
Abstract
In the past period, due to the rapid development of next-generation sequencing technology, accumulating evidence has clarified the complex role of the human microbiota in the development of cancer and the therapeutic response. More importantly, available evidence seems to indicate that modulating the composition of the gut microbiota to improve the efficacy of anti-cancer drugs may be feasible. However, intricate complexities exist, and a deep and comprehensive understanding of how the human microbiota interacts with cancer is critical to realize its full potential in cancer treatment. The purpose of this review is to summarize the initial clues on molecular mechanisms regarding the mutual effects between the gut microbiota and cancer development, and to highlight the relationship between gut microbes and the efficacy of immunotherapy, chemotherapy, radiation therapy and cancer surgery, which may provide insights into the formulation of individualized therapeutic strategies for cancer management. In addition, the current and emerging microbial interventions for cancer therapy as well as their clinical applications are summarized. Although many challenges remain for now, the great importance and full potential of the gut microbiota cannot be overstated for the development of individualized anti-cancer strategies, and it is necessary to explore a holistic approach that incorporates microbial modulation therapy in cancer.
Similar content being viewed by others


Introduction and overview
The human microbiota is dynamically composed of nearly 40 trillion microorganisms with 3000 species, including bacteria, fungi, and viruses, exhibiting variable richness among microbes and diverse constituents among individuals, and is significant for the maintenance of systematic homeostasis and functional stability.1,2,3,4,5 The vast majority of members of the human microbiota is located in the gastrointestinal tract (more than 97%), especially in the colon,1,6 named the gut microbiota, which has been extensively studied and confirmed to mediate a wide range of physiological functions, such as the development of the immune system and the synthesis of some nutrients.2,7,8,9 Gut dysbiosis occurs when the balance between the microbiota and the human host is disturbed, and manifests as changes in taxonomic composition, metabolic products and secretory vesicles, all of which have been linked to physiological disorders across a broad spectrum of illnesses including cancer.10,11,12,13,14,15,16,17,18,19,20
In addition to microorganisms within the digestive tract, the intratumoral microbiota has also drawn increasing attention in the era of precision medicine, since microbes colonizing the tumor microenvironment (TME) may be one of the causes leading to the cancer progression and the discrepancies in the efficacy of cancer therapies among patients.21,22,23,24,25,26 Actually, the local diversity and neoplasm-associated significance of intratumoral microbes were not broadly and deeply investigated until the development of next- and third-generation sequencing in recent years,27,28,29 despite their existence being reported a century ago.30 In contrast to its intestinal counterpart, the complex characterization of the intratumoral microbiota is still at an infancy stage, and its roles have not been fully characterized, although some understanding has been gained regarding how it impacts tumorigenesis and therapeutic efficacy. Two main reasons could account for this. The one is, intratumoral microbes are mostly intracellular and are present in cancer cells as well as their surrounding immune cells, which requires more sensitive observation methods to identify the location of intracellular bacteria.31,32,33 The other one is that, the biomass of microorganisms within the TME is very low compared to their gut counterparts, and even just 1 microbial cell may be found in every 104 tumor cells,34 which also greatly hinders the investigation of the intratumoral microbiome. Thus, it is necessary to overview some latest mechanistic studies using cutting-edge research methods, which would provide reference for other researchers.
The influences of the gut/tumor microbes on cancer development and treatment, favorable or detrimental, have already been demonstrated in massive mouse experiments. Above all, available evidence from animal experiments has shown that microbes can facilitate the initiation and progression of various types of cancer including gastric cancer,35,36 colorectal cancer,37,38 hepatocellular carcinoma,39,40 breast cancer20,31 and pancreatic ductal adenocarcinoma41,42. Furthermore, poor response after receiving cancer treatment, including chemotherapy,43,44 radiotherapy,45,46 surgery and immunotherapy,47,48 can be partially ascribed to some microbes, which was also confirmed in mice. The concrete research methods of these preclinical studies are different, but they have a common ground, that is, the pretreatment method for the mice. Specifically, the mice in these studies are inherently germ-free, or they would be pretreated with antibiotic to ensure the consistency of regular microbiota. The research methods are summarized in the Table 1.
The microbiota in the alimentary tract and TME can be considered, to some extent, as a dynamic system whose internal compositions are both interconnected and relatively independent. Specifically, tumors and other causes of the disruption of the intestinal mucosal barrier may provide access for the gut microbes, resulting in their switching to intratumoral microbes directly involved in the development of cancer.49 Thus, it is not surprising that both gut and intratumoral microbes can exert cancer-promoting effects.41,50,51,52,53,54,55 In the early stages of many digestive cancers, alterations at the cellular level in the alimentary tract often shows up as gut dysbiosis, followed by the pro-carcinogenic effects of various bacterially secreted oncogenic molecules. More importantly, diverse molecular mechanisms by which pathogenic microbes contribute to tumorigenesis56,57 have been found over the past few years. For example, a genotoxin called colibactin generated by pathogenic pks+ Escherichia coli can alkylate DNA, which may be involved in the development and progression of colon cancer.58,59 In addition, other typical tumor-related bacteria, such as Fusobacterium nucleatum and Helicobacter pylori (Hp), can promote cancer through a complex set of mechanisms, including chronic inflammation, DNA damage, and the activation of oncogenic pathways.60,61,62,63,64,65
The carcinogenic and anti-cancer mechanisms of microbes are extremely intricate, and only a tip of the iceberg has been thoroughly probed. Nonetheless, the potential of microbial strategies for cancer therapy have been demonstrated in many clinical trials. Specifically, human microbiota can be modified to boost the host response to the existing anti-cancer therapies and minimize the corresponding adverse toxicities and reduce drug resistance in immunotherapy, chemotherapy, cancer surgery, and radiation therapy, and specific interventions targeting the microbiota include (but not limited to) diet-based interventions, prebiotics, probiotics, postbiotics, targeted antibiotic approaches, and fecal microbiota transplantation (FMT).66,67 For example, clinical research results generated by Zheng et al. indicated that probiotic compound can significantly relieve inflammation, enhance immunity, and promote recovery in patients with gastric cancer after gastrectomy, and thus it may serve as an adjuvant treatment for gastric cancer in the future.68
One of the ultimate purposes of basic research is for clinical practice, and thus follow-up clinical trials based on the preclinical findings need to be designed and conducted as much as possible. Pan and colleagues have found that Clostridium butyricum strains MIYAIRI 588 (CBM588) can ameliorate acute pancreatitis by maintaining intestinal homeostasis in mice,69 and a recently published clinical trial showed that CBM588 can obviously prolong progression-free survival (PFS) in patients with metastatic renal cell carcinoma treated with nivolumab-ipilimumab.70 Against this background, animal experiments were conducted to preliminarily explore the properties of CBM588 in a general direction, and another team subsequently confirmed the anti-cancer effect of CBM588 through clinical trial based on the previous findings. Thus, combining basic mechanistic studies with corresponding clinical trials is essential, which will be conducive to moving the field of microbiology-oncology gradually forward from bench to bedside. However, the road that combines clinical trials with the basic studies is full of challenges, which presents a great obstacle to clinical translation of microbial strategies for cancer therapy. For example, unlike animal models, the baseline characteristics of the gut microbiota among human subjects are hard to keep consistent artificially, which dramatically impedes the design and implementation of corresponding clinical trials.
In this review, the initial clues of molecular mechanisms regarding the carcinogenic effects of gut and tumor microbes are first summarized, based on which the significance of microbes for conventional cancer treatment is also addressed. In addition, current and emerging microbial interventions for cancer therapy as well as their clinical applications are also highlighted, with emphasis on the latest major studies on boosting the efficacy of traditional cancer treatment and reducing its side effects via microbial strategies, which may provide insights into the formulation of individualized therapeutic strategies for cancer therapy. Finally, the authors’ perspectives regarding the outlook and challenges of microbial strategies in basic studies and clinical translation are summarized.
Contributions of microbes from different dimensions in cancer development
Gut dysbiosis refers to a less stable and diverse and more pathogenic microbiota that is reshaped when the sophisticated balance of the microecosystem in the gastrointestinal tract is disturbed, which contributes to a variety of pathological conditions by adversely affecting the physiological processes of the host.71,72 More importantly, pathogenic microbes may have a harmful impact in the development and treatment of cancer.73,74 To gain a better understanding of the molecular mechanisms, the influence of microbes on normal epithelial tissue and tumor microenvironment should first be explained before further discussion.
The microbes can impact cancer in various manners,75,76 one of which is contact-dependent effects that occur locally at the mucosal surface or in the TME. Another is contact-independent effects, which are systematically present via microbial metabolites and outer membrane vesicles (OMVs) in circulation. (Fig. 1) The concept of contact-dependent effects is well understood, but the mechanisms involved in contact-independent effects may be slightly more complex. Herein, contact-independent effects are defined as a biological phenomenon in which gut microbiota-derived detrimental molecules enter the bloodstream through capillaries, directly facilitating the development of distant cancer, or indirectly promoting its progerssion by weakening the antitumor immunity of the host. For example, lipoteichoic acid (LTA) and deoxycholic acid (DCA), a cell wall component and a metabolite of gram-positive gut bacteria, respectively, have been corroborated to promote the development of hepatocellular carcinomas after translocation into the liver through the enterohepatic circulation,77,78 which is typical contact-independent effect of gut microbes on cancer. In this chapter, we will depict the effects of microbes in cancer development from two different dimensions.

Interactions between the gut microbiota and cancer development. The gut microbiota can interact with cancer through various patterns, one of which is contact-dependent interactions that occur locally at mucosal surface or within primary lymphoid organs including the bone marrow and the thymus (a), and secondary lymphoid organs including the GALT, lymph nodes and the spleen (b) or the TME (c). Another one is contact-independent interactions which present systematically via microbial metabolites and OMVs in circulation (c). Specifically, a Gut microbes can interact directly with the gastrointesinal tract mucosal surface, resulting in genotoxic effect, epithelial cell proliferation, loss of cellular polarity, intestinal metaplasia; the hematopoiesis of the thymic and bone marrow could be stimulated by microbiota via RIG-IFN-1 signaling especially after HSCT, thus making radio-protective effect in the radiotherapy. b Gut microbes and their metabolites or OMVs interact with the GALT, LN and spleen, through the T cells and dendritic cells regulations via various patterns, such as enhancement of the TH17 response, IFN production, antigen presentations and signaling of IFN-1, IL-12, TLR4. c Microbes both in the gut and tumor could exert influence on the TME, either with immunostimulatory effect via presenting microbial specific antigen to the T cells, or with immunosuppressive effect via regulating the balance of the Treg and TILs. Besides, microbial modulation of the TME exemplified are means by which microbiome-secreted metabolites, cargo-carrying OMVs, or may induce a complex array of immunomodulatory actions via circulation. Microbial secreted moieties can impact the TME innate immune response, by modulating attraction and activation of innate immune cells such as neutrophils, producing TNFα and ROS to combat tumorigenesis, and influence the adaptive immune response by co-stimulating T cells mentioned above. (HSCT hematopoietic stem cell transplant, DC dendritic cell, GALT gut-associated lymphoid tissues, LN lymph node, TLR4 Toll-like receptor 4, TME tumor microenvironment, CTL cytotoxic T lymphocyte, NK cell natural killer cell, OMVs outer membrane vesicles, SCFAs short-chain fatty acids, TIL tumor-infilrating lymphocyte, PRR pattern recognition receptor, MDSC myeloid-derived suppressor cells, ROS reactive oxygen species, TNF α tumor necrosis factor α)
The effects of microbes on intestinal mucosal surface
Normally, the gut microbiota in healthy human body is generally considered as beneficial, but some luminal microbes may pose a potential threat to the host. Compared with healthy individuals, a variety of microbes are more frequently observed in the stool and on the gut mucosa of patients with gastrointestinal tumors,79,80,81 and in vivo experiments have shown that microorganisms play a paramount role in carcinogenesis.82,83 However, we still know little about the direct impacts of microbes on normal gut epithelial cells (ECs). In this section, we will emphasize how certain bacteria within the alimentary tract directly affect ECs and trigger malignant transformation.
When investigating the effects of microorganisms on cancer initiation, the first issue we should determine is whether they cause DNA damage and abnormal gene mutations in ECs. H. pylori plays a nonnegligible role in the process of gastric cancer initiation, and one of its main mechanisms inducing gastric carcinogenesis is causing DNA damage via oxidative stress in the gastric mucosa.84 Prior to direct contact with ECs, H. pylori secretes proteases and phospholipases to degrade the mucus layer on the mucosal surface in the stomach, which enhances H. pylori adherence.85 Subsequently, cytotoxin-associated gene A (CagA), one of the main virulence factors generated by H. pylori, upregulates the levels of spermine oxidase (SMO) that metabolizes the polyamine spermine into spermidine and generate H2O2, which would cause apoptosis and DNA damage of ECs; thus, a subpopulation of epithelial cells gradually becomes resistant to apoptosis and is at high risk for malignant transformation.84,86 To sum up, some pathogenic microorganisms have the ability to colonize the mucosal surface of digestive tract and can increase the risk of malignant transformation in ECs through DNA damage mechanism.
Bacteria may also induce epithelial inflammation and the disruption of the mucosal barrier, both of which are linked to the carcinogenesis. F. nucleatum, one of the resident bacteria constituting the oral microbiota, has been confirmed to accelerate the initiation, progression and metastasis of colorectal cancer (CRC) in recent studies,87,88 and its impact on intestinal epithelial cells has been increasingly identified. Engevik et al. found that F. nucleatum subsp. polymorphum can release OMVs to activate TLR4 and NF-κB on colonic epithelial cells, which ultimately stimulates the production of downstream proinflammatory factors associated with intestinal inflammation.89 Remarkably, the proinflammatory effects were absent in the context of an intact gut microbiota, which implicitly indicated the significance of a normal gut microbiota. Additionally, OMVs secreted from F. nucleatum can also adversely alter the epithelial homeostasis by impairing the intestinal mucosal barrier in ulcerative colitis.90 Because chronic inflammation and disruption of the intestinal mucosal barrier can increase the risk of tumorigenesis,91,92 we assume that the effects of F. nucleatum on ECs and mucosal barrier are the significant causes that induce the transformation of precancerous conditions to cancer.
The interactions between microbes and the tumor microenvironment (TME)
The TME is the internal environment upon which the existence and proliferation of tumor cells depend, and it contains a variety of cells, including tumor cells, stromal cells, and immune cells (such as T lymphocytes, B lymphocytes, natural killer cells, and tumor-associated macrophages), as well as a dense network of microvessels.93 Apart from the regular components, growing evidence has shown that bacteria reside in the cancer cells and immune cells within the TME,31,32 which has an underlying impact on the biological phenotype of cancer cells and local immune microenvironment within the TME.
On account of some inherent characteristics in tumors, the TME is well-suited for the invasion, colonization and growth of microbes. First, during the process of carcinogenesis, many angiogenic factors released by tumor cells induce vascularization,94 which is conducive to the invasion of distant microbes into TME. Additionally, tumor is generally characterized by inherent immune privilege,95 and microbes within the TME can also serve as immune inhibitors.96 This combined immunosuppressive phenomenon is favorable for the colonization and growth of intratumoral microbes.
Moreover, the conditions within the TME, such as local oxygen concentration, can influence the composition of tumor microbiota. For example, hypoxic and even anoxic inner regions is a characteristic feature of many solid tumors arising from an imbalance between oxygen supply and consumption,97,98 which is accompanied by the resultant accumulation of microaerophilic and anaerobic bacteria in the TME, such as Bacteroides fragilis and Enterococcus faecalis in CRC,99 and the relative abundance of aerobic bacteria in the tumor may be lower. Notably, there is spatial heterogeneity of oxygen concentration within tumor;100 however, it is unclear whether this uneven oxygen distribution would lead to diverse microbial members across different regions within the TME, which needs further study. Additionally, distinct microbiome compositions have been discovered across different tumor types,32 which may be a result from multifaceted effects, and more and further investigation is needed.
Intratumoral bacteria may affect the phenotype of cancer, such as enhancing the metastatic ability of malignant cells. Using the murine spontaneous breast-tumor model, Fu and colleagues found that significant amounts of tumor-resident bacteria reside in the cytoplasm of cancer cells and that these bacteria can facilitate the metastasis in breast cancer by reorganizing the cellular cytoskeleton and enhancing resistance to mechanical stress.31 Additionally, a conserved intracellular bacterial profile represented by Enterococcus and Streptococcus was also detected in human breast cancer, which could metastasize to distant sites with cancer cells.31 Thus, the two findings collectively suggest that microbes inhabit in human breast cancer, and the bug may promotes cancer progression. Similarly, F. nucleatum can reinforce the metastatic potential of CRC through various complex mechanisms.101,102 Additionally, other biological behaviors of CRC, including proliferative and invasive abilities, can also be enhanced by F. nucleatum.38,103 In the future, further clinical trials targeting the microbes within breast cancer should be designed and conducted, which may reduce breast cancer metastasis.
Additionally, the bacterial signals may promote cancer development by inhibiting local antitumor immunity.96 For example, F. nucleatum within the CRC is negatively associated with the density of CD3+ T-cell infiltrated in the TME, which relates to the downregulation of antitumor adaptive immunity.104 One thing to note, the bacteria that induce immunosuppression in the TME may actually be derived from the intestinal tract and the oral cavcity.52,105 The effects of intratumoral microorganisms on tumors are extremely complicated, and sometimes the same bacteria may not have identical impact on the same tumor. In colorectal cancer with low levels of microsatellite instability (MSI), F. nucleatum is positively correlated with tumor-infiltrating lymphocytes.106 Therefore, a bold conclusion can be drawn that other host factors besides the level of MSI may also influence the role of microorganisms within the TME, but more research is needed.
The effects of bacteria on the TME can be realized specifically through their OMVs or metabolites. OMVs constitute a crucial microbial delivery system that allows microbes to transfer their virulence factors, proteins and genetic materials in the systemic circulation. More importantly, microbe-derived cargos within OMVs can adversely reshape the TME. For example, OMVs released by H. pylori harbor active CagA that activates TLR and NF-κB pathways in gastric cells, which reinforces the inflammation and cell proliferation associated with carcinogenesis.107,108 In addition, certain microbial metabolites may be involved in the formation of the TME. DCA is a secondary bile acid produced by gut microorganisms after metabolizing primary bile acids. Song et al. suggested that DCA could facilitate vasculogenic mimicry and epithelial-mesenchymal transition (EMT) through activating vascular endothelial growth factor receptor 2, which is critical for the malignant transformation of intestinal epithelium.109
Other types of microbes such as fungal have also been found in the TME. For example, Malassezia species has been discovered in pancreatic ductal adenocarcinoma, and the glycans on its cell wall can bind to mannose-binding lectins to activate the complement cascade, which promotes tumor progression.41 Additionally, Dohlman and colleagues have confirmed the presence of Candida species in gastrointestinal tumors, which may correlate with worse survival outcomes, pro-inflammatory gene expression, and metastasis in cancer patients.34 Notably, relationship between fungal and bacterial communities within the TME is generally peace rather than competition;33 however, whether this harmonious relationship means a synergistic cancer-promoting effect remains unclear.
Mechanisms of microbes in tumorigenesis
Cancer-promoting bacteria may participate in the process of oncogenesis through a variety of different molecular pathways, and four main mechanisms are summarized here (Fig. 2): (1) DNA damage and epigenetics alterations; (2) interference with the DNA damage response (DDR) (3) abnormal signaling pathways; and (4) immune suppression.

Mechanisms of microbial tumorigenesis and tumor suppression. a Mechanisms of microbes instigating tumorigenesis and tumor suppression in the gut: (1) mucosal dysregulations: For example, the virulence factor CagA secreted by H. pylori can inject into the mucosal cells via T4SS with the combination of CEACAM and HopQ, thereby promoting cell proliferation and improve the transformation rate of tumor cells. (2) aberrant signals transduction: For example, Fap2 extracted from F. nucleatum can mediate tumor progression via binding to the Gal-GalNAc, and OMVs from F. nucleatum can also stimulate colonic epithelial cells producing TNF and trigger IL-8 signaling; FadA, another pathogenic factor from F. nucleatum, can interact with E-cadherin on the epithelial cells and activate NF-κB pathway via Wnt/β-Catenin signaling, resulting in tumorigenesis. (3) DNA damage and induced genetics/epigenetics alteration: e.g. T3SS of Salmonella enterica can bind the effector protein AvrA and cyclomodulin-like protein typhoid toxin, promoting tumorigenesis genetically and epigenetically, through genotoxin-mediated mutagenesis. Specifically, AvrA promotes cell proliferation, differentiation and inhibits cell-cycle arrest via JAK/STAT, Wnt/β-catenin or acetyltransferase-targeted p53 pathway, collectively resulting in tumorigenesis. Escherichia coli can induce DNA damages via a secreted genotoxin, colibactin, which can break the DNA doublestrand and crosslinks. (4) immune suppression: For example, intratumoral microbes can reduce immunosurveillance effect via PRR ligation with larger proportions of Tregs and lower ratio of TILs, e.g. CD8 + T lymph cells, thus inducing tumor proliferation and metastasis. b Mechanisms of microbes instigating tumorigenesis and tumor suppression in the TME: (1) Immunity boosting: For example, bacterial metabolites can elevate IFN-γ-producing CD8 + T cells, enhance the therapeutic effect of ICIs in mouse models, and SCFAs from gut bacteria can stimulate the formation of mucus from goblet cells, inhibit NF-κB activation, elicit inflammation signal and produce IL-18, promote the secretion of sIgA from B cells, thus boosting the immunity. (2) Metabolite regulation in anti-cancer activity: For example, SCFAs, such as butyrate, from commensal bacteria can induce the differentiation of macrophage and increase the antibacterial activity of macrophage, partly through inhibition of HDAC3 activity, which plays a role in glycolysis and autophagy, thus regulating the tumorigenesis and tumor suppression. (CagA the cytotoxin-associated gene A, T4SS the type 4 secretion system, CEACAM carcinoembryonic antigen-related cell adhesion molecules, Hop Q outer membrane adhesion, OMVs outer membrane vesicles, TNF tumor necrosis factor, IL-8 interleukin-8, Treg regulatory T cell, TILs tumor infiltrating lymphocytes, TME tumor microenvironment, IFN- γ interferon γ, T3SS the type 3 secretion system, PRR pattern recognition receptor, ICIs immune checkpoint inhibitors, sIgA secretory IgA, SCFAs short-chain fatty acids, HDAC histone deacetylase)
Inducing DNA damage and epigenetics alterations
In essence, cancer is nothing other than a disease of genes. Thus, if a microbe is involved in cancer initiation, it would probably give rise to genetic mutations represented by DNA damage in normal cells.110 A range of bacteria have the ability to induce DNA damage in host cells either directly through the effects of genotoxins or indirectly by activating cell-autonomous responses, which may be involved in the cancer initiation.
In a recent study, scholars from Yale University have found that bacterial strains isolated from patients with inflammatory bowel disease (IBD) exhibited DNA-damaging activities associated with malignant transformation from IBD to colon cancer.111 More importantly, a previously unexplored family of genotoxic small molecules termed the indolimines generated by Morganella morganii was discovered, which could increase the intestinal permeability and exacerbate colon tumorigenesis in gnotobiotic mice.111 Similarly, colibactin, a genotoxin expressed by pks+ E. coli, was also shown to induce DNA damage in colonic epithelial cells and correlate with faster cancer onset in patients with familial adenomatous polyposis, a precancerous stage for colon cancer.12 Mechanistically, colibactin can lead to alkylation and interstrand crosslinks after binding to DNA, which interfere with DNA replication and transcription, resulting in DNA double-strand breaks.112 Intriguingly, colibactin has also been detected in Klebsiella pneumoniae, Enterobacter aerogenes and Citrobacter koseri isolates,113 which implies possible carcinogenic effects of these bacteria. Other major genotoxin-producing bacteria include H. pylori,114 Bacteroides fragilis,115 Salmonella enterica,116 etc.
In addition to the direct effects induced by genotoxins, DNA damage can also be indirectly induced by infected cell-autonomous mechanisms in response to the presence of bacterial pathogens or their byproducts. Free radicals, such as reactive oxygen species (ROS), can be produced by infected host cells, and are also important DNA damaging agents because they can result in the base oxidation as well as the production of abasic sites (known as so-called AP sites) and DNA strand breaks. Pathogens including Chlamydia trachomatis,117,118 B. fragilis119 and H. pylori120 can trigger the production of ROS in infected cells, and the corresponding mechanisms have been thoroughly investigated. For example, similar to the H. pylori-secreted CagA described above, B. fragilis toxin can also upregulate SMO and result in SMO-dependent production of ROS, which induces DNA damage.119 More importantly, animal experiments corroborated that inhibiting SMO could significantly reduce ETBF-induced colon tumorigenesis, suggesting the vital role of this pathway in tumorigenesis.119
Apart from the production of ROS, other cell-autonomous responses inducing DNA damage can also be elicited by the bacteria. For example, H. pylori can induce DNA double-strand breaks (DSBs) after adhering to host cells, through binding the bacterial type IV secretion system to host cell integrin β1 and subsequent activation of NF-κB (nuclear factor-κB) signaling.121 Subsequently, DSBs are induced by the nucleotide excision repair endonucleases XPF and XPG, which are recruited to chromatin together with the NF-κB p65 subunit.121
Additionally, microbes may be involved in cancer development via epigenetic mechanisms. Epigenetic alterations mainly encompass the methylation of DNA, the posttranslational modification of histones, chromatin remodeling and regulation by noncoding RNAs, of which the methylation of DNA is the most well-explored. CRC development is closely linked with hypermethylation, which can slience tumor suppressor gene.122 Recently, Xia and colleagues found that the Hungatella hathewayi and F. nucleatum enriched in CRC were significantly associated with CDX2 and MLH1 (both are antioncogenes) promoter hypermethylation, respectively, through which the bacteria may drive intestinal tumorigenesis.123 Mechanistically, in vitro and in vivo experiments have demonstrated that both bacteria could upregulate DNA methyltransferase, which is required for hypermethylation.123
Interference with the DNA damage response (DDR)
The human genome constantly suffers from damage caused by exogenous factors including pathogenic microbes and endogenous genotoxic stress from cellular physiological processes such as DNA replication stress.124,125 Thus, human cells have evolved elaborate mechanisms, collectively termed the DNA damage response (DDR),126 to identify detrimental DNA mutations and repair impaired DNA sites, the normal outcomes of which include apoptosis as well as transient cell cycle arrest promoting DNA repair or cellular senescence.124 However, microbes not only induce DNA damage but also interfere with the DDR to hinder the repair of damaged DNA, both of which promote the passage of detrimental mutations to their progeny cells and may be associated with oncogenesis. When DSBs occur, DDR is initiated by the MRN complex, which is composed of MRE11, RAD50 and NBS1.127 Subsequently, ataxia-telangiectasia mutated kinase (ATM) is recruited and activated by the MRN complex, phosphorylating downstream proteins and subunits of the protein complex, which plays a pivotal role in the repair of damaged DNA.127,128,129
C. trachomatis, a pathogen associated with cervical and ovarian cancer, contributes to DNA damage by inducing the production of ROS as discussed above.117,118 More importantly, it can interfere with the DDR in infected host cells. Specifically, C. trachomatis inhibits the activation and recruitment of MRE11, ATM and 53BP1(p53-binding protein 1, a key player in orchestrating the choice of DNA repair pathway) at impaired DNA sites, as well as the activation of CHK1- and CHK2-mediated cell-cycle checkpoints, both of which may predispose host cells to malignant transformation.118 Likewise, H. pylori is a representative microbe that not only induces DSBs but also interferes with various DDR pathways. For example, H. pylori can elicit decreased expression of MutS and MutL at the protein level,130 both of which are components of the DNA mismatch repair system, and the aberrant upregulated expression of AID (activation-induced cytidine deaminase)131 associated with a high frequency of TP53 mutation. Consequently, the combination of these two effects of H. pylori may lead to higher point mutation rates and increased risk of carcinogenesis.
Additionally, H. pylori suppresses homologous recombination (HR), an error-free DNA damage repair pathway, while promoting non‑homologous end‑joining (NHEJ), an error-prone pathway, both of which are for DSBs.132,133 Specifically, Hp infection can inhibit the expression of MRE11 and downstream proteins RAD54 and RAD51, all of which are responsible for the regulation of HR, and it can facilitate the recruitment of 53BP1, which drives NHEJ.133,134,135,136 NHEJ is one of the major pathways for DSB repair, and plays a significant role in the maintenance of genome integrity via template-independent repair throughout the entire cell cycle. However, compared with HR, NHEJ induces chromosomal and genomic instability, especially in the context of defects in other DSB repair pathways, and an overactive NHEJ pathway may be associated with the development of malignancies.137,138 Thus, one of the Hp-carcinogenic mechanisms may be the inhibition of HR and the promotion of NHEJ.
The p53 protein is an important regulator of the DDR, promoting either the apoptosis or repair of damaged cells and is kept at a low level under unstressed states via the proteasome instructed by the E3 ubiquitin ligase MDM2.139 Normally, if DNA damage occurs, p53 will be phosphorylated to drive follow-up responses, such as cell cycle arrest.140,141 However, Hassin et al. found that H. pylori can induce the degradation of p53 to interfere with the DDR process.142 Specifically, Hp-secreted CagA interacts with apoptosis-stimulating protein of p53 (ASPP2), a protein activating p53 following DNA damage and consequently triggering apoptosis, and relocates it to an area near the plasma membrane, which confines p53 to the cytoplasm and consequently results in the MDM2-mediated proteasome-involved degradation of p53.143 More importantly, the degradation of p53 would increase the resistance of infected cells to apoptosis, thereby enhancing the colonization of Hp and predisposing these epithelial cells to cancerous transformation.143
Triggering aberrant signaling pathways
In addition to accelerating carcinogenesis by interfering with DDR pathways, microbes can also adversely impact other signaling pathways to promote cancer. Wnt/β-catenin signaling is a vital and highly conserved pathway controlling numerous biological processes, such as cell fate determination during embryonic development.144 However, aberrant activation of Wnt signaling has been demonstrated to be closely linked to many biological processes of cancers, including initiation and progression.145,146 Sufficient evidence has shown that bacteria can modulate the Wnt pathway, thereby triggering malignant transformation. Fusobacterium adhesin A (FadA) is a virulence factor generated by generated by F. nucleatum, and it can modulate E-cadherin/β-catenin signaling to promote colorectal carcinogenesis.88 Specifically, FadA binds to E-cadherin on the membrane, leading to the phosphorylation and internalization of E-cadherin, which is accompanied by increased β-catenin release and translocation into the nucleus due to the degradation of the E-cadherin/β-catenin complex, resulting in the aberrant activation of Wnt signaling associated with various cancers.88,147 Similarly, a virulence factor termed BFT secreted by ETBF can also activate Wnt signaling by cleaving E-cadherin.148,149
MAPK (mitogen-activated protein kinases) belongs to the family of serine-threonine kinases, which may be activated to promote carcinogenesis by certain bacteria. There are three kinds of crucial kinases in the MAPK family: extracellular signal-regulated kinase (ERK), JUN N-terminal kinase (JNK) and the stress-activated protein kinase p38 MAPK.150 Hp-derived CagA can trigger the ERK signaling cascade through interaction with growth factor receptor-bound protein 2 (GRB2), thereby activating T cell factor (TCF).151 Subsequently, TCF promotes the expression of induced myeloid leukemia cell differentiation protein 1 (MCL1), which may prevent the apoptosis of gastric epithelial cells.151 In addition, Salmonella Typhi, one of the risk factors for gallbladder carcinoma,152 can also activate the MAPK pathway and AKT pathway, which may accelerate the transformation of cells with silent p53 and overactive MYC.153,154
Eliciting immunosuppressive effects
The human immune system has a function termed immunosurveillance, whereby aberrant cells can be recognized and eliminated. Therefore, cancer cells must escape from detection and killing by the immune system for the tumorigenesis.
Recent studies have corroborated that bacteria can protect cancer cells from immunosurveillance, which may be linked to the development of cancer. For example, F. nucleatum can inhibit the attack of natural killer (NK) cells on tumor cells by binding TIGIT, an inhibitory receptor on human NK cells and various T cells, via the fusobacterial Fap2 protein.155 Additionally, gut microbes promotes pancreatic ductal adenocarcinoma by decreasing the intratumoral infiltration and activity of NK cells.42 Furthermore, F. nucleatum can selectively recruit tumor-infiltrating myeloid-derived suppressor cells (MDSCs), which may promote intestinal tumorigenesis by suppressing the immune response.156,157 More importantly, MDSCs may contribute to the formation of premetastatic niches158,159 and metastases by infiltrating primary tumors.160,161 Therefore, based on the above findings, we can conclude that F. nucleatum may indirectly facilitate metastasis by promoting the accumulation of MDSCs.162
Likewise, gut gram-negative bacteria/lipopolysaccharide direct hepatocytes to recruit MDSCs in liver in the context of benign liver disease or colitis that disrupts intestinal barrier, and thus promoting liver cancer by forming an immunosuppressive microenvironment.163 H. pylori also helps precancerous cells escape from immunosurveillance in the process of malignant transformation. For example, H. pylori can induce the expression of programmed death ligand 1 on gastric epithelial cells via the Sonic Hedgehog signaling pathway, whereby Hp-infected cells may escape immunosurveillance and progress to gastric cancer cells.164
Gut microbiota-derived metabolites also suppress anticancer immunity. Hezaveh et al. found that indole compounds, tryptophan metabolites produced by Lactobacillus, can activate the aryl hydrocarbon receptor in tumor-associated macrophages, which inhibits the intratumoral infiltration of TNFα + IFNγ + and CD8 + T cells in the pancreatic ductal adenocarcinoma and correlates with rapid disease progression and mortality.165
In addition to bacteria, pathogenic fungi also adversely regulate immunosurveillance. Rieber and colleagues have found that Aspergillus fumigatus and Candida albicans can induce MDSCs through the PRR Dectin-1 and its downstream adaptor protein CARD9, which functionally suppress T and NK cell responses.166
In the process of carcinogenesis, escape from immunosurveillance is an essential link. Ample evidence has substantiated that factors besides mutated cells themselves, such as the microbes discussed in this article, also suppress immunosurveillance against abnormal cells and contribute to malignant transformation.
Mechanisms of microbes in tumor suppression
Microorganisms not only promote cancer, but also inhibit its occurrence and progression through the following two mechanisms: direct killing effects on tumor cells and positive immunoregulatory effects.
Direct tumor-suppressive effects
As discussed above, bacterial genotoxins can initiate and promote cancer. However, some bacterial toxins also exhibit targeting property against cancer cells and thus may serve as underlying anticancer agents.167 Clostridium perfringens enterotoxin (CPE) is the virulence factor that causes the symptoms of C. perfringens type A food poisoning,168 while it also fights cancer cells by binding to transmembrane tight junction proteins claudin-3 and −4 that are highly expressed in human cancers, including breast,169 prostate170 and colon cancer.171 Mechanistically, the interaction between CPE and claudins triggers the formation of pore complex in the plasma membrane, resulting in the loss of osmotic equilibrium between intracellular and extracellular fluids and cell death.172 Other bacteria that have been identified as direct antitumor microbe include Pseudomonas aeruginosa, Salmonella typhimurium and Clostridium difficile, all of which generate toxins that display anticancer activity.173,174,175,176 Therefore, future chemotherapy agents may be developed from the toxins extracted from these microorganisms or their attenuated derivatives. Because bacterial toxins are generally toxic to normal cells, modification of the virulence factors with genetic engineering techniques is needed to overcome systematic toxicity in most cases.
Positive immunoregulatory effects
Some microbes can prevent and suppress cancer via immune mechanisms. On the one hand, normal gut microbiota is critical for the development of host immune system, and its absence would result in the structural and functional disability of the immune system,7 which may be associated with cancer initiation. For example, gut microbiota can promote the maturation of lymphoid organs and the differentiation of immune cells, which reflect the effects of microorganisms on the structure and function of immune system, respectively.177 Lymphoid tissue is divided into the central lymphoid organs and the peripheral organs. The central lymphoid organs are the sites in which B- and T-lymphocytes are generated, including bone marrow and thymus, while the peripheral lymphoid organs are the structures where mature lymphocytes are activated by antigen to provoke immune responses, including lymph nodes, spleen and gut-associated lymphoid tissue (GALT). The gut microbiota is of great significance to both of these lymphoid organs, which has been confirmed by the both early and recent research.
In 1956, Miyakawa and colleagues observed undeveloped and even atrophic lymphoid tissues in germ-free guinea pigs, including defects in Peyer ‘s patches, lymph nodes, and subepithelial lymphoid tissues.178 Recently, Zhang et al. reported the specific mechanisms of gut-microbiota-mediated peripheral lymphatic development.179 They demonstrated that, driven by the commensal fungi, CD45 + CD103 + RALDH + dendritic cells (DCs) in the gut move to peripheral lymph nodes and subsequently initiate their development via retinoic acid signaling, which is marked by the lymph node cellularity increase and volume expansion.179 More importantly, the structural and functional maintenance of the peripheral immune organs are permanently dependent on the DCs-introduced retinoic acid signaling.179 Gut microbiota is also essential for the development of GALT that enhances intestinal homeostasis. For example, peptidoglycan from gut gram-negative bacteria can be recognized by the NOD1 receptor in epithelial cells, which induces the expression of downstream β-defensin 3 and CCL20, and subsequently they can activate the chemokine receptor CCR6 and induce the genesis of isolated lymphoid follicles, a kind of GALT favorable for the maintenance of intestinal homeostasis.180 Additionally, gut microbiota also influences intestinal homeostasis by controlling the development of thymic components. 5-OP-RU is a vitamin B2 precursor derivative produced by the gut bacteria, but not by human cells, and it can move from mucosal surface to the thymus and promote the thymic development of mucosal-associated invariant T cells, an evolutionarily conserved subpopulation of T cells that mainly exists in the mucosae, thereby enhancing mucosal homeostasis.181 Thus, the commensal bacteria can promote the resistance of intestinal mucosa to pathogens via immune mechanisms, and thus decrease the risk of certain types of cancer such as CRC.182 Moreover, lymphoid organs are the nests of immune cells as described above, thus microbiota-induced lymphatic development and maturation are important for cancer prevention.
Based on the cancer-preventing effects of the gut microbiota, concrete strains have been found to tentatively treat cancer by enhancing anticancer immunity. Recently, a consortium of 11 bacterial strains isolated from healthy human donor feces displayed capability of inducing interferon-γ-producing CD8 + T cells in the intestine, and it can enhance the efficacy of immune checkpoint inhibitor in tumor-bearing mouse models, which both imply the potential of microbes for cancer therapy.183
Cancer-related microorganisms and effectors
Typical cancer-promoting microbes
Helicobacter pylori
H. pylori is a gram-negative, spiral-shaped bacterium residing in or underneath the mucus layer that coats the epithelial surface of the human stomach, and it is the most important biological risk factor for gastric cancer,184 which has already been classified as Class I carcinogen by WHO in 1994. In China, more than 70% of non-cardia gastric cancer and more than 60% of cardia gastric cancer can be attributed to H. pylori infection.185 The stomach is the harshest environment in the human body, secreting gastric juice that contains hydrochloric acid and proteolytic enzymes, which defends against the majority of pathogenic microbes.186 Thus, H. pylori has evolved intricate mechanisms to tolerate the acidic environment for the survival and colonization in the stomach. For example, H. pylori produces urease, an enzyme converting urea to ammonia, and it neutralizes gastric acid and provides ammonia for bacterial protein synthesis, which contributes to the H. pylori-mediated gastropathy.187 Additionally, H. pylori-induced gastric carcinogenesis is mainly mediated by CagA and vacuolating cytotoxin (VacA).188,189 These virulence factors can be injected into the epithelial cell via the type IV secretory system,190 then triggering a variety of carcinogenic mechanisms that are discussed in the previous chapter. Notably, the association between H. pylori and an increased risk of other malignancies besides gastric cancer have also been observed, such as CRC191 and gastric MALT lymphoma.192
Fusobacterium nucleatum
F. nucleatum is a gram negative, anaerobic oral commensal that has long been regarded as opportunistic pathogen of periodontal disease.193 Recently, ample evidence has found the presence of F. nucleatum in colon cancer tissue,194,195 and it has emerged as a causal bacteria implicated in CRC.88 Komiya and colleagues have collected CRC and saliva samples from 14 patients, and identical F. nucleatum strains were detected in both CRC and saliva from 6 patients, which implies that F. nucleatum in CRC may originate in the oral cavity.196 However, F. nucleatum is less prevalent in the healthy gut, introducing a question about how it migrates to and colonizes the developing TME. Abed et al. injected F. nucleatum into the veins of tumor-bearing mice and found that it could reach the tumor tissue, concluding that F. nucleatum might migrate to CRC through hematogenous route.197 Furthermore, Fap2 surface protein, a galactose-binding lectin expressed by some F. nucleatum strains, could mediate fusobacterial enrichment in CRC through binding to the Gal-GalNAc, a polysaccharide overexpressed in human CRC.197 Another key virulence factor of F. nucleatum is FadA adhesin, which promote colorectal carcinogenesis through multiple mechanisms, such as triggering β-catenin signaling.88,198 Notably, other bacteria of Fusobacterium species may be involved in the development of precancerous stage of CRC, ulcerative colitis.199 From the clinical point of view, F. nucleatum in the gut may be a target for CRC prevention and therapy in the future, just like eradication of H. pylori for gastric cancer.
Bacteroides fragilis
B. fragilis is part of the normal microbiota in the human colon and has important physiological meanings, such as promoting the development of host immune system.200 However, ETBF, a pathogenic strain of B. fragilis, has been demonstrated to be correlated with tumorigenesis of colon.201 The key virulence factor of ETBF is an enterotoxin termed fragilysin, which is essentially a zinc-dependent metalloprotease. Chung et al. have demonstrated that fragilysin could trigger pro-carcinogenic inflammatory cascade to accelerate colon tumorigenesis.202 Specifically, fragilysin triggers an IL-17 immune response that selectively activates NF-κB signaling in distal colonic epithelial cells, which collectively lead to pro-tumoral myeloid cells infiltration in distal colon.202 Additionally, Cao and colleagues have found that ETBF could promote intestinal inflammation and CRC development by down-regulating exosomal miR149-3p secreted by CRC cells,203 a miRNA inhibiting tumorigenesis in other cancers.204
Epstein-Barr Virus
Besides bacteria, viruses can also promote the development of cancer, and a typical representative is Epstein-Barr Virus (EBV). EBV is one of the eight known human herpesviruses and the first cancer-associated virus, and EBV infection may lead to malignancies including lymphoma, gastric cancer and nasopharyngeal carcinoma.205 EBV can exert carcinogenic effect through its protein components. For example, viral protein BNRF1 can induce centrosome amplification in B-lymphocytes, which is associated with chromosomal instability, and thus increase the risk of malignant transformation.206 On the other hand, EBV could promote tumor immune escape in gastric cancer and nasopharyngeal carcinoma. Specifically, EBV miRNAs BART11 and BART173p could inhibit FOXP1 and PBRM1, respectively, thereby enhancing the transcription of PD-L1 that is crucial for tumor immune escape.207 Additionally, EBV infection could inhibit the antitumor function of NK cells infiltrated in the EBV-associated epithelial malignancies, and thus promoting the cancer development.208
Cancer-inhibiting bacteria
Lactobacillus
Lactobacillus spp. are commonly used as food supplements, and their role in protecting against cancer was investigated initially in mice. The alleviating effects of Lactobacillus rhamnosus, Lactobacillus acidophilus and Lactobacillus fermentum on the development of colon cancer have been demonstrated in the mouse model.209 L. rhamnosus GG can stimulate type I interferon through the cGAS/STING signal transduction pathway, thereby improving the response to ICIs.210 Lactic acid bacteria (LAB) can effectively decrease the occurrence of CRC, which might be ascribed to the reduction of inflammatory factors. Moreover, LAB also affects the gut microbial community, which is marked by the decrease of the abundance of Bacteroides.209 Therefore, LAB is beneficial to inhibit the initiation and development of cancer.211 L. reuteri can promote the renewal and repair of intestinal epithelium and stimulate the host’s immunity.212 Specifically, L. reuteri was found to convert intraepithelial CD4 + T cells into CD4 + CD8αα + double-positive intraepithelial lymphocytes that relieve inflammatory bowel disease, thus preventing some alimentary tract cancer.213
Bifidobacterium
Existing evidence have found that Bifidobacterium species might have important cancer-inhibiting effects. For example, the tumor control effect of oral administration of Bifidobacterium in melanoma mice was demonstrated to be the same as that of PD-L1 antibody,214 and the combination of these two methods is highly effective in inhibiting tumor outgrowth.214 In mice fed with western style diet (WSD), an reshaped colonic microbiota composition might cause increased penetrability and reduced formation of mucus layer in the gut. However, it has been demonstrated that Bifidobacterium longum could regain mucus secretion in WSD-fed mice,215 which implies the potentially significance of Bifidobacterium species in the maintenance of intestinal homeostasis. β-glucan/galactan polysaccharides on the cell surface of Bifidobacterium bifidum were demonstrated to be crucial for the induction of Foxp3+ T regulatory cells that display suppressive capacity to experimental colitis.216 Thus, it is not surprsing that B. bifidum can regulate intestinal homestasis and prevent cancer initiation.216 The findings above emphasize the potential of Bifidobacterium in cancer treatment or prevention by affecting immune control and mucosal protection.
Faecalibaculum rodentium
F. rodentium and Holdemanella biformis (human homolog) are absent or lost in the course of tumorigenesis,217 both of which can produce SCFAs that control the proliferation of tumor cells and protein acetylation through the suppression of calcineurin and NFATc3 activation.217 Adenomatous polyposis coli (APC) gene mutations occur in more than 80% of CRCs when F. rodentium is applied to ApcMin/+ mice, or tumor growth in mice can be mitigated by treatment with azoxymethane and dextran sodium sulfate. Likewise, H. biformis appears to be similar to F. rodentium in suppressing tumor growth in the ApcMin/+ model by means of butyrate. Therefore, H. biformis may be applied in the design of cancer treatments.
Streptococcus thermophiles
S. thermophilus is a powerful probiotic with digestive and immune benefits, and it is normally depleted in CRC patients.218 More importantly, the inhibitory effect of S. thermophilus on tumorigenesis has been demonstrated in CRC mouse models.218 Specifically, oral gavage of S. thermophilus in CRC mosue would result in a significant reduction in tumor formation, and β-galactosidase secreted by S. thermophiles was found to be the active ingredient that inhibits CRC growth, which was confirmed by in vivo xenograft experiments and cell experiments218 In mouse CRC xenograft experiments, β-galactosidase was found to inhibit cell proliferation, cell colony formation and cell cycle arrest to promote CRC cell apoptosis, thus suppressing tumor growth.218 Impressively, β-galactosidase can increase the richness of another two probiotics, Lactobacillus and Bifidobacterium, suggesting a synergistic effect.218 S. thermophilus can also affect tumor growth by releasing folate,219 a major dietary element that plays an important role in cell metabolism and DNA replication, repair, methylation, and nucleotide synthesis. Research suggests that folate deficiency is fairly prevalent in humans,220 and the folate released by S. thermophilus might be involved in tumor suppression. In addition, S. thermophilus has an effect on the lymphocyte profile, the severity of colitis, and the regulatory T-cell response.221
Cooperative and competitive relationship among microbes in cancer development
Symbiotic, antagonistic and neutral relationships among the gut microbes exist, the former two of which may be involved in the carcinogenic mechanisms of microbes. It is well known that F. nucleatum is an oral-derived bacteria closely associated with the occurrence and progression of CRC.38,196 Thus, if F. nucleatum grows well in the oral cavity, it may be beneficial to its migration to CRC. Sakanaka et al. have discovered cooperative relationship between F. nucleatum and Streptococcus gordonii, another symbiotic bacteria colonized on the surface of human oral mucosa.222 Specifically, S. gordonii could secret ornithine, which in turn support the growth and biofilm development of F. nucleatum in oral cavity.222 Although the direct impact of this cooperation on the development and progression of CRC has not been confirmed, it is likely to promote the colonization of F. nucleatum in the cancer foci by enhancing its viability, which is linked to the development of CRC.
Additionally, carcinogenic microbes can be antagonized by some probiotic. For example, B. bifidum strain BF-1 can suppress the expression of Hp-induced genes in human cells, most of which are related to the NF-κB signaling pathways.223 Because Hp-induced NF-κB signaling can promote the malignant transformation via regulating chronic inflammation,224 BF-1 can protect host cells from carcinogenesis.
Effects of metabolites in cancer development
SCFAs/DCA
SCFAs, including propionic acid, butyrate and tryptophan, play a key role in a variety of host biochemical and physiological functions, e.g., maintaining intestinal barrier integrity and intestinal motility, as well as regulating immunological function and the gut-brain axis.225,226 Butyrate is one of the most widely studied SCFAs, which is produced through fermentation of dietary fibers by gut microbes. It can not only serve as an energy source for normal colonocytes, but also reduce the risk of CRC.227 It is well known that the destruction of intestinal mucosal barrier acts as an accomplice in the occurrence of CRC, while butyrate can repair and enhance the function of the gut barrier.228 Peng et al. demonstrated that one of the specific mechanisms by which butyrate enhances the intestinal barrier is to promote the assembly of tight junctions through activating AMP-Activated Protein Kinase.229 Additionally, butyrate also stimulates the expression of MUC2 in intestinal epithelial cells, which can enhance the mucous layer involved in the formation of intestinal barrier.230 On the other hand, butyrate can directly inhibit the proliferation of CRC cells by remodeling metabolism, which is manifested by the inhibition of Warburg effect and the enhancement of energy metabolism.231 Notably, β-hydroxybutyrate, a chemical substance structurally similar to the butyrate, also suppresses CRC by inducing the transcriptional regulator Hopx through the surface receptor Hcar2.232 What’s more, butyrate also inhibits other types of cancer. For example, sodium butyrate combined with cisplatin can enhance the apoptosis of gastric cancer cells through the mitochondrial apoptosis-related pathway, which might be an underlying strategy for gastric cancer.233
DCA, a secondary bile acid produced by gut microbes from primary bile acids through 7α-dehydroxylation, has an extensive range of effects on host metabolism and plays an important role in health.234 However, DCA may also play a key role in cancer development by mediating a variety of signaling pathways, including EGFR-MAPK and β-catenin signaling, and the p53 pathway.235 For example, obesity-induced increased DCA can provoke senescence-associated secretory phenotype in hepatic stellate cells through enterohepatic circulation, which in turn promotes the secretion of tumor-promoting factors and inflammatory factors associated with hepatocellular carcinoma.77 Furthermore, DCA also promotes CRC progression through antagonizing intestinal farnesoid X receptor.236 Besides, bioactive molecules generated from gut-bacteria-mediated bile acid metabolism may determine immune cells differentiation, which is crucial for tumor immunology.237 Taurine-conjugated bile acids, another metabolite of intestinal microbes, can produce hydrogen sulfide and DCA and promote the growth of CRC tumors.235 In addition, the bile acid pool in colon may influence FOXP3 + Treg cells, indicating a crucial role in immunity regulation.238 Interestingly, DCA may serve as a tumor suppressive factor in gallbladder cancer, which suggests an underlying strategy for the malignancy.239
Tryptophan and trimethylamine N-oxide (TMAO)
Tryptophan (Trp) is an essential amino acid that can be metabolized through the kynurenine pathway and microbial transformation, both of which are significant for host health. However, the two metabolic pathways of Trp are different in colon carcinogenesis, which may allow the immune escape of tumor cells. Colon cancer cells are more likely to absorb and process tryptophan than normal colonic epithelial cells.240 Specifically, the oncogene c-Myc can promote Trp absorption by upregulating Trp transporters SLC7A5 and SLC1A5 and accelerate Trp metabolism through increasing the level of related enzymes in the cytoplasm in colon cancer cells, both of which contribute to T cell inactivation and protein synthesis in the process of carcinogenesis.225 In addition, kynurenine, the intermediate product of Trp metabolism, can accelerate the progression of pancreatic cancer.241 Kynurenine also regulates immunity by promoting the nuclear translocation of AhR, which is an inflammatory and immune-related transcription factor.242 Moreover, Lactobacilli can convert tryptophan into indole-3-aldehyde that acts as an AhR agonist by increasing the expression of IL-22 and enhancing the activity of Th17 cells.243
TMAO is metabolized in the liver from trimethylamine (TMA) synthesized by host gut microbes,244 and it has been demonstrated to increase the risk of cardiovascular disease such as myocardial infarction and stroke.245,246 Omnivorous humans produce more TMAO than vegetarians,247 and its level is associated with the risk of cancer, including CRC.248 Furthermore, TMAO is capable of activating the PERK-mediated response and thus activating forkhead box protein O 1, which is crucial for metabolic regulation.244 Accordingly, the formation of TMA and TMAO can be the connections among diet, the gut microbiota and cancer. Gaining a better understanding of the role of TMAO in the pathogenesis of cancer will be favorable for cancer prevention and control.
Insulin resistance and inosine
In a Swedish study, the microbiota community of the pancreas in patients with impaired glucose tolerance (IGT) or type 2 diabetes mellitus (T2DM) was found to be altered.249 It is interesting to note that the abundance of butyrate-producing bacteria decreased in both prediabetic and T2DM patients.249,250 Insulin resistance has been found to be strongly related to microbial dysfunction.249 In a further study, gut bacteria associated with T2DM was found to impaire glucose tolerance and insulin signaling by producing a metabolite termed imidazole propionate from histidine,251 thus a relatively high concentration of imidazole propionate can be detected in T2DM patients.252,253 Insulin resistance has the potential to stimulate the growth of cancer via mTOR activation,253,254 partly because of imidazole propionate,251 and it leads to metabolic changes that promote cancer growth.249,255,256 Thus, it is possible that gut microbiota dysfunction that induces insulin resistance may contribute to tumor development.
Three bacteria, Bifidobacterium pseudolongum, Olsenella, and Lactobacillus johnsonii, have been shown to exert a positive effect on the effectiveness of immunosuppressors in mouse models due to the metabolite inosine.257. In fact, inosine is an immunotherapy-promoting metabolite and has been experimentally shown to have an effect on colon cancer, bladder cancer and melanoma.257 Mechanistically, inosine triggers the activation of Th1 cells by regulating T-cell-specific A2AR signaling. Thus, the development of inosine-based adjuvant therapies may enhance the efficacy of ICIs. In the future, a better understanding of the underlying mechanisms of inosine will be of great help to formulate proper ICI-based therapy strategies.
Niacin and vitamin B
Niacin acts as the precursor of nicotinamide dinucleotide (NAD) and NAD phosphate (NADP), both of which are involved in redox reactions. NAD also correlates transcriptional regulation with cellular energetics.258 Monosaccharides are produced in the fermentation of carbohydrates, which are further catabolized to produce pyruvate and NADH molecule.225 G protein-coupled receptor 109 A (GPR109A) acts as a receptor for both niacin and butyrate,259 through which niacin can inhibit the growth of colon cancer.260 Niacin also displays beneficial effects on colitis by prostaglandin D2 enhancement.261 Vitamin B contributes largely to the synthesis of DNA and protein, and it also plays a key role in the metabolism of ser-gly one-carbon.225 Gut bacteria can synthesize a group of B vitamins, including B1, B2, B3, B5, B6, B7, B9 and B12, which are essential for human health.225 More importantly, B vitamins will impact tumorigenesis through the SGOC pathway.262,263
Diacetyl spermine/oncotoxins
Bacterial biofilm, which contributes to the polyamine pool, plays a nonnegligible role in changing the TME.264 Polyamine metabolites are upregulated in the tissues of cancer patients.265,266 It is important that antibiotic therapy can clear the bacterial membrane, thus reducing the number of N(1),N(12)-diacetylspermine267 and polyamine metabolites that promote the growth cancer. Mechanistically, polyamine is associated with the proliferation of eukaryotes. Bacteria in Eggerthellaceae family have been found to produce urolithin,268 which is derived from polyphenols in some fruits with anti-inflammatory and antioxidative capabilities, and activate AhR to upregulate tight junction proteins,219 thus having antitumor activity. Moreover, the carcinogenic versions of the bacteria E. coli and B. fragilis may produce oncotoxins that accelerate carcinogenesis.12 Specifically, cytolethal-derived toxin from enteric pathogens (Escherichia and Bacillus spp.) and colibactin from Enterobacteriaceae are demonstrated to be tumorigenic due to their DNA damage effects.269 Thus, the modification of microbes and their products may be beneficial in the treatment of cancer since oncogenic toxins and metabolites produced by microbes can contribute to carcinogenesis.270
Targeting the gut microbiota in clinical cancer treatment
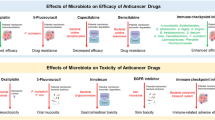
The gut microbiota can be regarded as a special organ, and its composition can be adjusted in various ways. More importantly, with the in-depth study on gut microbes in recent years, researchers have found a strong relationship between gut microorganisms and anticancer treatment efficacy,271,272,273 providing us with a new anticancer direction,274,275 which is to enhance efficacy and reduce therapeutic toxicity of conventional anti-cancer therapies by modulating the microbial composition in the gut,276 although we are still far from a full-fledged microbial anticancer treatment.277,278,279 The relationships between gut microbes and anti-cancer treatment and the current as well as emerging microbial interventions for cancer therapy are summarized here (Fig. 3).

The mechanisms of microbiota impacting efficacy of cancer treatment. a Specifically, administration of Enterococcus and Barnesiella can restore the antitumor efficacy of cyclophosphamide-based chemotherapy through stimulating tumor-specific T cells and producing IFN-γ, and butyrate, a product of dietary fiber fermented by gut microbes, can increase the anticancer effects of oxaliplatin-based chemotherapy by regulating the function of CD8 + T cells in the TME through IL-12 signaling; b Lactobacillus rhamnosus was illustrated to stimulate the antitumor activity of PD-1 immunotherapy through cGAS-STING signal pathway, activating IFN-α, β signaling, and activating cytotoxic CD8 + T cells; SCFAs limit the antitumor effects of CTLA-4 blockade via alleviating Treg cells, and higher concentration of butyrate could decrease the anticancer activity of Ipilimumab by inhibiting the accumulation of related CD4 + T cells; c probiotics can protect gut mucosa from radiation injury through a TLR-2/COX-2-dependent manner, stimulating mesenchymal stem cells to the crypt. (FMT fecal microbiome transplantation, SCFAs short-chain fatty acids, IL interleukin, IFN- γ interferon γ, CTLA-4 cytotoxic T lymphocyte-associated antigen 4, Treg cell regulatory T cell, TLR Toll-like receptor, COX-2 cyclo-oxygenase-2)
Gut microbiota and cancer therapy efficacy
An emerging role: The microbiota affecting immunotherapy
Cancer immunotherapy, as one of the revolutionary advances in the last ten years, mainly includes immune checkpoint therapy, typified by cytotoxic CTLA-4 and PD1, and adoptive T-cell therapy (ACT), represented by chimeric antigen receptor T-cell (CAR-T) therapy as well as cancer vaccines,280 and it has occupied an increasingly important position in the comprehensive treatment of cancer.281,282,283,284,285,286,287,288,289,290,291,292 To date, immunotherapy has improved treatment outcomes for many cancer patients, but there are still a large proportion of patients who receive immunotherapy with little benefit, showing primary or acquired resistance to treatment,293 including patients with melanoma,294 and patients with non-small cell lung cancer.295,296,297,298 Available evidence suggests that this discrepancy in efficacy may be linked with gut microbes.48,299,300,301,302,303,304
Among all immunotherapies, immune checkpoint inhibitors (ICIs) therapy is the most mature, and its main mechanism is upregulating the immune killing effect of T cells by targeting coinhibitory molecules including PD-1/ PD-L1, to boost the endogenous host immunity and prevent tumor cells from immune escape.305 Indeed, the response to ICIs seems to be predictable based on the gut microbial composition,47,306,307 because gut microbes can also be involved in the adjustment of host immunity, which may in turn indirectly affect the response of cancer patients to ICIs.47,306,308,309,310,311,312 For instance, active enterococci secretes SagA, an ortholog of the NlpC/p60 peptidoglycan hydrolase catalyzing the production of immune-active muropeptides, that can bind to NOD2, a key pattern recognition receptor, through which host immunity can be enhanced via multiple pathways and thus may ultimately augment anti–PD-L1 antitumor efficacy.313
L. rhamnosus was illustrated to stimulate the antitumor activity of PD-1 immunotherapy by triggering dendritic cells to produce IFN-α and IFN-β through the cGAS-STING signaling pathway.210 Bifidobacterium plays antitumor roles by inducing the maturation of dendritic cells, activating IFN-α and IFN-β signaling, and stimulating cytotoxic CD8 + T cells.214 In addition, vitamin B5, produced by intestinal bacteria and contained in most food, could promote the generation of IL-22-producing Tc22 cells, a kind of immune cell that has particularly efficient antitumor effects and correlates with stronger immunotherapy responses.314 As per these findings, novel therapeutic strategies based on microorganisms have been developed to modulate the gut microbiota to improve the clinical response to ICIs66,67,315 and to reduce therapeutic toxicity.316,317
However, due to the diversity within the gut microbiota, there are bound to be microbes that have the exact opposite effects on ICIs. For example, SCFAs limit the antitumor effects of CTLA-4 blockade,318 and high concentration of butyrate in cancer patients could decrease the anticancer activity of ipilimumab by inhibiting the accumulation of related T cells and IL-2 impregnation.318 It is well known that a large amount of the SCFAs in the human body comes from the fermentation of dietary fiber by intestinal bacteria. Therefore, some intestinal bacteria are actually able to indirectly inhibit the antitumor effect of CTLA-4 blockade by producing corresponding metabolites. From the findings of these studies, it is not difficult to understand the presence of reticular relationships among gut microbes, diet, human immunity and immune checkpoint inhibitors. First, diet and gut microbiota have effects on each other.319,320 Specifically, diet can influence the composition of gut microbiota, and gut microbes can participate in the digestion and absorption of nutrients. Secondly, healthy diet and balance gut microbiota are both essential for the maintenance of human immunity,321,322 which in turn defense against the invasion of pathogenic microbes and balance the gut microbiota.323 More importantly, as discussed above, gut microbes participate in the metabolism of nutrients, producing metabolites that affect the body’s immunity, ultimately impacting the effects of ICIs.
In addition to affecting the efficacy of ICIs, gut microbes also have an impact on ACT.324 To date, little research regarding the influence of gut microbes on ACT has been conducted, but such effect does exist.325 Depleting the gut microbes in tumor-bearing mice undergoing ACT with vancomycin slowed their tumor growth, whereas neomycin and metronidazole had no similar effect.326 Notably, relevant observational studies were conducted to confirm the impact of gut microbes on ACT. Smith M et al. retrospectively collected and analyzed clinical data from patients with acute lymphoblastic leukemia and patients with non-Hodgkin lymphoma, and they found that exposure to antibiotics, e.g. meropenem, piperacillin/tazobactam and imipenem/cilastatin, during the 4 weeks before CAR-T-cell therapy was associated with worse clinical outcomes and prognosis; furthermore, they found a higher abundance and richness of Ruminococcus, Bacteroides and Faecalibacterium in stool samples were correlated with a better response to CD19 CAR-T-cell therapy.327 Therefore, similar to the effects on immune checkpoint therapy, distinct gut microbial compositions do affect the efficacy of ACT, and the mechanisms behind these effects need to be further investigated.
Chemotherapy efficacy is closely linked to the gut microbial composition
Chemotherapy is one of the major treatments for cancer, but not all patients respond well to it. Taking patients with stage II and III gastric cancer as an example, postoperative adjuvant chemotherapy can significantly improve the five-year survival rate of this population, whereas there are still a considerable proportion of patients who do not benefit from chemotherapy.328 One reason for cancer patients respond differently to the identical chemotherapy drugs may be the differences in the composition of the gut microbiota among individuals. In other words, some microbes in the gut are involved in regulating the efficacy of chemotherapy,329,330 and this regulation includes both promoting and inhibitory effects.44,331,332,333
Gemcitabine is a commonly used chemotherapy agent for pancreatic ductal adenocarcinoma (PDAC). Gut microbes are involved in the pharmacokinetics of chemotherapy drugs, and the efficacy of gemcitabine for PDAC may be influenced by intestinal microorganisms.334 For instance, Gammaproteobacteria is able to metabolize gemcitabine and convert it to the inactive form, 2′,2′-difluorodeoxyuracil.43 Therefore, in the future, it may be possible to increase the anti-cancer effect of gemcitabine by combining antibiotics against Gammaproteobacteria with chemotherapy. In addition to the negative effects, however, a gut microbial metabolite, butyrate, can enhance the efficacy of gemcitabine against cancer cells by inducing apoptosis.335
Cyclophosphamide, another widely used immunostimulatory agent for chemotherapy, has been demonstrated to have mitigated antitumor efficacy in antibiotic-treated or germ-free mice due to a lack of Th1- and Th17- related immune responses. Interestingly, the administration of Enterococcus and Barnesiella can restore its antitumor efficacy through the stimulation of tumor-specific CD8 + and CD4 + T cells and Th1 and Th17 cells. In addition, erlotinib is a highly specific tyrosine kinase inhibitor that can reversibly inhibit epidermal growth factor receptor mutations and is mainly used for targeted therapy after the failure of chemotherapy for non-small cell lung cancer (NSCLC). Recently, gut microbes were found to be positively correlated with erlotinib treatment outcomes.336 Specifically, Bacteroides xylanisolvens and Bacteroides ovatus were positively correlated with the treatment outcomes of erlotinib, and oral administration of the bacteria could significantly enhance the efficacy of erlotinib and induce the expression of C-X-C motif ligand 9 (CXCL9) and IFN-γ in a murine lung cancer model.336 More importantly, the microbial signature that enhances the efficacy of erlotinib may also be used in the treatment of other cancers, as this signature is independent of cancer type.
The efficacy of oxaliplatin varies individually and it may be related to the presence of certain metabolites of gut microbes. For example, butyrate, a product of dietary fiber fermented by gut microbes, could increase the anticancer effects of oxaliplatin by regulating the function of CD8 + T cells in the TME through IL-12 signaling.337 Therefore, selected gut microbial metabolites may be used as adjuncts to oxaliplatin to enhance anticancer responses in the future. In addition, commensal microbes can also influence the cancer response to oxaliplatin by modulating the functions of myeloid-derived cells within the TME.338 Through related studies using cancer mouse models, it was found that tumor-infiltrating myeloid-derived cells responded poorly to cancer treatment under antibiotic treatment or sterile conditions, resulting in insufficient production of reactive oxygen species and cytotoxicity following chemotherapy, which ultimately led to a decline in the efficacy of oxaliplatin.338 Therefore, gut microbiota dysbiosis in cancer patients may be one of the reasons for resistance to chemotherapy drugs, and interventions targeting the gut microbiota could be a promising strategy to improve cancer chemotherapy efficacy.
Bidirectional relationships between the gut microbiota and radiotherapy
Radiation therapy (RT) is a long-established cancer therapy that has been used to treat most types of cancer for more than one hundred years. The basic principles of radiotherapy include two aspects: on the one hand, the DNA of cancer cells is destroyed by ionizing radiation directly to kill cancer cells; on the other hand, RT indirectly kills cancer cells by causing reactive oxygen species-dependent damage to DNA.339 However, RT not only kills cancer cells but also can cause varying degrees of adverse effects on normal tissues and commensal microorganisms in the body, especially those in the gut.339,340
A bidirectional relationship between RT and the gut microbiota exists.341 One of the adverse events of radiotherapy is gut microbiota dysbiosis, which is typically characterized by a relative decrease in the richness of favorable microbes, e.g., Bifidobacterium, and an increase in the relative richness of harmful microorganisms such as Fusobacteria and Proteobacteria,342 and these changes in the composition of gut microbiota in turn exacerbates radiation-related complications, such as radiation enteropathy.343,344 However, the presence of some commensal microbes is critical for improving the efficacy of radiotherapy and moderating RT-related adverse events.340 Working on mouse models of breast cancer, Shiao et al. found that depleting the gut bacteria with an antibiotic cocktail of ampicillin, imipenem, cilastatin, and vancomycin before radiotherapy resulted in faster tumor growth and shorter survival of tumor-bearing mice than RT alone, and a similar situation has been observed in mouse models of melanoma.345 However, what is thought-provoking is that when the tumor-bearing mice were administered the abovementioned antibiotic cocktail alone without receiving radiotherapy, their tumors grew more slowly than control group, which was somewhat paradoxical to previous experiments.345 In this regard, the depletion of gut microbes might cause changes in metabolism, which ultimately leads to a reduction in tumor-promoting metabolites such as serum glucose and SCFAs.345 In addition to bacteria, fungi have also been found to be associated with the response to radiation therapy, which suggests that other types of secondary microbes in the gut microbiota can also influence the efficacy of radiotherapy, although this effect may be negative.345 Accordingly, the relationship among gut microbes, tumors and radiotherapy is reticular, with a very broad research space.
Gut microbiota and therapy-related side effects
Conventional anticancer therapies have their own side effects, and even immunotherapy, which has been very popular in recent years, is no exception.346,347 It has been noted that the gut microbiome is associated with the toxicity of traditional anticancer therapies and that modulating the components of the gut microbiome may alleviate related toxicity.348 Therefore, understanding the relationship between different microbes and the side effects of traditional anticancer therapy is particularly important for individualized mitigation of these adverse events.
Immune checkpoint therapy can cause severe inflammatory side effects, and one of its most serious adverse events is colitis.349 Some researchers have found that in patients with severe ICI-related colitis, the abundance of Lactobacillus in the gut decreased obviously, and subsequent studies confirmed that the ICI-related colitis could be moderated via oral administration of this probiotic.350 Mechanistically, the ability of L. reuteri to inhibit ICI-related colitis is associated with a decrease in the distribution of group 3 innate lymphocytes.350 Moreover, the profiling of the gut microbiota in melanoma patients receiving combined PD-1 and CTLA-4 blockade suggested that a higher abundance of B. intestinalis was related to adverse events of immunotherapy.317 Similarly, the immunotoxicity of a novel immunotherapy drug, immune agonist antibodies (IAAs) targeting costimulatory molecules, is also linked to the gut microbiota.351 Specifically, germ-free and antibiotic-treated mice had fewer complications following treatment with the IAAs anti-CD40 and anti-CD137 than normal or microbial recolonized germ-free mice.351 Taken together, these findings indicate that gut microbiota signatures are clearly associated with the toxicity of ICIs, and the association could be a new breakthrough point for developing new therapeutic strategies in the future.
Chemotherapy, while saving cancer patients, also has many side effects, including intestinal flora imbalance, mucositis and diarrhea.352 For example, irinotecan, a common chemotherapy drug, can kill cancer cells, but it can also cause the death of normal epithelial cells and commensal microorganisms in the gut. Therefore, irinotecan tends to cause gastrointestinal toxic side effects and intestinal flora imbalance. The β-glucuronidase secreted by gut bacteria can prolong the clearance time of irinotecan in vivo, so gut microbes can exacerbate irinotecan-induced gastrointestinal toxicity.353 In addition, irinotecan-induced intestinal dysbiosis can exacerbate the gastrointestinal toxicity of irinotecan by damaging the intestinal mucosal barrier.354 Therefore, gut microbes are clearly involved in the mechanisms of irinotecan-related adverse events. Direct inhibition of β-glucuronidase may be able to reduce the gastrointestinal toxicity of irinotecan and improve patients’ quality of life.355 Moreover, the side effects of irinotecan can also be alleviated by taking certain probiotics, e.g. E. coli strain Nissle 1917, which could regulate gut barrier epithelial function, alleviate gut dysbiosis, and ultimately reduce intestinal complications caused by irinotecan.
RT not only kills cancer cell, but also causes varying degrees of adverse effects on normal tissues and disrupts the diversity and abundance of commensal gut microorganisms.340,356 The RT-induced dysbiotic gut microbiome in turn exacerbates the gastrointestinal toxicity of radiotherapy.340 Conversely, certain probiotics or probiotic preparations, such as L. rhamnosus and VSL#3 (a probiotic preparation composed of Bifidobacterium species, Lactobacillus, and Streptococcus) could protect the intestinal epithelium from injury and reduce the side effects of RT.357,358,359
Cancer surgery, especially surgical resection of gastrointestinal cancer with alimentary reconstruction, has many postoperative complications, the most common of which are surgical site infections and anastomotic leaks. Despite improvements in preoperative preparation, surgical techniques, and postoperative care over the years, anastomotic leaks and postoperative infections occasionally occur with serious consequences, including acute peritonitis and even death. To reduce the risk of these two complications after surgery, patients typically undergo preoperative bowel preparation to empty their colon of stool and take antibiotics to prevent infection. Clearly, these measures reduce the risk of postoperative complications by reducing the abundance of the relevant microbes in the patient’s gut. Metabolism following gastrectomy is related to microbial function alterations, such as the biosynthesis of organic compounds and nutrient transport.360 Related studies have confirmed that intestinal microbiota composition could predict short-term prognosis after gastrointestinal cancer surgery.361,362,363 For instance, low microbial diversity and mucin-degrading members of the Bacteroidaceae and Lachnospiraceae families are associated with postoperative anastomotic leaks.364,365 Surgical site infections are caused by various factors, such as drug-resistant and virulent microorganisms that have emerged as a result of globalization, antibiotic exposure, and the application of prolonged and invasive treatments.366 Curiously, is there some kind of commensal microorganism that can promote anastomosis healing and prevent surgical site infections? There is literature suggesting that some probiotics may be able to inhibit pathogenic microorganisms associated with postoperative infections. For example, some strains in Lactobacillus and Bifidobacterium are capable of inhibiting the growth of clinically isolated methicillin-resistant Staphylococcus aureus, a multidrug resistant microorganism that is a major nosocomial pathogen and relates to postoperative infections, by direct cell competitive exclusion as well as the production of inhibitors.367 In the future, it may not be impossible to develop microbial therapies to improve postoperative prognosis by targeting these related microorganisms.
Current and emerging microbial interventions/therapeutic strategies for cancer therapy
With a more comprehensive and in-depth understanding of the gut microbiome gained in recent years, an increasing number of potential microbial interventions for cancer therapy have been proposed,368 including FMT, treatment with prebiotics, probiotics or antibiotics, and dietary interventions, which have already illustrated great prospect of microbial therapies. In the future, some microbial strategies mentioned above may be translated to widely-accepted anti-cancer interventions.
Fecal microbial transplantation (FMT) applications in clinical medicine
FMT refers to the transplantation of the functional flora of healthy donors into the intestinal tract of recipients for the purpose of treating diseases, and it was first used to treat severe diarrhea more than 1600 years ago during the Eastern Jin Dynasty in ancient China, when Chinese doctors issued a prescription called “Huanglong soup”.369 The recipients mentioned above can not only refer to patients with diarrhea, but cancer patients. The transplantation of fecal microbes from patients with a complete response to ICIs into immunotherapy-refractory melanoma patients could reduce the tolerance to ICIs.66,67 Following FMT, the abundance of favorable microorganisms, including Ruminococcus and Bifidobacteriaceae, in the recipient’s gut significantly increased, which is associated with improved clinical responses.66,67 Mechanisitically, melanoma patients with an improved response to ICIs following FMT showed enhanced intratumoral and intestinal immune infiltration.66,67 The above changes all indicate that FMT can improve the anticancer efficacy of ICIs by modifying the recipient’s gut microbial composition and then improving host immunity. In addition to improving the efficacy of anticancer therapy, available evidence has confirmed that FMT could cure adverse events occuring during cancer treatment. A recent case series reported that the ICI-induced colitis of two patients was cured by FMT, accompanied by a remodeling of the gut microbiome.370 In contrast, corticosteroids that are thought to play a role in anti-integrin and anti-TNF before FMT were also administered to both patients, but none of them worked.370 In addition, some researchers conducted a randomized controlled trial in tyrosine kinase inhibitor (TKI)-treated patients with renal cell carcinoma and found that the transplantation of fecal microbes from healthy donors into patients was able to cure TKI-induced diarrhea.371 These study findings all illustrate the broad application prospects of FMT in cancer treatment in the future.
Defined microbial consortia and probiotics
One of the disadvantages of FMT is the nonspecific entire microbiome of healthy donors or responders is inserted into the recipient’s gut. To more specifically modulate the recipient’s gut microbiota to more efficiently improve their response to other forms of cancer treatment, it has been envisaged to more purposefully combine one or several microorganisms into a single formulation.372 Existing evidence has demonstrated that certain microbial consortia could indeed boost the efficacy of conventional cancer therapies. In an RCT evaluating metastatic renal cell carcinoma, patients treated with both ICIs and CBM588, a bifidogenic live bacterial product, were found to have significantly longer progression-free survival and higher response rates to ICIs than patients treated with ICIs alone,70 demonstrating that bifidogenic live bacterial products may be able to promote the anticancer effects of ICIs on metastatic renal cell carcinoma. Moreover, a consortium composed of 11 bacterial strains from the feces of healthy donors was isolated to stimulate CD8 + T cells that reduce IFN-γ without causing inflammation.183 Furthermore, subsequent studies confirmed that the transplantation of this bacterial consortium into mice could enhance the therapeutic effect of ICIs.183 FMT may abrogate ICI-associated colitis by increasing the number of regulatory T cells within the gut mucosa.370 Although the great potential of microbial consortia as an adjuvant therapy for cancer has been demonstrated in these studies, many problems are still encountered, including the route of administration, dosage and cross-infection.
In addition to the above-mentioned bacterial consortia, the auxiliary role of probiotics in cancer treatment has also attracted widespread attention. For example, a probiotic compound consisting of four strains could significantly improve the prognosis of gastric cancer patients receiving gastrectomy, which was reflected in the reduction in the postoperative inflammation risk, the enhancement of immunity, the restoration of gut microbial homeostasis and the promotion of postoperative recovery.68 In addition, cancer patients who receive other forms of anticancer treatment may improve their prognosis and alleviate adverse events by taking probiotics.373,374 Unfortunately, probiotics can also have negative effects on cancer treatment. The administration of commercially available probiotics for melanoma patients was found to be associated with worse response to ICIs,315 which reminds us that the role of microorganisms is very complex and requires continuous in-depth exploration.
Targeted antibiotics
Long-term use of broad-spectrum antibiotics may lead to gut dysbiosis, which is often associated with poor clinical outcomes of cancer patients.306,375,376 However, relevant studies have also demonstrated that carefully selected ATB regimens could indirectly exert anticancer effects and reduce complications during cancer treatment by targeting oncogenic or pathogenic microorganisms.377,378,379 It is commendable that carefully selected antibiotics targeting carcinogenic organisms can be used not only to improve the clinical outcomes of cancer patients but also to help prevent cancer in populations at high risk of cancer or those with precancerous lesions. Dietary heme, a metabolite of red meat, could induce the cytotoxicity of colonic contents, which in turn promotes compensatory hyperproliferation and hyperplasia of the epithelium, ultimately leading to an increased risk of colon cancer, while antibiotics such as ampicillin, metronidazole, and neomycin could strengthen the mucus barrier and epithelial integrity by killing mucin-degrading bacteria and sulfur-producing bacteria, thereby preventing heme-dependent cytotoxic micelles from reaching the gut epithelium and ultimately reducing the risk of colon cancer caused by heme.380
Bacteriophage-based strategies
Some scholars have also proposed the idea of using phages to modulate the composition of the gut microbiome for anticancer purposes. Some researchers have covalently linked azide-modified phages with irinotecan-loaded dextran nanoparticles to inhibit F. nucleatum playing an unignorable role in the tumorigenesis of CRC, and it was confirmed that the administration of the joint unit could significantly enhance the efficacy of chemotherapy drugs for CRC.381 Moreover, bacteriophages can also remodel the TME. The M13 phage could specifically bind to F. nucleatum, and researchers assembled silver nanoparticles (AgNPs) on the surface capsid protein of this phage (M13@Ag).382 Subsequently, it was confirmed that M13@Ag could eliminate F. nucleatum in the gut, reduce the amplification of immunosuppressive myeloid-derived suppressor cells caused by F. nucleatum in tumor sites, and then remodel the TME against CRC.382 In addition, M13 phage could also activate antigen-presenting cells to further awaken the body’s immune system for CRC suppression.382
Genetically engineered/surface-modified bacteria strategies
In addition to indirectly improving the efficacy of anticancer therapy by modulating the composition of gut microbes, genetic engineering and surface modification have been used to modify bacteria for direct anticancer purposes in recent years.383 Some researchers have successfully enhanced the anticancer activity of violacein under hypoxia by transferring the violacein biosynthetic cluster into the oncolytic strain VNP20009 of Salmonella, which acts as a targeted delivery vehicle with tumor-colonizing properties.384 Another approach is surface modification, that is, making various modifications to the envelope structure of bacteria to endow them with new biological properties.385 Li et al. decorated the surface of bacteria with checkpoint-blocking antibodies and tumor-specific antigens, and the modified bacteria achieved effective antitumor efficacy in antigen-overexpressing tumor models.386
Diet and prebiotic strategies
Dietary intervention is an indirect and more moderate strategy than the aforementioned approaches that directly modulate gut microbial composition. Many preclinical studies have confirmed that dietary intervention can alleviate chemotherapy-induced toxicity387 and enhance the body’s anticancer immune surveillance during immunotherapy.315,388,389,390,391 Relevant dietary strategies include fasting-mimicking diets(FMDs),392 high-fiber diets,315,393 and ketogenic diets.388 FMDs such as cyclic fasting, low-carbohydrate diets and calorie restriction could reshape anticancer immunity in cancer patients by enriching IFN-γ, enhancing intratumoral Th1/cytotoxic responses, and inducing the contraction of regulatory T-cell compartments, and stimulating other immune signatures related to favorable clinical outcomes.394
The concept of prebiotics was first proposed in 1995 by Glenn R Gibson, and it refers to indigestible food components that influence the host by selectively promoting targeted bacterial species growth in the colon to improve host health.395 In recent years, with the deepening of research, some prebiotics have been found to shift the metabolism of the gut microbiota in a direction that is beneficial to anticancer treatment and improve the efficacy of anticancer treatment.396,397 Prebiotic inulin can exert its effects through a variety of pathways, thereby increasing its activity in the intestine and enhancing the function of gut T lymphocytes, thereby overcoming resistance to MEK inhibitors.398 Ginseng polysaccharides, a prebiotic derived from ginseng, could enhance the cancer response to PD1 inhibitors by decreasing the ratio of kynurenine/tryptophan and increasing the microbial metabolite valeric acid, thereby contributing to the induction of Teff cells and the suppression of regulatory T cells.399 In addition, Ganoderma lucidum polysaccharide could alleviate AOM/DSS-induced gut dysbiosis, increase the production of SCFAs, and alleviate endotoxemia by suppressing the TLR4/MyD88/NF-κB pathway, which may be associated with its ability to reduce AOM/DSS-induced colitis and tumorigenesis.400 These two findings remind us that we can continue to extract new anticancer prebiotics from traditional Chinese herbal medicine to develop more cancer treatment options in the future.
Nanotechnology modulation of the gut microbiota for cancer therapy
Over the past decades, nanotechnology has been studied for cancer treatment, but there is little research on how to modulate the gut microbiota with nanotechnology to indirectly achieve anticancer goals. Recently, some researchers have used the membrane of Helicobacter pylori to fabricate a bacterial outer membrane-coated nanoparticle, which could compete with H. pylori to inhibit pathogen adhesion.401 Although the study did not definitively demonstrate that the inhibition of pathogen adhesion by such nanoparticles is relevant to cancer therapy, it provided us with an idea to use the membrane of target bacteria to prepare specific nanoparticles that could compete with target bacteria to inhibit their adhesion and reduce their abundance, thereby improving anticancer efficacy. Preparing anticancer nanoformulations with certain components of microorganisms is also a promising research direction for cancer treatment. Yeast cell walls were used to create four different-sized nanoformulations that could remodel the immune microenvironment in tumors and tumor-draining lymph nodes, thereby suppressing tumor growth.402 Notably, due to the superiority of accumulating in tumor-draining lymph node, the T-cell-mediated anticancer immune response induced by the small size of the nano-formulation is stronger than the big size.402
Spore-based anticancer strategy
Spore is defined as a dormant or reproductive body produced by plants, fungi, and some microorganisms and it can develop into a new individual either directly or after fusion with another spore. In this article, spore refers specifically to the dormant body of bacteria and fungi.
One of the most common forms of spore-based strategy is drug delivery system. The dormant spores of Bacillus cagulans, a probiotic conducive to the treatment of intestinal inflammation and the regulation of gut microbial balance, can resist the harsh acidic environment, complex chemicals as well as temperature in gastrointestinal tract and germinate to probiotics under the activation by some nutrients in the gut.403 Additionally, during the process of germination, the hydrophobic protein coat on the surface of spores falls off.404,405 Thus, based on these physiological properties of the spores, a new oral drug delivery system for cancer therapy was developed by Song and colleagues.403 Specifically, the spore of B. cagulans was modified with DCA and loaded with chemotherapeutics, and the complex can disintegrate in the intestinal microenvironment, which is consequently accompanied by the self-assembly of nanoparticles containing chemotherapy drugs.403 More importantly, this system can protect the agents from acidic environment of the stomach, overcome intestinal barriers and decrease degradation of drugs in the epithelial cells, which would ultimately increase basolateral drug release into the circulation enhance and enhance the tumor inhibition efficency.403 Similarly, Clostridium butyricum spore was also used to develop oral drug delivery system for PDAC chemotherapy, which could markedly increase intratumoral drug accumulation.406
Additionally, spores of bacteria can also be used to treat cancer. Clostridial spores have been thoroughly investigated in that the obligate anaerobic nature of Clostridium makes them exclusively localized to and germinate in the necrotic/ hypoxic area of solid tumors.407 Thus, clostridial spores can be carriers of anticancer drugs or some special genes, which direct at TME. What’s more, clostridial spores can be used to decrease the side effects of chemotherapy. The toxicity of chemotherapy is mainly due to the lack of specificity for tumor cells and the damage to normal cells. Thus, genes expressing enzymes that convert the innocuous prodrug to toxic derivative can be introduced into clostridium, and injection of the transgenic bacterial spores can decrease systematic side effects when combined with nontoxic prodrug administration.408
Cancer microbiota in clinical trials
Given the accumulating evidence involving the molecular mechanisms of microbiota effects on cancer development, an increasing number of clinical trials that aim to achieve clinical translation of microbial therapy are currently ongoing or have been completed,70,371,373,409,410,411,412 and some selected trials are summarized in Tables 2 and 3. Basically, there are two directions for the manipulation of the gut microbiota in cancer therapy: one is to boost therapeutic efficacy, and the other is to reduce therapy-related toxicity or side effects. For instance, a US trial (NCT04116775) for metastatic prostate cancer of FMT via endoscopy from pembrolizumab-sensitive participants into pembrolizumab-resistant participants aims to boost recipients’ antitumor efficacy and increase their tumor sensitivity to ICIs.413 Another clinical trial (NCT05032014) is assessing whether probiotics (Probio-49) can enhance PD-1 inhibitor efficacy in the treatment of liver cancer.414 To reduce immune-related toxicity, immunotherapy combined with FMT is being applied in renal cell carcinoma patients.415 Oral administration of probiotics is being used with concurrent pelvic chemoradiotherapy to evaluate its feasibility in the inhibition of radiation injury and related enteritis (NCT05032027).416 Another clinical trial actively is being performed to mitigate or prevent adverse events following chemotherapy with the use of probiotic supplements to keep breast cancer patients from experiencing chemotherapy-related toxicity.373 In addition, probiotic supplements can reduce and prevent the occurrence of chemotherapy-related cognitive impairment (CRCI).373 In addition, thyroid hormone withdrawal-related complications, such as dyslipidemia and constipation, in thyroid cancer patients following thyroidectomy could be alleviated by taking a probiotic complex.417 We are looking forward to seeing the prospective outcomes of these studies, which can be fundamental evidence for the clinical applications involving the gut microbiota, although further studies to determine the more specific and accurate molecular interactions underlying the microbiota and antitumor activity are still substantially needed.
Future challenges and outlook
Therapeutic resistance and adverse effect are still the main obstacles in the management of cancer treatment, despite great efforts to optimize therapeutic effects and minimize adverse toxicity.418 Hence, the future of utilizing the cancer-associated microbes in the clinic is not devoid of prospects and challenges that should be recognized and addressed.
Currently, due to lacks of uniformed methodology, including differences in sample selection and collection, technology, data quality as well as resource analysis, the homogeneity and consistency of mechanistic understanding of microbial effect on cancer could not be ensured. Different samples from same subjects may lead to largely heterogeneous results. For instance, the composition and richness of microbiota colonized on the digestive tract mucosa and those in feces are similar, but not identical.419 If only one type of sample is included in the study, it may lead to biased results. Henceforth, several different types of samples should be collected and investigated for objective research results.
In addition, errors may occur in the process of sample collection and handling. Because of the low biomass of tumor microbiota, any contamination of samples would dramatically hamper the microbial research, which can be caused by long surgery, cross-contamination from other samples and complex environment in laboratory.32,420 Thus, in order to ensure the rigorous research results, it is crucial to implement multiple measures to decrease the possibility of sample contamination, such as wearing clean protective clothing to cover all exposed human surfaces when collecting sample.420 In addition, technical variables, e.g., sample handling, DNA extraction, bioinformatics, and data acquisition, exist in identifying specific compositional and functional microbial signatures. Some may use 16 S rRNA sequencing of saliva or bile samples, while others may examine stool samples, and high-throughput data may be produced either by next-generation sequencing (NGS) or third-generation sequencing (Nanopore or SMRT sequencing), increasing the heterogeneity of data resources and accessibility difficulties. To address these challenges, a comprehensive “standard operation procedure (SOP)” for all methodologies could be introduced in coming years, with the precondition of reaching consensuses on sample collection, technique selection, and data sharing and analysis, despite the multiple existing protocols proposed by the Microbiome Quality Control (MBQC) project consortium.421
In addition to the methodological challenges described above, individual biological differences may encumber the application of microbial strategies. Various factors, including genetics, diet habits, age, sex, accompanying diseases and regional variations,422,423 can influence the features of human microbiota. He and colleagues have shown that host location has the strongest impact on gut microbiota variations compared to other factors, which is marked by the large variations in the abundance of Firmicutes among populations in different districts of Guangdong, China.424 This regional variation to human microbiota is one of main reasons limiting the spread and application of certain findings in other districts.424 For example, some microbes can serve as non-invasive diagnostic biomarkers of CRC,425 but it may suffer a setback when this finding is generalized to other regions.424 It must be noted that, from a deeper perspective, region is not a single factor, but a complex of various factors, including economic development, diet habit, ecological environment in the region and etc. Thus, it is not surprising that geography has such a noticeable influence on the human microbiota.
In the near future, emphasis should be placed on distinct microbiota stratification, and the unique strain obtained in different hosts might be researched by a “single microbe” profile, analogous to the single-cell sequence, which can facilitate the accurate capture of precise impacting mechanisms. Furthermore, some special preclinical models, e.g., patient-derived organotypic tumor spheroids in short-term 3D cultures within the same environmental surroundings, can be used to validate the findings in vitro and to link the molecular mechanisms to applications.
Despite accumulating evidence observed in human subjects, the corresponding clinical interventions targeted at microbes have yet to be translated to mature applications for cancer patients. The causes resulting in this phenomenon are extremely complex, which can be partly attributed to the individual differences in sensitivity to the same microbial agents. Can microbes-targeted interventions be integrated in existing cancer management system to exert more comprehensive and favorable antitumor effects? The problem remains unresolved till now and thus more preclinical research and prospective clinical trials are needed to figure out the challenges.
Finally, although many challenges remain for now, the great importance and full potential of gut microbiota cannot be overstated for the development of new anti-cancer strategies, and it is necessary to explore a holistic approach that incorporates microbial modulation therapy in the current cancer management system.
References
Sender, R., Fuchs, S. & Milo, R. Revised estimates for the number of human and bacteria cells in the body. PLoS Biol 14, e1002533 (2016).
Adak, A. & Khan, M. R. An insight into gut microbiota and its functionalities. Cell. Mol. Life Sci. 76, 473–493 (2019).
Martinez-Guryn, K., Leone, V. & Chang, E. B. Regional diversity of the gastrointestinal microbiome. Cell Host Microbe 26, 314–324 (2019).
Kovatcheva-Datchary, P. et al. Dietary fiber-induced improvement in glucose metabolism is associated with increased abundance of prevotella. Cell Metab 22, 971–982 (2015).
Cahenzli, J., Köller, Y., Wyss, M., Geuking, M. B. & McCoy, K. D. Intestinal microbial diversity during early-life colonization shapes long-term IgE levels. Cell Host Microbe 14, 559–570 (2013).
Sender, R., Fuchs, S. & Milo, R. Are we really vastly outnumbered? revisiting the ratio of bacterial to host. Cells in Humans. Cell 164, 337–340 (2016).
Gensollen, T., Iyer, S. S., Kasper, D. L. & Blumberg, R. S. How colonization by microbiota in early life shapes the immune system. Science 352, 539–544 (2016).
Cummings, J. H. Fermentation in the human large intestine: evidence and implications for health. Lancet 1, 1206–1209 (1983).
McNeil, N. I. The contribution of the large intestine to energy supplies in man. Am. J. Clin. Nutr. 39, 338–342 (1984).
Yu, L. X. & Schwabe, R. F. The gut microbiome and liver cancer: mechanisms and clinical translation. Nat. Rev. Gastroenterol. Hepatol. 14, 527–539 (2017).
Tilg, H., Adolph, T. E., Gerner, R. R. & Moschen, A. R. The intestinal microbiota in colorectal cancer. Cancer Cell 33, 954–964 (2018).
Dejea, C. M. et al. Patients with familial adenomatous polyposis harbor colonic biofilms containing tumorigenic bacteria. Science 359, 592–597 (2018).
Kadosh, E. et al. The gut microbiome switches mutant p53 from tumour-suppressive to oncogenic. Nature 586, 133–138 (2020).
Ma, C. et al. Gut microbiome-mediated bile acid metabolism regulates liver cancer via NKT cells. Science 360, 876 (2018).
Meisel, M. et al. Microbial signals drive pre-leukaemic myeloproliferation in a Tet2-deficient host. Nature 557, 580–584 (2018).
Viennois, E., Gewirtz, A. T. & Chassaing, B. Connecting the dots: dietary fat, microbiota dysbiosis, altered metabolome, and colon cancer. Gastroenterology 162, 38–39 (2022).
Liu, N. N. et al. Microbiome dysbiosis in lung cancer: from composition to therapy. NPJ Precis Oncol 4, 33 (2020).
Verstraelen, H. Of microbes and women: BRCA1, vaginal microbiota, and ovarian cancer. Lancet Oncol 20, 1049–1051 (2019).
Buchta Rosean, C. et al. Preexisting commensal dysbiosis is a host-intrinsic regulator of tissue inflammation and tumor cell dissemination in hormone receptor-positive breast cancer. Cancer Res. 79, 3662–3675 (2019).
Parida, S. et al. A procarcinogenic colon microbe promotes breast tumorigenesis and metastatic progression and concomitantly activates notch and β-catenin axes. Cancer Discov 11, 1138–1157 (2021).
Liou, J. M. et al. Screening and eradication of Helicobacter pylori for gastric cancer prevention: the Taipei global consensus. Gut 69, 2093–2112 (2020).
Zhao, K. & Hu, Y. Microbiome harbored within tumors: a new chance to revisit our understanding of cancer pathogenesis and treatment. Signal Transduct Target Ther 5, 136 (2020).
Cogdill, A. P., Gaudreau, P. O., Arora, R., Gopalakrishnan, V. & Wargo, J. A. The impact of intratumoral and gastrointestinal microbiota on systemic cancer therapy. Trends Immunol 39, 900–920 (2018).
Heymann, C. J. F., Bard, J. M., Heymann, M. F., Heymann, D. & Bobin-Dubigeon, C. The intratumoral microbiome: Characterization methods and functional impact. Cancer Lett 522, 63–79 (2021).
Wong-Rolle, A., Wei, H. K., Zhao, C. & Jin, C. Unexpected guests in the tumor microenvironment: microbiome in cancer. Protein Cell 12, 426–435 (2021).
LaCourse, K. D. et al. The cancer chemotherapeutic 5-fluorouracil is a potent Fusobacterium nucleatum inhibitor and its activity is modified by intratumoral microbiota. Cell Rep. 41, 111625 (2022).
Consortium, I. T. P.-C. A. O. W. G. Pan-cancer analysis of whole genomes. Nature 578, 82–93 (2020).
Erdag, G. et al. Immunotype and immunohistologic characteristics of tumor-infiltrating immune cells are associated with clinical outcome in metastatic melanoma. Cancer Res. 72, 1070–1080 (2012).
Kather, J. N. et al. Topography of cancer-associated immune cells in human solid tumors. Elife 7, e36967 (2018).
Stearn, E. W., Sturdivant, B. F. & Stearn, A. E. The life history of a micro-parasite isolated from carcinomatous growths. Proc. Natl Acad. Sci. USA. 11, 662–669 (1925).
Fu, A. et al. Tumor-resident intracellular microbiota promotes metastatic colonization in breast cancer. Cell 185, 1356–1372.e1326 (2022).
Nejman, D. et al. The human tumor microbiome is composed of tumor type-specific intracellular bacteria. Science 368, 973–980 (2020).
Narunsky-Haziza, L. et al. Pan-cancer analyses reveal cancer-type-specific fungal ecologies and bacteriome interactions. Cell 185, 3789–3806.e3717 (2022).
Dohlman, A. B. et al. A pan-cancer mycobiome analysis reveals fungal involvement in gastrointestinal and lung tumors. Cell 185, 3807–3822.e3812 (2022).
Kwon, S. K. et al. Human gastric microbiota transplantation recapitulates premalignant lesions in germ-free mice. Gut 71, 1266–1276 (2022).
Palrasu, M. et al. Helicobacter pylori pathogen inhibits cellular responses to oncogenic stress and apoptosis. PLoS Pathog 18, e1010628 (2022).
Kumar, R. et al. Streptococcus gallolyticus subsp. gallolyticus promotes colorectal tumor development. PLoS Pathog 13, e1006440 (2017).
Yang, Y. et al. Fusobacterium nucleatum Increases Proliferation of Colorectal Cancer Cells and Tumor Development in Mice by Activating Toll-Like Receptor 4 Signaling to Nuclear Factor-κB, and Up-regulating Expression of MicroRNA-21. Gastroenterology 152, 851–866.e824 (2017).
Dapito, D. H. et al. Promotion of hepatocellular carcinoma by the intestinal microbiota and TLR4. Cancer Cell 21, 504–516 (2012).
Yu, L. X. et al. Endotoxin accumulation prevents carcinogen-induced apoptosis and promotes liver tumorigenesis in rodents. Hepatology 52, 1322–1333 (2010).
Aykut, B. et al. The fungal mycobiome promotes pancreatic oncogenesis via activation of MBL. Nature 574, 264–267 (2019).
Yu, Q. et al. Intestinal microbiota modulates pancreatic carcinogenesis through intratumoral natural killer cells. Gut Microbes 14, 2112881 (2022).
Geller, L. T. et al. Potential role of intratumor bacteria in mediating tumor resistance to the chemotherapeutic drug gemcitabine. Science 357, 1156–1160 (2017).
Yu, T. et al. Fusobacterium nucleatum promotes chemoresistance to colorectal cancer by modulating autophagy. Cell 170, 548–563.e516 (2017).
Dong, J. et al. Oral microbiota affects the efficacy and prognosis of radiotherapy for colorectal cancer in mouse models. Cell Rep 37, 109886 (2021).
Li, Z. et al. Gut microbiota modulate radiotherapy-associated antitumor immune responses against hepatocellular carcinoma Via STING signaling. Gut Microbes 14, 2119055 (2022).
Routy, B. et al. Gut microbiome influences efficacy of PD-1-based immunotherapy against epithelial tumors. Science 359, 91–97 (2018).
Derosa, L. et al. Gut bacteria composition drives primary resistance to cancer immunotherapy in renal cell carcinoma patients. Eur. Urol. 78, 195–206 (2020).
Xie, Y. et al. Microbiota in tumors: from understanding to application. Adv Sci. 9, e2200470 (2022).
Plummer, M. et al. Global burden of cancers attributable to infections in 2012: a synthetic analysis. Lancet Glob Health 4, e609–e616 (2016).
Cremonesi, E. et al. Gut microbiota modulate T cell trafficking into human colorectal cancer. Gut 67, 1984–1994 (2018).
Pushalkar, S. et al. The pancreatic cancer microbiome promotes oncogenesis by induction of innate and adaptive immune suppression. Cancer Discov 8, 403–416 (2018).
Gopalakrishnan, V., Helmink, B. A., Spencer, C. N., Reuben, A. & Wargo, J. A. The influence of the gut microbiome on cancer, immunity, and cancer immunotherapy. Cancer Cell 33, 570–580 (2018).
Long, X. et al. Peptostreptococcus anaerobius promotes colorectal carcinogenesis and modulates tumour immunity. Nat Microbiol 4, 2319–2330 (2019).
Hexun, Z. et al. High abundance of Lachnospiraceae in the human gut microbiome is related to high immunoscores in advanced colorectal cancer. Cancer Immunol. Immunother. 75, 315–326 (2022).
Bhatt, A. P., Redinbo, M. R. & Bultman, S. J. The role of the microbiome in cancer development and therapy. CA Cancer J. Clin 67, 326–344 (2017).
Doocey, C. M., Finn, K., Murphy, C. & Guinane, C. M. The impact of the human microbiome in tumorigenesis, cancer progression, and biotherapeutic development. BMC Microbiol 22, 53 (2022).
Pleguezuelos-Manzano, C. et al. Mutational signature in colorectal cancer caused by genotoxic pks(+) E. coli. Nature 580, 269–273 (2020).
Wilson, M. R. et al. The human gut bacterial genotoxin colibactin alkylates DNA. Science 363, 709 (2019).
Yang, Y. et al. Fusobacterium nucleatum Increases Proliferation of Colorectal Cancer Cells and Tumor Development in Mice by Activating Toll-Like Receptor 4 Signaling to Nuclear Factor-kappaB, and Up-regulating Expression of MicroRNA-21. Gastroenterology 152, 851–866.e824 (2017).
Sayed, I. M. et al. Helicobacter pylori infection downregulates the DNA glycosylase NEIL2, resulting in increased genome damage and inflammation in gastric epithelial cells. J. Biol. Chem. 295, 11082–11098 (2020).
Han, T. et al. H. pylori infection alters repair of DNA double-strand breaks via SNHG17. J. Clin. Investig. 130, 3901–3918 (2020).
Yachida, S. et al. Metagenomic and metabolomic analyses reveal distinct stage-specific phenotypes of the gut microbiota in colorectal cancer. Nat. Med. 25, 968–976 (2019).
Garrett, W. S. The gut microbiota and colon cancer. Science 364, 1133–1135 (2019).
Elinav, E., Garrett, W. S., Trinchieri, G. & Wargo, J. The cancer microbiome. Nat. Rev. Cancer 19, 371–376 (2019).
Baruch, E. N. et al. Fecal microbiota transplant promotes response in immunotherapy-refractory melanoma patients. Science 371, 602–609 (2021).
Davar, D. et al. Fecal microbiota transplant overcomes resistance to anti-PD-1 therapy in melanoma patients. Science 371, 595–602 (2021).
Zheng, C. et al. Adjuvant treatment and molecular mechanism of probiotic compounds in patients with gastric cancer after gastrectomy. Food Funct 12, 6294–6308 (2021).
Pan, L. L. et al. Clostridium butyricum strains suppress experimental acute pancreatitis by maintaining intestinal homeostasis. Mol. Nutr. Food Res. 63, e1801419 (2019).
Dizman, N. et al. Nivolumab plus ipilimumab with or without live bacterial supplementation in metastatic renal cell carcinoma: a randomized phase 1 trial. Nat. Med. 28, 704–712 (2022).
Amabebe, E., Robert, F. O., Agbalalah, T. & Orubu, E. S. F. Microbial dysbiosis-induced obesity: role of gut microbiota in homoeostasis of energy metabolism. Br. J. Nutr. 123, 1127–1137 (2020).
Mousa, W. K., Chehadeh, F. & Husband, S. Microbial dysbiosis in the gut drives systemic autoimmune diseases. Front. Immunol. 13, 906258 (2022).
Sadrekarimi, H. et al. Emerging role of human microbiome in cancer development and response to therapy: special focus on intestinal microflora. J. Transl. Med. 20, 301 (2022).
Laniewski, P., Ilhan, Z. E. & Herbst-Kralovetz, M. M. The microbiome and gynaecological cancer development, prevention and therapy. Nat Rev Urol 17, 232–250 (2020).
Garrett, W. S. Cancer and the microbiota. Science 348, 80–86 (2015).
Zitvogel, L., Ayyoub, M., Routy, B. & Kroemer, G. Microbiome and anticancer immunosurveillance. Cell 165, 276–287 (2016).
Yoshimoto, S. et al. Obesity-induced gut microbial metabolite promotes liver cancer through senescence secretome. Nature 499, 97–101 (2013).
Loo, T. M. et al. Gut microbiota promotes obesity-associated liver cancer through PGE(2)-mediated suppression of antitumor immunity. Cancer Discov 7, 522–538 (2017).
Zhang, J. et al. Expansion of colorectal cancer biomarkers based on gut bacteria and viruses. Cancers (Basel) 14, 1–19 (2022).
Yu, X. et al. Gut microbiota changes and its potential relations with thyroid carcinoma. J. Adv. Res. 35, 61–70 (2022).
Ubachs, J. et al. Gut microbiota and short-chain fatty acid alterations in cachectic cancer patients. J. Cachexia Sarcopenia Muscle 12, 2007–2021 (2021).
Drewes, J. L. et al. Human colon cancer-derived Clostridioides difficile strains drive colonic tumorigenesis in mice. Cancer Discov 12, 1873–1885 (2022).
Wong, S. H. et al. Gavage of fecal samples from patients with colorectal cancer promotes intestinal carcinogenesis in germ-free and conventional mice. Gastroenterology 153, 1621–1633.e1626 (2017).
Butcher, L. D., den Hartog, G., Ernst, P. B. & Crowe, S. E. Oxidative stress resulting From Helicobacter pylori infection contributes to gastric carcinogenesis. Cell. Mol. Gastroenterol. Hepatol. 3, 316–322 (2017).
Beil, W. et al. Role of vacA and cagA in Helicobacter pylori inhibition of mucin synthesis in gastric mucous cells. J. Clin. Microbiol. 38, 2215–2218 (2000).
Chaturvedi, R. et al. Spermine oxidase mediates the gastric cancer risk associated with Helicobacter pylori CagA. Gastroenterology 141, 1696–1708.e1691-1692 (2011).
Guo, S. et al. Exosomes derived from Fusobacterium nucleatum-infected colorectal cancer cells facilitate tumour metastasis by selectively carrying miR-1246/92b-3p/27a-3p and CXCL16. Gut 70, 1507–1519 (2020).
Rubinstein, M. R. et al. Fusobacterium nucleatum promotes colorectal carcinogenesis by modulating E-cadherin/β-catenin signaling via its FadA adhesin. Cell Host Microbe 14, 195–206 (2013).
Engevik, M. A. et al. Fusobacterium nucleatum secretes outer membrane vesicles and promotes intestinal inflammation. mBio 12, e02706–20 (2021).
Liu, L., Liang, L., Yang, C., Zhou, Y. & Chen, Y. Extracellular vesicles of Fusobacterium nucleatum compromise intestinal barrier through targeting RIPK1-mediated cell death pathway. Gut Microbes 13, 1–20 (2021).
Zhang, Y., Zhang, J., Xia, Y. & Sun, J. Bacterial translocation and barrier dysfunction enhance colonic tumorigenesis. Neoplasia 35, 100847 (2022).
Multhoff, G., Molls, M. & Radons, J. Chronic inflammation in cancer development. Front. Immunol. 2, 98 (2011).
Hui, L. & Chen, Y. Tumor microenvironment: sanctuary of the devil. Cancer Lett 368, 7–13 (2015).
Lugano, R., Ramachandran, M. & Dimberg, A. Tumor angiogenesis: causes, consequences, challenges and opportunities. Cell. Mol. Life Sci. 77, 1745–1770 (2020).
Joyce, J. A. & Fearon, D. T. T cell exclusion, immune privilege, and the tumor microenvironment. Science 348, 74–80 (2015).
Ma, J. et al. The role of the tumor microbe microenvironment in the tumor immune microenvironment: bystander, activator, or inhibitor? J. Exp. Clin. Cancer Res. 40, 327 (2021).
Vaupel, P. & Harrison, L. Tumor hypoxia: causative factors, compensatory mechanisms, and cellular response. Oncologist 9(Suppl 5), 4–9 (2004).
Milotti, E., Fredrich, T., Chignola, R. & Rieger, H. Oxygen in the tumor microenvironment: mathematical and numerical modeling. Adv. Exp. Med. Biol. 1259, 53–76 (2020).
Khodaverdi, N., Zeighami, H., Jalilvand, A., Haghi, F. & Hesami, N. High frequency of enterotoxigenic Bacteroides fragilis and Enterococcus faecalis in the paraffin-embedded tissues of Iranian colorectal cancer patients. BMC Cancer 21, 1353 (2021).
Yuan, Y. Spatial heterogeneity in the tumor microenvironment. Cold Spring Harb. Perspect. Med. 6, a02683 (2016).
Xu, C. et al. Fusobacterium nucleatum promotes colorectal cancer metastasis through miR-1322/CCL20 axis and M2 polarization. Gut Microbes 13, 1980347 (2021).
Chen, S. et al. Fusobacterium nucleatum promotes colorectal cancer metastasis by modulating KRT7-AS/KRT7. Gut Microbes 11, 511–525 (2020).
Gao, Y. et al. Fusobacterium nucleatum stimulates cell proliferation and promotes PD-L1 expression via IFIT1-related signal in colorectal cancer. Neoplasia 35, 100850 (2023).
Mima, K. et al. Fusobacterium nucleatum and T cells in colorectal carcinoma. JAMA Oncol 1, 653–661 (2015).
Abed, J. et al. Colon cancer-associated Fusobacterium nucleatum may originate from the oral cavity and reach colon tumors via the circulatory system. Front Cell Infect Microbiol 10, 400 (2020).
Hamada, T. et al. Fusobacterium nucleatum in colorectal cancer relates to immune response differentially by tumor microsatellite instability status. Cancer Immunol Res 6, 1327–1336 (2018).
Chmiela, M., Walczak, N. & Rudnicka, K. Helicobacter pylori outer membrane vesicles involvement in the infection development and Helicobacter pylori-related diseases. J. Biomed. Sci. 25, 78 (2018).
González, M. F., Díaz, P., Sandoval-Bórquez, A., Herrera, D. & Quest, A. F. G. Helicobacter pylori outer membrane vesicles and extracellular vesicles from Helicobacter pylori-Infected cells in gastric disease development. Int. J. Mol. Sci. 22, 4823 (2021).
Song, X. et al. Microbial metabolite deoxycholic acid promotes vasculogenic mimicry formation in intestinal carcinogenesis. Cancer Sci 113, 459–477 (2022).
Barrett, M., Hand, C. K., Shanahan, F., Murphy, T. & O’Toole, P. W. Mutagenesis by microbe: the role of the microbiota in shaping the cancer genome. Trends Cancer 6, 277–287 (2020).
Cao, Y. et al. Commensal microbiota from patients with inflammatory bowel disease produce genotoxic metabolites. Science 378, eabm3233 (2022).
Vizcaino, M. I. & Crawford, J. M. The colibactin warhead crosslinks DNA. Nat. Chem. 7, 411–417 (2015).
Putze, J. et al. Genetic structure and distribution of the colibactin genomic island among members of the family Enterobacteriaceae. Infect. Immun. 77, 4696–4703 (2009).
Toller, I. M. et al. Carcinogenic bacterial pathogen Helicobacter pylori triggers DNA double-strand breaks and a DNA damage response in its host cells. Proc. Natl Acad. Sci. USA. 108, 14944–14949 (2011).
Valguarnera, E. & Wardenburg, J. B. Good gone bad: one toxin away from disease for Bacteroides fragilis. J. Mol. Biol. 432, 765–785 (2020).
Martin, O. C. B. et al. Infection with genotoxin-producing Salmonella enterica synergises with loss of the tumour suppressor APC in promoting genomic instability via the PI3K pathway in colonic epithelial cells. Cell. Microbiol. 21, e13099 (2019).
Azenabor, A. A. & Mahony, J. B. Generation of reactive oxygen species and formation and membrane lipid peroxides in cells infected with Chlamydia trachomatis. Int. J. Infect. Dis. 4, 46–50 (2000).
Chumduri, C., Gurumurthy, R. K., Zadora, P. K., Mi, Y. & Meyer, T. F. Chlamydia infection promotes host DNA damage and proliferation but impairs the DNA damage response. Cell Host Microbe 13, 746–758 (2013).
Goodwin, A. C. et al. Polyamine catabolism contributes to enterotoxigenic Bacteroides fragilis-induced colon tumorigenesis. Proc. Natl Acad. Sci. USA. 108, 15354–15359 (2011).
Xu, H. et al. Spermine oxidation induced by Helicobacter pylori results in apoptosis and DNA damage: implications for gastric carcinogenesis. Cancer Res 64, 8521–8525 (2004).
Hartung, M. L. et al. H. pylori-Induced DNA strand breaks are introduced by nucleotide excision repair endonucleases and promote NF-κB target gene expression. Cell Rep 13, 70–79 (2015).
Tse, J. W. T., Jenkins, L. J., Chionh, F. & Mariadason, J. M. Aberrant DNA methylation in colorectal cancer: what should we target? Trends Cancer 3, 698–712 (2017).
Xia, X. et al. Bacteria pathogens drive host colonic epithelial cell promoter hypermethylation of tumor suppressor genes in colorectal cancer. Microbiome 8, 108 (2020).
Ciccia, A. & Elledge, S. J. The DNA damage response: making it safe to play with knives. Mol. Cell 40, 179–204 (2010).
Tubbs, A. & Nussenzweig, A. Endogenous DNA damage as a source of genomic instability in cancer. Cell 168, 644–656 (2017).
Harper, J. W. & Elledge, S. J. The DNA damage response: ten years after. Mol. Cell 28, 739–745 (2007).
Lee, J. H. & Paull, T. T. ATM activation by DNA double-strand breaks through the Mre11-Rad50-Nbs1 complex. Science 308, 551–554 (2005).
Lee, J. H. & Paull, T. T. Activation and regulation of ATM kinase activity in response to DNA double-strand breaks. Oncogene 26, 7741–7748 (2007).
Lavin, M. F. ATM and the Mre11 complex combine to recognize and signal DNA double-strand breaks. Oncogene 26, 7749–7758 (2007).
Kim, J. J. et al. Helicobacter pylori impairs DNA mismatch repair in gastric epithelial cells. Gastroenterology 123, 542–553 (2002).
Matsumoto, Y. et al. Helicobacter pylori infection triggers aberrant expression of activation-induced cytidine deaminase in gastric epithelium. Nat. Med. 13, 470–476 (2007).
Li, X. & Heyer, W. D. Homologous recombination in DNA repair and DNA damage tolerance. Cell Res 18, 99–113 (2008).
Koeppel, M., Garcia-Alcalde, F., Glowinski, F., Schlaermann, P. & Meyer, T. F. Helicobacter pylori infection causes characteristic DNA damage patterns in human cells. Cell Rep 11, 1703–1713 (2015).
Shibata, A. et al. DNA double-strand break repair pathway choice is directed by distinct MRE11 nuclease activities. Mol. Cell 53, 7–18 (2014).
Panier, S. & Boulton, S. J. Double-strand break repair: 53BP1 comes into focus. Nat. Rev. Mol. Cell Biol. 15, 7–18 (2014).
Hanada, K. et al. Helicobacter pylori infection introduces DNA double-strand breaks in host cells. Infect. Immun. 82, 4182–4189 (2014).
Sishc, B. J. & Davis, A. J. The role of the core non-homologous end joining factors in carcinogenesis and cancer. Cancers (Basel) 9, 1–30 (2017).
Gaymes, T. J., Mufti, G. J. & Rassool, F. V. Myeloid leukemias have increased activity of the nonhomologous end-joining pathway and concomitant DNA misrepair that is dependent on the Ku70/86 heterodimer. Cancer Res 62, 2791–2797 (2002).
Kastenhuber, E. R. & Lowe, S. W. Putting p53 in context. Cell 170, 1062–1078 (2017).
Shieh, S. Y., Ikeda, M., Taya, Y. & Prives, C. DNA damage-induced phosphorylation of p53 alleviates inhibition by MDM2. Cell 91, 325–334 (1997).
Williams, A. B. & Schumacher, B. p53 in the DNA-Damage-Repair Process. Cold Spring Harb. Perspect. Med. 6, a026070 (2016).
Hassin, O. & Oren, M. Drugging p53 in cancer: one protein, many targets. Nat. Rev. Drug Discov. 22, 127–144 (2022).
Buti, L. et al. Helicobacter pylori cytotoxin-associated gene A (CagA) subverts the apoptosis-stimulating protein of p53 (ASPP2) tumor suppressor pathway of the host. Proc. Natl Acad. Sci. USA. 108, 9238–9243 (2011).
Clevers, H. Wnt/beta-catenin signaling in development and disease. Cell 127, 469–480 (2006).
Gregorieff, A. & Clevers, H. Wnt signaling in the intestinal epithelium: from endoderm to cancer. Genes Dev 19, 877–890 (2005).
Zhan, T., Rindtorff, N. & Boutros, M. Wnt signaling in cancer. Oncogene 36, 1461–1473 (2017).
Yu, F. et al. Wnt/β-catenin signaling in cancers and targeted therapies. Signal Transduct Target Ther 6, 307 (2021).
Wu, S., Morin, P. J., Maouyo, D. & Sears, C. L. Bacteroides fragilis enterotoxin induces c-Myc expression and cellular proliferation. Gastroenterology 124, 392–400 (2003).
Wu, S., Lim, K. C., Huang, J., Saidi, R. F. & Sears, C. L. Bacteroides fragilis enterotoxin cleaves the zonula adherens protein, E-cadherin. Proc. Natl Acad. Sci. USA. 95, 14979–14984 (1998).
Fang, J. Y. & Richardson, B. C. The MAPK signalling pathways and colorectal cancer. Lancet Oncol 6, 322–327 (2005).
Mimuro, H. et al. Helicobacter pylori dampens gut epithelial self-renewal by inhibiting apoptosis, a bacterial strategy to enhance colonization of the stomach. Cell Host Microbe 2, 250–263 (2007).
Nagaraja, V. & Eslick, G. D. Systematic review with meta-analysis: the relationship between chronic Salmonella typhi carrier status and gall-bladder cancer. Aliment. Pharmacol. Ther. 39, 745–750 (2014).
Kuijl, C. et al. Intracellular bacterial growth is controlled by a kinase network around PKB/AKT1. Nature 450, 725–730 (2007).
Scanu, T. et al. Salmonella manipulation of host signaling pathways provokes cellular transformation associated with gallbladder carcinoma. Cell Host Microbe 17, 763–774 (2015).
Gur, C. et al. Binding of the Fap2 protein of Fusobacterium nucleatum to human inhibitory receptor TIGIT protects tumors from immune cell attack. Immunity 42, 344–355 (2015).
Kostic, A. D. et al. Fusobacterium nucleatum potentiates intestinal tumorigenesis and modulates the tumor-immune microenvironment. Cell Host Microbe 14, 207–215 (2013).
Gabrilovich, D. I. Myeloid-derived suppressor cells. Cancer Immunol Res 5, 3–8 (2017).
Yan, H. H. et al. Gr-1 + CD11b + myeloid cells tip the balance of immune protection to tumor promotion in the premetastatic lung. Cancer Res 70, 6139–6149 (2010).
Erler, J. T. et al. Hypoxia-induced lysyl oxidase is a critical mediator of bone marrow cell recruitment to form the premetastatic niche. Cancer Cell 15, 35–44 (2009).
Toh, B. et al. Mesenchymal transition and dissemination of cancer cells is driven by myeloid-derived suppressor cells infiltrating the primary tumor. PLoS Biol 9, e1001162 (2011).
Cui, T. X. et al. Myeloid-derived suppressor cells enhance stemness of cancer cells by inducing microRNA101 and suppressing the corepressor CtBP2. Immunity 39, 611–621 (2013).
Sakamoto, Y. et al. Relationship between Fusobacterium nucleatum and antitumor immunity in colorectal cancer liver metastasis. Cancer Sci 112, 4470–4477 (2021).
Zhang, Q. et al. Gut microbiome directs hepatocytes to recruit MDSCs and promote cholangiocarcinoma. Cancer Discov 11, 1248–1267 (2021).
Holokai, L. et al. Increased programmed death-ligand 1 is an early epithelial cell response to Helicobacter pylori Infection. PLoS Pathog 15, e1007468 (2019).
Hezaveh, K. et al. Tryptophan-derived microbial metabolites activate the aryl hydrocarbon receptor in tumor-associated macrophages to suppress anti-tumor immunity. Immunity 55, 324–340.e328 (2022).
Rieber, N. et al. Pathogenic fungi regulate immunity by inducing neutrophilic myeloid-derived suppressor cells. Cell Host Microbe 17, 507–514 (2015).
Sharma, P. C. et al. Recent advances in microbial toxin-related strategies to combat cancer. Semin. Cancer Biol. 86, 753–768 (2022).
Brynestad, S. & Granum, P. E. Clostridium perfringens and foodborne infections. Int. J. Food Microbiol. 74, 195–202 (2002).
Kominsky, S. L. et al. Clostridium perfringens enterotoxin elicits rapid and specific cytolysis of breast carcinoma cells mediated through tight junction proteins claudin 3 and 4. Am. J. Pathol. 164, 1627–1633 (2004).
Romanov, V., Whyard, T. C., Waltzer, W. C. & Gabig, T. G. A claudin 3 and claudin 4-targeted Clostridium perfringens protoxin is selectively cytotoxic to PSA-producing prostate cancer cells. Cancer Lett 351, 260–264 (2014).
Pahle, J. et al. Rapid eradication of colon carcinoma by Clostridium perfringens Enterotoxin suicidal gene therapy. BMC Cancer 17, 129 (2017).
Shrestha, A., Uzal, F. A. & McClane, B. A. The interaction of Clostridium perfringens enterotoxin with receptor claudins. Anaerobe 41, 18–26 (2016).
Mohamed, M. F. et al. Pseudomonas aeruginosa ExoT induces G1 cell cycle arrest in melanoma cells. Cell. Microbiol. 23, e13339 (2021).
Punj, V. et al. Bacterial cupredoxin azurin as an inducer of apoptosis and regression in human breast cancer. Oncogene 23, 2367–2378 (2004).
Tan, W. et al. Targeting of pancreatic cancer cells and stromal cells using engineered oncolytic Salmonella typhimurium. Mol. Ther. 30, 662–671 (2022).
Zhang, Y., Li, Y., Li, H., Chen, W. & Liu, W. Clostridium difficile toxin B recombinant protein inhibits tumor growth and induces apoptosis through inhibiting Bcl-2 expression, triggering inflammatory responses and activating C-erbB-2 and Cox-2 expression in breast cancer mouse model. Biomed. Pharmacother. 101, 391–398 (2018).
Sommer, F. & Bäckhed, F. The gut microbiota-masters of host development and physiology. Nat. Rev. Microbiol. 11, 227–238 (2013).
Miyakawa, M., Iijima, S., Kobayashi, R. & Tajima, M. Observation on the Lymphoid Tissue of the Germ-Free Guinea Pig*. Pathol. Int. 7, 183–210 (1957).
Zhang, Z. et al. Peripheral lymphoid volume expansion and maintenance are controlled by gut microbiota via RALDH + dendritic cells. Immunity 44, 330–342 (2016).
Bouskra, D. et al. Lymphoid tissue genesis induced by commensals through NOD1 regulates intestinal homeostasis. Nature 456, 507–510 (2008).
Legoux, F. et al. Microbial metabolites control the thymic development of mucosal-associated invariant T cells. Science 366, 494–499 (2019).
Yu, L. C. Microbiota dysbiosis and barrier dysfunction in inflammatory bowel disease and colorectal cancers: exploring a common ground hypothesis. J. Biomed. Sci. 25, 79 (2018).
Tanoue, T. et al. A defined commensal consortium elicits CD8 T cells and anti-cancer immunity. Nature 565, 600–605 (2019).
Stewart, O. A., Wu, F. & Chen, Y. The role of gastric microbiota in gastric cancer. Gut Microbes 11, 1220–1230 (2020).
Yang, L. et al. The relative and attributable risks of cardia and non-cardia gastric cancer associated with Helicobacter pylori infection in China: a case-cohort study. Lancet Public Health 6, e888–e896 (2021).
Martinsen, T. C., Fossmark, R. & Waldum, H. L. The phylogeny and biological function of gastric juice-microbiological consequences of removing gastric acid. Int. J. Mol. Sci. 20, 6031 (2019).
Mobley, H. L. The role of Helicobacter pylori urease in the pathogenesis of gastritis and peptic ulceration. Aliment. Pharmacol. Ther. 10(Suppl 1), 57–64 (1996).
Wen, S. & Moss, S. F. Helicobacter pylori virulence factors in gastric carcinogenesis. Cancer Lett 282, 1–8 (2009).
Ansari, S. & Yamaoka, Y. Helicobacter pylori virulence factor cytotoxin-associated gene A (CagA)-mediated gastric pathogenicity. Int. J. Mol. Sci. 21, 7430 (2020).
Odenbreit, S. et al. Translocation of Helicobacter pylori CagA into gastric epithelial cells by type IV secretion. Science 287, 1497–1500 (2000).
Butt, J. & Epplein, M. Helicobacter pylori and colorectal cancer-A bacterium going abroad? PLoS Pathog 15, e1007861 (2019).
Blosse, A. et al. Deregulation of miRNA in Helicobacter pylori-Induced gastric MALT lymphoma: from mice to human. J. Clin. Med. 8, 845 (2019).
Chen, Y., Shi, T., Li, Y., Huang, L. & Yin, D. Fusobacterium nucleatum: the opportunistic pathogen of periodontal and peri-implant diseases. Front. Microbiol. 13, 860149 (2022).
Castellarin, M. et al. Fusobacterium nucleatum infection is prevalent in human colorectal carcinoma. Genome Res 22, 299–306 (2012).
Kostic, A. D. et al. Genomic analysis identifies association of Fusobacterium with colorectal carcinoma. Genome Res 22, 292–298 (2012).
Komiya, Y. et al. Patients with colorectal cancer have identical strains of Fusobacterium nucleatum in their colorectal cancer and oral cavity. Gut 68, 1335–1337 (2019).
Abed, J. et al. Fap2 mediates Fusobacterium nucleatum colorectal adenocarcinoma enrichment by binding to tumor-expressed Gal-GalNAc. Cell Host Microbe 20, 215–225 (2016).
Guo, P. et al. FadA promotes DNA damage and progression of Fusobacterium nucleatum-induced colorectal cancer through up-regulation of chk2. J. Exp. Clin. Cancer Res. 39, 202 (2020).
Ohkusa, T. et al. Induction of experimental ulcerative colitis by Fusobacterium varium isolated from colonic mucosa of patients with ulcerative colitis. Gut 52, 79–83 (2003).
Mazmanian, S. K., Liu, C. H., Tzianabos, A. O. & Kasper, D. L. An immunomodulatory molecule of symbiotic bacteria directs maturation of the host immune system. Cell 122, 107–118 (2005).
Zamani, S. et al. Enterotoxigenic Bacteroides fragilis: a possible etiological candidate for bacterially-induced colorectal precancerous and cancerous lesions. Front Cell Infect Microbiol 9, 449 (2019).
Chung, L. et al. Bacteroides fragilis toxin coordinates a pro-carcinogenic inflammatory cascade via targeting of colonic epithelial cells. Cell Host Microbe 23, 203–214.e205 (2018).
Cao, Y. et al. Enterotoxigenic Bacteroidesfragilis promotes intestinal inflammation and malignancy by inhibiting exosome-packaged miR-149-3p. Gastroenterology 161, 1552–1566.e1512 (2021).
Zhang, M. et al. miR-149-3p reverses CD8(+) T-cell exhaustion by reducing inhibitory receptors and promoting cytokine secretion in breast cancer cells. Open Biol 9, 190061 (2019).
Farrell, P. J. Epstein-Barr virus and cancer. Annu. Rev. Pathol. 14, 29–53 (2019).
Shumilov, A. et al. Epstein-Barr virus particles induce centrosome amplification and chromosomal instability. Nat Commun 8, 14257 (2017).
Wang, J. et al. EBV miRNAs BART11 and BART17-3p promote immune escape through the enhancer-mediated transcription of PD-L1. Nat Commun 13, 866 (2022).
Duan, X. et al. EBV infection in epithelial malignancies induces resistance to antitumor natural killer cells via F3-mediated platelet aggregation. Cancer Res 82, 1070–1083 (2022).
Chou, Y. C., Ho, P. Y., Chen, W. J., Wu, S. H. & Pan, M. H. Lactobacillus fermentum V3 ameliorates colitis-associated tumorigenesis by modulating the gut microbiome. Am. J. Cancer Res. 10, 1170–1181 (2020).
Si, W. et al. Lactobacillus rhamnosus GG induces cGAS/STING- dependent type I interferon and improves response to immune checkpoint blockade. Gut 71, 521–533 (2022).
Zhang, S. L. et al. Lacticaseibacillus paracasei sh2020 induced antitumor immunity and synergized with anti-programmed cell death 1 to reduce tumor burden in mice. Gut Microbes 14, 2046246 (2022).
Wu, H. et al. Lactobacillus reuteri maintains intestinal epithelial regeneration and repairs damaged intestinal mucosa. Gut Microbes 11, 997–1014 (2020).
Cervantes-Barragan, L. et al. Lactobacillus reuteri induces gut intraepithelial CD4(+)CD8alphaalpha(+) T cells. Science 357, 806–810 (2017).
Sivan, A. et al. Commensal Bifidobacterium promotes antitumor immunity and facilitates anti-PD-L1 efficacy. Science 350, 1084–1089 (2015).
Schroeder, B. O. et al. Bifidobacteria or fiber protects against diet-induced microbiota-mediated colonic mucus deterioration. Cell Host Microbe 23, 27–40.e27 (2018).
Verma, R. et al. Cell surface polysaccharides of Bifidobacterium bifidum induce the generation of Foxp3(+) regulatory T cells. Sci. Immunol. 3, 1–14 (2018).
Zagato, E. et al. Endogenous murine microbiota member Faecalibaculum rodentium and its human homologue protect from intestinal tumour growth. Nat. Microbiol. 5, 511–524 (2020).
Li, Q. et al. Streptococcus thermophilus inhibits colorectal tumorigenesis through secreting beta-galactosidase. Gastroenterology 160, 1179–1193.e1114 (2021).
Singh, R. et al. Enhancement of the gut barrier integrity by a microbial metabolite through the Nrf2 pathway. Nat Commun 10, 89 (2019).
Konings, E. J. et al. Folate intake of the Dutch population according to newly established liquid chromatography data for foods. Am. J. Clin. Nutr. 73, 765–776 (2001).
Wasilewska, E., Zlotkowska, D. & Wroblewska, B. Yogurt starter cultures of Streptococcus thermophilus and Lactobacillus bulgaricus ameliorate symptoms and modulate the immune response in a mouse model of dextran sulfate sodium-induced colitis. J. Dairy Sci. 102, 37–53 (2019).
Sakanaka, A. et al. Fusobacterium nucleatum metabolically integrates commensals and pathogens in oral biofilms. mSystems 7, e0017022 (2022).
Shirasawa, Y., Shibahara-Sone, H., Iino, T. & Ishikawa, F. Bifidobacterium bifidum BF-1 suppresses Helicobacter pylori-induced genes in human epithelial cells. J. Dairy Sci. 93, 4526–4534 (2010).
Maubach, G., Vieth, M., Boccellato, F. & Naumann, M. Helicobacter pylori-induced NF-κB: trailblazer for gastric pathophysiology. Trends Mol. Med. 28, 210–222 (2022).
Krautkramer, K. A., Fan, J. & Backhed, F. Gut microbial metabolites as multi-kingdom intermediates. Nat. Rev. Microbiol. 19, 77–94 (2021).
Chattopadhyay, I., Nandi, D. & Nag, A. The pint- sized powerhouse: Illuminating the mighty role of the gut microbiome in improving the outcome of anti- cancer therapy. Semin. Cancer Biol. 70, 98–111 (2021).
Zhang, M., Li, R. W., Yang, H., Tan, Z. & Liu, F. Recent advances in developing butyrogenic functional foods to promote gut health. Crit. Rev. Food Sci. Nutr. 62, 1–22 (2022).
Liu, H. et al. Butyrate: A Double-Edged Sword for Health? Adv. Nutr. 9, 21–29 (2018).
Peng, L., Li, Z. R., Green, R. S., Holzman, I. R. & Lin, J. Butyrate enhances the intestinal barrier by facilitating tight junction assembly via activation of AMP-activated protein kinase in Caco-2 cell monolayers. J. Nutr. 139, 1619–1625 (2009).
Willemsen, L. E., Koetsier, M. A., van Deventer, S. J. & van Tol, E. A. Short chain fatty acids stimulate epithelial mucin 2 expression through differential effects on prostaglandin E(1) and E(2) production by intestinal myofibroblasts. Gut 52, 1442–1447 (2003).
Li, Q. et al. Butyrate suppresses the proliferation of colorectal cancer cells via targeting pyruvate kinase M2 and metabolic reprogramming. Mol. Cell. Proteomics 17, 1531–1545 (2018).
Dmitrieva-Posocco, O. et al. β-Hydroxybutyrate suppresses colorectal cancer. Nature 605, 160–165 (2022).
Li, Y., He, P., Liu, Y., Qi, M. & Dong, W. Combining sodium butyrate with cisplatin increases the apoptosis of gastric cancer in vivo and in vitro via the mitochondrial apoptosis pathway. Front. Pharmacol. 12, 708093 (2021).
Ridlon, J. M. et al. The ‘in vivo lifestyle’ of bile acid 7alpha-dehydroxylating bacteria: comparative genomics, metatranscriptomic, and bile acid metabolomics analysis of a defined microbial community in gnotobiotic mice. Gut Microbes 11, 381–404 (2020).
Ridlon, J. M., Wolf, P. G. & Gaskins, H. R. Taurocholic acid metabolism by gut microbes and colon cancer. Gut Microbes 7, 201–215 (2016).
Fu, T. et al. FXR regulates intestinal cancer stem. Cell Proliferation. Cell 176, 1098–1112.e1018 (2019).
Hang, S. et al. Bile acid metabolites control TH17 and Treg cell differentiation. Nature 576, 143–148 (2019).
Song, X. et al. Microbial bile acid metabolites modulate gut RORgamma(+) regulatory T cell homeostasis. Nature 577, 410–415 (2020).
Lin, R. et al. Deoxycholic acid modulates the progression of gallbladder cancer through N(6)-methyladenosine-dependent microRNA maturation. Oncogene 39, 4983–5000 (2020).
Wyatt, M. & Greathouse, K. L. Targeting dietary and microbial tryptophan-indole metabolism as therapeutic approaches to colon cancer. Nutrients 13, 1189 (2021).
Wang, L. et al. NO(*) /RUNX3/kynurenine metabolic signaling enhances disease aggressiveness in pancreatic cancer. Int. J. Cancer 146, 3160–3169 (2020).
Venkateswaran, N. et al. MYC promotes tryptophan uptake and metabolism by the kynurenine pathway in colon cancer. Genes Dev 33, 1236–1251 (2019).
Thorburn, A. N., Macia, L. & Mackay, C. R. Diet, metabolites, and “western-lifestyle” inflammatory diseases. Immunity 40, 833–842 (2014).
Chen, S. et al. Trimethylamine N-oxide binds and activates PERK to promote metabolic dysfunction. Cell Metab 30, 1141–1151.e1145 (2019).
Xu, R., Wang, Q. & Li, L. A genome-wide systems analysis reveals strong link between colorectal cancer and trimethylamine N-oxide (TMAO), a gut microbial metabolite of dietary meat and fat. BMC Genomics 16(Suppl 7), S4 (2015).
Wang, Z. et al. Non-lethal inhibition of gut microbial trimethylamine production for the treatment of atherosclerosis. Cell 163, 1585–1595 (2015).
Koeth, R. A. et al. Intestinal microbiota metabolism of L-carnitine, a nutrient in red meat, promotes atherosclerosis. Nat. Med. 19, 576–585 (2013).
Chan, C. W. H. et al. Trimethylamine-N-oxide as one hypothetical link for the relationship between intestinal microbiota and cancer—Where we are and where shall we go? J. Cancer 10, 5874–5882 (2019).
Wu, H. et al. The gut microbiota in prediabetes and diabetes: a population-based cross-sectional study. Cell Metab. 32, 379–390.e373 (2020).
Forslund, K. et al. Disentangling type 2 diabetes and metformin treatment signatures in the human gut microbiota. Nature 528, 262–266 (2015).
Koh, A. et al. Microbially produced imidazole propionate impairs insulin signaling through mTORC1. Cell 175, 947–961.e917 (2018).
Koh, A. et al. Microbial imidazole propionate affects responses to metformin through p38gamma-dependent inhibitory AMPK phosphorylation. Cell Metab 32, 643–653.e644 (2020).
Velazquez-Torres, G. et al. Diabetes mellitus type 2 drives metabolic reprogramming to promote pancreatic cancer growth. Gastroenterol Rep (Oxf) 8, 261–276 (2020).
Fuentes-Mattei, E. et al. Effects of obesity on transcriptomic changes and cancer hallmarks in estrogen receptor-positive breast cancer. J. Natl Cancer Inst. 106, 158 (2014).
He, X. et al. Metformin and thiazolidinediones are associated with improved breast cancer-specific survival of diabetic women with HER2 + breast cancer. Ann. Oncol. 23, 1771–1780 (2012).
He, X. X., Tu, S. M., Lee, M. H. & Yeung, S. J. Thiazolidinediones and metformin associated with improved survival of diabetic prostate cancer patients. Ann. Oncol. 22, 2640–2645 (2011).
Mager, L. F. et al. Microbiome-derived inosine modulates response to checkpoint inhibitor immunotherapy. Science 369, 1481–1489 (2020).
Peterson, C. T., Rodionov, D. A., Osterman, A. L. & Peterson, S. N. B Vitamins and their role in immune regulation and cancer. Nutrients 12, 3380 (2020).
Thangaraju, M. et al. GPR109A is a G-protein-coupled receptor for the bacterial fermentation product butyrate and functions as a tumor suppressor in colon. Cancer Res 69, 2826–2832 (2009).
Singh, N. et al. Activation of Gpr109a, receptor for niacin and the commensal metabolite butyrate, suppresses colonic inflammation and carcinogenesis. Immunity 40, 128–139 (2014).
Li, J. et al. Niacin ameliorates ulcerative colitis via prostaglandin D2-mediated D prostanoid receptor 1 activation. EMBO Mol. Med. 9, 571–588 (2017).
Li, K. et al. ILF3 is a substrate of SPOP for regulating serine biosynthesis in colorectal cancer. Cell Res 30, 163–178 (2020).
Choi, H. H. et al. EGF relays signals to COP1 and facilitates FOXO4 degradation to promote tumorigenesis. Adv Sci. 7, 2000681 (2020).
Hosseinkhani, F. et al. The contribution of gut bacterial metabolites in the human immune signaling pathway of non-communicable diseases. Gut Microbes 13, 1–22 (2021).
Li, J., Meng, Y., Wu, X. & Sun, Y. Polyamines and related signaling pathways in cancer. Cancer Cell Int 20, 539 (2020).
Li, L. et al. p53 regulation of ammonia metabolism through urea cycle controls polyamine biosynthesis. Nature 567, 253–256 (2019).
Johnson, C. H. et al. Metabolism links bacterial biofilms and colon carcinogenesis. Cell Metab 21, 891–897 (2015).
Selma, M. V. et al. Isolation of Human Intestinal Bacteria Capable of Producing the Bioactive Metabolite Isourolithin A from Ellagic Acid. Front. Microbiol. 8, 1521 (2017).
He, Z. et al. Campylobacter jejuni promotes colorectal tumorigenesis through the action of cytolethal distending toxin. Gut 68, 289–300 (2019).
Zitvogel, L., Daillere, R., Roberti, M. P., Routy, B. & Kroemer, G. Anticancer effects of the microbiome and its products. Nat. Rev. Microbiol. 15, 465–478 (2017).
Huang, J. et al. Effects of microbiota on anticancer drugs: current knowledge and potential applications. EBioMedicine 83, 104197 (2022).
Rani, V. et al. Human gut microbiome: a new frontier in cancer diagnostics & therapeutics. Curr. Pharm. Des. 27, 4578–4592 (2021).
Gunjur, A. Cancer and the microbiome. Lancet Oncol 21, 888 (2020).
Singh, A. et al. Microbiome and host crosstalk: a new paradigm to cancer therapy. Semin. Cancer Biol. 70, 71–84 (2021).
Lou, X., Chen, Z., He, Z., Sun, M. & Sun, J. Bacteria-mediated synergistic cancer therapy: small microbiome has a big hope. Nanomicro Lett 13, 37 (2021).
Andreeva, N. V., Gabbasova, R. R. & Grivennikov, S. I. Microbiome in cancer progression and therapy. Curr. Opin. Microbiol. 56, 118–126 (2020).
Knippel, R. J., Drewes, J. L. & Sears, C. L. The cancer microbiome: recent highlights and knowledge gaps. Cancer Discov 11, 2378–2395 (2021).
Cheng, W. Y., Wu, C. Y. & Yu, J. The role of gut microbiota in cancer treatment: friend or foe? Gut 69, 1867–1876 (2020).
Zhu, R. et al. Gut microbiota: influence on carcinogenesis and modulation strategies by drug delivery systems to improve cancer therapy. Adv Sci. 8, 2003542 (2021).
Waldman, A. D., Fritz, J. M. & Lenardo, M. J. A guide to cancer immunotherapy: from T cell basic science to clinical practice. Nat. Rev. Immunol. 20, 651–668 (2020).
Reck, M. et al. Pembrolizumab versus chemotherapy for PD-L1-positive non-small-cell lung cancer. N. Engl. J. Med. 375, 1823–1833 (2016).
Robert, C. et al. Nivolumab in previously untreated melanoma without BRAF mutation. N. Engl. J. Med. 372, 320–330 (2015).
Peters, S. et al. First-line nivolumab plus ipilimumab versus chemotherapy in patients with unresectable malignant pleural mesothelioma: 3-year outcomes from CheckMate 743. Ann. Oncol. 33, 488–499 (2022).
Kang, Y. K. et al. Nivolumab plus chemotherapy versus placebo plus chemotherapy in patients with HER2-negative, untreated, unresectable advanced or recurrent gastric or gastro-oesophageal junction cancer (ATTRACTION-4): a randomised, multicentre, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol 23, 234–247 (2022).
Takahashi, M. et al. Nivolumab versus chemotherapy in Japanese patients with advanced esophageal squamous cell carcinoma: a subgroup analysis of a multicenter, randomized, open-label, phase 3 trial (ATTRACTION-3). Esophagus 18, 90–99 (2021).
Chai, Q., Shen, Y., Du, J., Zhu, J. & Wu, B. Economic burden of patients with advanced non-small-cell lung cancer receiving nivolumab versus chemotherapy in China. Immunotherapy 12, 245–254 (2020).
Kato, K. et al. Nivolumab versus chemotherapy in patients with advanced oesophageal squamous cell carcinoma refractory or intolerant to previous chemotherapy (ATTRACTION-3): a multicentre, randomised, open-label, phase 3 trial. Lancet Oncol 20, 1506–1517 (2019).
Larkin, J. et al. Overall survival in patients with advanced melanoma who received nivolumab versus investigator’s choice chemotherapy in CheckMate 037: A Randomized, Controlled, Open-Label Phase III Trial. J. Clin. Oncol. 36, 383–390 (2018).
Weber, J. S. et al. Nivolumab versus chemotherapy in patients with advanced melanoma who progressed after anti-CTLA-4 treatment (CheckMate 037): a randomised, controlled, open-label, phase 3 trial. Lancet Oncol 16, 375–384 (2015).
Powles, T. et al. Pembrolizumab plus axitinib versus sunitinib monotherapy as first-line treatment of advanced renal cell carcinoma (KEYNOTE-426): extended follow-up from a randomised, open-label, phase 3 trial. Lancet Oncol 21, 1563–1573 (2020).
Rini, B. I. et al. Pembrolizumab plus axitinib versus sunitinib for advanced renal-cell carcinoma. N. Engl. J. Med. 380, 1116–1127 (2019).
Overman, M. J. et al. Durable clinical benefit with nivolumab plus ipilimumab in DNA mismatch repair-deficient/microsatellite instability-high metastatic colorectal cancer. J. Clin. Oncol. 36, 773–779 (2018).
Sharma, P., Hu-Lieskovan, S., Wargo, J. A. & Ribas, A. Primary, adaptive, and acquired resistance to cancer immunotherapy. Cell 168, 707–723 (2017).
Gide, T. N., Wilmott, J. S., Scolyer, R. A. & Long, G. V. Primary and acquired resistance to immune checkpoint inhibitors in metastatic melanoma. Clin. Cancer Res. 24, 1260–1270 (2018).
Brahmer, J. R. et al. The Society for Immunotherapy of Cancer consensus statement on immunotherapy for the treatment of non-small cell lung cancer (NSCLC). J Immunother Cancer 6, 75 (2018).
Gandhi, L. et al. Pembrolizumab plus chemotherapy in metastatic non-small-cell lung cancer. N. Engl. J. Med. 378, 2078–2092 (2018).
Rittmeyer, A. et al. Atezolizumab versus docetaxel in patients with previously treated non-small-cell lung cancer (OAK): a phase 3, open-label, multicentre randomised controlled trial. Lancet 389, 255–265 (2017).
Fehrenbacher, L. et al. Atezolizumab versus docetaxel for patients with previously treated non-small-cell lung cancer (POPLAR): a multicentre, open-label, phase 2 randomised controlled trial. Lancet 387, 1837–1846 (2016).
Jin, Y. et al. The diversity of gut microbiome is associated with favorable responses to anti-programmed death 1 immunotherapy in Chinese patients With NSCLC. J. Thorac. Oncol. 14, 1378–1389 (2019).
Rangan, P. & Mondino, A. Microbial short-chain fatty acids: a strategy to tune adoptive T cell therapy. J. Immunother. Cancer 10, e004147 (2022).
Oster, P. et al. Helicobacter pylori infection has a detrimental impact on the efficacy of cancer immunotherapies. Gut 71, 457–466 (2022).
Elkrief, A., Derosa, L., Zitvogel, L., Kroemer, G. & Routy, B. The intimate relationship between gut microbiota and cancer immunotherapy. Gut Microbes 10, 424–428 (2019).
Ochi, N. et al. The effects of antibiotics on the efficacy of immune checkpoint inhibitors in patients with non-small-cell lung cancer differ based on PD-L1 expression. Eur. J. Cancer 149, 73–81 (2021).
Naqash, A. R. et al. The role of gut microbiome in modulating response to immune checkpoint inhibitor therapy in cancer. Ann Transl Med 9, 1034 (2021).
Wei, S. C., Duffy, C. R. & Allison, J. P. Fundamental mechanisms of immune checkpoint blockade therapy. Cancer Discov 8, 1069–1086 (2018).
Gopalakrishnan, V. et al. Gut microbiome modulates response to anti-PD-1 immunotherapy in melanoma patients. Science 359, 97–103 (2018).
Yonekura, S. et al. Cancer induces a stress ileopathy depending on beta-adrenergic receptors and promoting dysbiosis that contributes to carcinogenesis. Cancer Discov 12, 1128–1151 (2022).
York, A. Microbiome: Gut microbiota sways response to cancer immunotherapy. Nat. Rev. Microbiol. 16, 121 (2018).
Morad, G., Helmink, B. A., Sharma, P. & Wargo, J. A. Hallmarks of response, resistance, and toxicity to immune checkpoint blockade. Cell 184, 5309–5337 (2021).
Le, D. T. et al. PD-1 blockade in tumors with mismatch-repair deficiency. N. Engl. J. Med. 372, 2509–2520 (2015).
Le, D. T. et al. Mismatch repair deficiency predicts response of solid tumors to PD-1 blockade. Science 357, 409–413 (2017).
Ayers, M. et al. IFN-gamma-related mRNA profile predicts clinical response to PD-1 blockade. J. Clin. Invest. 127, 2930–2940 (2017).
Griffin, M. E. et al. Enterococcus peptidoglycan remodeling promotes checkpoint inhibitor cancer immunotherapy. Science 373, 1040–1046 (2021).
Bourgin, M., Kepp, O. & Kroemer, G. Immunostimulatory effects of vitamin B5 improve anticancer immunotherapy. Oncoimmunology 11, 2031500 (2022).
Spencer, C. N. et al. Dietary fiber and probiotics influence the gut microbiome and melanoma immunotherapy response. Science 374, 1632–1640 (2021).
Wang, D. D. et al. The gut microbiome modulates the protective association between a Mediterranean diet and cardiometabolic disease risk. Nat. Med. 27, 333–343 (2021).
Andrews, M. C. et al. Gut microbiota signatures are associated with toxicity to combined CTLA-4 and PD-1 blockade. Nat. Med. 27, 1432–1441 (2021).
Coutzac, C. et al. Systemic short chain fatty acids limit antitumor effect of CTLA-4 blockade in hosts with cancer. Nat Commun 11, 2168 (2020).
Leeming, E. R., Johnson, A. J., Spector, T. D. & Le Roy, C. I. Effect of diet on the gut microbiota: rethinking intervention duration. Nutrients 11, 2862 (2019).
Krajmalnik-Brown, R., Ilhan, Z. E., Kang, D. W. & DiBaise, J. K. Effects of gut microbes on nutrient absorption and energy regulation. Nutr. Clin. Pract. 27, 201–214 (2012).
Childs, C. E., Calder, P. C. & Miles, E. A. Diet and immune function. Nutrients 11, 1933 (2019).
Rooks, M. G. & Garrett, W. S. Gut microbiota, metabolites and host immunity. Nat. Rev. Immunol. 16, 341–352 (2016).
Kogut, M. H., Lee, A. & Santin, E. Microbiome and pathogen interaction with the immune system. Poult. Sci. 99, 1906–1913 (2020).
Schubert, M. L., Rohrbach, R., Schmitt, M. & Stein-Thoeringer, C. K. The potential role of the intestinal micromilieu and individual microbes in the immunobiology of chimeric antigen receptor T-cell therapy. Front. Immunol. 12, 670286 (2021).
CD19. CAR T-cell clinical outcome is associated with the gut microbiome. Cancer Discov 12, 1182 (2022).
Uribe-Herranz, M. et al. Gut microbiota modulates adoptive cell therapy via CD8α dendritic cells and IL-12. JCI Insight 3, e94952 (2018).
Smith, M. et al. Gut microbiome correlates of response and toxicity following anti-CD19 CAR T cell therapy. Nat. Med. 28, 713–723 (2022).
Sasako, M. et al. Five-year outcomes of a randomized phase III trial comparing adjuvant chemotherapy with S-1 versus surgery alone in stage II or III gastric cancer. J. Clin. Oncol. 29, 4387–4393 (2011).
Liu, Y. et al. Fusobacterium nucleatum confers chemoresistance by modulating autophagy in oesophageal squamous cell carcinoma. Br. J. Cancer 124, 963–974 (2021).
Lim, Y. et al. Chemoradiation therapy changes oral microbiome and metabolomic profiles in patients with oral cavity cancer and oropharyngeal cancer. Head Neck 43, 1521–1534 (2021).
Daillère, R. et al. Enterococcus hirae and Barnesiella intestinihominis Facilitate Cyclophosphamide-Induced Therapeutic Immunomodulatory Effects. Immunity 45, 931–943 (2016).
Inamura, K. Gut microbiota contributes towards immunomodulation against cancer: new frontiers in precision cancer therapeutics. Semin. Cancer Biol. 70, 11–23 (2021).
Viaud, S. et al. The intestinal microbiota modulates the anticancer immune effects of cyclophosphamide. Science 342, 971–976 (2013).
Alexander, J. L. et al. Gut microbiota modulation of chemotherapy efficacy and toxicity. Nat. Rev. Gastroenterol. Hepatol. 14, 356–365 (2017).
Panebianco, C. et al. Butyrate, a postbiotic of intestinal bacteria, affects pancreatic cancer and gemcitabine response in in vitro and in vivo models. Biomed. Pharmacother. 151, 113163 (2022).
Heshiki, Y. et al. Predictable modulation of cancer treatment outcomes by the gut microbiota. Microbiome 8, 28 (2020).
He, Y. et al. Gut microbial metabolites facilitate anticancer therapy efficacy by modulating cytotoxic CD8(+) T cell immunity. Cell Metab 33, 988–1000.e1007 (2021).
Iida, N. et al. Commensal bacteria control cancer response to therapy by modulating the tumor microenvironment. Science 342, 967–970 (2013).
Petroni, G., Cantley, L. C., Santambrogio, L., Formenti, S. C. & Galluzzi, L. Radiotherapy as a tool to elicit clinically actionable signalling pathways in cancer. Nat. Rev. Clin. Oncol. 19, 114–131 (2022).
Oh, B. et al. The gut microbiome and gastrointestinal toxicities in pelvic radiation therapy: a clinical review. Cancers (Basel) 13, 2353 (2021).
Guo, Y. et al. Effect of Helicobacter pylori on gastrointestinal microbiota: a population-based study in Linqu, a high-risk area of gastric cancer. Gut 69, 1598–1607 (2020).
Poonacha, K. N. T., Villa, T. G. & Notario, V. The interplay among radiation therapy, antibiotics and the microbiota: impact on cancer treatment outcomes. Antibiotics (Basel) 11, 331 (2022).
Gerassy-Vainberg, S. et al. Radiation induces proinflammatory dysbiosis: transmission of inflammatory susceptibility by host cytokine induction. Gut 67, 97–107 (2018).
Reis Ferreira, M. et al. Microbiota- and radiotherapy-induced gastrointestinal side-effects (MARS) study: a large pilot study of the microbiome in acute and late-radiation enteropathy. Clin. Cancer Res. 25, 6487–6500 (2019).
Shiao, S. L. et al. Commensal bacteria and fungi differentially regulate tumor responses to radiation therapy. Cancer Cell 39, 1202–1213.e1206 (2021).
Palamaris, K. et al. Immune checkpoint inhibitors’ associated renal toxicity: a series of 12 cases. J Clin Med 11, 4786 (2022).
Yazbeck, V. et al. An overview of chemotoxicity and radiation toxicity in cancer therapy. Adv. Cancer Res. 155, 1–27 (2022).
Li, W., Deng, X. & Chen, T. Exploring the modulatory effects of gut microbiota in anti-cancer therapy. Front. Oncol. 11, 644454 (2021).
Khan, S. & Gerber, D. E. Autoimmunity, checkpoint inhibitor therapy and immune-related adverse events: a review. Semin. Cancer Biol. 64, 93–101 (2020).
Wang, T. et al. Probiotics lactobacillus reuteri abrogates immune checkpoint blockade-associated colitis by inhibiting group 3 innate lymphoid cells. Front. Immunol. 10, 1235 (2019).
Blake, S. J. et al. The immunotoxicity, but not anti-tumor efficacy, of anti-CD40 and anti-CD137 immunotherapies is dependent on the gut microbiota. Cell Rep Med 2, 100464 (2021).
Akbarali, H. I., Muchhala, K. H., Jessup, D. K. & Cheatham, S. Chemotherapy induced gastrointestinal toxicities. Adv. Cancer Res. 155, 131–166 (2022).
Yue, B., Gao, R., Wang, Z. & Dou, W. Microbiota-host-irinotecan axis: a new insight toward irinotecan chemotherapy. Front Cell Infect Microbiol 11, 710945 (2021).
Kaliannan, K. et al. Decreased tissue omega-6/omega-3 fatty acid ratio prevents chemotherapy-induced gastrointestinal toxicity associated with alterations of gut microbiome. Int. J. Mol. Sci. 23, 5332 (2022).
Roberts, A. B., Wallace, B. D., Venkatesh, M. K., Mani, S. & Redinbo, M. R. Molecular insights into microbial β-glucuronidase inhibition to abrogate CPT-11 toxicity. Mol. Pharmacol. 84, 208–217 (2013).
Bai, J. et al. Gut microbiome and its associations with acute and chronic gastrointestinal toxicities in cancer patients with pelvic radiation therapy: a systematic review. Front. Oncol. 11, 745262 (2021).
Ciorba, M. A. et al. Lactobacillus probiotic protects intestinal epithelium from radiation injury in a TLR-2/cyclo-oxygenase-2-dependent manner. Gut 61, 829–838 (2012).
Delia, P. et al. Use of probiotics for prevention of radiation-induced diarrhea. World J. Gastroenterol. 13, 912–915 (2007).
Touchefeu, Y. et al. Systematic review: the role of the gut microbiota in chemotherapy- or radiation-induced gastrointestinal mucositis - current evidence and potential clinical applications. Aliment. Pharmacol. Ther. 40, 409–421 (2014).
Erawijantari, P. P. et al. Influence of gastrectomy for gastric cancer treatment on faecal microbiome and metabolome profiles. Gut 69, 1404–1415 (2020).
Morris, M. S., Graham, L. A., Chu, D. I., Cannon, J. A. & Hawn, M. T. Oral antibiotic bowel preparation significantly reduces surgical site infection rates and readmission rates in elective colorectal surgery. Ann. Surg. 261, 1034–1040 (2015).
Schardey, H. M. et al. Bacteria: a major pathogenic factor for anastomotic insufficiency. Antimicrob. Agents Chemother. 38, 2564–2567 (1994).
El Bairi, K. et al. Can the microbiota predict response to systemic cancer therapy, surgical outcomes, and survival? The answer is in the gut. Expert Rev. Clin. Pharmacol. 13, 403–421 (2020).
van Praagh, J. B. et al. Mucus microbiome of anastomotic tissue during surgery has predictive value for colorectal anastomotic leakage. Ann. Surg. 269, 911–916 (2019).
van Praagh, J. B. et al. Intestinal microbiota and anastomotic leakage of stapled colorectal anastomoses: a pilot study. Surg. Endosc. 30, 2259–2265 (2016).
Alverdy, J. C., Hyoju, S. K., Weigerinck, M. & Gilbert, J. A. The gut microbiome and the mechanism of surgical infection. Br. J. Surg. 104, e14–e23 (2017).
Sikorska, H. & Smoragiewicz, W. Role of probiotics in the prevention and treatment of meticillin-resistant Staphylococcus aureus infections. Int. J. Antimicrob. Agents 42, 475–481 (2013).
Liu, L. & Shah, K. The potential of the gut microbiome to reshape the cancer therapy paradigm: a review. JAMA Oncol 8, 1059–1067 (2022).
Stripling, J. & Rodriguez, M. Current evidence in delivery and therapeutic uses of fecal microbiota transplantation in human diseases-Clostridium difficile disease and beyond. Am. J. Med. Sci. 356, 424–432 (2018).
Wang, Y. et al. Fecal microbiota transplantation for refractory immune checkpoint inhibitor-associated colitis. Nat. Med. 24, 1804–1808 (2018).
Ianiro, G. et al. Faecal microbiota transplantation for the treatment of diarrhoea induced by tyrosine-kinase inhibitors in patients with metastatic renal cell carcinoma. Nat Commun 11, 4333 (2020).
Nowak, A., Zaklos-Szyda, M., Rosicka-Kaczmarek, J. & Motyl, I. Anticancer potential of post-fermentation media and cell extracts of probiotic strains: An In Vitro Study. Cancers (Basel) 14, 1853 (2022).
Juan, Z. et al. Probiotic supplement attenuates chemotherapy-related cognitive impairment in patients with breast cancer: a randomised, double-blind, and placebo-controlled trial. Eur. J. Cancer 161, 10–22 (2022).
Wei, D. et al. Probiotics for the prevention or treatment of chemotherapy- or radiotherapy-related diarrhoea in people with cancer. Cochrane Database Syst. Rev. 8, Cd008831 (2018).
Mohiuddin, J. J. et al. Association of antibiotic exposure with survival and toxicity in patients with melanoma receiving immunotherapy. J. Natl Cancer Inst. 113, 162–170 (2021).
Ahmed, J. et al. Use of broad-spectrum antibiotics impacts outcome in patients treated with immune checkpoint inhibitors. Oncoimmunology 7, e1507670 (2018).
Secombe, K. R. et al. Antibiotic treatment targeting gram negative bacteria prevents neratinib-induced diarrhea in rats. Neoplasia 30, 100806 (2022).
Sheahan, B. J., Theriot, C. M., Cortes, J. E. & Dekaney, C. M. Prolonged oral antimicrobial administration prevents doxorubicin-induced loss of active intestinal stem cells. Gut Microbes 14, 2018898 (2022).
Hattori, N. et al. Antibiotics suppress colon tumorigenesis through inhibition of aberrant DNA methylation in an azoxymethane and dextran sulfate sodium colitis model. Cancer Sci 110, 147–156 (2019).
Ijssennagger, N. et al. Gut microbiota facilitates dietary heme-induced epithelial hyperproliferation by opening the mucus barrier in colon. Proc. Natl Acad. Sci. USA. 112, 10038–10043 (2015).
Zheng, D. W. et al. Phage-guided modulation of the gut microbiota of mouse models of colorectal cancer augments their responses to chemotherapy. Nat Biomed Eng 3, 717–728 (2019).
Dong, X. et al. Bioinorganic hybrid bacteriophage for modulation of intestinal microbiota to remodel tumor-immune microenvironment against colorectal cancer. Sci Adv 6, eaba1590 (2020).
Yang, J. J. et al. Association of dietary fiber and yogurt consumption with lung cancer risk: a pooled analysis. JAMA Oncol 6, e194107 (2020).
Hashimi, S. M., Xu, T. & Wei, M. Q. Violacein anticancer activity is enhanced under hypoxia. Oncol. Rep. 33, 1731–1736 (2015).
Wu, L., Bao, F., Li, L., Yin, X. & Hua, Z. Bacterially mediated drug delivery and therapeutics: strategies and advancements. Adv. Drug Deliv. Rev. 187, 114363 (2022).
Li, J. et al. Decorating bacteria with triple immune nanoactivators generates tumor-resident living immunotherapeutics. Angew. Chem. Int. Ed. Engl. 61, e202202409 (2022).
Zhang, X. Y. et al. Can dietary nutrients prevent cancer chemotherapy-induced cardiotoxicity? an evidence mapping of human studies and animal models. Front Cardiovasc. Med. 9, 921609 (2022).
Ferrere, G. et al. Ketogenic diet and ketone bodies enhance the anticancer effects of PD-1 blockade. JCI Insight 6, e145207 (2021).
Lévesque, S. et al. A synergistic triad of chemotherapy, immune checkpoint inhibitors, and caloric restriction mimetics eradicates tumors in mice. Oncoimmunology 8, e1657375 (2019).
Pietrocola, F. et al. Caloric restriction mimetics enhance anticancer immunosurveillance. Cancer Cell 30, 147–160 (2016).
Pomatto-Watson, L. C. D. et al. Daily caloric restriction limits tumor growth more effectively than caloric cycling regardless of dietary composition. Nat. Commun. 12, 6201 (2021).
Ligorio, F. et al. Exceptional tumour responses to fasting-mimicking diet combined with standard anticancer therapies: A sub-analysis of the NCT03340935 trial. Eur. J. Cancer 172, 300–310 (2022).
Wedlake, L. et al. Randomized controlled trial of dietary fiber for the prevention of radiation-induced gastrointestinal toxicity during pelvic radiotherapy. Am. J. Clin. Nutr. 106, 849–857 (2017).
Vernieri, C. et al. Fasting-mimicking diet is safe and reshapes metabolism and antitumor immunity in patients with cancer. Cancer Discov 12, 90–107 (2022).
Gibson, G. R. & Roberfroid, M. B. Dietary modulation of the human colonic microbiota: introducing the concept of prebiotics. J. Nutr. 125, 1401–1412 (1995).
Salminen, S. et al. The International Scientific Association of Probiotics and Prebiotics (ISAPP) consensus statement on the definition and scope of postbiotics. Nat. Rev. Gastroenterol. Hepatol. 18, 649–667 (2021).
Marco, M. L. et al. The International Scientific Association for Probiotics and Prebiotics (ISAPP) consensus statement on fermented foods. Nat. Rev. Gastroenterol. Hepatol. 18, 196–208 (2021).
Li, Y. et al. Prebiotic-induced anti-tumor immunity attenuates tumor growth. Cell Rep 30, 1753–1766.e1756 (2020).
Huang, J. et al. Ginseng polysaccharides alter the gut microbiota and kynurenine/tryptophan ratio, potentiating the antitumour effect of antiprogrammed cell death 1/programmed cell death ligand 1 (anti-PD-1/PD-L1) immunotherapy. Gut 71, 734–745 (2022).
Guo, C. et al. Ganoderma lucidum polysaccharide modulates gut microbiota and immune cell function to inhibit inflammation and tumorigenesis in colon. Carbohydr Polym 267, 118231 (2021).
Zhang, Y. et al. Inhibition of pathogen adhesion by bacterial outer membrane-coated nanoparticles. Angew. Chem. Int. Ed. Engl. 58, 11404–11408 (2019).
Xu, J. et al. Yeast-derived nanoparticles remodel the immunosuppressive microenvironment in tumor and tumor-draining lymph nodes to suppress tumor growth. Nat Commun 13, 110 (2022).
Song, Q. et al. A probiotic spore-based oral autonomous nanoparticles generator for cancer therapy. Adv Mater 31, e1903793 (2019).
Aps, L. et al. Bacterial spores as particulate carriers for gene gun delivery of plasmid DNA. J. Biotechnol. 228, 58–66 (2016).
Knecht, L. D., Pasini, P. & Daunert, S. Bacterial spores as platforms for bioanalytical and biomedical applications. Anal. Bioanal. Chem. 400, 977–989 (2011).
Han, Z. Y., Chen, Q. W., Fu, Z. J., Cheng, S. X. & Zhang, X. Z. Probiotic spore-based oral drug delivery system for enhancing pancreatic cancer chemotherapy by gut-pancreas-axis-guided delivery. Nano Lett 22, 8608–8617 (2022).
Minton, N. P. et al. Chemotherapeutic tumour targeting using clostridial spores. FEMS Microbiol. Rev. 17, 357–364 (1995).
Theys, J. et al. Repeated cycles of Clostridium-directed enzyme prodrug therapy result in sustained antitumour effects in vivo. Br. J. Cancer 95, 1212–1219 (2006).
Hibberd, A. A. et al. Intestinal microbiota is altered in patients with colon cancer and modified by probiotic intervention. BMJ Open Gastroenterol 4, e000145 (2017).
Mego, M. et al. Prevention of irinotecan induced diarrhea by probiotics: a randomized double blind, placebo controlled pilot study. Complement. Ther. Med. 23, 356–362 (2015).
Demers, M., Dagnault, A. & Desjardins, J. A randomized double-blind controlled trial: impact of probiotics on diarrhea in patients treated with pelvic radiation. Clin. Nutr. 33, 761–767 (2014).
García-Peris, P. et al. Effect of a mixture of inulin and fructo-oligosaccharide on Lactobacillus and Bifidobacterium intestinal microbiota of patients receiving radiotherapy: a randomised, double-blind, placebo-controlled trial. Nutr. Hosp. 27, 1908–1915 (2012).
Fecal Microbiota Transplant and Pembrolizumab for Men With Metastatic Castration Resistant Prostate Cancer. https://ClinicalTrials.gov/show/NCT04116775.
Probiotics Enhance the Treatment of PD-1 Inhibitors in Patients With Liver Cancer. https://ClinicalTrials.gov/show/NCT05032014.
Preventing Toxicity in Renal Cancer Patients Treated With Immunotherapy Using Fecal Microbiota Transplantation. https://ClinicalTrials.gov/show/NCT04163289.
Oral Probiotics on Radiation Enteritis Stage II Induced by Pelvic Concurrent Chemoradiotherapy. https://ClinicalTrials.gov/show/NCT05032027.
Lin, B. et al. Randomized Clinical Trial: Probiotics Alleviated Oral-Gut Microbiota Dysbiosis and Thyroid Hormone Withdrawal-Related Complications in Thyroid Cancer Patients Before Radioiodine Therapy Following Thyroidectomy. Front. Endocrinol. (Lausanne) 13, 834674 (2022).
Jardim, D. L., Goodman, A., de Melo Gagliato, D. & Kurzrock, R. The challenges of tumor mutational burden as an immunotherapy biomarker. Cancer Cell 39, 154–173 (2021).
Parthasarathy, G. et al. Relationship between microbiota of the colonic mucosa vs feces and symptoms, colonic transit, and methane production in female patients with chronic constipation. Gastroenterology 150, 367–379.e361 (2016).
Eisenhofer, R. et al. Contamination in low microbial biomass microbiome studies: issues and recommendations. Trends Microbiol 27, 105–117 (2019).
Sinha, R. et al. Assessment of variation in microbial community amplicon sequencing by the Microbiome Quality Control (MBQC) project consortium. Nat. Biotechnol. 35, 1077–1086 (2017).
Kurilshikov, A. et al. Large-scale association analyses identify host factors influencing human gut microbiome composition. Nat. Genet. 53, 156–165 (2021).
Manor, O. et al. Health and disease markers correlate with gut microbiome composition across thousands of people. Nat Commun 11, 5206 (2020).
He, Y. et al. Regional variation limits applications of healthy gut microbiome reference ranges and disease models. Nat. Med. 24, 1532–1535 (2018).
Yao, Y. et al. A New Biomarker of Fecal Bacteria for Non-Invasive Diagnosis of Colorectal Cancer. Front Cell Infect Microbiol 11, 744049 (2021).
Microbiota Transplant to Cancer Patients Who Have Failed Immunotherapy Using Faeces From Clinical Responders. https://ClinicalTrials.gov/show/NCT05286294.
Fecal Microbial Transplantation Non-Small Cell Lung Cancer and Melanoma. https://ClinicalTrials.gov/show/NCT04951583.
CBM588, Nivolumab, and Ipilimumab in Treating Patients With Stage IV or Advanced Kidney Cancer. https://ClinicalTrials.gov/show/NCT03829111.
Prebiotics in Rectal Cancer. https://ClinicalTrials.gov/show/NCT05516641.
Effect of Prolonged Nightly Fasting on Immunotherapy Outcomes in HNSCC-Role of Gut Microbiome. https://ClinicalTrials.gov/show/NCT05083416.
Fecal Microbiota Transplantation in Treating Immune-Checkpoint Inhibitor Induced-Diarrhea or Colitis in Genitourinary Cancer Patients. https://ClinicalTrials.gov/show/NCT04038619.
Gut Microbiome Modification Through Dietary Intervention in Patients With Colorectal Cancer: Response to Surgery. https://ClinicalTrials.gov/show/NCT04869956.
Engineering Gut Microbiome to Target Breast Cancer. https://ClinicalTrials.gov/show/NCT03358511.
Probiotics and Breast Health. https://ClinicalTrials.gov/show/NCT03290651.
Using Probiotics to Reactivate Tumor Suppressor Genes in Colon Cancer. https://ClinicalTrials.gov/show/NCT03072641.
The effect of Probiotics on preventing patients with breast cancer from cancer-related cognitive impairmentand and its mechanism. https://www.chictr.org.cn/showproj.aspx?proj=24294
Prevention of Irinotecan Induced Diarrhea by Probiotics. https://ClinicalTrials.gov/show/NCT01410955.
Impact of Probiotics BIFILACT® on Diarrhea in Patients Treated With Pelvic Radiation. https://ClinicalTrials.gov/show/NCT01839721.
Fecal Microbiota Transplantation in Diarrhea Induced by Tyrosine-kinase Inhibitors. https://ClinicalTrials.gov/show/NCT04040712.
Action of Synbiotics on Irradiated GI Mucosa in Rectal Cancer Treatment. https://ClinicalTrials.gov/show/NCT03420443.
Mixture of Prebiotics on Intestinal Microbiota of Patients Receiving Abdominal Radiotherapy. https://ClinicalTrials.gov/show/NCT01549782.
Acknowledgements
This work was supported by the National Natural Science Foundation of China, No. 82102998, No. 82072688; Sichuan Science and Technology Program, No. 2021YFS0111. The views expressed are those of the authors and not necessarily those of the NSF, the Sichuan Science and Technology Program. We thank Pro. Weixi Xiong for her substantial contribution on the English editing in this paper. We apologize for not being able to cite all the publications related to this topic due to space constraints of the journal.
Author information
Authors and Affiliations
Contributions
L-Y.Z. and J-X.M. contributed equally to this work; the conception and design of the study: J-K.H., L-Y.Z.; acquisition of data from published papers: L-Y.Z., J-X.M., G.Y., W-H.Z., K.Y., L.L., D.K.; analysis and interpretation of data: L-Y.Z., J-X.M., L-X.C., K.L.; manuscript preparation and manuscript editing: L-Y.Z., J-X.M., manuscript review and corresponding author: J-K.H., K.Y.
Corresponding authors
Ethics declarations
Competing interests
The authors no competing interests.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Zhao, LY., Mei, JX., Yu, G. et al. Role of the gut microbiota in anticancer therapy: from molecular mechanisms to clinical applications. Sig Transduct Target Ther 8, 201 (2023). https://doi.org/10.1038/s41392-023-01406-7
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41392-023-01406-7
- Springer Nature Limited