
Abstract
The swift advancement of technology has led to the widespread utilization of artificial intelligence (AI) in the diagnosis of diseases and prediction of prognoses, particularly in the field of intensive care unit (ICU) and Anesthesia. Numerous evidential data have demonstrated the extensive potential of AI in monitoring and predicting patient outcomes in these fields. Using bibliometric analysis, this study provides an overview of the current state of knowledge regarding the application of AI in ICU and Anesthesia and investigates prospective avenues for future research. Web of Science Core Collection was queried on May 6, 2023, to select articles and reviews regarding AI in ICU and Anesthesia. Subsequently, various analytical tools including Microsoft Excel 2022, VOSviewer (version 1.6.16), Citespace (version 6.2.R2), and an online bibliometric platform were employed to examine the publication year, citations, authors, countries, institutions, journals, and keywords associated with this subject area. This study selected 2196 articles from the literature. focusing on AI-related research within the fields of ICU and Anesthesia, which has increased exponentially over the past decade. Among them, the USA ranked first with 634 publications and had close international cooperation. Harvard Medical School was the most productive institution. In terms of publications, Scientific Reports (impact factor (IF) 4.996) had the most, while Critical Care Medicine (IF 9.296) had the most citations. According to numerous references, researchers may focus on the following research hotspots: “Early Warning Scores”, “Covid-19″, “Sepsis” and “Neural Networks”. “Procalcitonin” and “Convolutional Neural Networks” were the hottest burst keywords. The potential applications of AI in the fields of ICU and Anesthesia have garnered significant attention from scholars, prompting an increase in research endeavors. In addition, it is imperative for various countries and institutions to enhance their collaborative efforts in this area. The research focus in the upcoming years will center on sepsis and coronavirus, as well as the development of predictive models utilizing neural network algorithms to improve well-being and quality of life in surviving patients.
Graphical Abstract

Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
The utilization of artificial intelligence (AI) in contemporary healthcare has flourished in light of scientific and technological advancements since its inception in the 1950s [1, 2]. AI entails the creation of intricate algorithms to manage complex tasks proficiently and effectively. Applying AI to healthcare aims to unveil concealed information in vast data sets and aid policymakers and clinicians in making sound clinical judgments [3]. Additionally, AI technology is employed to identify illnesses, screen individuals with cancer, determine therapies, mitigate medication errors, and enhance productivity [3,4,5,6].
Anesthesia and intensive care unit (ICU), as data-intensive disciplines, have created opportunities for the application of AI through the massive monitoring data and patient health data generated during perioperative and intensive care periods, particularly in the development of risk and outcome prediction models. These models offer a multitude of potential applications, such as augmenting clinical decision-making, fostering shared decision-making with patients and their families, identifying and mitigating health risks, preventing health issues, evaluating and regulating modifiable risk factors, mitigating care appropriately, enhancing evidence-based resource allocation decisions, and automating various processes [7].
In recent years, the swift advancement and progression of medical science have resulted in a substantial increase in the number of academic papers published annually, leading to a phenomenon known as information overload or filtering failure [8]. Scholars frequently encounter difficulties in comprehending the research trends and hotspots within a vast literature corpus. Researchers and stakeholders benefit from bibliometric analysis by gaining an informed understanding of their fields of study and encouraging interdisciplinarity [9]. It can not only enable researchers to gain a clearer overview of the research on a given topic but also identifies research abundancies, gaps, and trends of potential moderators [9].
Through the analysis of bibliometric data and visualization network patterns, this study identifies the emerging topics, publication patterns, global collaborations, research trends, and research domains in the field of AI as applied to ICU and Anesthesia. The study aims how AI-related knowledge in publications is used in the field of ICU and Anesthesia, provides a broad synthesis of research areas, shows how it has changed over time, and identifies impactful research.
2 Methods
2.1 Source and data collection
The data derived from the Science Citation Index Expanded (SCI-Expanded) of the Web of Science Core Collection (WoSCC) is deemed representative, readily accessible, and extensively employed within the realm of bibliometrics [10, 11]. To ensure the accuracy and comprehensiveness of the data, two impartial researchers independently obtained publications pertaining to artificial intelligence in the field of ICUs that were published on May 6, 2023, with the aim of verifying that no updates had been made to the data.
The primary subject terms encompass "ICU" "Anesthesia" and "artificial intelligence". Search strategy = (TS (Topics)= (intensive care units) OR TS = (ICU) OR TS = (Critical Care Medicine) OR TS = (Anaesthesi*)) AND TS = ("artificial intelligence" OR "robotic*" OR "expert*system*" OR "intelligent learning" OR "feature*extraction" OR "feature*mining" OR "feature*learning" OR "machine learning" OR "feature*selection" OR "unsupervised clustering" OR "image*segmentation" OR "supervised learning" OR "semantic segmentation" OR "deep network*" OR "Bayes*network" OR "deep learning" OR "neural network*" OR "neural learning" OR "neural nets model" OR "artificial neural network" OR "data mining" OR "graph mining" OR "data clustering" OR "big data" OR "knowledge graph").
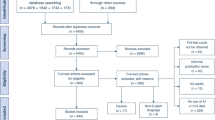
In addition, document types were limited to originals and reviews. And language was restricted to English. (Fig. 1).

Flowchart of the searching stage in the study. SCI-Expanded, Science Citation Index Expanded
2.2 Data analysis and data visualization
The institutions and countries with the highest productivity and citation rates were analyzed and graphed using R software (v4.1.2.) and Microsoft Excel 2022. The visualization tools employed included VOSviewer (version 1.6.16) [12, 13], Citespace (version 6.2.R2) [14,15,16], and an online platform for bibliometric analysis [17]. The online platform (https://bibliometric.com/) was utilized to generate visual representations of country/region cooperation networks and publication quantities [10]. The resulting knowledge maps exhibited a network of nodes and links that conveyed significant information. The sizing of nodes in a map is determined by the frequency of their respective items, including country/region, journal, and institution. The presence of cooperation, co-occurrence, and co-citation between two nodes establishes a relationship between them. Nodes that exhibit elevated centrality and burstness scores are likely to possess high importance.
In CtieSpace various structural metrics are commonly employed to assess the significance of nodes, such as betweenness centrality (BC), burstness, and sigma score. Nodes exhibiting BC values exceeding 0.1 are distinguished by purple rings, signifying their extensive connections with other nodes in the network [18]. Citation burst, which gauges the magnitude and duration of sudden shifts in the scientific community in response to a given publication or keyword, is represented by red rings for nodes with pronounced citation bursts [19]. Nodes with high centrality and burstness scores exhibit correspondingly high sigma scores. Additionally, VOSviewer employs the total link strength (TLS) index to quantitatively measure link strength, which was used to measure link strength quantitatively [13, 20]. More detailed descriptions of the maps are available at https://www.vosviewer.com/documentation.
3 Results
3.1 Analysis of publications and citations according
Utilizing the aforementioned screening strategy, a total of 2196 documents were amassed from WoSCC, comprising 1962 original articles and 234 reviews, spanning the temporal range of 2001–2022 (Fig. 1). Figure 2 illustrates a consistent annual increase in AI research pertaining to ICU and Anesthesia since 2001. with a notable surge in the last five years, accounting for nearly 70% of all publications on AI publications. At the endpoint of the search period, the total number of citations for all papers amounted to 35,960, with an average citation rate of 16.38 per item and the h-index was 79. Presently, researchers are directing their attention toward the application of AI to the ICU and Anesthesia.

Global trend of publications and total citations on Al research in ICU from 2001 to 2022. AI artificial intelligence. ICU intensive care unit
3.2 Analysis of top productive countries/regions
All publications were distributed in 81 countries/regions. As evidenced by Fig. 3A and Table 1, the world map depicted in the aforementioned sources revealed that the United States, China, England, and Italy were among the countries/regions with over 100 articles. Figure 3B provides an overview of the publishing patterns of the top 10 countries/regions, while Supplementary Table S1 illustrates that the United States was the leading country/regions with 634 articles, followed by China (323), England (117), and Italy (104). In addition, the United States also ranked first in the total number of citations (14,949). Figure 3C demonstrated that the United States collaborated with numerous countries/regions such as China, England, and Italy, but there is a lack of cooperation between other nations/regions. Additionally, Fig. 3D depicts the collaborative efforts of various countries/regions, as analyzed by VOSviewer, with a total of 34 countries/regions being considered in the calculations, provided that the minimum number of publications exceeded 10. The co-authorship visualization map reveals that the top five countries/regions with the highest total link strength are the United States, England, Italy, China, and Germany.

Analysis of Top Productive Countries/Regions. A World map based on the total publications of different countries/regions. B The trend of the annual publication quantity in the top 10 countries/regions from 2001 to 2021. C The international collaborations' visualization map of countries/regions. The thickness of the line between countries reflects the frequency of the cooperation. D The countries/regions' citation network visualization map generated by using VOSviewer. The thickness of the lines reflected the citation strength
3.3 Analysis of top institutions
The study on artificial intelligence in ICU and Anesthesia involved the participation of 2756 institutions. The top ten institutions with the highest number of contributions are presented in Table 1, with Harvard Medical School, Stanford University, and the University of Pittsburgh occupying the top three positions, having contributed 51, 33, and 33 articles. Notably, eight out of the top ten institutions are based in the United States. Supplementary Figure S1A illustrates that 86 institutions have published more than eight papers, with Harvard Medical School (TLS = 86) and the University of California, San Francisco (TLS = 84), and the University of Pennsylvania (TLS = 78) the top three institutions. Furthermore, the cooperation among institutions is illustrated in Supplementary Figure S1B. Notably, the University of California System, Boston Children's Hospital, University of Oxford, Columbia University, and University of California Berkeley are identified as hub nodes that have BC values above 0.1. These nodes are distinguished by purple rings, signifying their extensive connections to numerous other nodes [21, 22].
3.4 Analysis of top journal
The papers have been disseminated across 652 journals, with 68 of them containing no less than five articles. Supplementary Table S2 presents the journals that exhibited the highest productivity, namely Scientific report (N = 50), PLoS One (N = 43), and Journal of Biomedical Informatics (N = 33). Furthermore, Critical Care Medicine was cited 1056 times, surpassing all other journals significantly. VOSviewer's visualization maps of citing and co-cited journals, depicted in Supplementary Figure S2A, B, revealed numerous journals with active citation relationships co-occurring in both maps. The dual map of journals in Supplementary Fig. 2C shows the relationship between citing and cited journals. Based on the citation paths, two main types of citations were observed. There is mainly one field of citing papers: Medicine, Medical, Clinical. While the cited papers were concentrated in two fields: (1) Molecular, Biology, Genetics; (2) Health, Nursing, Medicine.
3.5 Analysis of top cited references and co-citation references
Utilizing the g-index [23], a yearly personal network, containing a total of 688,720 references, is constructed by identifying the most frequently cited papers from 2001 to 2022 (Fig. 4). The analysis of Fig. 4A reveals 1020 nodes and 1956 links, with a Modularity Q of 0.8716 and a Silhouette S of 0.9225, indicating a favorable clustering effect and network homogeneity. Figure 4B presents a chronological representation of each cluster, showcasing the most cited references within each cluster. The Log-Likelihood Ratio (LLR) method was employed for this analysis. Table 2 presents a comprehensive list of 11 major cluster labels. The cluster with the highest number of occurrences was identified as "early warning scores" (#0) [24, 25], while "telemedicine" (#7) [26, 27] and "brain injuries" (#13) [28, 29] were among the earliest research topics in this field. Currently, "early warning scores" (#0), "covid-19" (#1) [30, 31], and "neural networks" (#3) [32, 33] are the most popular research areas Table 3 outlines the top 10 co-cited references, with the reference published by Johnson A.E.W. receiving the highest number of citations. Additionally, Supplementary Table S3 provides a list of the top 5 cited references and citing articles for Cluster #1 covid-19.

Citespace visualization map of Cluster view. A Timeline view and B Co-citation references. The time evolution is indicated with different coloured lines, and the nodes on the lines indicate the references cited. C CiteSpace visualization map of the top 25 references with the strongest citation bursts from 2001 to 2022. Citation burst is represented by red rings for nodes with pronounced citation bursts
3.6 Analysis of Keyword Co-Occurrence
The VOSviewer software was utilized to generate an overlay visualization map of keywords, following the merging of synonyms and meaningless keywords. The map incorporates a total of 3991 author keywords, with 74 keywords appearing in at least 10 instances in Fig. 5A. Additionally, Table 4 presents the top 20 co-occurrence author keywords that are most frequently observed. Notably, yellow nodes in Fig. 5A represent recently emerging keywords, such as "covid-19", "machine learning", "sepsis", and "deep learning", among others. These keywords serve to summarize current research frontiers. Keywords with strong bursts in the top 20 through Citespace are illustrated in Fig. 5B. By merging the most prevalent keywords in Fig. 5A with those in Fig. 5B, the keywords that demonstrate continuous citation bursts until 2022 are "procalcitonin", "convolutional neural networks (CNN)", "deep learning", and "covid-19". These keywords were of particular interest to us due to their efficacy in identifying frontiers in AI in ICU and Anesthesia.

Analysis of Keyword Co-Occurrence. A The time-overlay visualization map of the co-occurrence keywords generated by using VOSviewer. B CiteSpace visualization map of top 24 keywords with the strongest citation bursts of publications in the field of predictive models in postoperative complications from 2001 to 2022. Citation burst is represented by red rings for nodes with pronounced citation bursts
4 Discussion
4.1 General information
Over the last two decades, the field of AI has undergone rapid evolution, [34, 35], resulting in a significant increase in its utilization within the ICU and Anesthesia domains. A 2016 multicenter observational study by Matthew M. Churpek found that several machine learning methods predicted clinical deterioration more accurately than logistic regression [25]. The use of AI in ICU began to explode. Notably, within the past five years, more than half of all publications have focused on this area of research. The USA has demonstrated the highest productivity, with 634 papers published, surpassing all other countries worldwide. However, there has been a gradual rise in papers from China, England, and other countries, indicating a growing interest among researchers in applying AI in these regions. The expeditious progress of AI has been propelled by advancements in machine learning and deep learning. The findings revealed that the mean citations per article and total citations per article were significantly greater in the United States compared to other countries (Supplementary Table S1). Furthermore, within the University of Florida, Bihorac Azra, who holds the highest number of publications, introduced the development of MySurgeryRisk. This framework utilizes automated predictive analytics and machine learning algorithms, demonstrating a remarkable ability to accurately evaluate the likelihood of surgical complications and mortality [36]. Despite China ranking second in terms of published articles, the total number of citations was only 2901, with an average citation of 8.9, which was even lower than that of England (3223 cited, Average Article Citations = 27.54). China's paper output has increased; however, the quality of the articles remains suboptimal. This may be attributed to two factors: (1) the delayed initiation of AI research in ICU and Anesthesia in China, which has resulted in limited global academic influence. (2) Despite significant advancements, the core algorithms of AI have not been innovative enough, and there has been a lack of collaboration with international experts.
Furthermore, it is noteworthy that eight out of the top ten institutions in the field of AI application in ICU and Anesthesia are based in the United States. This underscores the importance for institutions from other countries to establish and maintain close collaborations with American counterparts to facilitate globalization and advancement in this area. Notably, Critical Care Medicine received more citations than other journals in this field, indicating its remarkable influence. Moreover, journals such as Scientific Reports, Journal of Biomedical Informatics, Critical Care, and Artificial Intelligence in Medicine demonstrated high productivity as well. Furthermore, the potential for the publication of additional exists, which could enhance their impact factor and academic prestige.
Through co-authorship analysis, it was determined that the United States served as the hub of AI in ICU and Anesthesia with strong collaborative ties to England, Italy, and China. While Harvard Medical School exhibited close cooperation with the Massachusetts Institute of Technology and the University of Pittsburgh, the majority of institutions were loosely clustered, with a density of only 0.0153, indicating an absence of international cooperation among institutions.
4.2 Knowledge base
Co-citation analysis provides a pragmatic approach to assessing the degree of interconnection among scholarly articles. Papers that garner a high frequency of citations are typically deemed more significant in this domain. The top 10 co-citations in Table 5 are all well-known papers.
Over the course of the last 22 years, there has been a consistent rise in the number of articles pertaining to artificial intelligence, with a significant surge in growth observed since 2016. Analysis of the most co-cited articles suggests that this trend may be attributed to three key factors: (1) the report by Johnson et al. [23] on the MIMIC-III database, a large centralized database that offers open access to samples for the development of various clinical research models in the future; (2) he effectiveness of tree boosting as a machine learning technique for solving real-world problems with minimal resources, as highlighted by Chen et al. [37]. Tree boosting is an effective machine learning method capable of solving real-world problems with minimal resources. Churpek et al. [25] demonstrated the superior predictive accuracy of machine learning algorithms over traditional regression methods, with the random forest model emerging as the most precise approach for handling large datasets. (3) Singer [38] redefined the clinical definitions of sepsis and septic shock, and introduced the Sequential [Sepsis-related] Organ Failure Assessment (SOFA) score.
In the same year, Desautels T. [39] used machine learning to establish Insight scores for sepsis, which were superior to all previous scores. Nemati S. used artificial intelligence to establish early recognition scores and risk factors for sepsis [40]. In 2018, Pollard T. J. [24] described the eICU collaborative research database, which covers over 200,000 ICU admissions monitored by eICU projects across the United States and is open source for free. Rajkomar A. [32] used the Fast Healthcare Interoperability Resources format to construct a deep learning predictive model and demonstrated that this model outperforms traditional clinical predictive models in all cases. And can be used to create accurate and scalable predictions for various clinical scenarios.
As of 2019, a comprehensive account of the clinical trajectory and risk factors linked to COVID-19, encompassing viral shedding, has yet to be documented. As the original investigator, Zhou F. [30] employed the generalized linear model to pinpoint older patients, those with elevated SOFA scores, and individuals with d-dimer levels exceeding 1 mug/mL as potential risk factors for unfavorable prognosis.
4.3 Emerging hotspots
Timeline views of co-cited references provided researchers with a visual representation of the dynamic evolution and hotspots in research of AI on ICU and Anesthesia. Figure 4B showed that the research focus has shifted from #5 big data #7 telemedicine study and #10 epidemiology, #13 brain injuries and #11 arrhythmia to #0 early warning scores, #1 covid-19, #2 sepsis, #3 neural networks, #4 hypotension, and #6 machine learning.
In 2019, the outbreak of COVID-19 resulted in a significant surge in the number of patients. Consequently, the diagnosis, risk prediction, and prognosis judgment of COVID-19 patients became a top priority. AI methods have emerged as critical tools for leveraging the rapidly expanding pool of COVID-19-positive patient datasets. As of July 1, 2020, Wynants L. [31] employed PROBAST (Predictive Model Bias Risk Assessment Tool) to evaluate the bias risk of 169 studies and 232 predictive models. The results revealed that the Jehi diagnostic model and the 4C mortality score exhibited promising potential. Adamidi E.S. [41] conducted a comparative analysis of six widely used artificial intelligence classification algorithms, namely random forest, linear regression, support vector machine, convolutional neural network (CNN), decision tree, and XGBoost, by examining 101 studies published between January 1, 2020, and December 30, 2020, in the context of COVID-19. The study found that CNN demonstrated superior performance in machine learning applications, particularly in imaging studies. The authors suggest that emerging technologies such as explainable AI and Federated Learning could play a crucial role in addressing dynamic crises such as the COVID-19 pandemic.
Artificial neural networks represent a prevalent type of machine learning modeling that draws inspiration from biological neural networks. These networks are widely used as classifier algorithms [42] and are most readily comparable to gradient-boosting methods. Comprising neural layers, including an input layer, one or more hidden layers, and an output layer, artificial neural networks have gained significant popularity. There are two common types of neural networks, including recurrent neural networks that can process large amounts of data and "learn" from missed predictions, and convolutional neural networks that specialize in transforming imaging data [43]. In recent years, neural networks have developed rapidly in pain, and Wu C. L. [44] has used a variety of CNN models to construct a pain evaluation model based on facial expressions. Found to have high performance. Besides, Chelazzi C. [45] used neural networks to develop SUMPOT, a new postoperative complication prediction model, which showed high accuracy in postoperative pain and other complications. More importantly, CNN performs well in machine learning problems compared to other supervised and unsupervised machine learning [46].
4.4 Limitations
Despite the rigorous nature of the bibliometric analysis, certain limitations were inevitable. Firstly, research results may involve international cooperation with different countries., which may lead to deviations in the study's retrieved institutional affiliations. Secondly, although WoSCC is the most commonly used database in scientific econometric analysis, and can represent a significant amount of information, there may still be some loss in paper collection. Additionally, the latest publications may not have had sufficient time to be cited, which might have had some impact on the overall results.
5 Conclusion
Overall, this study presents the enhanced quantitative bibliometric analysis that delineates the knowledge map of artificial intelligence in the domains of ICU and Anesthesia from 2001 to 2022 and prognosticates future research trends. The findings indicate that the United States exhibited the highest degree of international communication and collaboration and produced the most superior publications. However, there is a need for further improvements among organizations. Furthermore, the algorithm that garnered the highest usage in model creation was the "neural network", while the focal points of interest were Covid-19 and sepsis. Through further investigation in this field, more precise predictive models can be developed to assess the likelihood of associated illnesses and ultimately decrease mortality rates.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.
Abbreviations
- AI:
-
Artificial intelligence
- BC:
-
Betweenness centrality
- CNN:
-
Convolutional neural networks
- ICU:
-
Intensive care unit
- IF:
-
Impact factor
- LLR:
-
Log-likelihood ratio
- SCI-Expanded:
-
Science Citation Index Expanded
- SOFA:
-
Sequential organ failure assessment score
- TLS:
-
Total link strength
- TS:
-
Topics
- WoSCC:
-
Web of Science Core Collection
References
Kermany DS, Goldbaum M, Cai W, Valentim CCS, Liang H, Baxter SL, et al. Identifying medical diagnoses and treatable diseases by image-based deep learning. Cell. 2018;172(5):1122–1131.e9.
Miotto R, Wang F, Wang S, Jiang X, Dudley JT. Deep learning for healthcare: review, opportunities and challenges. Brief Bioinform. 2018;19(6):1236–46.
Jiang F, Jiang Y, Zhi H, Dong Y, Li H, Ma S, et al. Artificial intelligence in healthcare: past, present and future. Stroke Vasc Neurol. 2017;2(4):230–43.
Islam MM, Poly TN, Walther BA, Yang HC, Li YJ. Artificial intelligence in ophthalmology: A meta-analysis of deep learning models for retinal vessels segmentation. J Clin Med. 2020;9(4):1018.
Islam MM, Yang HC, Poly TN, Jian WS, Jack Li YC. Deep learning algorithms for detection of diabetic retinopathy in retinal fundus photographs: A systematic review and meta-analysis. Comput Methods Programs Biomed. 2020;191:105320.
Murdoch TB, Detsky AS. The inevitable application of big data to health care. JAMA. 2013;309(13):1351–2.
Gorges M, Ansermino JM. Augmented intelligence in pediatric anesthesia and pediatric critical care. Curr Opin Anaesthesiol. 2020;33(3):404–10.
Kreps GL, Neuhauser L. Artificial intelligence and immediacy: designing health communication to personally engage consumers and providers. Patient Educ Couns. 2013;92(2):205–10.
Niu B, Hong S, Yuan J, Peng S, Wang Z, Zhang X. Global trends in sediment-related research in earth science during 1992–2011: a bibliometric analysis. Scientometrics. 2013;98(1):511–29.
Zhang F, Xia Q, Zhang L, Wang H, Bai Y, Wu W. A bibliometric and visualized analysis of early mobilization in intensive care unit from 2000 to 2021. Front Neurol. 2022;13:848545.
Shen Z, Wu H, Chen Z, Hu J, Pan J, Kong J, et al. The global research of artificial intelligence on prostate cancer: A 22-year bibliometric analysis. Front Oncol. 2022;12:843735.
Yu Y, Li Y, Zhang Z, Gu Z, Zhong H, Zha Q, et al. A bibliometric analysis using VOSviewer of publications on COVID-19. Ann Transl Med. 2020;8(13):816.
van Eck NJ, Waltman L. Software survey: VOSviewer, a computer program for bibliometric mapping. Scientometrics. 2010;84(2):523–38.
Synnestvedt MB, Chen C, Holmes JH. CiteSpace II: visualization and knowledge discovery in bibliographic databases. AMIA Annu Symp Proc. 2005. p. 724–8.
Chen C, Dubin R, Kim MC. Emerging trends and new developments in regenerative medicine: a scientometric update (2000–2014). Expert Opin Biol Ther. 2014;14(9):1295–317.
Chen C. Searching for intellectual turning points: progressive knowledge domain visualization. Proc Natl Acad Sci U S A. 2004;101 Suppl 1:5303–10.
Wu H, Tong L, Wang Y, Yan H, Sun Z. Bibliometric analysis of global research trends on ultrasound microbubble: A quickly developing field. Front Pharmacol. 2021;12:646626.
Wu H, Wang Y, Tong L, Yan H. Global research trends of ferroptosis: A rapidly evolving field with enormous potential. Front Cell Dev Biol. 2021;9:646311.
Chen C, Hu Z, Liu S, Tseng H. Emerging trends in regenerative medicine: a scientometric analysis in CiteSpace. Expert Opin Biol Ther. 2012;12(5):593–608.
Wu H, Li Y, Tong L, Wang Y, Sun Z. Worldwide research tendency and hotspots on hip fracture: a 20-year bibliometric analysis. Arch Osteoporos. 2021;16(1):73.
Wu H, Zhou Y, Xu L, Tong L, Wang Y, Liu B, et al. Mapping knowledge structure and research frontiers of ultrasound-induced blood-brain barrieropening: A scientometric study. Front Neurosci. 2021;15:706105.
Gao J, Xing D, Dong S, Lin J. The primary total knee arthroplasty: a global analysis. J Orthop Surg Res. 2020;15(1):190
Johnson AE, Pollard TJ, Shen L, Lehman LW, Feng M, Ghassemi M, et al. MIMIC-III, a freely accessible critical care database. Sci Data. 2016;3:160035.
Pollard TJ, Johnson AEW, Raffa JD, Celi LA, Mark RG, Badawi O. The eICU Collaborative Research Database, a freely available multi-center database for critical care research. Sci Data. 2018;5:180178.
Churpek MM, Yuen T, Winslow C, Meltzer DO, Kattan MW, Edelson DP. Multicenter comparison of machine learning methods and conventional regression for predicting clinical deterioration on the wards. Crit Care Med. 2016;44(2):368–74.
Young LB, Chan PS, Lu X, Nallamothu BK, Sasson C, Cram PM. Impact of telemedicine intensive care unit coverage on patient outcomes: a systematic review and meta-analysis. Arch Intern Med. 2011;171(6):498–506.
Lilly CM, Cody S, Zhao H, Landry K, Baker SP, et al. Hospital mortality, length of stay, and preventable complications among critically ill patients before and after tele-ICU reengineering of critical care processes. JAMA. 2011;305(21):2175–83.
Aboukhalil A, Nielsen L, Saeed M, Mark RG, Clifford GD. Reducing false alarm rates for critical arrhythmias using the arterial blood pressure waveform. J Biomed Inform. 2008;41(3):442–51.
Sayadi O, Shamsollahi MB. Life-threatening arrhythmia verification in ICU patients using the joint cardiovascular dynamical model and a Bayesian filter. IEEE Trans Biomed Eng. 2011;58(10):2748–57.
Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020;395(10229):1054–62.
Wynants L, Van Calster B, Collins GS, Riley RD, Heinze G, Schuit E, et al. Prediction models for diagnosis and prognosis of covid-19: systematic review and critical appraisal. BMJ. 2020;369:m1328.
Rajkomar A, Oren E, Chen K, Dai AM, Hajaj N, Hardt M, et al. Scalable and accurate deep learning with electronic health records. NPJ Digit Med. 2018;1:18.
Esteva A, Kuprel B, Novoa RA, Ko J, Swetter SM, Blau HM, et al. Dermatologist-level classification of skin cancer with deep neural networks. Nature. 2017;542(7639):115–8.
Falini S, Angelotti G, Cecconi M. ICU management based on big data. Curr Opin Anaesthesiol. 2020;33(2):162–9.
Datta R, Singh S. Artificial intelligence in critical care: Its about time! Med J Armed Forces India. 2021;77(3):266–75.
Bihorac A, Ozrazgat-Baslanti T, Ebadi A, Motaei A, Pardalos PM, et al. MySurgeryRisk: Development and validation of a machine-learning risk algorithm for major complications and death after surgery. Ann Surg. 2019;269(4):652–62.
Chen T, Guestrin C. XGBoost: A scalable tree boosting system. KDD16: Proceedings of the 22nd acm sigkdd international conference on knowledge discovery and data mining; 2016 Aug 13–17; San Francisco: Association for Computing Machinery; 2016. p. 785–94.
Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M, et al. The third international consensus definitions for sepsis and septic shock (sepsis-3). JAMA. 2016;315(8):801–10.
Desautels T, Calvert J, Hoffman J, Jay M, Kerem Y, Shieh L, et al. Prediction of sepsis in the intensive care unit with minimal electronic health record data: A machine learning approach. JMIR Med Inform. 2016;4(3):e28.
Nemati S, Holder A, Razmi F, Stanley MD, Clifford GD, Buchman TG. An interpretable machine learning model for accurate prediction of sepsis in the ICU. Crit Care Med. 2018;46(4):547–53.
Adamidi ES, Mitsis K, Nikita KS. Artificial intelligence in clinical care amidst COVID-19 pandemic: A systematic review. Comput Struct Biotechnol J. 2021;19:2833–50.
Gutierrez G. Artificial Intelligence in the Intensive Care Unit. Crit Care. 2020;24(1):101.
Farhat A, Shah N, Wang Z, Raman L. Machine learning: Brief overview for biomedical researchers. J Transl Sci. 2019. https://doi.org/10.15761/JTS.1000343.
Wu CL, Liu SF, Yu TL, Shih SJ, Chang CH, Yang Mao SF, et al. Deep learning-based pain classifier based on the facial expression in critically Ill patients. Front Med (Lausanne). 2022;9:851690.
Chelazzi C, Villa G, Manno A, Ranfagni V, Gemmi E, Romagnoli S. The new SUMPOT to predict postoperative complications using an artificial neural network. Sci Rep. 2021;11(1):22692.
Shah N, Arshad A, Mazer MB, Carroll CL, Shein SL, Remy KE. The use of machine learning and artificial intelligence within pediatric critical care. Pediatr Res. 2023;93(2):405–12.
Acknowledgements
We kindly thank the AI-anesthesiology group members who were involved in this study. The Graphical Abstract in the manuscript were drawn in Figdraw.
Funding
This research was partly funded by the National Key R&D Program of China (NO. 2018YFC2001800) and CAMS Innovation Fund for Medical Sciences (NO. 2019-I2M-5011); Funding acquisition: Xuechao Hao and Tao Zhu.
Author information
Authors and Affiliations
Contributions
Congjun Li and Ruihao Zhou performed the experiments, analyzed the data, prepared figures and/or tables and drafted the manuscript. Guo Chen, Xuechao Hao and Tao Zhu: conceptualization and supervision. Congjun Li, Ruihao Zhou and Guo Chen: methodology, data validation. Congjun Li and Ruihao Zhou: review and draft editing.
Funding support was supplied by Xuechao Hao and Tao Zhu. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
Dr. Tao Zhu is a member of the Editorial Board in Anesthesiology and Perioperative Science and recuses himself from every editorial procedure of this submission including peer-review and academic decisions. The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Li, C., Zhou, R., Chen, G. et al. Knowledge mapping and research hotspots of artificial intelligence on ICU and Anesthesia: from a global bibliometric perspective. APS 1, 33 (2023). https://doi.org/10.1007/s44254-023-00031-5
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1007/s44254-023-00031-5