
Abstract
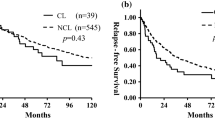
The study objective was to study the therapeutic effect of surgical treatment for hepatocellular carcinoma (HCC) originating from the caudate lobe. From 1995 to 2003, caudate lobe resection was carried out for 97 cases; among them 39 were for HCC, who were divided into two groups. Group A consisted of 19 cases undergoing isolated caudatectomy, and group B consisted of 20 cases undergoing caudatectomy combined with other liver resections. The factors that might influence postoperative recovery were com-pared between the two groups. A special instrument, Peng’s Multifunctional Operative Dissector, was used for surgical dissection. All tumors were resected successfully. One patient died of postoperative re-nal failure. Hydrothorax occurred in three patients, ascites occurred in four patients, and bile leakage occurred in one patient. Thirty cases received long-term follow-up with survival rates at 1, 3, and 5 years of 53%, 50%, and 39%, respectively. Caudate lobectomy is an effective therapeutic method for HCC originating in the caudate lobe. Isolated caudatectomy should be performed as the first choice whenever possible. Anterior transhepatic approach is appropriate in some cases. Peng’s Multifunctional Operative Dissector is a very useful instrument for surgical dissection.
Similar content being viewed by others

References
Peng SY, Mou YP, Peng CH, et al. Resection of caudate lobe of liver: report of 26 cases. Chin J Surg 1999;37:12–13.
Peng SY, Li JT, Du JJ, et al. The role and significance of looping round the major hepatic vein in difficult hepatecto-mies (in Chinese). Chin J Gen Surg 2003;18:444–445.
Peng SY, Mou YP, Cai XJ, et al. Isolated complete caudate lobectomy through the anterior transhepatic approach (in Chinese). Chin J Gen Surg 2003;18:74–76.
Peng SY, Cai XJ, Liu YB, et al. Curettage and aspiration dissection technique employed in different kinds of surgical operation (in Chinese). Chin J Pract Surg 2001;21:162.
Bartlett D, Fong Y, Blumgart LH. Complete resection of the caudate lobe of the liver: technique and results. Br J Surg 1996;83:1076–1081.
Shibata T, Maetani Y, Ametani F, et al. Efficacy of nonsur-gical treatments for hepatocellular carcinoma in the caudate lobe. Cardiovasc Intervent Radiol 2002;25:186–192.
Miyayama S, Matsui O, Kameyama T, et al. Angiographic anatomy of arterial branches to the caudate lobe of the liver; with special reference to its effect on transarterial emboliza-tion for hepatocellular carcinoma. Jpn J Clin Radiol 1990;35:353–359.
Asahara T, Dohi K, Katayama K. Isolated caudate lobectomy for hepatocellular carcinomadA left-sided approach. Asian J Surg 2000;23:15–122.
Yang MC, Lee PO, Sheu JC, et al. Surgical treatment of he-patocellular carcinoma originating from the caudate lobe. World J Surg 1996;20:562–566.
Shimada M, Matsumata T, Maeda T, et al. Characteristics of hepatocellular carcinoma originating in the caudate lobe. Hepatology 1994;19:911.
Yamamoto J, Takayama T, Kosuge T, et al. An isolated cau-date lobectomy by the transhepatic approach for hepatocel-lular carcinoma in cirrhotic liver. Surgery 1992;111:699–702.
Yanaga K, Matsumata T, Hayashi H, et al. Isolated hepatic caudate lobectomy. Surgery 1994;115:757–761.
Peng SY, Liu YB, Xu B, et al. Role and significance of extra-hepatic control of hepatic vein and inferior vena cava in dif-ficult hepatectomies for patients with liver tumor (in Chinese). Chin J Surg 2004;42:260–264.
Author information
Authors and Affiliations
Corresponding author
Additional information
Supported by grants from Zhejiang Province Natural Science Fund, China (Fund No. 0306GJHZ).
Rights and permissions
About this article
Cite this article
Peng, S.Y., Li, J.T., Liu, Y.B. et al. Surgical treatment of hepatocellular carcinoma originating from caudate lobe—A report of 39 cases. J Gastrointest Surg 10, 371–378 (2006). https://doi.org/10.1016/j.gassur.2005.09.026
Issue Date:
DOI: https://doi.org/10.1016/j.gassur.2005.09.026