored, linked and analysed at a secure joint project platform at Statistics Denmark. Because of the register-based design all data were pseudonymized by the original registry holders, and researchers did not have access to personal identifiers. Thus, individual informed consent from participants was waived. The study was performed in accordance with the Declaration of Helsinki.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Mogensen, H., Tettamanti, G., Frederiksen, L.E. et al. Educational attainment in survivors of childhood cancer in Denmark, Finland, and Sweden. Br J Cancer 130, 260–268 (2024). https://doi.org/10.1038/s41416-023-02499-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41416-023-02499-1
- Springer Nature Limited
This article is cited by
-
Return to school practices after hematopoietic cell transplantation: a survey of transplant centers in the United States
Bone Marrow Transplantation (2024)