
Abstract
Objective
To evaluate educational impact of game-based learning (GBL) in orthodontic education.
Methods
A systematic search was undertaken across four databases (Scopus, PubMed, ProQuest Dissertations & Theses Global, and Google Scholar) to identify relevant articles published from January 2000 to December 2023. Additionally, the reference lists of identified literature were examined to further search for relevant literature. The last search was performed on 28 January 2024.
Results
Following the article selection process, seven articles were included in this systematic review, comprising four randomized control trials and three questionnaire surveys. Six articles were assessed to have a moderate risk of biases, whereas one research exhibited a low risk of bias. GBL interventions assessed in five articles were designed in digital format, while one study implemented evaluated traditional learning, and another employed a card game format. Two RCTs indicated a greater effectiveness of GBL in enhancing learner performance compared to traditional learning methods, while one article found no significant difference. Across all articles, positive perceptions of GBL were consistently highlighted at both undergraduate and postgraduate levels.
Conclusion
This systematic review supports the potential of GBL in orthodontic education. The implementation of GBL is recommended to integrate entertaining and educational elements, fostering learner performance within engaging learning environments. However, it is imperative to acknowledge that the overall quality of evidence is limited, primarily due to the moderate risk of biases identified in six of the included articles. Consequently, further high-quality experimental studies are required to validate the effectiveness of GBL in orthodontic education.
Similar content being viewed by others


Introduction
Orthodontics is a dental specialty that emphasizes diagnosing, preventing, and managing craniofacial problems and malocclusions, with a variety of fixed and removable orthodontic appliances [1]. World Federation of Orthodontists (WFO) has set the goals for orthodontic education as to develop learner competencies covering both specific and general skills such as lifelong learning and communication skills [2]. Not only a cognitive domain, but also psychomotor skills are required for orthodontists, which include bracket placement and wire bending [3]. These competencies will allow orthodontists to manage orthodontic problems with patient safety and maintain their skills and knowledge.
A variety of teaching and learning approaches should be required for orthodontic education. Lectures, seminars, and clinical practice are generally required for orthodontic training [2]. Case-based learning can also be considered as effective for orthodontic courses [4]. In addition, technology-enhanced simulations including virtual realities appear to be effective learning strategies in orthodontic education, as they allow learners to improve their competence in safe learning environments [5]. Virtual setups could also be used for learning orthodontic treatment planning through tooth movement simulation [6]. A combination of teaching strategies will support learners to achieve expected learning outcomes in orthodontic education.
Game-based learning (GBL) can be considered as another interactive teaching and learning strategy. There appears to be an increasing use of GBL in dental education [7]. This approach allows learners to gain knowledge and skills through feedback provided during task completion [8, 9]. An entertaining component could engage students with their lessons [10]. There is evidence demonstrating effectiveness of GBL in dental education although further high-quality research is not yet sufficient [7, 11, 12]. Considering these arguments, GBL should be recommended for orthodontic training programs.
Albeit the advantages of the GBL, its educational impact over traditional methods has not yet been clearly evident. In addition, although there had been an increase in research evaluating GBL in orthodontic education, its effectiveness has not been yet comprehensively reviewed. Therefore, this systematic review was conducted to evaluate educational impact of GBL in orthodontic education.
Materials and methods
Review design
A systematic review was selected to evaluate whether or not GBL can have educational impact in orthodontic training. This method employed scientific procedures to prevent potential biases in systematically reviewing available evidence, enabling researchers to critically synthesize relevant information into comprehensive evidence [13, 14].
Search strategy
The systematic search was conducted across four electronic databases, which were Scopus, PubMed, ProQuest Dissertations & Theses Global (PQDT), and Google Scholar. In addition, the reference lists of included articles were screened for additional relevant evidence. Gray literature was also sought to encompass research in GBL wherever feasible. Systematic searches were iteratively performed to develop a robust search strategy [15]. The search terms were developed following the PICO approach (Table 1). However, terms for comparison were omitted from the search strategy to enhance sensitivity.
Inclusion and exclusion criteria
All types of empirical studies evaluating GBL in orthodontic education published from January 2000 to December 2023 were considered as inclusion criteria for this systematic review. However, articles were excluded if they focused on GBL designed for patients or laypeople rather than orthodontic learners. Articles without describing details of GBL or without presenting its education impact were excluded. They were also excluded if they were not available in full-text. These inclusion and exclusion criteria are presented in Table 2.
Article selection
Following the systematic search, titles, abstracts, and full-text were independently screened by two researchers (K.S. and R.C.) by considering inclusion and exclusion criteria. Any disagreements on the article selection between the researchers were resolved by discussing and consulting with the third researcher (T.N.).
Risk of bias assessment for included articles
The risk of bias assessment of included articles can be considered as essential, as the quality of evidence could reflect the strength of systematic reviews. A risk of bias assessment of articles included in this systematic review was performed by a researcher (KS), which was then verified by another one (RC).
The bias assessment of articles with randomized control trials (RCTs) was performed using a revised tool for assessing risk of bias in randomized trials (RoB 2), which included five domains: (1) Randomisation process, (2) Deviations from intended interventions, (3) Outcome data missing, (4) of Outcome measurement, and (5) Selection of reported results [16]. The judgements included “low risk of bias,” “some concerns”, or “high risk of bias” [16]. However, in this systematic review, ‘some concerns’ were labeled as ‘moderate risk of bias’ to facilitate comparison with non-RCTs.
For included articles of non-RCTs, the bias assessment was conducted using the Cochrane Collaboration tool which is ‘Risk of Bias In Non-randomized Studies of Interventions’ (ROBINS-I), which included seven domains: (1) Confounding, (2) Participant selection, (3) Intervention classification, (4) Deviations from intended interventions, (5) Data missing, (6) Outcome measurement, and (7) Selection of reported results, in which the risk of bias was evaluated whether it is low, moderate, serious, or critical [17].
Data extraction and synthesis
The data retrieved from included articles were extracted in the following aspects: details of GBL, learning subjects, research objectives, methodology, outcome measurement, key findings, and risk of bias assessment (Table 3). A narrative approach was conducted to synthesize the extracted data.
Results
Articles identified from the search
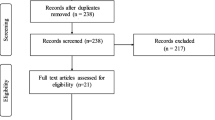
The flow of article selection process was presented in the PRISMA diagram (Fig. 1), the search through the four electronic databases revealed 342 articles (PubMed = 233, Scopus = 64, and PQDT Global = 45). Following the removal of 62 duplicate records, 280 articles were screened based on the consideration of their titles and abstracts according to the inclusion and exclusion criteria, in which 261 of them were excluded. Together with three articles identified from the citation searching (n = 1) and Google Scholar (n = 2), 22 full-texts were assessed for their eligibility, where 15 articles were excluded due to being relevant to GBL for maxillofacial surgeons rather than orthodontic practitioners (n = 6), being relevant to learning interventions considered as non-GBL (n = 4), and no education impact of GBL reported (n = 5). Consequently, there were seven full-texts included in this systematic review [18,19,20,21,22,23,24].

PRISMA 2020 flow diagram of the article selection process.
Characteristics of articles included in this systematic review
Four articles evaluated GBL using RCTs to compare its educational impact between GBL and traditional learning approaches [18, 19, 21, 22]. Three studies employed a survey design to explore learner perceptions toward the use of GBL without controlled group [20, 23, 24]. Only one article evaluated the educational impact of GBL in orthodontic postgraduates [21], while the remaining research investigated impact in dental undergraduates [18,19,20, 22,23,24]. Most of the included studies were assessed to have a moderate risk of biases [18, 20,21,22,23,24], whereas one research article exhibited a low risk of bias [19].
Characteristics of GBL evaluated in the included articles
GBL in all included articles emphasized on the educational impact on cognitive domain [18,19,20,21,22,23,24]. Five articles evaluated GBL in digital format designed specifically for orthodontic education were technology enhanced learning [19,20,21,22,23], one research gamified traditional learning approach with the incorporation of audience response system to traditional [18], and one GBL was a card game format [24]. The topics for GBL were varied, covering basic orthodontic concept [18, 22, 24], model analysis [23], cephalometric tracing and analysis [21, 23], prediction in orthognathic surgery [19], and orthodontic bracket bonding [20].
Educational outcomes of the interventions in the included articles
Performance improvement
Three studies evaluated learner performance following the completion of GBL tasks [18, 19, 21], all of which concluded that GBL could offer cognitive improvement in specific aspects of orthodontic education. However, the expected learning outcomes to be achieved across these GBL interventions varied. One study demonstrated better knowledge retention among dental undergraduates with the implementation of an audience response system as an element of GBL [18]. Another study revealed a higher level of cephalometric tracing accuracy among orthodontic residents following the use of shooting game-based activities, although no significant difference of tracing speed was observed [21]. These two studies indicated that GBL can be effective in enhancing learner performance compared to traditional learning methods in orthodontic education. However, one research found no significant difference in knowledge improvement related to the diagnosis and treatment planning of orthognathic cases [19].
User experiences
Six articles investigated user experience toward the use of GBL in orthodontic education contexts, employing questionnaires to assess learner experiences, particularly in terms of enjoyment and engagement, following the learning tasks [18, 20,21,22,23,24]. Among them, three RCTs compared user perceptions between GBL and traditional learning, revealing that participants tended to perceive GBL as more positively in terms of both learning and motivating aspects [18, 21, 22]. However, class involvement of participants was significantly different between GBL and traditional learning [18]. The remaining three articles conducted questionnaire surveys following the GBL activities and found that participants tended to perceive GBL as an effective learning approach, with all studies reporting positive perceptions toward GBL [20, 23, 24]. The findings across the six articles highlighted a notable trend toward favorable perceptions of GBL in orthodontic education at both undergraduate and postgraduate levels.
Discussion
This systematic review revealed an increasing use of GBL in orthodontic education in recent years, where only one article was published before 2020 [18]. This trend demonstrated a delayed implementation of GBL in orthodontic education, compared to other healthcare disciplines [7]. The rising number of GBL interventions may be attributed to 3D modeling technologies in orthodontic practice [5]. Nearly all GBL interventions evaluated in the included articles were developed for dental undergraduates, while only one study was conducted among orthodontic residents. This could be a result from the fact that orthodontic residents, unlike undergraduate students, are already committed to pursuing their specialty in the field and are highly motivated to acquire knowledge and skills. Postgraduates prioritize the mastery of clinical practice within a specific area as the primary considerations in making decisions about fellowships [25]. Consequently, strategies to promote learning motivation and engagement may be perceived as relatively less important for postgraduates compared undergraduates.
Available evidence has demonstrated that GBL in orthodontic education yields positive educational outcomes, comparable to traditional learning approaches. The necessity of acquiring knowledge and improving skills has become an important component when assessing GBL within healthcare education [7, 26,27,28,29]. These outcomes were evaluated through learner performance and self-perceived assessments. Dental students have the opportunity to enhance their knowledge through feedback received following their interactions within GBL environments [30,31,32]. Technology could enhance GBL to provide immediate feedback enabling interactive asynchronous learning [7]. Certainly, this highlights the positive impact of GBL on orthodontic education by enhancing learner knowledge and competence.
GBL also provides entertaining support, facilitating learner engagement with the learning content. Evidence from all reviewed articles suggests that learners view GBL interventions positively, emphasizing their entertainment value, particularly citing their embedded features such as immediate feedback [18, 23] and competition components [21, 24]. Additionally, a VR format provides an immersive learning environment, reducing distractions from the surrounding environment [19, 20, 22]. These entertainment components motivate learners to actively participate and sustain their interest throughout the learning tasks, facilitating the repetition of a game cycle [33]. Consequently, the integration of entertaining and educational components is essential to engage learners in GBL activities, ultimately leading to the achievement of learning outcomes.
All GBL approaches evaluated in the included articles were primarily designed to enhance cognitive abilities. Despite the hands-on nature of orthodontic practice [2], none of the reviewed articles specifically assessed GBL with a focus on psychomotor skills. Haptic technologies can be integrated into GBL to simulate clinical situations, offering users the opportunity to improve their proficiency in specific tasks [34]. This emphasis on psychomotor skills within GBL could be particularly beneficial for orthodontic residents seeking to gain experience and proficiency in tasks such as wire bending, bracket positioning, or mini-implant placement. Consequently, this expansion of GBL applications to orthodontic postgraduates could enhance skill acquisition and proficiency, with a focus on advanced techniques, supplementing the basic concepts usually addressed at the undergraduate level.
This systematic review was carefully constructed to ensure methodological robustness, where two researchers independently screened and selected identified articles to mitigate potential selection bias. Furthermore, the review had no language restrictions in article selection, thereby minimizing language bias. However, there appears to be heterogeneity in the research outcomes of the included articles, including cognitive improvement, knowledge retention, tracing performance, and learning motivation. Concerning the quality of included articles, only one exhibited a low risk of bias, while the remaining six raised concerns regarding bias. Consequently, additional RCTs with rigorous research design are required to evaluate specific learning outcomes. This is crucial for facilitating meta-analysis aimed at confirming the efficacy of GBL in orthodontic education. Qualitative research should also be performed to investigate in-depth information on how orthodontic residents achieve learning outcomes within the repetition of the game cycle.
Conclusion
Limited evidence from the articles included in this systematic review demonstrates the potential of GBL in orthodontic education, particularly for cognitive enhancement at the undergraduate level. Students were able to improve their knowledge and comprehension with engagement and motivation through learning activities that integrated entertaining and educational components. However, further research on the application of GBL to enhance skill acquisition and proficiency in orthodontic postgraduates is necessary to ascertain the effectiveness of GBL in orthodontic education.
Data availability
The data that support the findings of this study are available from the corresponding author, up-on reasonable request.
References
Chadwick SM, Bearn DR, Jack AC, O’Brien KD. Orthodontic undergraduate education: developments in a modern curriculum. Eur J Dent Educ. 2002;6:57–63. https://doi.org/10.1034/j.1600-0579.2002.60203.x.
Ono T, Pangrazio-Kulbersh V, Perillo L, Artese F, Czochrowska E, Darendeliler MA, et al. World Federation of Orthodontists guidelines for postgraduate orthodontic education. J World Federation Orthod. 2023;12:41–9. https://doi.org/10.1016/j.ejwf.2023.03.002.
Proffit WR, Fields HW, Larson B, Sarver DM. Contemporary Orthodontics, 6th ed.; Elsevier: 2018.
Alhazmi A, Quadri MFA. Comparing case-based and lecture-based learning strategies for orthodontic case diagnosis: a randomized controlled trial. J Dent Educ. 2020;84:857–63. https://doi.org/10.1002/jdd.12171.
Sipiyaruk K, Kaewsirirat P, Santiwong P. Technology-enhanced simulation-based learning in orthodontic education: a scoping review. Dent Press J Orthod. 2023;28:e2321354. https://doi.org/10.1590/2177-6709.28.3.e2321354.oar.
Sereewisai B, Chintavalakorn R, Santiwong P, Nakornnoi T, Neoh SP, Sipiyaruk K. The accuracy of virtual setup in simulating treatment outcomes in orthodontic practice: a systematic review. BDJ Open. 2023;9:41. https://doi.org/10.1038/s41405-023-00167-3.
Sipiyaruk K, Hatzipanagos S, Reynolds PA, Gallagher JE. Serious games and the COVID-19 pandemic in dental education: an integrative review of the literature. Computers. 2021;10:42.
Buajeeb W, Chokpipatkun J, Achalanan N, Kriwattanawong N, Sipiyaruk K. The development of an online serious game for oral diagnosis and treatment planning: evaluation of knowledge acquisition and retention. BMC Med Educ. 2023;23:830. https://doi.org/10.1186/s12909-023-04789-x.
Sipiyaruk K, Hatzipanagos S, Vichayanrat T, Reynolds PA, Gallagher JE. Evaluating a dental public-health game across two learning contexts. Educ Sci. 2022, 12, https://doi.org/10.3390/educsci12080517.
Breuer J, Bente G. Why so serious? On the relation of serious games and learning. Eludamos. J Comput Game Cult. 2010;4:7–24.
Sipiyaruk K, Gallagher JE, Hatzipanagos S, Reynolds PA. A rapid review of serious games: from healthcare education to dental education. Eur J Dent Educ. 2018;22:243–57. https://doi.org/10.1111/eje.12338.
Zaror C, Mariño R, Atala-Acevedo C. Current state of serious games in dentistry: a scoping review. Games Health J. 2021;10:95–108. https://doi.org/10.1089/g4h.2020.0042.
Moher D, Cook DJ, Eastwood S, Olkin I, Rennie D, Stroup DF. Improving the quality of reports of meta-analyses of randomised controlled trials: the QUOROM statement. Onkologie. 2000;23:597–602. https://doi.org/10.1159/000055014.
Cook DJ, Sackett DL, Spitzer WO. Methodologic guidelines for systematic reviews of randomized control trials in health care from the Potsdam Consultation on Meta-Analysis. J Clin Epidemiol. 1995;48:167–71. https://doi.org/10.1016/0895-4356(94)00172-m.
Snyder H. Literature review as a research methodology: an overview and guidelines. J Bus Res. 2019;104:333–9. https://doi.org/10.1016/j.jbusres.2019.07.039.
Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898 https://doi.org/10.1136/bmj.l4898.
Sterne JAC, Hernán MA, Reeves BC, Savović J, Berkman ND, Viswanathan M, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016;355:i4919. https://doi.org/10.1136/bmj.i4919.
Dhaliwal HK, Allen M, Kang J, Bates C, Hodge T. The effect of using an audience response system on learning, motivation and information retention in the orthodontic teaching of undergraduate dental students: a cross-over trial. J Orthod. 2015;42:123–35. https://doi.org/10.1179/1465313314y.0000000129.
Sakowitz SM, Inglehart MR, Ramaswamy V, Edwards S, Shoukri B, Sachs S, et al. A comparison of two-dimensional prediction tracing and a virtual reality patient methods for diagnosis and treatment planning of orthognathic cases in dental students: a randomized preliminary study. Virtual Real. 2020;24:399–409. https://doi.org/10.1007/s10055-019-00413-w.
Huang Y, Cheng X, Chan U, Zheng L, Hu Y, Sun Y, et al. Virtual reality approach for orthodontic education at School of Stomatology, Jinan University. J Dent Educ. 2022;86:1025–35. https://doi.org/10.1002/jdd.12915.
Zhang Z, Liao W, Xiong X, Zhu R, Wang J. Evaluation of online game-based and traditional teaching methods in cephalometric landmarks identifications. Am J Orthod Dentofac Orthopedics. 2022;161:e534–e543. https://doi.org/10.1016/j.ajodo.2021.09.014.
Chen D, Liu X, Liu Y, Wang X, Zheng J, Wu L. Virtual reality used in undergraduate orthodontic education. Eur J Dental Educ. 2023, https://doi.org/10.1111/eje.12968.
Rahmani N, Davoodabadi F, Noormohammadi R, Karamitanha F, Nourian A. Using edutainments in teaching orthodontic lateral cephalometric and dental cast analysis. J Med Edu. 2023;22:e134615. https://doi.org/10.5812/jme-134615.
Tran LK, Lipp MJ. Making competency-based predoctoral orthodontics fun: Introducing dealodontics. J Dent Educ. 2023;87:385–93. https://doi.org/10.1002/jdd.13133.
Borman KR, Biester TW, Rhodes RS. Motivations to pursue fellowships are gender neutral. Arch Surg. 2010;145:671–8. https://doi.org/10.1001/archsurg.2010.116.
Maheu-Cadotte M-A, Cossette S, Dubé V, Fontaine G, Lavallée A, Lavoie P, et al. Efficacy of serious games in healthcare professions education: a systematic review and meta-analysis. Simul Healthc. 2021;16:199–212.
Min A, Min H, Kim S. Effectiveness of serious games in nurse education: a systematic review. Nurse Educ Today. 2022;108:105178. https://doi.org/10.1016/j.nedt.2021.105178.
Xu M, Luo Y, Zhang Y, Xia R, Qian H, Zou X. Game-based learning in medical education. Front Public Health. 2023, 11, https://doi.org/10.3389/fpubh.2023.1113682.
Hope DL, Grant GD, Rogers GD, King MA. Gamification in pharmacy education: a systematic quantitative literature review. Int J Pharm Pract. 2023;31:15–31. https://doi.org/10.1093/ijpp/riac099.
Arayapisit T, Pojmonpiti D, Dansirisomboon K, Jitverananrangsri K, Poosontipong D, Sipiyaruk K. An educational board game for learning orofacial spaces: An experimental study comparing collaborative and competitive approaches. Anat Sci Educ. 2023;16:666–76. https://doi.org/10.1002/ase.2257.
Amir LR, Leonardy IC, Dewatmoko SN, Yanuar R, Suniarti DF, Idrus E, et al. Serious game as oral histology learning strategy for undergraduate dental students; crossover randomized controlled trial. BMC Oral Health. 2023;23:585. https://doi.org/10.1186/s12903-023-03286-3.
Teerawongpairoj C, Tantipoj C, Sipiyaruk K. The design and evaluation of gamified online role-play as a telehealth training strategy in dental education: an explanatory sequential mixed-methods study. Sci Rep. 2024;14:9216. https://doi.org/10.1038/s41598-024-58425-9.
Garris R, Ahlers R, Driskell JE. Games, motivation, and learning: a research and practice model. Simul Gaming. 2002;33:441–67. https://doi.org/10.1177/1046878102238607.
Mäkinen H, Haavisto E, Havola S, Koivisto J-M. User experiences of virtual reality technologies for healthcare in learning: an integrative review. Behav Inf Technol. 2022;41:1–17. https://doi.org/10.1080/0144929X.2020.1788162.
Acknowledgements
We would like to express our sincere gratitude to Associate Professor Udom Thongudomporn for his invaluable insights to enhance the quality of this article.
Author information
Authors and Affiliations
Contributions
Conceptualization, KS, PAR, TN, PS, and RC; methodology, KS, PAR, TN, PS, and RC; validation, KS, TN, and RC; investigation, KS, TN, and RC; formal analysis, KS and RC; data curation, KS and RC; writing-original draft preparation, KS, PAR, TN, PS, and RC; writing-review and editing, KS, PAR, TN, PS, and RC All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
Ethical approval was not required for this systematic review, as only publicly accessible documents were used as evidence.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Sipiyaruk, K., Reynolds, P.A., Nakornnoi, T. et al. Game-based learning in orthodontic education: a systematic review. BDJ Open 10, 56 (2024). https://doi.org/10.1038/s41405-024-00218-3
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41405-024-00218-3
- Springer Nature Limited