
Abstract
The κ-opioid receptor (KOP-r) system and its endogenous ligands, the dynorphins, are involved in the neurobiological regulation of addictive states, and of mood. There are limited data on the impact of selective KOP-r antagonism in humans on basic biobehavioral functions, or on addictive diseases and mood disorders. Previously studied selective KOP-r antagonists have unusual pharmacodynamic and pharmacokinetic properties (slow development of KOP-r selectivity, extremely long duration of action) that limit translation to human studies. A recently developed selective KOP-r-antagonist, Opra Kappa (LY2456302; CERC-501), has medication-like duration of action, oral bioavailability, and target engagement. The current study is the first investigation of the effects of a KOP-r-antagonist in cocaine-dependent persons in comparison with normal volunteers. In a stress-minimized inpatient setting, we determined the neuroendocrine and neurobehavioral effects of repeated administration of an active dose of Opra Kappa (10 mg p.o. daily, four consecutive days in comparison with an initial baseline day). Healthy volunteers (n=40), persons diagnosed with cocaine dependence in early abstinence (<2 months, EACD) (n=23), and drug-free former cocaine-dependent persons (7-month to 25-year abstinence, DFFCD) (n=7) were studied, with measurements including circulating neuroendocrine hormones, affect, and, in cocaine-dependent persons, cocaine craving. Modest adverse events related to Opra Kappa included pruritus, observed in a subset of individuals. No significant change was observed in serum prolactin levels following Opra Kappa administration, but modest increases in circulating adrenocorticotropic hormone and cortisol were observed. No significant changes were noted in measures of depression or cocaine craving in this stress-minimized setting. Overall, these studies demonstrate that effects of 10 mg Opra Kappa are largely consistent with those predicted for a selective KOP-r antagonist. This medication regimen was tolerable, and is therefore feasible for further studies in cocaine-dependent persons.
Similar content being viewed by others
Introduction
In 2014, there were an estimated 1.5 million current (past-month) cocaine users aged ⩾12 year, which is ∼0.6% of the population, in the United States. Data from the 2011 Drug Abuse Warning Network (DAWN) report showed that cocaine was involved in 505 224 of the nearly 1.3 million visits to emergency departments for illicit drug misuse or abuse, translating to ∼40% of drug misuse or abuse-related emergency department visits that involved cocaine (SAMHSA, 2013).
In spite of intensive efforts, no medication for reducing cocaine use disorders has been approved (Czoty et al, 2016; Kreek et al, 2002; Montoya and Vocci, 2008). Long-term cocaine exposure causes changes in several molecular end points in experimental animals, including changes in levels of components of the endogenous opioid system, in particular κ-opioid receptors (KOP-r) and their endogenous agonist neuropeptides, the dynorphins, in brain areas involved in reward, mood, and anxiety (Daunais et al, 1993; Fagergren et al, 2003; Spangler et al, 1993; Staley et al, 1997; Unterwald et al, 1994). Similar changes have been observed in postmortem brain of humans with cocaine abuse or dependence (Hurd and Herkenham, 1993; Staley et al, 1997). Similar changes in KOP-r/dynorphin function have been noted in response to experimental stress in animals, resulting in depressant-like behavioral effects (Donahue et al, 2015; Reed et al, 2012). A recent human PET study has also determined that human brain KOP-r populations are affected in persons with transdiagnostic symptoms of trauma, including signs of anhedonia or dysphoria and anxiety (Pietrzak et al, 2014).
Exogenous administration of ‘unbiased’ KOP-r agonists is known to cause aversion, sedation/anhedonia, and depressant-like effects in animals, and dose-dependent dysphoria and psychotomimetic/hallucinogenic effects in humans (Bals-Kubik et al, 1993; Pfeiffer et al, 1986; Zhang et al, 2005). Activation of the KOP-r/dynorphin system is also a major counterregulatory mechanism to basal dopaminergic function, and also to cocaine-induced changes thereto (Di Chiara and Imperato, 1988; Spanagel et al, 1990; Thompson et al, 2000; Van't Veer et al, 2013; Zhang et al, 2004).
KOP-r antagonists have been recently proposed, based on mechanistic neurochemical and pharmacological data, to be potential pharmacotherapeutics for a range of conditions related to stress dysfunction and hedonic states (Carlezon and Krystal, 2016). For instance, such compounds have been shown to decrease stress-induced reinstatement of drug taking in preclinical species (Beardsley et al, 2005; Zhou et al, 2013). Therefore, KOP-r ligands with limited pharmacodynamic efficacy (ie, KOP-r antagonists or appropriate partial agonists) are potential pharmacotherapeutic targets as medications for cocaine use disorders, and comorbid conditions including depression and anxiety (Butelman et al, 2012). Until very recently, the selective KOP-r antagonists available (eg, nor-BNI) were compounds with extremely long duration of action (several days to weeks) (Broadbear et al, 1994; Butelman et al, 1993), as well as delayed onset of KOP-r antagonism. A phase I clinical trial with another long-acting KOP-r antagonist, JDTic, was suspended after 2 of the 6 subjects who received this compound experienced a single, asymptomatic event of multiple beats of nonsustained ventricular tachycardia (NSVT), as identified by direct cardiologist reads of 24 h Holter monitor strips (Buda et al, 2015). Overall, the aforementioned properties of previously studied KOP-r antagonists was the impetus to develop novel small-molecule selective KOP-r antagonists with more commonly seen ‘medication-like’ properties (Chang et al, 2011; Rorick-Kehn et al, 2014).
The compound studied here, LY2456302 (now known as CERC-501) and referred to by the Lilly group informally as ‘Opra Kappa,’ is a small-molecule KOP-r antagonist (with ~30-fold selectivity for KOP-r vs MOP-r, ~200-fold vs DOP-r, as determined using radioligand binding in membranes prepared from HEK or CHO cells heterologously expressing human KOP-r, MOP-r, or DOP-r, with [3H]diprenorphine as the radioligand) (Rorick-Kehn et al, 2014). Opra Kappa was previously studied in phase I studies in single ascending doses (2–60 mg per os (p.o.), 1 dose/day separated by at least 7 days of washout, n=21), and in repeated daily doses for consecutive days (2, 10, or 35 mg p.o. for 14 consecutive days; n=9, 10, and 9, for the 2, 10, and 35 mg doses respectively) (Lowe et al, 2014). One subject experienced NSVT at a 25 mg dose; no subjects receiving the higher 60 mg dose experienced NSVT. This compound demonstrated appropriate safety properties, pharmacokinetics, and oral bioavailability.
This is the first study on the effects of a selective KOP-r antagonist in humans diagnosed with cocaine dependence, or any other addictive or psychiatric disease. The selection of Opra Kappa dose was guided by the findings from a PET study, indicating that a 10 mg p.o. acute dose was sufficient to occupy >90% of brain KOP-r receptors (Naganawa et al, 2015). Opra Kappa doses of >10 mg were concluded to have decreased KOP-r to MOP-r selectivity (Rorick-Kehn et al, 2015). In this study, the 10 mg p.o. dose of Opra Kappa was administered for four consecutive days in persons with cocaine-dependence diagnoses and compared to healthy volunteers in a stress-minimized inpatient setting.
Materials and methods
History
Following discussions with Eli Lilly in September 2013, a protocol was designed to test Opra Kappa in healthy volunteers and persons with a history of cocaine dependence at the Rockefeller University Hospital. An application to the Food and Drug Administration (FDA) for use of Opra Kappa as an investigational new drug (IND) was approved in May 2014. Simultaneously, this protocol received approval from the institutional review board (IRB) at Rockefeller University in May 2014. Eli Lilly agreed to gift 5 mg capsules for this study upon approvals. The first patient was enrolled in September 2014 and the last patient in February 2017.
Study Drug
The drug investigated in these studies, Opra Kappa, also referred to as LY2456302 [(S)-3-fluoro-4-(4-((2 (3,5-dimethylphenyl)pyrrolidin-1-yl)methyl)phenoxy) benzamide], was synthesized using Good Manufacturing Practice by Eli Lilly (Indianapolis, IN) as 5 mg capsules and stored in blister packages, as required by the FDA (Almac, Souderton, PA). On each of study days 2–5, 2 5 mg capsules (ie, a 10 mg dose) were administered orally at the 0 min timepoint (between 0900 and 1000 h).
Subjects
The volunteers were recruited from the general population within the New York City tristate area using a variety of methods: Rockefeller University IRB-approved flyers and advertisements, self-referral via website, recommendation from other participants, or referrals by clinicians with knowledge of our study. All participants were eligible if they were between 18 and 65 years of age and were able to read, understand, and provide written, dated informed consent in English. Exclusion criteria are listed in detail in Supplementary Table S1.
A telephone screen was conducted by one of the nurse practitioners, and included information on major acute diseases, medications, and current illicit or licit substance use and abuse including alcohol. Potential subjects were then met in person with the same clinician in the Rockefeller outpatient clinic for subject characterization and ascertainment. A written informed consent was obtained from each subject before any study procedures were conducted.
Screening for all participants included a medical, psychiatric, comprehensive substance abuse history, sexual history, physical exam, laboratory testing, and electrocardiogram (EKG). Laboratory testing included Helicobacter pylori stool antigen testing, complete blood cell counts, chemistries, endocrine tests, hepatitis serologies, and an HIV test. Urine toxicology was obtained from all our study subjects to determine the presence of mixed opiates, methadone, cocaine metabolites, benzodiazepines, and cannabis at each visit in the clinic. Urine toxicology does not include hallucinogens (eg, LSD, PCP, salvinorin A), but subjects were queried on these by the clinicians. All volunteers were required to have 24 h urine collections for daily monitoring while in the inpatient unit. All of the toxicology reports are confidentially maintained. All participants, whether they were healthy volunteers or those with substance abuse histories, underwent an extensive ascertainment of their substance abuse and mental health history before being considered for this study. Tools used in that screening process were: the Structured Clinical Interview for DSM-IV Axis 1 Disorders (SCID-I) (First et al, 2002), the Kreek–McHugh–Schluger–Kellogg (KMSK) Scale (Kellogg et al, 2003), the Beck Depression Inventory-II (BDI-II) (Beck et al, 1996), the Addiction Severity Index (ASI) (McLellan et al, 1980), and the Fagerstrom Test for Nicotine Dependence (Fagerstrom and Schneider, 1989).
A total of 70 participants were eligible to participate, and were initially stratified into the following three groups: healthy volunteers (HVs), cocaine-dependent participants in early abstinence (EACD, 24 h to 2 months), and drug-free former cocaine-dependent participants (DFFCD, drug-free for ⩾6 months). Participants were categorized as healthy volunteers if they had no history of substance dependence, and no current history of substance abuse in the past 6 months. Subjects were determined to have current or former cocaine dependence based upon a clinical interview, with DSM IV diagnosis and past or current pattern of either daily cocaine use or ⩾2 cocaine binges per week, for a period of 6 months. Six months of use is the time required for DSM-IV diagnosis; our criteria of daily use or 2 binges per week is more stringent than DSM-IV criteria. In addition, cocaine-dependent subjects who had current alcohol or opiate abuse were excluded.
Exclusion criteria
Individuals were excluded if they: (1) had an active psychotic disorder or current active DSM-IV axis I disorder other than substance use disorder as determined through clinical interview, (2) were HIV-1 positive, (3) had uncompensated liver disease such as ascites or coagulopathy, (4) weighed <50 kg, (5) had a sustained diastolic blood pressure >90 mm Hg, (6) had hemoglobin <10 g/dl, (7) were pregnant, (8) were sexually active female subjects with child-bearing potential who are unable or unwilling to use effective methods of birth control 2 weeks before and 2 weeks after study medication administration, (9) male subjects sexually active with females, and who are unable or unwilling to use effective methods of birth control 2 weeks after study medication administration, (10) were taking medications that are primarily metabolized by CYP2C8 at least 7 days before the study, (11) had H. pylori antigen-positive or active gastric diseases, such as peptic ulcer disease, or (12) were cigarette smokers and unwilling or unable to either abstain from smoking or use nicotine replacement therapy (Supplementary Table S1). Of the cocaine groups, 18 of 23 EACD subjects and 3 of 7 DFFCD subjects were cigarette smokers. Of healthy volunteers, 4 of 40 were smokers. All of the subjects who smoked either successfully abstained (18 of 25 total cigarette smokers) or used nicotine replacement (patch, 5 of 25; lozenge, 2 of 25) during the study.
Procedures
Subjects were admitted for a 5-day inpatient study at the Rockefeller University Hospital. Subjects were admitted the night before the first study day to attain stress minimization. Upon admission, all subjects completed the BDI-II (Beck et al, 1996), and for subjects currently smoking nicotine products, the Fagerstrom Test for Nicotine Dependence (FTND). In addition, subjects with current or past cocaine dependence completed the Cocaine Craving Questionnaire (CCQ). Subjects fasted beginning at 00:00 h of each day of the study, were awakened at approximately 06:00 h, had a low-fat breakfast between 07:00 and 07:30 h, and remained nil per os until 3 h after medication administration.
The first study day was a baseline in which no medication was given, but all procedures were performed to determine baseline levels, including determination of stress hormones, adrenocorticotropic hormone (ACTH), cortisol, and prolactin, as well as responses in subject-reported measures. On study days 2–5, a daily dose of Opra Kappa (10 mg) was administered orally between 09:00 and 10:00 h. All experiments were conducted at approximately the same time of day. Before administration of study medication, an updated sexual history and serum pregnancy test was obtained for female subjects of child-bearing capacity.
Neuroendocrine measures
On study day 1 (baseline), study day 2, and study day 5, ACTH, cortisol, and prolactin were measured from blood samples taken at −30, 0, +60, +120, +180, +240, and +480 min timepoints via an intravenous line placed at least 30 min before the first timepoint.
Subject-reported behavioral measures
All subjects were administered BDI-II on study days (−30 and +480 min timepoints), visual analog scales (VAS; 10 cm long) for mood effects (ranging from ‘terrible’ to ‘terrific’), and a similar VAS scale for Drug effects (ranging from ‘Cold Turkey’ to ‘High’). In addition, subjects with current or prior cocaine dependence diagnoses (CD) also completed a VAS for Craving (ranging from ‘none’ to ‘extremely intense’), as well as the Cocaine Craving Questionnaire (CCQ-Now) on each test day (−30 and +120, +240, and +480 min timepoints).
We incorporated several elements requested by the FDA during initial protocol review. Measures of liver function (AST, ALT, and coagulation studies) were obtained at screening (∼1 week before inpatient admission) and also upon discharge (+480 min timepoint on study day 5). To monitor potential events after discharge, all participants had either an in-person or telephone assessment by the same admitting nurse practitioner within ∼1 week of discharge. A small number of subjects did not complete the study; in no case was lack of retention due to effects of the study drug (see Supplementary Table S2 for list of reasons for early discharge).
Neuroendocrine Assays
For each assay, samples from study days 1, 2, and 5 of each subject were run concurrently and control serum was analyzed in parallel.
Serum prolactin
Prolactin levels were quantified in our Laboratory using a commercially available radioimmunoassay (MP Biomedicals, Santa Ana, CA). For quality control, identical, pooled samples (separate from all subject samples) were run in quadruplicate, with duplicates at the start and end of every assay to be used in calculating intra- and interassay coefficients of variability (% CVs; 8.4 and 12.5, respectively). Each radioimmunoassay sampling timepoint was run in duplicate, with the average value being used for quantitation. In cases where the duplicate values deviated by >15%, the sample data were discarded, and additional collected serum for this timepoint was reanalyzed. In rare cases, serum prolactin levels for specific timepoints could not be obtained because of unavailability of additional serum sample.
Plasma ACTH
ACTH levels, sampled at each of the timepoints described above in the Procedures section, were measured in our Laboratory using a commercially available radioimmunoassay (DiaSorin, Saluggia, IT), according to the manufacturer’s instructions. Plasma ACTH was measured for the first 34 subjects enrolled in the study (16 normal volunteers, 18 subjects with a history of cocaine dependence). During the course of this study, the ACTH radioimmunoassay provided by Diasorin was discontinued, and for reasons of expense, as well as concern about comparison of data using technology with different ACTH antibodies, we did not examine ACTH levels in the remaining 36 subjects. For quality control, identical, pooled samples (separate from all subject samples) were run in quadruplicate, with duplicates at the start and end of every assay to be used in calculating intra- and interassay coefficients of variability (%CVs; 7.5 and 12.0, respectively). Each radioimmunoassay sampling timepoint was run in duplicate, with the average value being used for quantitation. In cases where the duplicate values deviated by >15%, the timepoint was discarded, and additional collected plasma for this timepoint was reanalyzed.
Serum cortisol
Cortisol levels were determined in serum samples at each timepoint by the Clinical Chemistry Service at the Department of Laboratory Medicine of Memorial Sloan Kettering Cancer Center, through its standing agreement with the Rockefeller University Hospital. Measurements are conducted with an automated immunoassay analyzer (AIA 360, Tosoh Bioscience, South San Francisco, CA). Intra-assay CVs reported for cortisol for this assay range from 2.5 to 3.1%, and inter-assay CVs range from 4.7 to 5.1%.
Statistical Analysis
Given the low number of subjects in the DFFCD group, we analyzed only the HV group and the EACD group in all comparisons. DFFCD group data are presented in the Supplementary Materials. For neuroendocrine measures, area under the curve (AUC) (0–480 min after administration of Opra Kappa) was calculated and used for statistical analysis. For prolactin, given the pronounced sex differences in circulating levels and biological regulation of this hormone, males and females were separated for analysis. For ACTH and cortisol, on the other hand, subjects of both sexes were grouped together for analyses. In order to determine whether there was any effect of cocaine-dependence history on the effect of Opra Kappa, a two-way repeated measures ANOVA (group × day, 3 measurements at days 1, 2, and 5) was applied to probe differences in the primary outcomes (levels of the hormone markers and total scores from questionnaires) among the groups. For each hormonal assay, only subjects for whom all timepoints were available on all three days were included.
Results
Safety and Tolerability
Adverse events
Reports of adverse events were mild and did not require intervention, with pruritus, mostly confined to distal body parts, being the most commonly reported (see Table 1). The mood changes that occurred were generally modestly positive (eg, sensations of ‘well-being,’ feeling ‘focused’, or ‘relaxed’), with similar representation among the HV, EACD, and DFFCD groups, suggesting no apparent relationship to cocaine use history. Gastrointestinal side effects were mainly described as discomfort, and four patients experienced nausea (with no vomiting or diarrhea). Over half of patients experienced a mild side effect from Opra Kappa at some point during their 4 days of receiving a dose (~60%). Side effects generally occurred equally throughout study days, although the highest number of side effects occurred on the first day of study medication. A total of 10 patients out of 70 experienced more than one side effect on a single study day, and these 10 patients account for more than half of the overall number of side effects experienced.
Subjects not completing study
One patient, a 27-year-old female healthy volunteer, was discharged because of an unanticipated side effect on the first day of receiving 10 mg Opra Kappa; she developed a rash on her thighs, neck, torso, and knees with a corresponding itch and there was concern for an allergy. She responded well to topical hydrocortisone, a single oral dose of an antihistamine, was observed for 1 day, and discharged. Descriptions of the 10 patients who did not complete the study, mainly because of i.v. access issues, are listed in the Supplementary Table S2.
Vital signs
No significant changes were observed in vital signs (systolic blood pressure, heart rate) or liver enzyme function (AST, ALT, coagulation).
Nicotine replacement
Of the 25 cigarette lifetime smokers in this study (4 HV, 18 EACD, and 3 DFFCD, Table 2), 7 opted for nicotine replacement therapy (7–14 mg nicotine patch or 4 mg lozenges) (1 HV, 5 EACD, and 1 DFFCD).
Neuroendocrine Results
Serum prolactin
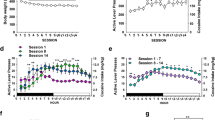
The response of serum prolactin was analyzed separately by gender. The daily time course of prolactin over the 3 days of measurement (baseline, day 1; 1st Opra Kappa, day 2; 4th Opra Kappa, day 5) are shown for male healthy volunteers and male EACD subjects (Figure 1a and b). AUCs, from 0 to 480 min following Opra Kappa administration, were examined using a two-way ANOVA, drug use history × day, with repeated measures by day (Figure 1c). There was no significant effect of drug history, no effect of day, and no drug history × day interaction. Similarly, the daily time courses of prolactin are shown for female healthy volunteers and female EACD subjects (Figure 1d and e). AUCs, from 0 to 480 min following Opra Kappa administration, were examined using a two-way ANOVA, drug use history × day, with repeated measures by day (Figure 1f). There was no significant effect of drug history, no effect of day, and no drug history × day interaction, indicating that in neither males nor females did Opra Kappa have an effect on prolactin release. The time courses of prolactin in DFFCD males and females are shown in Supplementary Figures S1 and S2, respectively.

Serum prolactin levels determined in subjects at predetermined timepoints from samples obtained over a range of 30 min before to 480 min after administration of 10 mg/kg Opra Kappa (or the corresponding time on baseline day 0). (a) Time course of serum prolactin levels in male HVs (n=24). (b) Time course of serum prolactin levels in male EACD subjects (n=19). (c) Area under the curve, from 0 to 480 min with respect to Opra Kappa administration, for male HV subjects (n=24) and EACD subjects (n=18). (d) Time course of serum prolactin levels in female HVs (n=16). (e) Time course of serum prolactin levels in female EACD subjects (n=4). (f) Area under the curve, from 0 to 480 min with respect to Opra Kappa administration, for female HV subjects (n=16) and EACD subjects (n=4). No statistically significant difference across days or drug use history were observed for serum prolactin levels.
Plasma ACTH
The response of plasma ACTH was analyzed with males and females together, given that we observed no differences in baseline levels or AUC across sex in healthy volunteers (analysis not shown). The daily time course of ACTH over the 3 days of measurement (baseline, day 1; 1st Opra Kappa, day 2; 4th Opra Kappa, day 5) are shown for healthy volunteers and EACD subjects (Figure 2a and b). AUCs, from 0 to 480 min following Opra Kappa administration, were examined with a two-way ANOVA, drug use history × day, with repeated measures by day (Figure 2c). There was a significant effect of drug history (F(1, 27) =10.9, p<0.005) and a significant effect of day (F(2, 54) =7.3, p<0.005), but no significant interaction of drug history × day. Newman–Keuls post hoc test revealed that days 2 and 5 of Opra Kappa exhibited significantly enhanced ACTH AUC over baseline day (p<0.05), with no difference between days 2 and 5. The time course of ACTH in DFFCD subjects is shown in Supplementary Figure S3.

Plasma ACTH levels determined in subjects at predetermined time points from samples obtained over a range of 30 min before to 480 min after administration of 10 mg/kg Opra Kappa (or the corresponding time on baseline day 1). (a) Time course of plasma ACTH levels in combined male and female healthy volunteers (n=16) on day 1 of study (baseline day), day 2 of study (day 1 of Opra Kappa administration), and day 5 of study (day 4 of Opra Kappa administration). (b) Time course of plasma ACTH levels in combined male and female EACD subjects (n=14) on day 1 of study (baseline day), day 2 of study (day 1 of Opra Kappa administration), and day 5 of study (day 4 of Opra Kappa administration). (c) Area under the curve, from 0 to 480 min with respect to OpRA Kappa administration, for HV subjects (n=16) and EACD subjects (n=13).
Serum cortisol
The response of serum cortisol was analyzed with males and females together, given that we observed no differences in baseline levels or AUC across sex in healthy volunteers (analysis not shown). The daily time course of cortisol over the 3 days of measurement (baseline, day 1; 1st Opra Kappa, day 2; 4th Opra Kappa, day 5) are shown for healthy volunteers and EACD subjects (Figure 3a and b). AUCs, from 0 to 480 min following Opra Kappa administration, were examined using a two-way ANOVA, drug use history × day, with repeated measures by day (Figure 3c). There was a significant effect of drug history (F(1, 58) =10.9, p<0.005) and a significant effect of day (F(2, 116)=16.89, p<0.0001), but no significant interaction of drug history × day. Newman–Keuls post hoc test revealed that days 2 and 5 of Opra Kappa exhibited significantly enhanced cortisol AUC over baseline day (p<0.0005). The time course of cortisol in DFFCD subjects is shown in Supplementary Figure S3.

Serum cortisol levels determined in subjects at predetermined timepoints from samples obtained over a range of 30 min before to 480 min after administration of 10 mg/kg Opra Kappa (or the corresponding time on baseline day 1). (a) Time course of serum cortisol levels in combined male and female healthy volunteers (n=40) on day 1 of study (baseline day), day 2 of study (day 1 of Opra Kappa administration), and day 5 of study (day 4 of Opra Kappa administration). (b) Time course of serum cortisol levels in combined male and female EACD subjects (n=23) on day 1 of study (baseline day), day 2 of study (day 1 of Opra Kappa administration), and day 5 of study (day 4 of Opra Kappa administration). (c) Area under the curve, from 0 to 480 min with respect to Opra Kappa administration, for HV subjects (n=39) and EACD subjects (n=23).
Subject-Reported Measures
We present below data for healthy volunteers vs the EACD group, as described above. A summary of statistical comparisons is presented in the Supplementary Materials (Supplementary Table S3). Data for the smaller DFFCD group (n=7 total) were not analyzed, and are presented in Supplementary Materials (Supplementary Table S4).
BDI-II scores
In the morning of the baseline day, BDI-II scores for HV were predominantly 0 (mean=0.2; SEM=0.07). For the EACD group, BDI-II scores were higher (mean 2.3; SEM=0.7), but still considerably below the score indicative of minimal depression (ie, 13). Nevertheless, BDI-II scores for HV in the morning of the baseline day (day 1) were lower than for CD (Mann–Whitney test, U=290; p<0.003; Table 3 and Supplementary Table S3).
Morning and afternoon BDI-II scores were compared for days 1, 2, and 5 using Friedman’s ANOVAs. All these ANOVAs, for both HV and EACD, were nonsignificant, indicating no change in BDI-II scores across study days (Table 3 and Supplementary Table S3).
VAS scales for mood
In the morning of the baseline day, at time −30 min, VAS mood scores (0 to 10; ‘terrible’ to ‘terrific’) were slightly higher for HV (mean =7.5; 95% CL ±0.6) than for EACD (mean=7.0; 95% CL ±0.9) (Table 3 and Supplementary Table S3).
A two-way (study day × time of day) repeated measures ANOVA for HV found no main effects, but a significant interaction F(6, 234)=3.09. Tukey’s post hoc tests detected only differences at time −30 min (ie, predrug scores), with small decreases at day 2 and day 5, as compared with the baseline day. A similar ANOVA for EACD yielded no significant main effects or interaction (Table 3 and Supplementary Table S3).
VAS scales for drug effect in EACD
Baseline values for the drug VAS (10 cm; from ‘Cold Turkey’ to ‘High’) measured at time −30 min on the baseline day were intermediate (mean 4.9; 95% CL ±0.3). A two-way (study day × time of day) repeated measures ANOVA detected only an interaction between study day × time (F(6, 96)=2.21; p<0.05). The post hoc Dunnett’s tests detected that the +240 timepoint on Opra Kappa day 2 and the +480 timepoint on Opra Kappa day 5 were each smaller than their respective score on the baseline day. Overall, the magnitude of the changes for VAS ‘Drug’ scores across days was modest (Table 3 and Supplementary Table S3).
VAS scales for craving in EACD
Baseline values for the craving VAS (10 cm; from ‘None’ to ‘Extremely Intense’) measured at time −30 min on the baseline were relatively low. They had a mean value of 2.8 (CL±1.1) and did not change appreciably at later times on the baseline day. A two-way (study day × time of day) repeated measures ANOVA did not detect any significant main effect or interaction (Table 3 and Supplementary Table S3).
CCQ-Brief in EACD
The CCQ-brief scale ranges from 1 to 7 (low to high craving score). Scores for the CCQ-brief at time −30 min on the baseline day had a mean value of 2.2 (95% CL±0.4) and did not change appreciably through the day. A two-way (study day × time of day) repeated measures ANOVA detected only a main effect of study day (F(2, 40)=5.43; p<0.01) and no main effect of time of day or interaction. Dunnett’s post hoc test detected that CCQ-Brief scores were lower on Opra Kappa day 5, compared with baseline day 1 (Supplementary Table S3 and Supplementary Figure S5). We also plotted CCQ scores for each individual EACD subject on the first day of Opra Kappa dosing (day 2 of the study) (Supplementary Figure S6). There were no robustly observable trends that emerged.
Discussion
This is the first report of a selective KOP-r antagonist in persons with a history of cocaine dependence (n=30) as compared with HVs (n=40). We determined the effect of Opra Kappa in a group of EACD (n=23) and compared them with the effects in healthy volunteers (n=40). We also have examined a small group of cocaine-dependent subject with more extended abstinence from cocaine (7 months to 25 years), DFFCD (n=7). Our statistical analyses compare the HV and EACD groups, with data for the smaller DFFCD presented for comparison in the Supplementary Materials (the results are qualitatively very similar for DFFCD group compared with the EACD group). As indicated in the introduction there have been numerous studies indicating changes in the dynorphin/KOP-r system shortly after chronic cocaine in both animals and humans (see, eg, Hurd and Herkenham, 1993; Unterwald et al, 1994), corresponding to the EACD group studied here. It should be noted that with regard to extended abstinence, there is only some evidence in rodents of changes in dynorphin/KOP-r (Bailey et al, 2007).
Safety/Feasibility
All of the individual side effects experienced by patients were in the mild-to-moderate category and there were no severe adverse events. Pruritus was an expected effect of Opra Kappa; it was typically experienced distally, on hands and feet, and was short-lived (<30 min). This adverse event, although not reported in the prior study of effects of Opra Kappa in human subjects following single administration but reported in 3 of 9 subjects given repeated administrations of 35 mg/kg Opra Kappa (Lowe et al, 2014), is possibly target (KOP-r) mediated. The KOP-r agonist nalfurafine has been shown to be clinically effective in treating pruritus, and is approved in Japan for this use (Eastwood et al, 2017). In rodent models, some KOP-r antagonists have been shown to induce pruritus, although this pruritogenic effect may not be directly mediated through KOP-r (Cowan et al, 2015; Dimattio et al, 2014). In this study, pruritus was not associated with erythema in all but two instances, and resolved without intervention.
Neuroendocrine Profile
The previous study of the safety and tolerability for Opra Kappa (Lowe et al, 2014) reported no clinically significant changes in neuroendocrine hormones (prolactin, luteinizing hormone, ACTH, cortisol). There was an indication that cortisol 24- h ‘mean ratio of change’ was increased following dosing with 10 or 35 mg Opra Kappa on day 1 of repeated administration, but the effect sizes were not reported. There was no indication that females and males were analyzed separately for prolactin and luteinizing hormone levels (possibly because of low n for females) (Lowe et al, 2014). The current study has a larger number of both males and females, allowing for separate gender analysis of prolactin levels, as appropriate (Kreek et al, 1999). The current study clearly demonstrated no effect of Opra Kappa on prolactin levels, as reflected by no change in AUC on days 1 and 4 of Opra Kappa administration, and no change in serum levels at the −30 and 0 min timepoints on day 4 of administration (study day 5) compared with study days 1 and 2 (Figure 1).
However, we observed a significant increase in the AUC of both ACTH and cortisol over the time course of 0–480 min on both days 1 and 4 of Opra Kappa administration, compared with the baseline day (Figures 2 and 3). Examination of the time-course curves indicates that the levels of ACTH and cortisol are higher at timepoints corresponding to expected peak levels of Opra Kappa (2–3 h following administration; Lowe et al, 2014). This increase in HPA hormones is not expected for a selective κ-antagonist. For instance, the selective κ-antagonist norBNI caused no alteration of cortisol at 24 h after treatment in primates, at a time when it causes selective KOP-r antagonism (Williams et al, 2003). The slight increase in ACTH and cortisol levels at the time of peak plasma Opra Kappa levels may indicate a modest amount of MOP-r antagonism, as naloxone and other MOP-r antagonists are well known to cause HPA activation in humans (Schluger et al, 1998). A prior study on blockade of fentanyl-induced pupil miosis suggested that doses of Opra Kappa >10 mg had some MOP-r antagonist effects 2 h following oral administration (Rorick-Kehn et al, 2015).
For the two HPA axis hormones, ACTH and cortisol, there was an effect of cocaine history on baseline levels and AUC, with increased levels observed in the group with history of cocaine dependence (Figures 2 and 3). However, there is no indication that Opra Kappa had a differential effect on HPA axis responsivity in persons with a history of cocaine dependence vs healthy volunteers (Figures 2 and 3). The underlying mechanistic source of the elevations in baseline ACTH and cortisol levels in persons with a history of cocaine dependence compared with healthy volunteers is not known, and may involve changes at the levels of the endogenous regulation of ACTH release in response to stress, including the corticotropin-releasing factor (CRF)/CRHR1 system and/or the vasopressin/V1b receptor system. Previous reports of cortisol levels during abstinence from cocaine have indicated increases or no change in comparison with normal volunteers (see, eg, Mendelson et al, 1988; Vescovi et al, 1992).
Subject-Reported Effects
Administration of an active dose of LY2456302 for 4 consecutive days only had slight or no effect on subject-reported measures in both HV and EACD. Scores on the Beck Depression Inventory were unchanged after 4 consecutive days of Opra Kappa administration as compared with baseline. In addition, ‘mood’ VAS scores were unchanged at all postdrug times in both HV and EACD. Similarly, Opra Kappa resulted in no significant changes in the scores on the ‘drug’ VAS scale as compared with the baseline day. Overall, the above data indicate that repeated active doses of Opra Kappa had only subtle, if any, effects on subjective states in both HV and EACD in a stress-minimized setting.
A VAS scale measuring craving per se in CD also detected no effect of Opra Kappa as compared with the baseline day. Cocaine craving scores assessed by the CCQ-Brief questionnaire declined in days 2 and 5 as compared with the baseline day. However, there was no interaction between day of study and time of day, and therefore it is likely that this slight decline is because of the prolonged exposure to a stress-minimized environment in CD.
These findings overall suggest that the KOP-r/dynorphin ‘tone’ is low in systems that subserve the aforementioned subject-reported measures, under stress-minimized conditions, even in CD. Future studies could determine whether Opra Kappa would have a discernible effect in participants with higher baseline dysphoria, craving, or BDI-II scores, or in persons exposed to environmental stressors. Of interest, a recent study using a close analog of Opra Kappa, LY2224496 (also known as FP3FBZ; Melief et al, 2011) was able to significantly decrease anxiety-like and depression-like effects observed in rats after chronic (14 day) extended access (18 h/day) cocaine self-administration, but not in the absence of cocaine self-administration (Valenza et al, 2017). The effects of short-acting selective KOR antagonists on cocaine self-administration in animal models have yet to be reported, with studies in progress in our laboratory.
Conclusion
Opra Kappa, at an oral dose of 10 mg, which has previously been shown to result in substantial occupancy of central nervous system KOP-r receptors for >24 h, has been administered to healthy volunteers and subjects with a history of cocaine dependence, with 4 daily repeated administrations. The dose of 10 mg has been shown to be safe, with modest side effects, including pruritus, both likely because of on-target drug effects at KOP-r in a small subset of individuals. Adverse effects overall were similarly modest. The spectrum or frequency of side effects does not appear to be related to a history of cocaine dependence. There were no substantial changes caused by Opra Kappa, as measured in the Beck Depression Inventory or cocaine craving scales (CCQ) or craving VAS, in subjects with a history of cocaine dependence. It should be noted that Beck Depression scores and CCQ craving measures were relatively low under these stress-minimized conditions before Opra Kappa administration. With regard to neuroendocrine measures, the absence of any effect of circulating prolactin levels is consistent with those expected for a KOP-r antagonist, with negligible agonist efficacy at KOP-r (Bart et al, 2005). However, statistically significant increases in circulating ACTH and cortisol suggest there may be modest antagonism of MOP-r at this dose (Schluger et al, 1998). Overall, these results suggest that Opra Kappa is safe for studies of clinical efficacy in substance abuse and mood disorders, but caution should be exercised for administration in subjects with MOP-r -agonist dependence, as moderate MOP-r antagonism may result in precipitated withdrawal. Further studies with this novel medication in cocaine (as well as other psychostimulants and alcohol) use disorders are therefore warranted.
Funding and disclosure
The authors declare no conflict of interest.
References
Substance Abuse and Mental Health Services Administration. Drug Abuse Warning Network: 2011: National Estimates of Drug-Related Emergency Department Visits. HHS Publication No. United States Department of Health and Human Services, Rockville, MD, 2013: 13-4760.
Bailey A, Gianotti R, Ho A, Kreek MJ (2007). Downregulation of kappa-opioid receptors in basolateral amygdala and septum of rats withdrawn for 14 days from an escalating dose "binge" cocaine administration paradigm. Synapse (New York, NY) 61: 820–826.
Bals-Kubik R, Ableitner A, Herz A, Shippenberg TS (1993). Neuroanatomical sites mediating the motivational effects of opioids as mapped by the conditioned place preference paradigm in rats. J Pharmacol Exp Ther 264: 489–495.
Bart G, Schluger JH, Borg L, Ho A, Bidlack JM, Kreek MJ (2005). Nalmefene induced elevation in serum prolactin in normal human volunteers: partial kappa opioid agonist activity? Neuropsychopharmacology 30: 2254–2262.
Beardsley PM, Howard JL, Shelton KL, Carroll FI (2005). Differential effects of the novel kappa opioid receptor antagonist, JDTic, on reinstatement of cocaine-seeking induced by footshock stressors vs cocaine primes and its antidepressant-like effects in rats. Psychopharmacology 183: 118–126.
Beck AT, Steer RA, Ball R, Ranieri W (1996). Comparison of Beck Depression Inventories -IA and -II in psychiatric outpatients. J Pers Assess 67: 588–597.
Broadbear JH, Negus SS, Butelman ER, de Costa BR, Woods JH (1994). Differential effects of systemically administered nor-binaltorphimine (nor-BNI) on kappa-opioid agonists in the mouse writhing assay. Psychopharmacology 115: 311–319.
Buda JJ, Ivy Carroll F, Kosten TR, Swearingen D, Walters BB (2015). A double-blind, placebo-controlled trial to evaluate the safety, tolerability, and pharmacokinetics of single, escalating oral doses of JDTic. Neuropsychopharmacology 40: 2059–2065.
Butelman ER, Negus SS, Ai Y, de Costa BR, Woods JH (1993). Kappa opioid antagonist effects of systemically administered nor-binaltorphimine in a thermal antinociception assay in rhesus monkeys. J Pharmacol Exp Ther 267: 1269–1276.
Butelman ER, Yuferov V, Kreek MJ (2012). kappa-opioid receptor/dynorphin system: genetic and pharmacotherapeutic implications for addiction. Trends Neurosci 35: 587–596.
Carlezon WA Jr., Krystal AD (2016). Kappa-opioid antagonists for psychiatric disorders: from bench to clinical trials. Depress Anxiety 33: 895–906.
Chang C, Byon W, Lu Y, Jacobsen LK, Badura LL, Sawant-Basak A et al (2011). Quantitative PK-PD model-based translational pharmacology of a novel kappa opioid receptor antagonist between rats and humans. AAPS J 13: 565–575.
Cowan A, Kehner GB, Inan S (2015). Targeting Itch with ligands selective for kappa opioid receptors. Handb Exp Pharmacol 226: 291–314.
Czoty PW, Stoops WW, Rush CR (2016). Evaluation of the "pipeline" for development of medications for cocaine use disorder: a review of translational preclinical, human laboratory, and clinical trial research. Pharmacol Rev 68: 533–562.
Daunais JB, Roberts DC, McGinty JF (1993). Cocaine self-administration increases preprodynorphin, but not c-fos, mRNA in rat striatum. Neuroreport 4: 543–546.
Di Chiara G, Imperato A (1988). Opposite effects of mu and kappa opiate agonists on dopamine release in the nucleus accumbens and in the dorsal caudate of freely moving rats. J Pharmacol Exp Ther 244: 1067–1080.
Dimattio KM, Yakovleva TV, Aldrich JV, Cowan A, Liu-Chen LY (2014). Zyklophin, a short-acting kappa opioid antagonist, induces scratching in mice. Neurosci Lett 563: 155–159.
Donahue RJ, Landino SM, Golden SA, Carroll FI, Russo SJ, Carlezon WA Jr (2015). Effects of acute and chronic social defeat stress are differentially mediated by the dynorphin/kappa-opioid receptor system. Behav Pharmacol 26: 654–663.
Eastwood B, Strang J, Marsden J (2017). Effectiveness of treatment for opioid use disorder: a national, five-year, prospective, observational study in England. Drug Alcohol Depend 176: 139–147.
Fagergren P, Smith HR, Daunais JB, Nader MA, Porrino LJ, Hurd YL (2003). Temporal upregulation of prodynorphin mRNA in the primate striatum after cocaine self-administration. Eur J Neurosci 17: 2212–2218.
Fagerstrom KO, Schneider NG (1989). Measuring nicotine dependence: a review of the Fagerstrom Tolerance Questionnaire. J Behav Med 12: 159–182.
First MB, Spitzer RL, Gibbon M, Williams JBW (2002) Structured Clinical Interview for DSM-IV-TR Axis I Disorders, Research Version, Patient edition (SCID-I/P; version 2.0). Biometrics Research Department, State Psychiatric Institute: New York.
Hurd YL, Herkenham M (1993). Molecular alterations in the neostriatum of human cocaine addicts. Synapse (New York, NY) 13: 357–369.
Kellogg SH, McHugh PF, Bell K, Schluger JH, Schluger RP, LaForge KS et al (2003). The Kreek-McHugh-Schluger-Kellogg scale: a new, rapid method for quantifying substance abuse and its possible applications. Drug Alcohol Depend 69: 137–150.
Kreek MJ, LaForge KS, Butelman E (2002). Pharmacotherapy of addictions. Nat Rev Drug Discov 1: 710–726.
Kreek MJ, Schluger J, Borg L, Gunduz M, Ho A (1999). Dynorphin A1-13 causes elevation of serum levels of prolactin through an opioid receptor mechanism in humans: gender differences and implications for modulation of dopaminergic tone in the treatment of addictions. J Pharmacol Exp Ther 288: 260–269.
Lowe SL, Wong CJ, Witcher J, Gonzales CR, Dickinson GL, Bell RL et al (2014). Safety, tolerability, and pharmacokinetic evaluation of single- and multiple-ascending doses of a novel kappa opioid receptor antagonist LY2456302 and drug interaction with ethanol in healthy subjects. J Clin Pharmacol 54: 968–978.
McLellan AT, Luborsky L, Woody GE, O'Brien CP (1980). An improved diagnostic evaluation instrument for substance abuse patients. The Addiction Severity Index. J Nerv Ment Dis 168: 26–33.
Melief EJ, Miyatake M, Carroll FI, Beguin C, Carlezon WA, Cohen BM et al (2011). Duration of action of a broad range of selective kappa opioid receptor antagonists is positively correlated with c-Jun N-terminal kinase-1 activation. Mol Pharmacol 80: 920–929.
Mendelson JH, Teoh SK, Lange U, Mello NK, Weiss R, Skupny A et al (1988). Anterior pituitary, adrenal, and gonadal hormones during cocaine withdrawal. Am J Psychiatry 145: 1094–1098.
Montoya ID, Vocci F (2008). Novel medications to treat addictive disorders. Curr Psychiatry Rep 10: 392–398.
Naganawa M, Dickinson GL, Zheng MQ, Henry S, Vandenhende F, Witcher J et al (2015). Receptor occupancy of the kappa opioid antagonist LY2456302 measured with PET and the novel radiotracer 11C-LY2795050. J Pharmacol Exp Ther 356: 260–6.
Pfeiffer A, Brantl V, Herz A, Emrich HM (1986). Psychotomimesis mediated by kappa opiate receptors. Science (New York, NY) 233: 774–776.
Pietrzak RH, Naganawa M, Huang Y, Corsi-Travali S, Zheng MQ, Stein MB et al (2014). Association of in vivo kappa-opioid receptor availability and the transdiagnostic dimensional expression of trauma-related psychopathology. JAMA Psychiatry 71: 1262–1270.
Reed B, Fang N, Mayer-Blackwell B, Chen S, Yuferov V, Zhou Y et al (2012). Chromatin alterations in response to forced swimming underlie increased prodynorphin transcription. Neuroscience 220: 109–118.
Rorick-Kehn LM, Witcher JW, Lowe SL, Gonzales CR, Weller MA, Bell RL et al (2015). Determining pharmacological selectivity of the kappa opioid receptor antagonist LY2456302 using pupillometry as a translational biomarker in rat and human. Int J Neuropsychopharmacol 18: pyu036.
Rorick-Kehn LM, Witkin JM, Statnick MA, Eberle EL, McKinzie JH, Kahl SD et al (2014). LY2456302 is a novel, potent, orally-bioavailable small molecule kappa-selective antagonist with activity in animal models predictive of efficacy in mood and addictive disorders. Neuropharmacology 77: 131–144.
Schluger JH, Ho A, Borg L, Porter M, Maniar S, Gunduz M et al (1998). Nalmefene causes greater hypothalamic-pituitary-adrenal axis activation than naloxone in normal volunteers: implications for the treatment of alcoholism. Alcohol Clin Exp Res 22: 1430–1436.
Spanagel R, Herz A, Shippenberg TS (1990). The effects of opioid peptides on dopamine release in the nucleus accumbens: an in vivo microdialysis study. J Neurochem 55: 1734–1740.
Spangler R, Unterwald EM, Kreek MJ (1993). 'Binge' cocaine administration induces a sustained increase of prodynorphin mRNA in rat caudate-putamen. Brain Res Mol Brain Res 19: 323–327.
Staley JK, Rothman RB, Rice KC, Partilla J, Mash DC (1997). Kappa2 opioid receptors in limbic areas of the human brain are upregulated by cocaine in fatal overdose victims. J Neurosci 17: 8225–8233.
Thompson AC, Zapata A, Justice JB Jr, Vaughan RA, Sharpe LG, Shippenberg TS (2000). Kappa-opioid receptor activation modifies dopamine uptake in the nucleus accumbens and opposes the effects of cocaine. J Neurosci 20: 9333–9340.
Unterwald EM, Rubenfeld JM, Kreek MJ (1994). Repeated cocaine administration upregulates kappa and mu, but not delta, opioid receptors. Neuroreport 5: 1613–1616.
Valenza M, Butelman ER, Kreek MJ (2017). Effects of the novel relatively short-acting kappa opioid receptor antagonist LY2444296 in behaviors observed after chronic extended-access cocaine self-administration in rats. Psychopharmacology 234: 2219–2231.
Van't Veer A, Bechtholt AJ, Onvani S, Potter D, Wang Y, Liu-Chen LY et al (2013). Ablation of kappa-opioid receptors from brain dopamine neurons has anxiolytic-like effects and enhances cocaine-induced plasticity. Neuropsychopharmacology 38: 1585–97.
Vescovi PP, Coiro V, Volpi R, Passeri M (1992). Diurnal variations in plasma ACTH, cortisol and beta-endorphin levels in cocaine addicts. Horm Res 37: 221–224.
Williams KL, Ko MC, Rice KC, Woods JH (2003). Effect of opioid receptor antagonists on hypothalamic-pituitary-adrenal activity in rhesus monkeys. Psychoneuroendocrinology 28: 513–528.
Zhang Y, Butelman ER, Schlussman SD, Ho A, Kreek MJ (2004). Effect of the endogenous kappa opioid agonist dynorphin A(1-17) on cocaine-evoked increases in striatal dopamine levels and cocaine-induced place preference in C57BL/6J mice. Psychopharmacology 172: 422–429.
Zhang Y, Butelman ER, Schlussman SD, Ho A, Kreek MJ (2005). Effects of the plant-derived hallucinogen salvinorin A on basal dopamine levels in the caudate putamen and in a conditioned place aversion assay in mice: agonist actions at kappa opioid receptors. Psychopharmacology 179: 551–558.
Zhou Y, Leri F, Grella S, Aldrich J, Kreek MJ (2013). Involvement of dynorphin and kappa opioid receptor in yohimbine-induced reinstatement of heroin seeking in rats. Synapse (New York, NY) 67: 358–361.
Acknowledgements
We thank Elizabeth Ducat and the late Brenda Ray for clinical assessments and other duties performed for the early conduct of this study. We thank research assistants Konrad Ben, Alexandra Dunn, Jose Erazo, and Catherine Guariglia for technical assistance, sample collection, and sample processing. We gratefully acknowledge the Clinical Chemistry Service within the Department of Laboratory Medicine of Memorial Sloan Kettering for providing services for the measurement of serum cortisol. We thank Eli Lilly for providing the compound LY2456302, especially Andrew Dahlem, Linda Rohrick-Kehn, and Sitra Tauscher-Wisniewski for help in procuring this compound as well as protocol approval from Lilly. Funding was generously provided by a grant from the Dr. Miriam O. and Sheldon G. Adelson Medical Research Foundation. We also gratefully acknowledge support from the NIH-CTSA grant to the Rockefeller University Hospital (1UL1TR001866).
Author information
Authors and Affiliations
Corresponding author
Additional information
Supplementary Information accompanies the paper on the Neuropsychopharmacology website
Supplementary information
Rights and permissions
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 4.0 International License. The images or other third party material in this article are included in the article's Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
About this article

Cite this article
Reed, B., Butelman, E., Fry, R. et al. Repeated Administration of Opra Kappa (LY2456302), a Novel, Short-Acting, Selective KOP-r Antagonist, in Persons with and without Cocaine Dependence. Neuropsychopharmacol. 43, 739–750 (2018). https://doi.org/10.1038/npp.2017.205
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/npp.2017.205
- Springer Nature Switzerland AG
This article is cited by
-
Co-targeting the kappa opioid receptor and dopamine transporter reduces motivation to self-administer cocaine and partially reverses dopamine system dysregulation
Scientific Reports (2024)
-
Efficacy and safety of aticaprant, a kappa receptor antagonist, adjunctive to oral SSRI/SNRI antidepressant in major depressive disorder: results of a phase 2 randomized, double-blind, placebo-controlled study
Neuropsychopharmacology (2024)
-
Reprogramming the tumor microenvironment by genome editing for precision cancer therapy
Molecular Cancer (2022)
-
Novel Pharmacological Agents for the Treatment of Cocaine Use Disorder
Current Behavioral Neuroscience Reports (2022)
-
Improving translation of animal models of addiction and relapse by reverse translation
Nature Reviews Neuroscience (2020)