
Abstract
Summary. Objective: To prospectively evaluate right atrial refractoriness and sustained atrial fibrillation (AF) inducibility at programmed electrical stimulation in two groups of patient: a series of patients with chronic persistent AF, studied immediately after successful low energy internal atrial cardioversion, and a group of control patients without history of supraventricular arrhythmias.
Patients: Nineteen patients with chronic persistent AF (mean AF duration 11 ± 10 months, range 2–61 months) submitted to successful internal low energy atrial cardioversion in fully conscious state and 11 control patients without history of supraventricular arrhythmias.
Methods: An electrophysiological evaluation was performed to measure atrial refractoriness and AF inducibility, by delivering single atrial extrastimuli in high right atrium, at decremental coupling, during spontaneous sinus rhythm and after 8 beats at 600, 500, 400 and 330 ms cycle length. If sustained AF was induced the protocol was terminated.
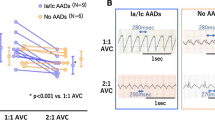
Results: During programmed atrial stimulation sustained AF was induced in 8 out 19 (42%) of the AF patients but in none of the control group. Atrial effective refractory period was significantly shorter in AF patients compared to controls both at basic cycle length, at 600 ms, 500 ms and 400 ms cycle length, meanwhile no statistically significant differences were found at 330 ms cycle length. An altered relationship between atrial effective refractory period and cycle length was found in AF patients compared to controls: the slope of linear correlation slope was significantly lower in AF group than in controls (0.04 ± 0.07 vs 0.17 ± 0.10, p < 0.002).
Conclusions: Marked abnormalities of atrial refractoriness and of its heart rate relationship are observed after internal cardioversion of chronic persistent AF in humans and these abnormalities are associated with an high vulnerability to AF. These observations may explain the high risk of AF recurrences in the early phases following successful cardioversion. In this scenario antiarrhythmic drug therapy seems to be mandatory for reducing arrhythmia relapses.
Similar content being viewed by others

References
Lown B, Amarasingham R, Neumann J. New method for terminating cardiac arrhythmias. JAMA 1962;182:548–555.
Rossi M, Lown B. The use of quinidine in cardioversion. Am J Cardiol 1967;19:234–238.
Van Gelder IC, Crijns HJ, Van Gilst WH, Verwer R, Lie KI. Prediction of uneventful cardioversion and maintenance of sinus rhythm from direct-current electrical cardioversion of chronic atrial fibrillation or flutter. Am J Cardiol 1991;68:41–46.
Wijffels MCEF, Kirchof CJHJ, Dorland R, Allessie MA. Atrial fibrillation begets atrial fibrillation: A study in awake chronically instrumented goats. Circulation 1995;92:1954–1968.
Daoud EG, Bogun F, Harvey M, Man KC, Strickberger SA, Morady F. Effect of atrial fibrillation on atrial refractoriness in humans. Circulation 1996;94:1600–1606.
Kumagai K, Akimitsu S, Kawahira K, Kawanami F, Yamanouchi Y, Hiroki T, Arakawa K. Electrophysiological properties in chronic lone atrial fibrillation. Circulation 1991;84:1662–1668.
Levy S, Ricard P, Gueunoun M, Yapo F, Trigano J, Mansouri C, Paganelli F. Low energy cardioversion of spontaneous atrial fibrillation: Immediate and long term results. Circulation 1997;96:253–259.
Boriani G, Biffi M, Bronzetti G, Ayers GM, Zannoli R, Branzi A, Capucci A, Magnani B. Efficacy and tolerability in fully conscious patients of transvenous low energy internal atrial cardioversion for atrial fibrillation. Am J Cardiol 1998;81:241–244.
Attuel P, Childers R, Cauchemez B, Poveda J, Mugica J, Coumel P. Failure in rate adaptation of the atrial refractory period: Its relationship to vulnerability. Int J Cardiol 1982;2:179–197.
Bianconi L, Mennuni M, Lukic V, Castro A, Chieffi M, Santini M. Effects of oral propafenone administration before electrical cardioversion of chronic atrial fibrillation: A placebo controlled study. J Am Coll Cardiol 1996;28:700–706.
Josephson ME. Clinical Cardiac Electrophysiology, 2nd ed. Philadelphia: Lea and Febiger, 1993:22–70.
Luck JC, Engel TR. Dispersion of atrial refractoriness in patients with sinus node dysfunction. Circulation 1979;60:404–412.
Cosio FG, Palacios J, Vidal JM, Cocina EG, Gomez-Sanchez MA, Tamargo L. Electrophysiologic studies in atrial fibrillation. Slow conduction of premature impulses: A possible manifestation of the background for reentry. Am J Cardiol 1983;51:122–130.
Capucci A Biffi M, Boriani G, Ravelli F, Nollo G, Sabbatani P, Orsi C, Magnani B. The dynamic electrophysiologic behaviour of human atria during paroxysmal atrial fibrillation. Circulation 1995;92:1193–1202.
Denes P, Wu D, Dhingra R, Pietras RJ, Rosen KM. The effects of cycle length on cardiac refractory periods in man. Circulation 1974;49:32–41.
Pandozi C, Bianconi L, Villani M, Gentilucci G, Castro A, Altamura G, Jesi AP, Lamberti F, Ammirati F, Santini M. Electrophysiological characteristics of the human atria after cardioversion of persistent atrial fibrillation. Circulation 1998;25:2860–2865.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Boriani, G., Biffi, M., Zannoli, R. et al. Evaluation of Atrial Refractoriness and Atrial Fibrillation Inducibility Immediately after Internal Cardioversion in Patients with Chronic Persistent Atrial Fibrillation. Cardiovasc Drugs Ther 13, 507–511 (1999). https://doi.org/10.1023/A:1007823619899
Issue Date:
DOI: https://doi.org/10.1023/A:1007823619899