
Abstract
Background
We have developed a tridirectional regimen combining intraperitoneal, intravenous, and oral chemotherapy as a treatment for patients with advanced gastric cancer and individualized these chemotherapeutics according to mRNA expression. This multicenter Phase III umbrella study compared the efficacy and safety of individualized tridirectional intraperitoneal and systemic chemotherapy with that of standard systemic chemotherapy.
Methods
BRCA1/TOPO1 mRNA expression was examined in all enrolled patients. The patients were then randomized in a ratio of 3:1 to an individualized arm and a control arm. Patients in the control arm received systemic intravenous/oral chemotherapy, whereas those in the individualized arm received sensitive chemotherapeutics selected from oxaliplatin/cisplatin/docetaxel/irinotecan/S-1 according to their BRCA1/TOPO1 mRNA expression and received individualized tridirectional intraperitoneal/intravenous/oral chemotherapy. The primary endpoint was progression-free survival and the secondary endpoints were response rate, overall survival, and safety.
Results
Overall, 233 of 240 patients enrolled between August 2014 and December 2016 were included in the efficacy analysis. Baseline patient characteristics were balanced between the two arms. The objective response rate was 33.9% in the control arm and 49.1% in the individualized arm (P = 0.039). In the control and individualized arms, median progression-free survival was 5.9 months and 8.0 months, respectively (hazard ratio 0.521, 95% confidence interval 0.362–0.750, P = 0.0005) and median overall survival was 13.5 months and 16.4 months, respectively (hazard ratio 0.684, 95% confidence interval 0.474–0.988, P = 0.0430). Both regimens were tolerable.
Conclusion
The primary analysis demonstrated the statistical superiority of this tridirectional individualized regimen and suggests that this regimen has clinical efficacy in patients with advanced gastric cancer.
Trial registration
Chinese Clinical Trial Registry (chictr.org.cn) Identifier: ChiCTR-IPR-15006201.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Gastric cancer continues to be a serious global health problem. It is the fifth most common cancer and the third leading cause of cancer-related death worldwide [1]. The highest rates of gastric cancer occur in China, Japan, Korea, Eastern Europe, and South America, with 42% of cases occurring in China [2]. Gastric adenocarcinoma is the most common histological type of all malignancies originating in the stomach, accounting for about 95% of all cases [3]. Even though screening strategies for early detection have been shown to be successful in Japan, they are either not feasible or not implemented in other countries, leading to late diagnosis in most patients with gastric cancer [3]. Treatment for advanced gastric cancer is unsatisfactory. Despite the considerable progress made in targeted therapy in the last 20 years, few treatments have demonstrated efficacy in gastric cancer. Chemotherapy remains the foundation of treatment for patients with advanced gastric cancer, who have a poor prognosis with a median survival of about 1 year.
Peritoneal dissemination appears to be the most common pattern of metastasis in patients with advanced gastric cancer and is life-threatening. Liver, abdominal, and retroperitoneal lymph node and pelvic metastases are also common [4]. Our recent study found that about 81.1% of patients with gastric cancer had metastasis in the abdominal cavity at the time of diagnosis or recurrence [4]. Peritoneal recurrence was reported to develop in 60% of patients with T3-4 tumors after curative surgery [5], and intraperitoneal spread of tumor cells was observed in 54% of patients with advanced gastric cancer who died of recurrence after curative resection [6]. All the commonly used imaging techniques have been found to have major limitations in the diagnosis of peritoneal carcinomatosis because of the low volume density of peritoneal nodules [7]. Despite recent developments in chemotherapeutics and molecularly targeted drugs, any treatment, if administered only via the intravenous route, cannot adequately control gastric cancer, especially in patients with peritoneal metastasis. Nowadays, hyperthermic intraperitoneal chemotherapy is the most widely accepted treatment strategy for peritoneal dissemination. The high intraperitoneal drug concentration achieved by this treatment can directly act on free tumor cells and also peritoneal nodules. Intraperitoneal drugs can be absorbed through the peritoneum to the portal vein and release chemotherapeutic effects in the liver [8]. A systematic review and meta-analysis of 20 prospective randomized controlled trials that included 2,145 patients with advanced gastric cancer concluded that intraperitoneal chemotherapy has a more positive effect on peritoneal recurrence and distant metastasis than surgery alone [9]. A series of Phase I, II, and III clinical trials in Japan led to development of a tridirectional regimen combining intraperitoneal paclitaxel with oral S-1 and intravenous paclitaxel for the treatment of patients with gastric cancer and peritoneal metastasis. The Phase II study yielded promising results, with a 1-year overall survival rate of 78% [10], and the Phase III study suggested that the clinical efficacy of intraperitoneal paclitaxel was superior to that of standard systemic chemotherapy (S-1/cisplatin) in patients with gastric cancer and peritoneal metastasis [11]. Other chemotherapeutic agents commonly used for gastric cancer, such as 5-fluorouracil, cisplatin, oxaliplatin, and irinotecan, have been confirmed to be safe for intraperitoneal use in patients with gastrointestinal tumors [12, 13]. However, there have been no clinical studies of the efficacy and safety of the tridirectional regimen, including intraperitoneal administration, in advanced gastric cancer or on how to identify which patients will benefit from intraperitoneal chemotherapy.
The current preferred chemotherapeutic regimens for advanced gastric cancer are platinum-based or 5-fluorouracil-based, and some of the guidelines also recommend taxanes, irinotecan, and epirubicin for first-line therapy. Previous large prospective randomized clinical studies have yielded consistent results for these first-line chemotherapy regimens in patients with advanced gastric cancer, with objective response rates of 24.5%–42.0% and median survival in the range of 9.5–12.4 months. S-1, which contains tegafur, CDHP (5-chloro-2, 4-dihydroxypyridine), and otastat potassium, is a promising therapy for patients with advanced gastric cancer, particularly those with peritoneal metastasis, considering that 5-fluorouracil released from S-1 can pass through the peritoneum-plasma barrier and CDHP can inhibit degradation of 5-fluorouracil by dihydropyrimidine dehydrogenase [14]. In recent decades, many molecular biomarkers have been investigated for their ability to predict the probability of response to chemotherapeutic drugs, and individualized approaches to chemotherapy may improve the likelihood of a response and reduce unnecessary toxicity [15]. However, there have been no such clinical studies on predictive biomarkers for the chemotherapeutics used in gastric cancer. Retrospective translational studies performed by our group over the last 15 years have identified breast cancer susceptibility gene 1 (BRCA1) as a potential predictive biomarker for platinum and docetaxel sensitivity [16] and topoisomerase 1 (TOPO1) for irinotecan [17]. BRCA1 has a central role in the DNA damage response pathway. It induces an approximately 10–1000-fold increase in resistance to the DNA-damaging chemotherapeutic drugs cisplatin, etoposide, and bleomycin while inducing an approximately 800–1000-fold increase in sensitivity to taxanes [18]. Irinotecan and its active metabolite SN-38 induce DNA damage by stabilizing a transient covalent complex between DNA and TOPO1, which then results in DNA strand breaks, replication arrest, and apoptosis. Repair of irinotecan-associated and TOPO1-mediated DNA damage requires removal of the stalled TOPO1 and resolution of the associated DNA break [19].
On the basis of these biological, pharmacokinetic, and biochemical lines of evidence and promising clinical data, we initiated a multicenter randomized Phase III umbrella study of a tridirectional chemotherapy regimen individualized according to BRCA1/TOPO1 mRNA levels in patients with stage IV gastric adenocarcinoma. We hypothesized that patients in an individualized group receiving tridirectional intraperitoneal and systemic chemotherapy based on their baseline tumor BRCA1/TOPO1 mRNA levels would have a higher response rate and better survival than those in a control group receiving standard non-individualized bidirectional systemic chemotherapy.
Methods
Study design and patient eligibility
This multicenter, prospective, randomized study included patients with advanced gastric cancer enrolled at any of eight Chinese cancer centers between August 2014 and June 2016. The study protocol was approved by each local ethics committee, and written informed consent was obtained from all study participants. The study data were collected by the investigators and stored and analyzed by the Clinical Cancer Institute of Nanjing University. At baseline, all patients underwent a physical examination, routine blood count and biochemistry work-up, and computed tomography scans of the thorax and abdomen (including the pelvis). An emission computed tomography scan of bone and a magnetic resonance imaging scan of the brain were required only if bone or brain metastasis was suspected. Patients were eligible for inclusion if they had histologically confirmed stage IV adenocarcinoma of the stomach or gastro-esophageal junction with at least one site of measurable disease according to the Response Evaluation Criteria in Solid Tumors (RECIST) v1.1 and if paraffin-embedded tumor tissue, either a tumor block or at least ten sections mounted on slides, was available. Other eligibility criteria included the following: age ≥ 18 years; Eastern Cooperative Oncology Group performance status of 0, 1, or 2; adequate hematologic function (absolute neutrophil count ≥ 1,500/μL, platelets ≥ 75,000/μL, and hemoglobin ≥ 8 g/dL); adequate liver function (serum bilirubin ≤ 1.5 × the upper limit of normal [ULN], aspartate transaminase or alanine aminotransferase ≤ 2.5 × ULN [or ≤ 5 × ULN in patients with liver metastases], alkaline phosphatase ≤ 2.5 × ULN [or ≤ 5 × ULN in patients with liver metastases, or ≤ 10 × ULN in patients with bone but no liver metastases], albumin ≥ 25 g/L); and adequate renal function (creatinine clearance ≥ 60 mL/min). Patients with two or more primary tumors or other serious disease, those with active gastrointestinal bleeding or brain metastasis, and those who had previously received chemotherapy were excluded.
Random assignment and treatment plan
After enrollment, BRCA1 and TOPO1 mRNA levels for all patients enrolled in the study were assessed by quantitative polymerase chain reaction according to the method described in previously published literature, and the cutoff level for expression of each mRNA was determined by a retrospective clinical study in over 1,000 patients with advanced gastric cancer [16, 17]. Enrolled patients were randomly assigned at a ratio of 3:1 to either an individualized arm (individualized drug selection and tridirectional chemotherapy) or a control arm (traditional systemic chemotherapy) by simple randomization before mRNA assessment. The randomization process was centralized at Nanjing Drum Tower Hospital (Nanjing, China) and stratified by center. Neither the investigators nor the patients were masked to treatment assignment.
Patients in the control arm received bidirectional systemic chemotherapy (arm A: intravenous docetaxel 45 mg/m2 on days 1 and 15, with oral S-1 at a dose of 40 mg/m2 twice daily on days 1–14, repeated every 4 weeks). Patients in the individualized arm received individualized tridirectional intraperitoneal and systemic chemotherapy based on their BRCA1/TOPO1 mRNA expression levels and the trial protocol. The flowchart in Fig. 1 shows the decision-making process underlying the treatment recommendations for each patient. The general principle was that the treatment recommendations should reflect the mRNA test results for each individual patient. The gray blocks indicate the different tests performed at various stages and the blue blocks indicate the treatment suggestions based on each of the test results. Patients in the individualized arm were first divided into groups based on their BRCA1 mRNA expression, and those with a higher BRCA1 level received taxane-based chemotherapy (arm B1: intraperitoneal docetaxel 15 mg/m2 on days 1 and 15, intravenous docetaxel 30 mg/m2 on days 1 and 15, with oral S-1 at a dose of 4 0 mg/m2 twice daily on days 1–14, repeated every 4 weeks) while those with a lower BRCA1 level received platinum-based chemotherapy (arm B2: intraperitoneal cisplatin 30 mg/m2 on days 1 and 15, intravenous oxaliplatin 75 mg/m2 on days 1 and 15, with oral S-1 at a dose of 40 mg/m2 twice daily on days 1–14, repeated every 4 weeks). The remaining patients were then re-divided based on their TOPO1 mRNA expression; those with a higher TOPO1 level received irinotecan-based chemotherapy (arm B3: intraperitoneal irinotecan 45 mg/m2 on days 1 and 15, intravenous irinotecan 90 mg/m2 on days 1 and 15, with oral S-1 at a dose of 40 mg/m2 twice daily on days 1–14, repeated every 4 weeks) and the remainder received taxane-based chemotherapy (arm B4: intraperitoneal docetaxel 15 mg/m2 on days 1 and 15, intravenous docetaxel 30 mg/m2 on days 1 and 15, with oral S-1 at a dose of 40 mg/m2 twice daily on days 1–14, repeated every 4 weeks). Trastuzumab was added to chemotherapy for patients with metastatic adenocarcinoma overexpressing human epidermal growth factor receptor-2.

Randomization and individual selection model. The gray blocks indicate the different tests performed at various stages and the blue blocks indicate the treatment suggestions based on each of the test results
All patients in the individualized arm received both intraperitoneal and systemic chemotherapy. Each intraperitoneal drug, such as docetaxel, cisplatin, or irinotecan, was administered with at least 1,000 mL of physiological saline preheated to 41℃–42.5℃ via a peritoneal access port implanted temporarily for 1–2 h after standard premedication for the corresponding drug. For patients with peritoneal metastasis, extensive peritoneal lavage was performed using warm physiological saline to wash away non-adherent peritoneal cancer cells before intraperitoneal chemotherapy.
Patients underwent treatment for six cycles or until an unacceptable adverse event, disease progression, or death. Before each cycle, all patients underwent a routine examination with blood tests. After the second, fourth, and sixth cycles of chemotherapy, the objective tumor response was evaluated for each patient according to the RECIST v1.1. Treatment could be continued beyond six cycles after carefully decision-making by the treating physician. Second-line therapies were permitted after discontinuation of the study treatment, and patients were monitored at 2-month intervals until death.
Clinical assessments
The primary endpoint of the trial was progression-free survival (PFS) and secondary endpoints were the objective tumor response rate, overall survival (OS), and safety. PFS was calculated from the date of randomization to the date of disease progression or death. The objective tumor response was evaluated for each patient according to the RECIST v1.1. OS was calculated from the date of randomization to the date of death or last clinical follow-up. Adverse events were graded according to the Common Terminology Criteria for Adverse Events (CTCAE) version 3.0 devised by the National Cancer Institute.
Statistical analysis
On the assumption that median PFS would be 8 months in the individualized group and 5 months in the control arm, we calculated that a total sample size of 240 patients would be needed to be able to reject the null hypothesis that the individualized and control PFS curves would be equal with a probability (power) of 0.850. The probability of type I error associated with the test of this null hypothesis (α) was 0.05.
The statistical analysis included the full analysis dataset. The baseline characteristics of the individualized group and the control group were compared using Fisher’s exact test or the chi-squared test for categorical variables and the t-test for continuous variables. Objective response rates were compared between the individualized and control arms using the chi-squared test and adverse events using a one-sided Fisher’s exact test. Kaplan–Meier curves for PFS and OS were generated and compared using the log-rank test. Unstratified hazard ratios (HRs) and corresponding 95% confidence intervals (CIs) were calculated using a Cox proportional hazards regression model for analyses of PFS and OS in all randomly assigned patients and pre-specified subgroups. A P-value < 0.05 was used as the cutoff point for statistical significance. The GraphPad Prism software package (version 5.01, GraphPad Software, Inc., La Jolla, CA) was used to generate the Kaplan–Meier curves. The SPSS statistical software package (version 16.0, SPSS Inc., Chicago, IL) was used for all other statistical analyses.
Results
Patient characteristics
Of 240 patients enrolled from the eight participating cancer centers between August 2014 and December 2016, 233 were finally included in the efficacy analysis. Table 1 shows the patient characteristics at baseline. The patients had a mean age of 57.3 years and a median age of 60 years (range, 21–79). Overall, 108 (45.0%) were Eastern Cooperative Oncology Group PS 1 and 65 (27.1%) were PS 2. There were no significant differences in baseline characteristics, including epidemiological characteristics, tumor characteristics, and expression of each mRNA, between the control arm and the individualized arm. The median follow-up duration was 18 months.
Progression-free survival
Median PFS was 5.9 months in the control arm and 8.0 months in the individualized arm (HR 0.521; 95% CI 0.362–0.750; P = 0.0005; Fig. 2).

Progression-free survival according to treatment arm
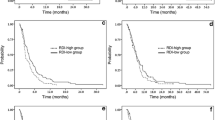
To identify which type of metastatic pattern would benefit from the individualized tridirectional regimen, we divided all the patients into five subgroups based on the first metastatic site found at diagnosis (Table 1) and then analyzed PFS between the control arm and the individualized arm according to subgroup (Fig. 3). The most significant difference in PFS was found in the subgroup with peritoneal metastasis (6.4 months in the control arm vs 9.4 months in the individualized arm [HR 0.207; 95% CI 0.086–0.500]). A significant difference was also found in the subgroup with liver metastasis (5.7 months in the control arm vs 7.4 months in the individualized arm [HR 0.490; 95% CI 0.241–0.997]). In the subgroup with metastasis elsewhere in the peritoneal cavity, median PFS was longer in the individualized arm than in the control arm (5.8 months vs 7.0 months [HR 0.457; 95% CI 0.203–1.026]); this result did not reach statistical significance, likely because of the small sample size. There was no significant between-arm difference in the subgroup with retroperitoneal metastasis (5.8 months vs 7.0 months [HR 0.483; 95% CI 0.217–1.077]) or in the subgroup with metastasis outside the peritoneal cavity (5.8 months vs 7.0 months [HR 0.483; 95% CI 0.217–1.077]).

Hazard ratios for progression-free survival according to pattern of metastasis and treatment arm
We also examined the difference in PFS for patients who received docetaxel-based tridirectional chemotherapy according to their BRCA1 mRNA expression level. Median PFS was 5.8 months in the medium BRCA1 subgroup and 8.8 months in the high BRCA1 subgroup (HR 0.431; 95% CI 0.233–0.795; Fig. 4).

Progression-free survival in patients who received docetaxel-based chemotherapy according to their BRCA1 mRNA expression level. BRCA1, breast cancer susceptibility gene 1; mPFS, median progression-free survival
Objective response rate
The median number of chemotherapy cycles was 6 (range, 1–12). The individualized arm (49.1%; 95% CI 41.6–56.7) achieved higher objective response than the control arm (33.9%; 95% CI 21.8–46.0) (Table 2).
Overall survival
Median OS was 13.5 months in the control arm and 16.4 months in the individualized arm (HR 0.684; 95% CI 0.474–0.988; Fig. 5).

Median survival according to treatment arm. mOS, median overall survival
Toxicities
Table 3 shows the adverse events according to treatment arm. The most common grade 3–4 adverse events were neutropenia (24.2% in the control arm vs 24.0% in the individualized arm), leucopenia (16.1% vs 12.9%), thrombocytopenia (8.1% vs 14.6%), fatigue (9.7% vs 5.8%), and decreased appetite (8.1% vs 6.4%). The patients in the individualized arm were at higher risk of thrombocytopenia than those in the control arm (grade 1–4, 35.5% vs 45.6%, P = 0.167; grade 3–4, 8.1% vs 14.6%, P = 0.187) but the difference was not statistically significant. The only adverse event that showed a significant difference between the two arms was peripheral sensory neuropathy (grade 1–4, 11.3% vs 41.5%, P < 0.001; grade 3–4, 0% vs 4.1%, P = 0.111). There were no serious adverse events caused by intraperitoneal puncture and no treatment-related deaths.
Discussion
In this multicenter, randomized Phase III trial, patients in the individualized arm, who received a new comprehensive regimen with individualized chemotherapeutic drug selection and tridirectional intraperitoneal, intravenous, and oral drug administration, had significantly better outcomes in terms of objective response rate, PFS, and OS than those in the control arm, who received standard systemic intravenous and oral chemotherapy.
Advanced gastric cancer is still a life-threatening disease with low response rates and a short survival outcome [3]. Nowadays, systemic chemotherapy for advanced gastric cancer continues to be conventional, with reported objective response rates of 24.5%–42.0% and median survival of 9.5–12.4 months. The efficacy of chemotherapy is not satisfactory. For any regimen currently used in clinical practice, less than half of patients achieve an objective response. Development of predictive biomarkers to identify patients who are more likely to benefit from chemotherapy is very important in gastric cancer research. For prognostic biomarkers, advances in genome-wide sequencing and microarray analysis have allowed identification of molecular signatures that can promote more precise classification and prognostication of some human cancers, such as non-small-cell lung cancer and breast cancer [20]. Several studies have yielded promising results in terms of biomarkers predictive of chemosensitivity. A multicenter Phase III trial from Europe confirmed that assessment of ERCC1 mRNA expression is feasible in clinical practice and predicts the response to docetaxel and cisplatin [15]. However, there is still no widely accepted gene signature for personalized chemotherapy in gastric cancer. In the last 15 years, our research team has focused on biomarkers predictive of chemosensitivity in gastric cancer. After filtering biomarkers from hundreds of candidates, identifying several promising biomarkers in basic research, and confirming the association of three mRNA levels with the response to corresponding chemotherapeutic drugs in retrospective studies [16, 17], we initiated this multicenter, randomized, prospective Phase III trial of individualized chemotherapy according to BRCA1 and TOPO1 mRNA levels. In this study, patients in the individualized arm who received therapy tailored to their baseline tumor BRCA1/TOPO1 mRNA levels had a higher objective response rate (49.1% vs 33.9%, P = 0.039), better PFS (8.0 months vs 5.9 months, P = 0.0005), and OS (16.4 months vs 13.5 months, P = 0.0430) than patients in the control arm who received non-individualized therapy. Furthermore, we conducted a direct comparison in patients who received docetaxel-based tridirectional chemotherapy according to their BRCA1 mRNA level. The patients with a high level of BRCA1 (≥ 11.3) achieved a higher objective response rate (56.1% vs 36.1%, P = 0.060) and better PFS (8.8 months vs 5.8 months, P = 0.007) than those in the insensitive subgroup with a medium level of BRCA1 (5.63 ≤ BRCA1 < 11.3). These results confirmed our experimental and clinical data that the BRCA1 level was associated with the corresponding chemotherapeutic drugs.
Our study also demonstrated that tridirectional chemotherapy, which includes intraperitoneal administration, was significantly superior to conventional systemic chemotherapy for advanced gastric cancer. A recent study showed that about 81.1% of patients with advanced gastric cancer had metastasis in the abdominal cavity at the time of recurrence or diagnosis [4]. In that study, peritoneal metastasis was the most frequent and serious pattern of gastric cancer with a short survival time, while metastasis to the liver, abdominal cavity, retroperitoneal lymph nodes, or pelvis were also common. Effective treatment strategies for these patterns of metastasis from gastric cancer to the abdominal cavity are urgently needed in clinical practice. Many studies have reported that intraperitoneal administration of chemotherapeutic drugs is a safe and effective method for treating peritoneal metastasis [10, 11]. The theoretical advantages of comprehensive hyperthermic intraperitoneal chemotherapy are that it can wash away non-adherent peritoneal cancer cells by extensive peritoneal lavage and that it adds the direct cytotoxic effects of heat to a high local chemotherapeutic drug concentration with reduced systemic toxicity [21]. Intraperitoneal drugs can also be absorbed through the peritoneum to the portal vein and release their antitumor effects in the liver [8]. The major problem with intraperitoneal chemotherapy is the limited depth of penetration of active anticancer components directly into the tumor; therefore, an optimal solution may consist of intraperitoneal and intravenous administration. Oral administration of S-1 also has the advantage over 5-fluorouracil for gastric cancer with peritoneal metastasis in that 5-fluorouracil from S-1 can cross the peritoneum-plasma barrier and CDHP from S-1 can inhibit degradation of 5-fluorouracil by dihydropyrimidine dehydrogenase [14]. In our study, the tridirectional regimen was shown to be of benefit for patients with metastasis to the peritoneum, liver, or elsewhere in the abdominal cavity but not for patients with retroperitoneal metastasis or metastasis outside the abdominal cavity. This finding may be helpful for individualized clinical decision-making in patients with gastric cancer.
We also confirmed that in addition to cisplatin, the most popular intraperitoneally used chemotherapeutic drug for gastric cancer, other drugs, such as docetaxel and irinotecan, are effective and safe when administered intraperitoneally for gastric cancer. It has been reported that cisplatin can be immediately absorbed through the peritoneum because of its small molecular size [22]. In contrast, docetaxel, one of the taxanes, is absorbed through openings in the lymphatic system, such as the stomata and milky spots, which are important sites for peritoneal dissemination [23], because of its large molecular weight and fat solubility [24]. It has also been demonstrated that intraperitoneal docetaxel has dual anticancer effects via the peritoneal surface and capillary blood supply because it has the pharmacokinetic advantage after intraperitoneal delivery which is 515 times higher than systemic administration [25]. Intraperitoneal administration of irinotecan was significantly more effective than intravenous administration in terms of antitumor effect against both peritoneal and liver metastasis in both an animal model and in a Phase 1 clinical trial [26]. These studies also demonstrated that the areas under the curve for irinotecan and its active metabolite, SN-38, were higher when irinotecan was administered intraperitoneally than when it was injected intravenously [27].
There were no treatment-related deaths in this study. Peripheral sensory neuropathy was more common in the individualized arm than in the control arm; 36.6% of the patients (60/164) in the individualized arm received oxaliplatin, whereas none of the patients in the control arm received oxaliplatin. All other non-hematological and hematological adverse events were similar between the two arms. There were no serious adverse events associated with intraperitoneal puncture.
The limitations of this study were the complex selection process and relatively small sample size. A simpler selection process would be preferable for clinical use. This study tested the efficacy of both individualized selection and tridirectional administration of chemotherapy, and a larger sample size of patients would yield more insights from subgroup analyses.
To the best of our knowledge, this is the first prospective randomized clinical trial to test the concept of individualized tridirectional chemotherapy for advanced gastric cancer and has demonstrated the feasibility of the approach. This new strategy may help to improve clinical practice for patients with advanced gastric cancer, especially those with metastasis inside the abdominal cavity.
Availability of data and materials
The data generated in the present study may be requested from the corresponding author.
References
Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65:87–108.
Washington K. 7th edition of the AJCC cancer staging manual: stomach. Ann Surg Oncol. 2010;17:3077–9.
Ajani JA, Lee J, Sano T, Janjigian YY, Fan D, Song S. Gastric adenocarcinoma. Nat Rev Dis Primers. 2017;3:17036.
Wei J, Yang Y, Du J, et al. Peritoneal metastasis in relation to outcome and herapeutic strategy in gastric cancer. Transl Cancer Res. 2017;6:149–56.
Sugarbaker PH, Yonemura Y. Clinical pathway for the management of resectable gastric cancer with peritoneal seeding: best palliation with a ray of hope for cure. Oncology. 2000;58:96–107.
Fujimoto S, Takahashi M, Mutou T, Kobayashi K, Toyosawa T. Successful intraperitoneal hyperthermic chemoperfusion for the prevention of postoperative peritoneal recurrence in patients with advanced gastric carcinoma. Cancer. 1999;85:529–34.
Montori G, Coccolini F, Ceresoli M, et al. The treatment of peritoneal carcinomatosis in advanced gastric cancer: state of the art. Int J Surg Oncol. 2014;2014:912418.
Speyer JL, Sugarbaker PH, Collins JM, Dedrick RL, Klecker RW Jr, Myers CE. Portal levels and hepatic clearance of 5-fluorouracil after intraperitoneal administration in humans. Cancer Res. 1981;41:1916–22.
Coccolini F, Cotte E, Glehen O, et al. Intraperitoneal chemotherapy in advanced gastric cancer. Meta-analysis of randomized trials. Eur J Surg Oncol. 2014;40:12–26.
Ishigami H, Kitayama J, Kaisaki S, et al. Phase II study of weekly intravenous and intraperitoneal paclitaxel combined with S-1 for advanced gastric cancer with peritoneal metastasis. Ann Oncol. 2010;21:67–70.
Ishigami H, Yamaguchi H, Yamashita H, Asakage M, Kitayama J. Surgery after intraperitoneal and systemic chemotherapy for gastric cancer with peritoneal metastasis or positive peritoneal cytology findings. Gastric Cancer. 2017;20:128–34.
Glockzin G, Gerken M, Lang SA, Klinkhammer-Schalke M, Piso P, Schlitt HJ. Oxaliplatin-based versus irinotecan-based hyperthermic intraperitoneal chemotherapy (HIPEC) in patients with peritoneal metastasis from appendiceal and colorectal cancer: a retrospective analysis. BMC Cancer. 2014;14:807.
Murata S, Yamamoto H, Naitoh H, et al. Feasibility and safety of hyperthermic intraperitoneal chemotherapy using 5-fluorouracil combined with cisplatin and mitomycin C in patients undergoing gastrectomy for advanced gastric cancer. J Surg Oncol. 2017;116(8):1159–65.
Sasako M, Sakuramoto S, Katai H, et al. Five-year outcomes of a randomized phase III trial comparing adjuvant chemotherapy with S-1 versus surgery alone in stage II or III gastric cancer. J Clin Oncol. 2011;29:4387–93.
Cobo M, Isla D, Massuti B, et al. Customizing cisplatin based on quantitative excision repair cross-complementing 1 mRNA expression: a phase III trial in non-small-cell lung cancer. J Clin Oncol. 2007;25:2747–54.
Wei J, Costa C, Ding Y, et al. mRNA expression of BRCA1, PIAS1, and PIAS4 and survival after second-line docetaxel in advanced gastric cancer. J Natl Cancer Inst. 2011;103:1552–6.
Shen J, Wei J, Wang H, et al. A three-gene signature as potential predictive biomarker for irinotecan sensitivity in gastric cancer. J Transl Med. 2013;11:73.
Quinn JE, James CR, Stewart GE, et al. BRCA1 mRNA expression levels predict for overall survival in ovarian cancer after chemotherapy. Clin Cancer Res. 2007;13:7413–20.
Gilbert DC, Chalmers AJ, El-Khamisy SF. Topoisomerase I inhibition in colorectal cancer: biomarkers and therapeutic targets. Br J Cancer. 2012;106:18–24.
Chen HY, Yu SL, Chen CH, et al. A five-gene signature and clinical outcome in non-small-cell lung cancer. N Engl J Med. 2007;356:11–20.
Wei J, Wu ND, Liu BR. Regional but fatal: Intraperitoneal metastasis in gastric cancer. World J Gastroenterol. 2016;22:7478–85.
Sautner T, Hofbauer F, Depisch D, Schiessel R, Jakesz R. Adjuvant intraperitoneal cisplatin chemotherapy does not improve long-term survival after surgery for advanced gastric cancer. J Clin Oncol. 1994;12:970–4.
Tsujimoto H, Hagiwara A, Shimotsuma M, et al. Role of milky spots as selective implantation sites for malignant cells in peritoneal dissemination in mice. J Cancer Res Clin Oncol. 1996;122:590–5.
Chang YF, Li LL, Wu CW, et al. Paclitaxel-induced apoptosis in human gastric carcinoma cell lines. Cancer. 1996;77:14–8.
Fushida S, Kinoshita J, Yagi Y, et al. Dual anti-cancer effects of weekly intraperitoneal docetaxel in treatment of advanced gastric cancer patients with peritoneal carcinomatosis: a feasibility and pharmacokinetic study. Oncol Rep. 2008;19:1305–10.
Matsui A, Okuda M, Tsujitsuka K, Enomoto K, Maruyama K. Pharmacology of intraperitoneal CPT-11. Surg Oncol Clin N Am. 2003;12:795–811.
Turcotte S, Sideris L, Younan R, Drolet P, Dube P. Pharmacokinetics of intraperitoneal irinotecan in a pig model. J Surg Oncol. 2010;101:637–42.
Acknowledgements
Not applicable.
Patient consent for publication
Written informed consent was obtained from all patients prior to initiation of the study.
Funding
This work was funded by grants from the National Key Research and Development Program of China (grant numbers 2017YFC1308900 and SQ2018ZX090301) and the National Natural Science Foundation of China (grant numbers 81370064 and 81672367).
Author information
Authors and Affiliations
Contributions
BRL, WXG, YY, and JW: conception and design. YY, LY, LY, and CYG: material preparation. YY, JW, JD, ZYZ, RFW, FLZ, WSS, XYL, SYS, XQL, CLN, GC, XPQ, WXG, and BR: data collection. BRL and YY: confirmation of the authenticity of all the raw data. HQQ, YY, and MMG: data analysis. YY: writing of the first draft of the manuscript. All authors commented on previous versions of the manuscript and have read and approved the final version.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Ethics Committee of all participating centers and performed in line with the principles of the Declaration of Helsinki.
Consent for publication
Informed consent was obtained from all study participants.
Competing interests
The authors declare that they have no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Yang, Y., Wei, J., Du, J. et al. Umbrella strategy with systemic and intraperitoneal chemotherapy versus systemic chemotherapy in patients with advanced gastric cancer: a multicenter, randomized Phase III clinical trial. CCB 2, 3 (2023). https://doi.org/10.1007/s44272-023-00003-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s44272-023-00003-7