
Abstract
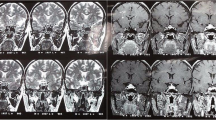
We describe two young men with cystic pituitary enlargement on magnetic resonance imaging (MRI) causing hypopituitarism. The first patient presented acutely unwell with headache and vomiting associated with anterior and posterior pituitary dysfunction. The second patient presented with hypopituitarism after a long history of hypogonadism. In both cases yellow/brown fluid was found at surgery and histological examination revealed inflammatory infiltrate with foamy histiocytes, lymphocytes and multinucleated giant cells containing cholesterol clefts. Full recovery of pituitary function occurred after surgery in the first but not the second patient. The first case is the first documented case of xanthomatous hypophysitis with recovery of pituitary function following surgery. The cases differed in duration of disease, as indicated by the long history of symptoms, the histological finding of marked fibrosis and the lack of recovery of pituitary function in the second. Xanthomatous pituitary lesions categorized in the literature as xanthomatous hypophysitis, xanthogranulomatous hypophysitis and xanthogranuloma of the sellar region have overlapping histological features. Our two cases revealed histological features that do not fit completely into any of the categories but share features of all three. These findings suggest that the various xanthomatous lesions of the sellar region may be a spectrum of a common inflammatory process rather than distinct pathological entities.
Similar content being viewed by others


References
Folkerth RD, Price DL Jr, Schwartz M, Black PM, De Girolami U. Xanthomatous hypophysitis. Am J Surg Pathol 1998;22:736–741.
Wright AR, Hermann RC, Parisi JE. Neurological manifestations of Erdheim-Chester disease. J Neurol Neurosurg Psychiatry 1999;66:72–75.
Paulus W, Honegger J, Keyvani K, Fahlbusch R. Xanthogranuloma of the sellar region; a clinicopathological entity different from adamantinomatous craniopharyngioma. Acta Neuropathol (Berl) 1999;97:371–382.
Cheung CC, Ezzat S, Smyth HS, Asa SL. The spectrum and significance of primary hypophysitis. J Clin Endocrinol Metab 2001;86:1048–1053.
Deodhare SS, Bilbao JM, Kovacs K et al. Xanthomatous hypophysitis: A novel entity of obscure etiology. Endocrine Pathology 1999;10:237–241.
Tashiro T, Sano T, Xu B et al. Spectrum of different types of hypophysitis: A clinicopathologic study of hypophysitis in 31 cases. Endocrine Pathology 2002;13:183–195.
Sano T, Kovacs K, Scheithauer BW, Rosenblum MK, Petito CK, Greco CM. Pituitary pathology in acquired immunodeficiency syndrome. Arch Pathol Lab Med 1989;113:1066–1070.
Bullmann C, Faust M, Hoffmann A et al. Five cases with central diabetes insipidus and hypogonadism as first presentation of neurosarcoidosis. Eur J Endocrinol 2000;142:365–372.
Lohr KM, Ryan LM, Toohill RJ, Anderson T. Anterior pituitary involvement in Wegener's granulomatosis. J Rheumatol 1988;15:855–857.
Vadakekalem J, Stamos T, Shenker Y. Sometimes the hooves do belong to zebras! An unusual case of hypopituitarism. J Clin Endocrinol Metab 1995;80:17–20.
Toth M, Szabo P, Racz K et al. Granulomatous hypophysitis associated with Takayasu's disease. Clin Endocrinol (Oxf) 1996;45:499–503.
De Bruin W, van't Verlaat J, Graamans K, De Bruin T. Sellar granulomatous mass in a pregnant woman with active Crohn's disease. Neth J Med 1991;39:136–141.
Kelly WF, Bradey N, Scoones D. Rosai-Dorfman disease presenting as a pituitary tumour. Clin Endocrinol (Oxf) 1999;50:133–137.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Burt, M.G., Morey, A.L., Turner, J.J. et al. Xanthomatous Pituitary Lesions: A Report of Two Cases and Review of the Literature. Pituitary 6, 161–168 (2003). https://doi.org/10.1023/B:PITU.0000011177.43408.56
Issue Date:
DOI: https://doi.org/10.1023/B:PITU.0000011177.43408.56