
Abstract
Purpose
PR interval prolongation > 200 ms resulting in the diagnosis of first-degree atrioventricular block (AVB1) is caused by a delay in the AV nodal/His conduction and/or the right intra-atrial conduction (RIAC). The aim of the study was to assess the prevalence of AVB1 due to RIAC delay (AVB1 with normal AH and HV) in patients with atrial fibrillation (AF) and atrial flutter (AFlu).
Methods
We included 1067 consecutive patients (33% female, age 63 ± 13 years) referred for catheter ablation of AF (AF-group) (453 patients), AF and AFlu (136 patients), AFlu (292 patients), and AVNRT/AVRT (186 patients). AH-, HV-, PR-interval, and P-wave duration were measured on the 12-lead ECG and the intracardiac electrograms in sinus rhythm. RIAC delay was defined as a prolonged PR interval > 200 ms with normal AH and HV intervals.
Results
The prevalence of AVB1 is higher in patients with AFlu (41%) and AF (21%) and patients with both arrhythmias (30%) as compared with a reference group (8%) of patients with AVNRT/AVRT. AVB1 was due to RIAC delay in 42 of 67 patients (63%) in the AF-group, in 37 of 96 patients (39%) in the AFlu-group, and in 17 of 36 patients (47%) in the AF/AFlu group, respectively. AV nodal conduction delay was more common in AFlu patients compared with AF patients.
Conclusion
RIAC delay is a common underlying cause of AVB1 in patients with AF and AFlu. These findings may impact the prescription of antiarrhythmic and AV-nodal blocking drugs.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Purpose
First-degree atrioventricular block (AVB1), defined as PR interval longer than 200 ms, is frequently encountered in clinical practice and generally considered benign [1]. Since the PR interval is measured between the onset of the P wave and of the QRS-complex on the 12-lead ECG, it is dependent on both, the right intra-atrial conduction (RIAC) and the AV conduction over the AV node and the His bundle. The electrical and structural remodeling of the atrium observed in patients with AF [2, 4] and cavotricuspid isthmus (CTI)-dependent AFlu [3] may result in (right) atrial conduction delay influencing the PR interval measurements. The exact contribution of the RIAC interval on the PR interval commonly used for electrical characterization of the heart has not been systematically investigated in patients with AF and AFlu. Furthermore, the prevalence of RIAC delay defined as AVB1 with normal AH and HV intervals is unknown.
The aim of this study was to assess the prevalence of AVB1 due to RIAC delay by standard invasive electrophysiological measurements in patients referred for catheter ablation of AF and AFlu. In addition, patients undergoing catheter ablation of AVNRT or AVRT were analyzed as a reference group representing patients without any known or suspected right atrial myocardial conduction disease.
2 Methods
We included 1067 consecutive patients undergoing an electrophysiological study for ablation of AF (AF-group), CTI-dependent AFlu (AFlu-group), and AVNRT/AVRT (reference-group). Diagnosis of CTI-dependent AFlu was performed by positive entrainment maneuver from the CTI in case of persistent flutter in the electrophysiology lab and based on 12-lead documentation showing a negative saw-tooth waves in inferior leads and positive waves in V1. Patients with documented AF in the AFlu-group and documented AFlu in the AF-group were combined in an AF/AFlu-group. Measurements on the 12-lead ECG and intracardiac electrograms using standard quadripolar and decapolar catheters with 5 mm and 2 mm interelectrode spacing (Abbot Medical and Biosense Webster, USA) were performed by two experienced technicians at the end of the procedure in sinus rhythm on the EP recording system (Sensis, Siemens, Germany). Intervals were defined as follows: atrium-His (AH) interval—onset of atrial signal to onset of His-deflection on the His recording (normal: 60–125 ms), His-ventricle (HV) interval—onset of His-deflection to onset of QRS interval (normal: 35–55 ms), P-wave duration—onset to offset of the P wave of all 12 leads, PR interval—beginning of P wave to first deflection of QRS, QRS duration—onset to offset of the QRS complex of all 12 leads, and RIAC—onset of P wave to onset of the atrial signal on His catheter. RIAC delay was defined as a prolonged PR interval > 200 ms with normal AH and HV intervals. The definition of persistent and paroxysmal AF was performed according to the AHA/ACC/HRS guidelines [5]. Patients treated with antiarrhythmic drugs (class IC and class III) were excluded.
3 Results
A total of 858 patients (33% female, 63 ± 13 years) were analyzed. Thereof, 237 (28%), 319 (37%), 120 (14%), and 182 (21%) were included in the AFlu-group, the AF-group, the AF/AFlu-group, and the reference-group, respectively. Baseline data were significantly different between the groups (Table 1). Data of an age- and sex-matched analysis are shown in supplemental Table 1 and 2. The baseline data of the patients with paroxysmal and persistent AF were not different. AVB1 was present in 67 patients (21%) of the AF-group, in 96 patients (41%) of the AFlu-group, in 36 patients (30%) of the AF/AFlu-group, and in 15 patients (8%) of the reference-group. In the patients with AVB1, RIAC delay was observed in 42 of 67 patients (63%) in the AF-group, in 37 of 96 patients (39%) in the AFlu-group, and in 17 of 36 patients (47%) in AF/AFlu-group. The difference in RIAC delay between the AF-group (63%) and the AFlu-group (39%) was statistically significant (p = 0.013). PR interval prolongation was rare in the reference group, but if present was also due to RIAC delay in 40%. In patients without AVB1, the prevalence of a RIAC time > 45 ms [6] was 57%, 63%, 63%, and 27% in the AF-group, the AF/AFlu-group, the AFlu-group, and the reference-group, respectively.
4 Discussion
Whereas it is known that AV conduction is determined by the RIAC and the conduction over the AV node and the His bundle, its dispersion has never been quantified in such a large cohort of patients with AF and CTI-dependent AFlu. The main findings of this analysis are as follows:
-
1.
The prevalence of AVB1 is high in patients with AFlu and AF and a combination of both arrhythmias as compared with a reference group of patients with AVNRT/AVRT.
-
2.
The prevalence of RIAC delay as the cause of PR prolongation is significant in patients with AF, AFlu, and a combination of AF and AFlu, with the highest proportion observed in the AF group.
In previous studies, PR prolongation has been shown to be independently associated with the risk of developing AF [7] and all-cause mortality [8]. However, the individual contribution of the RIAC and the AV nodal conduction on the PR interval have not been investigated in this context. In consequence, whether the reported risk for these events is due to right atrial conduction delays or the delay within the AV node is unclear. To address this lack of knowledge, we analyzed patients with AF and AFlu to investigate whether differences in the site of the conduction impairment (RIAC or AV nodal) can be observed for these groups.
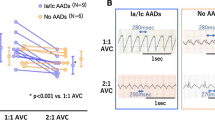
In our patients, the prevalence of AVB1 defined by PR prolongation > 200 ms was relatively high in patients with AF (21%) and even higher in CTI-dependent AFlu (41%). Interestingly, RIAC delay as a measure of solely right intra-atrial conduction delay (without AV conduction delay) was observed more often in patients with AF than with AFlu, whereas the AFlu-group showed an AVB1 more often due to AV nodal conduction delay. This observation is in contrast to the only other study investigating electrophysiological difference in the right atrium between patients with AFlu and AF [9]. Medi et al. reported that patients with AFlu showed more advanced remodeling with slowed conduction and lower voltage areas especially in the posterior right atrium than with AF. However, this was a small study with only 10 and 13 patients in the AFlu and AF group, respectively, and the baseline details such as type of AF and prescription of AV blocking agents was not reported, which might explain the differences, as well as an inhomogeneous distribution of a right atrial remodeling (Fig. 1).

Bar chart of prevalence of AV-block first degree (AVBI) and right atrial conduction (RIAC) delay in patients with atrial fibrillation (AF), atrial flutter (AFlu), and the patients with both arrhythmias, AF and AFlu. The dark blue bar represents the percentage prevalence of AVBI in the overall cohort of the respective group; the light blue bar represents the percentage prevalence of RIAC delay in the cohort of AVBI patients of the respective group
In addition, our findings may have additional clinical implications based on the differentiation between AV nodal-related versus RIAC-related conduction delay. For example, since the administration of negative dromotropic and/or antiarrhythmic drugs performed with caution in patients with AV nodal conduction disturbances [8], our findings show that the use of these drug therapies should not be limited because of AVB1 per se because the cause of AVB1 is a delay in the RIAC and not in the AV-node or His bundle in a significant number of cases. In conclusion, if the knowledge of the location of the atrioventricular conduction delay in patients with AVB1 is of clinical importance, an electrophysiological study might be indicated.
Based on our observations, one could hypothesize that AF results in more pronounced RA remodeling resulting in an increase of conduction delay compared with AFlu. This is in line with a basic research study in neonatal rat ventricular myocytes showing that irregular (AF-like) compared regular electrical activation (AFlu-like) results in a phenotype consistent with findings in atrial cardiomyocytes from AF patients [10]. Whether this knowledge about the differences in right atrial conduction delay should be used, e.g., in additional right atrial ablation strategies in patients with persistent AF or to perform AF ablation in patients with AFlu and RIAC delay due to the increased risk for AF [5] is an interesting research question that might be addressed in future studies. In this context, we await the results of the CRAFT study (https://clinicaltrials.gov/ct2/show/NCT03401099) investigating the impact of cryoballoon PVI in patients referred for catheter ablation of CTI-dependent flutter without previously documented AF.
5 Limitations
The four groups differ with regard to baseline data. This is relevant especially for age, which was shown to correlate with the atrial conduction [11]. However, since the AFlu group was older than the AF group but the delay was more prevalent in the AF group, an older age in the AF group might not decrease this difference. The age- and sex-matched analyses shown in the supplemental tables confirm this observation. Furthermore, despite studying a large sample of 858 patients, the number of patients with RIAC delay in the different groups is relatively small. This was addressed by critical interpretation of the observations. One further limitation is the measurement of the PR interval itself and the absolute definition of a cut-off of 200 ms without addressing the heart rate dependency. Beta blockers were continued during the study; this can have an effect on the AV conduction. However, we focused our view on the RIAC delay, which by definition excluded patients with AH and/or HV extension. Also, despite not being observed or reported in other studies, an impact of the CTI ablation line on the PR interval cannot be excluded. Finally, our findings are observational in nature. Whether the underlying mechanisms can be explained mainly by remodeling associated with the respective arrhythmias, the predisposing risk factors, or whether specific molecular mechanisms such as connexin distribution or dysregulation are present [12], are currently unknown and requires further investigations.
6 Conclusion
In conclusion, PR prolongation has a high prevalence in patients with AFlu and AF but frequently represents what we could call a “pseudo”-AVB1. In clinical practice, RIAC delay should be considered as a potential cause of AVB1 in any patient with PR prolongation and especially in patients with AF. The presented findings may help to discriminate the reason for AVB1 in patients with AFlu and AF and may have clinical implications when prescribing antiarrhythmic drugs, betablockers, or calcium-channel blockers or planning catheter ablation.
References
Bexton RS, Camm AJ. First degree atrioventricular block. Eur Heart J. 1984;5(Suppl A):107–9.
Teh AW, et al. Electroanatomic remodeling of the left atrium in paroxysmal and persistent atrial fibrillation patients without structural heart disease. J Cardiovasc Electrophysiol. 2012;23:232–8.
Nattel S, Burstein B, Dobrev D. Atrial remodeling and atrial fibrillation: mechanisms and implications. Circ Arrhythm Electrophysiol. 2008;1:62–73.
Franz MR, Karasik PL, Li C, Moubarak J, Chavez M. Electrical remodeling of the human atrium: similar effects in patients with chronic atrial fibrillation and atrial flutter. J Am Coll Cardiol. 1997;30:1785–92.
January CT, Wann LS, Alpert JS, Calkins H, Cigarroa JE, Cleveland JC Jr, et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the Heart Rhythm Society. Circulation. 2014;130:2071–104.
Bayés de Luna A. Basic Electrocardiography: Normal and Abnormal ECG Patterns. Hoboken: Wiley-Blackwell; 2007.
Schnabel RB, Sullivan LM, Levy D, Pencina MJ, Massaro JM, D'Agostino RB Sr, et al. Development of a risk score for atrial fibrillation (Framingham Heart Study): a community-based cohort study. Lancet. 2009;373(9665):739–45.
Cheng S, Keyes MJ, Larson MG, et al. Long-term outcomes in individuals with prolonged PR interval or first-degree atrioventricular block. JAMA. 2009;301(24):2571–7.
Medi C, et al. Right atrial remodeling is more advanced in patients with atrial flutter than with atrial fibrillation. J Cardiovasc Electrophysiol. 2012;23:1067–72.
Lenski M, Schleider G, Kohlhaas M, Adrian L, Adam O, Tian Q, et al. Arrhythmia causes lipid accumulation and reduced glucose uptake. Basic Res Cardiol. 2015;110(4):40.
Kojodjojo P, Kanagaratnam P, Markides V, Davies DW, Peters N. Age-related changes in human left and right atrial conduction. J Cardiovasc Electrophysiol. 2006;17(2):120–7.
Temple IP, Inada S, Dobrzynski H, Boyett MR. Connexins and the atrioventricular node. Heart Rhythm. 2013;10:297–304.
Funding
Open access funding provided by University of Basel.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Florian Spies – No conflict of interest
Sven Knecht – No conflict of interest
Ivan Zeljkovic – No conflict of interest
Tobias Reichlin – No conflict of interest
Antonio Madaffari - No conflict of interest
Stefan Osswald - No conflict of interest
Christian Sticherling – Advisory Board of Medtronic and Biotronik, received educational grants from Biotronik and research grant from Biosense Webster.
Michael Kühne - received grants from the Swiss National Science Foundation and the Swiss Heart Foundation, and lecture/consulting fees from Daiichi-Sankyo, Boehringer Ingelheim, Bayer, Pfizer-BMS, AstraZeneca, Sanofi-Aventis, Novartis, MSD, Medtronic, Boston Scientific, St. Jude Medical, Biotronik, Sorin, Zoll and Biosense Webster.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Spies, F., Knecht, S., Zeljkovic, I. et al. First-degree atrioventricular block in patients with atrial fibrillation and atrial flutter: the prevalence of intra-atrial conduction delay. J Interv Card Electrophysiol 61, 421–425 (2021). https://doi.org/10.1007/s10840-020-00838-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10840-020-00838-3