
Abstract
Objective
To characterize outcomes of paediatric moderate-to-severe traumatic brain injury (TBI), defined by a Glasgow Coma Scale (GCS) ≤ 12.
Design
Retrospective, single-centre cohort study (July 2010 and June 2020).
Setting
Medical-surgical tertiary paediatric intensive care unit (PICU) in a level 1 university medical trauma centre.
Patients
One-hundred and thirty subjects < 18 years (moderate N = 56, severe N = 74).
Measurements and main results
Subjects were stratified according to favourable (Paediatric Cerebral Performance Category [PCPC] Scale ≤ 3) and poor (PCPC ≥ 4) neurological outcome determined at PICU discharge. One-hundred and six patients (81.5%) had PCPC ≤ 3; of those, N = 55 (52%) had moderate TBI and N = 51 (48%) severe TBI. Twelve patients (9.2%) died, of whom eight (66.7%) within 24 h of PICU admission. Intracranial pressure (ICP) monitoring was performed in N = 12 (50%) patients with PCPC ≥ 4 and in N = 15 (14.2%) patients with PCPC ≤ 3. No clinically relevant differences in serum sodium, glucose, temperature, or blood pressure management during the first 72 h of PICU admission were observed between patients with and without favourable outcome. Mortality was highest among patients with severe TBI (N = 11, 14.9%). Among survivors with PCPC ≥ 4, N = 11 (91.7%) were discharged to a rehabilitation facility compared to N = 22 (20.8%) with PCPC ≤ 3.
Conclusion
Severe paediatric TBI (pTBI) remains an important cause of serious morbidity and mortality. Patients with moderate pTBI had a favourable outcome at PICU discharge, although the outcome measurement used may not be granular enough to discriminate. Follow-up after discharge is essential to optimize outcome on physical, cognitive, behavioural, and social functioning.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Traumatic brain injury (TBI) remains a major cause of mortality and long-term disability in children worldwide, affecting more than 3 million children every year with a conservative incidence estimate of 50 per 100,000 persons [1]. Approximately, 1 out of 7 children with TBI seeking emergency medical care from hospitals suffer from moderate-to-severe TBI, with mortality rates in severe TBI up to 24% [2,3,4]. Many factors ultimately influence the outcome of paediatric TBI (pTBI) patients. The non-modifiable primary brain injury resulting from an external force is subsequently followed by a pathophysiologic cascade of events, including cerebral swelling, metabolic disturbances, seizures, cerebral vasospasms, and neuroinflammation which all contribute to secondary injury. The resulting sustained elevated intracranial pressure (ICP) is a key variable, as high ICP may further impair blood flow, thereby causing brain ischemia [5,6,7].
Clinical management of pTBI patients admitted to the paediatric intensive care unit (PICU) is targeted at limiting this secondary injury. However, there is little high-quality scientific evidence that supports the current management of pTBI. Randomized controlled trials evaluating management of moderate and severe TBI in children are very scarce [5, 8]. This lack of good evidence is reflected in the international guidelines for severe pTBI, at best providing level II recommendations [6]. However, it has also been reported that patients with moderate pTBI (i.e. those with Glasgow Coma Scale [GCS] 8–12) may suffer from physical and cognitive impairments and reduced adaptive functioning [2, 3, 9]. Also, the initial assessment of GCS is not always accurate and may lead to over- or underestimation of neurological severity [10]. As such, therapeutic interventions targeted for patients with severe TBI may potentially also offer outcome benefits in patients with moderate TBI. We therefore sought to characterize the outcomes of a cohort of children with moderate-to-severe TBI by using the Paediatric Cerebral Performance Category (PCPC) as we did not have data on more extensive psychometric testing after PICU admission [11, 12].
Materials and methods
Study population
This study was designed as a descriptive, retrospective study obtained from written and electronical health records of children < 18 years with moderate to severe TBI (GCS ≤ 12) admitted between July 2010 and June 2020 to the PICU of the Beatrix Children’s Hospital/University Medical Center Groningen (UMCG), a level 1 trauma centre. Patients with (suspected) abusive head trauma were excluded. The Institutional Review Board approved the study and waived the need for informed consent (Institutional Review Board UMCG, METc2021/534).
PICU management of children with TBI is guided by local practice algorithms based on the international paediatric guidelines [6]. Updates of these international guidelines were also implemented in our local practice algorithm. Depending on severity of injury, patients were mechanically ventilated in a time-cycled, pressure-limited mode of ventilation. All ventilated patients received analgesia and sedation by continuous intravenous infusion with benzodiazepines, opioids, and/or propofol. Wake-up calls were done at the discretion of the physician in charge if interruption of sedatives was not contraindicated, e.g. stable ICP < 20 mmHg and stable cerebral perfusion pressure or no clinical signs of raised ICP. After our local clinical algorithm was revised in 2017, amplitude integrated electroencephalography was used in all patients for detection of subclinical epileptic activity. Insertion of an ICP manometer was ultimately at the discretion of the attending neurosurgeon. A stepwise approach was used when there were signs of acute intracranial hypertension (for patients with ICP monitoring ICP > 20 mmHg for at least 5 min or bradycardia ± relative hypertension in patients without ICP monitoring), including checking for optimal baseline care and administration of hyperosmolar agents, with a shift in time from the use of mannitol towards the use of hypertonic saline. Cranial computed tomography scans were evaluated by one (paediatric) radiologist at the time of PICU admission and not reanalysed for this study.
Data collection
We collected baseline patient characteristics, trauma mechanism, the presence of associated lesions, data on (pre-) hospital treatment, radiological features on the first cranial computed tomography, and clinical, physiological and laboratory data from the first 7 days of PICU admission (definitions are described in Supplemental Table 1). The Paediatric RISk of Mortality II (PRISM-II) — 24-h score was calculated to assess patient acuity [13]. The GCS and paediatric trauma score were calculated to assess TBI and trauma severity [14, 15].
Endpoints
Favourable outcome was defined by PCPC ≤ 3, reflecting normal outcome, mild and moderate disability. Poor outcome was defined by PCPC scale ≥ 4, reflecting severe disability, coma or vegetative state and death or brain death [11]. PCPC score was determined at PICU discharge using discharge notes and letters. Secondary outcomes included mortality < 24 h of admission, PICU-free days at day 28 (defined as the number of days alive and out of the PICU during the first 28 days), PICU and hospital length of stay (LOS), ventilator days, GCS at PICU discharge and discharge status (home, other hospital or rehabilitation facility). Patients who died before PICU discharge within 28 days were assigned zero PICU-free days.
Statistical analysis
We stratified patients by PCPC (i.e. ≤ 3 and ≥ 4). Categorical variables were described as absolute number and percentage (%) of total and continuous variables as median and interquartile range (IQR). Continuous variables were analysed with the Mann–Whitney U-test, and categorical data was analysed using the χ2 test (Fisher exact test if the value of any cell was < 5). The Wilcoxon signed-rank test was used for repeated measurements comparing weighted means from days 0–1 to 2–3 of PICU admission. All analyses were performed with SPSS v23.0 (IBM Statistical Package for the Social Sciences [SPSS] for Windows, Armonk, NY: IBM Corp.). P-values < 0.05 were accepted as statistically significant.
Results
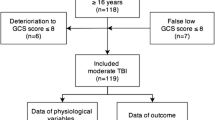
During the study period, 434 patients with the admission diagnosis “trauma” were identified from the PICU database. After exclusion of patients without TBI (N = 201), mild TBI [i.e. GCS > 12] (N = 97) or (suspected) abusive head trauma (N = 6), data from 130 patients was eligible for analysis (Supplemental Fig. 1), of whom N = 56 (43.1%) had moderate TBI and N = 74 (56.9%) had severe TBI. One-hundred and six patients (81.5%) had favourable neurological outcome (i.e. PCPC ≤ 3) at PICU discharge (Fig. 1). Of those patients, N = 55 (51.9%) had moderate TBI and N = 51 (48.1%) severe TBI.

Paediatric Cerebral Performance Category Scale, percentage of patients per category split by severity of neurotrauma
Patients with accidental fall as the cause of injury significantly more often had favourable neurological outcome, N = 44 (97.8%). Regarding patients with PCPC ≥ 4, significantly more patients had lower GCS, lower initial motor score, bilateral dilated and fixed pupils, higher pre-hospital intubation rate, more associated lesions (including more thoracic trauma), more hypotension upon hospital arrival and more often pre-hospital cardiac arrest. Paediatric trauma score and PRISM II were significantly higher in patients with PCPC ≥ 4 (Table 1). All patients with PCPC ≥ 4 had cranial computed tomography lesions, with significantly more subdural hematomas, intraparenchymal and intraventricular haemorrhages, the presence of midline shift and absent cisterns, whereas 19% of patients with PCPC ≤ 3 had no cranial computed tomography lesions (Supplemental Table 2).
PICU-free days at day 28 were significantly lower in patients with PCPC ≥ 4 (median 0 days, IQR 0.0–16.7) compared to PCPC ≤ 3 (median 26.3 days, IQR 23.4–27.2). No significant difference in PICU LOS or hospital LOS between patients with PCPC ≤ 3 and PCPC ≥ 4 was found (Table 2). Patients with PCPC ≥ 4 had significantly more ventilator days and lower GCS at PICU discharge. Discharge to a rehabilitation facility was more common among surviving patients with PCPC ≥ 4 (N = 11 [91.7%]) compared with patients with PCPC ≤ 3 (N = 22 [20.8%]) (Table 2). Twelve patients (9.2%) died, of whom 8 (66.7%) within 24 h of PICU admission. Mortality was the highest among patients with severe TBI (N = 11 [14.9%]).
We found no difference in the number of patients with decompressive craniectomy between the two groups. All decompressive craniectomies were performed on the day of admission for evacuation of extracerebral hematomas. ICP monitoring was performed in N = 12 (50%) patients with PCPC ≥ 4 and in N = 15 (14.2%) patients with PCPC ≤ 3. The median age of these patients was 11.8 years, with an IQR of 8.4–14.9 year. Use of vasopressors, neuromuscular blocking agents and bolus(es) of hypertonic saline or mannitol was significantly more common in patients with PCPC ≥ 4 during the first 72 h of PICU admission. We also observed that more patients with PCPC ≥ 4 were on benzodiazepines, opioids or propofol during days 2–3 (Table 3). Also, initiation of enteral feeding in the first 72 h of admission was significantly lower in this category.
Except for significant differences between patients with PCPC ≤ 3 and PCPC ≥ 4 in weighted averaged serum sodium concentrations and temperature on days 0–1 (140 mmol/l vs. 144 mmol/l and 36.9 °C vs 36.5 °C), days 2–3 (141 mmol/l vs. 145 mmol/l and 37.2 °C vs. 36.8 °C), and serum glucose on days 0–1 (6.0 mmol/l vs. 7.2 mmol/l) (Fig. 2), no other differences were observed (Supplemental Table 3). In approximately one-third of patients in both outcome groups, we observed mean arterial blood pressure [(MAP)] between p5-and p50 (N = 32 [34.4%] vs. N = 8 [36.4%]) on days 0–1 and N = 20 (41.7%) vs. N = 6 (37.5%) on days 2–3 (Fig. 2).

Inhospital measurements on days 0–1 and days 2–3 categorized by Paediatric Cerebral Performance Category Scale ≤ 3 and Paediatric Cerebral Performance Category Scale ≥ 4
Discussion
In the present study, we observed significant morbidity and mortality in severe pTBI, whereas subjects with moderate TBI had a favourable outcome. Overall mortality rate was high and in two-thirds of the patients within the first 24 h of PICU admission, which is comparable to previously reported [16,17,18,19]. We observed similar differences in injury characteristics such as trauma mechanism [20], fixed pupils [16, 21,22,23,24] and low motor score [16, 25]. Significantly, more associated lesions were seen in the poor outcome group, including more thoracic injuries, which make patients prone to secondary injury due to hypoxia or hypovolemia [18, 21, 26]. These findings underscore the need for preventive measures despite advances in management and neuromonitoring in pTBI as it remains subject of debate if outcomes can significantly be improved by PICU management [7]. Thus, preventive measures, such as speed limits, traffic education and the use of bicycle helmets [27, 28], are key in reducing early mortality and long-term morbidity.
Similar to observations by others, fall and road traffic accident (either as pedestrian, cyclist or passenger) are the most common cause of trauma [1, 18, 29], with fall being more present in younger subjects and traffic accidents in older subjects [3, 30, 31]. We, like others, found that subjects with a fall had more often a favourable outcome despite the initial injury severity [20]. This may be explained by a different trauma impact compared with the acceleration-deceleration forces that account for immediate shearing of connective nerve fibres in traffic-related injuries [7].
While we found in our cohort that subjects with moderate pTBI almost all had favourable outcome at PICU discharge, it has been reported that these patients may suffer from long-term physical and cognitive impairments and reduced adaptive functioning [2, 3, 7, 9]. Also, initial assessment of GCS may not always be adequately representative for the injury severity. For example, the neurological status may have changed from the initial score assessed at the trauma scene to the score calculated in the emergency department, or the score may have been simply miscalculated. This may thus lead to over- or underestimation of the true neurological severity [10]. With this in mind, we therefore decided to include subjects with moderate pTBI as well in our analysis. Furthermore, it may be speculated that therapeutic interventions targeted for patients with severe TBI may also offer outcome benefits in patients with moderate TBI, although this remains to be further studied.
We acknowledge that our study is affected by the fact that we arbitrarily defined neurologic good outcome by PCPC ≤ 3 since data on Glasgow Outcome Scale-extended (GOS-E) or GOS-E Peds were unavailable [11, 12, 32, 33]. PCPC ≤ 3 includes patients with mild-to-moderate disability at PICU discharge, as reflected in the number of subjects in our cohort discharged to a rehabilitation facility. It can be argued that PCPC may not be granular enough to discriminate between good and poor outcome, and our study was not designed to explore long-term patient outcome. It is known that lifelong disability in physical, cognitive, behavioural and social function is common in patients with TBI [3, 34], although further neurological improvement from poor to favourable ≥ 6 months after PICU discharge may still occur [20]. One group of investigators reported that 61% of children with moderate-to-severe TBI required specialized medical and educational services 1 year after trauma [9]. Others found that almost two-third of patients with moderate-to-severe TBI functioned similar to normative age peers 10-year post-trauma [31]. This signifies the need for long-term follow-up to evaluate functional status over time and to intervene with appropriate rehabilitation to get the full potential for (complete) recovery [28, 35].
In principle, patients with especially severe pTBI were managed according to the international pTBI guidelines [6]. Nonetheless, we observed a low use of ICP monitoring. Due to the retrospective nature of the study and the limited number of data points, only weighted average analysis of ICP and CPP was done; a more detailed analysis considering minute-by-minute fluctuations in these parameters was not feasible. We did find statistically significant, but clinically irrelevant differences in serum sodium between subjects with PCPC ≤ 3 and ≥ 4, but this must be seen in the context of injury severity and more subjects with PCPC ≥ 4 receiving hypertonic saline or mannitol. As such, we could not confirm an association between serum sodium > 150 mmol/l and mortality [36], but this is probably due to the fact that we included subjects with moderate pTBI in our analyses. Nonetheless, it appears justified to implement advanced neuromonitoring or measurement of biomarkers for individualized post-trauma care to optimize outcome [37,38,39,40].
There are several limitations to our study that need to be discussed. First, our study was designed as a retrospective observational, single-centre study. This limits generalizability of our findings. Furthermore, data was obtained from the patient’s medical record; thus, inherently, clinical and outcome data may have been missing, leading to selection bias. Missing clinical data were not imputed. Second, although our unit implemented the international paediatric TBI guidelines, practice variability leading to confounding by indication (i.e. the sickest patient is the most likely to get a specific intervention) may have significantly impacted our study findings. This type of bias can only be overcome by randomization. Third, the period studied includes revisions from the international paediatric TBI guidelines in 2012 and 2019 [6]. Our study was not designed as a quality study, so we could not ascertain how changes in clinical management were implemented and thereby affected the primary outcome.
Conclusion
We report significant morbidity and mortality in subjects with severe pTBI, whereas subjects with moderate TBI had a favourable outcome. Overall mortality rate was high and in two-thirds of the patients within the first 24 h of PICU admission. Significantly more associated lesions were seen subjects with poor outcome. These findings underscore the need for preventive measures such as speed limits, traffic education and the use of bicycle helmets to reduce early mortality and long-term morbidity in pTBI. Follow up after discharge is essential to optimize outcome on physical, cognitive, behavioural and social functioning.
Availability of data and materials
G. K. is the guarantor of the paper. G. K. has full access to the data which shall be shared upon request.
References
Dewan MC, Mummareddy N, Wellons JC, Bonfield CM (2016) Epidemiology of global pediatric traumatic brain injury: qualitative review. World Neurosurg 91:497-509.e1. https://doi.org/10.1016/j.wneu.2016.03.045
Rivara FP, Koepsell TD, Wang J, et al (2011) Disability 3, 12, and 24 months after traumatic brain injury among children and adolescents. Pediatrics 128(5). https://doi.org/10.1542/peds.2011-0840
Centers for Disease Control and Prevention C. The report to congress on the management of traumatic brain injury in children. Division of Unintentional Injury Prevention. Published online 2018:1–90. https://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=emed18&NEWS=N&AN=617352660. Accessed Sept 2021.
Stanley RM, Bonsu BK, Zhao W, Ehrlich PF, Rogers AJ, Xiang H (2012) US estimates of hospitalized children with severe traumatic brain injury: implications for clinical trials. Pediatrics 129(1). https://doi.org/10.1542/peds.2011-2074
Appavu B, Foldes ST, Adelson PD (2019) Clinical trials for pediatric traumatic brain injury: definition of insanity? J Neurosurg Pediatr 23(6):661–669. https://doi.org/10.3171/2019.2.PEDS18384
Kochanek PM, Tasker RC, Carney N, et al (2019) Guidelines for the Management of Pediatric Severe Traumatic Brain Injury, Third Edition: Update of the Brain Trauma Foundation Guidelines. Vol 20. https://doi.org/10.1097/PCC.0000000000001735
Maas AIR, Menon DK, David Adelson PD et al (2017) Traumatic brain injury: integrated approaches to improve prevention, clinical care, and research. Lancet Neurol 16(12):987–1048. https://doi.org/10.1016/S1474-4422(17)30371-X
Bragge P, Synnot A, Maas AI et al (2016) A state-of-the-science overview of randomized controlled trials evaluating acute management of moderate-to-severe traumatic brain injury. J Neurotrauma 33(16):1461–1478. https://doi.org/10.1089/neu.2015.4233
Rivara FP, Koepsell TD, Wang J et al (2012) Incidence of disability among children 12 months after traumatic brain injury. Am J Public Health 102(11):2074–2079. https://doi.org/10.2105/AJPH.2012.300696
Stocchetti N, Pagan F, Calappi E et al (2004) Inaccurate early assessment of neurological severity in head injury. J Neurotrauma 21(9):1131–1140. https://doi.org/10.1089/neu.2004.21.1131
Fiser DH (1992) Assessing the outcome of pediatric intensive care. J Pediatr 121(1):68–74. https://doi.org/10.1016/S0022-3476(05)82544-2
Fiser DH, Long N, Roberson PK, Hefley G, Zolten K, Brodie-Fowler M (2000) Relationship of pediatric overall performance category and pediatric cerebral performance category scores at pediatric intensive care unit discharge with outcome measures collected at hospital discharge and 1- and 6- month follow-up assessments. Crit Care Med 28(7):2616–2620. https://doi.org/10.1097/00003246-200007000-00072
Pollack MM, Ruttimann UEGPR (1988) Pediatric risk of mortality (PRISM) score. Crit Care Med 16(11):1110–1116. https://doi.org/10.1097/00003246-198811000-00006
Tepas JJ 3rd, Mollitt DL, Talbert JLBM (1987) The pediatric trauma score as a predictor of injury severity in the injured child. J Pediatr Surg 22(1):14–18. https://doi.org/10.1016/s0022-3468(87)80006-4
Teasdale G, Maas A, Lecky F, Manley G, Stocchetti N, Murray G (2014) The Glasgow Coma Scale at 40 years: standing the test of time. Lancet Neurol 13(8):844–854. https://doi.org/10.1016/S1474-4422(14)70120-6
Emami P, Czorlich P, Fritzsche FS et al (2017) Impact of Glasgow Coma Scale score and pupil parameters on mortality rate and outcome in pediatric and adult severe traumatic brain injury: a retrospective, multicenter cohort study. J Neurosurg 126(3):760–767. https://doi.org/10.3171/2016.1.JNS152385
Bennett TD, DeWitt PE, Greene TH et al (2017) Functional outcome after intracranial pressure monitoring for children with severe traumatic brain injury. JAMA Pediatr 171(10):965–971. https://doi.org/10.1001/jamapediatrics.2017.2127
Tude Melo JR, Di RF, Blanot S et al (2010) Mortality in children with severe head trauma: predictive factors and proposal for a new predictive scale. Neurosurgery 67(6):1542–1547. https://doi.org/10.1227/NEU.0b013e3181fa7049
Ducrocq SC, Meyer PG, Orliaguet GA et al (2006) Epidemiology and early predictive factors of mortality and outcome in children with traumatic severe brain injury: experience of a French pediatric trauma center. Pediatr Crit Care Med 7(5):461–467. https://doi.org/10.1097/01.PCC.0000235245.49129.27
Slovis JC, Gupta N, Li NY, Kernie SG, Miles DK (2018) Assessment of recovery following pediatric traumatic brain injury. Pediatr Crit Care Med 19(4):353–360. https://doi.org/10.1097/PCC.0000000000001490
Rosario BL, Horvat CM, Wisniewski SR et al (2018) Presenting characteristics associated with outcome in children with severe traumatic brain injury: a secondary analysis from a randomized, controlled trial of therapeutic hypothermia. Pediatr Crit Care Med 19(10):957–964. https://doi.org/10.1097/PCC.0000000000001676
Hochstadter E, Stewart TC, Alharfi IM, Ranger A, Fraser DD (2014) Subarachnoid hemorrhage prevalence and its association with short-term outcome in pediatric severe traumatic brain injury. Neurocrit Care 21(3):505–513. https://doi.org/10.1007/s12028-014-9986-7
Davis AL, Hochstadter E, Daya T et al (2019) The base deficit, international normalized ratio, and Glasgow Coma Scale (BIG) score, and functional outcome at hospital discharge in children with traumatic brain injury. Pediatr Crit Care Med 20(10):970–979. https://doi.org/10.1097/PCC.0000000000002050
Murphy S, Thomas NJ, Gertz SJ et al (2017) Tripartite stratification of the Glasgow Coma Scale in children with severe traumatic brain injury and mortality: an analysis from a multi-center comparative effectiveness study. J Neurotrauma 34(14):2222–2229. https://doi.org/10.1089/neu.2016.4793
Fortune PM, Shann F (2010) The motor response to stimulation predicts outcome as well as the full Glasgow Coma Scale in children with severe head injury. Pediatr Crit Care Med 11(3):339–342. https://doi.org/10.1097/PCC.0b013e3181c014ab
Stewart TC, Alharfi IMFD (2013) The role of serious concomitant injuries in the treatment and outcome of pediatric severe traumatic brain injury. J Trauma Acute Care Surg 75(5):836–842. https://doi.org/10.1097/TA.0b013e3182a685b0
Olivier J, Creighton P (2017) Bicycle injuries and helmet use: a systematic review and meta-analysis. Int J Epidemiol 46(1):278–292. https://doi.org/10.1093/ije/dyw153
Maas AIR, Menon DK, Manley GT et al (2022) Traumatic brain injury: progress and challenges in prevention, clinical care, and research. Lancet Neurol 21(11):1004–1060. https://doi.org/10.1016/S1474-4422(22)00309-X
Sarnaik A, Ferguson NM, O’Meara AI et al (2018) Age and mortality in pediatric severe traumatic brain injury: results from an international study. Neurocrit Care 28(3):302–313. https://doi.org/10.1007/s12028-017-0480-x
Taylor C, Bell JM, Breiding MJ, Xu L (2017) Morbidity and mortality weekly report traumatic brain injury-related emergency department visits, hospitalizations, and deaths-United States, 2007 and 2013 Surveillance Summaries. Surveillance Summaries 66(9):1–8 (https://www.cdc.gov/mmwr/volumes/66/ss/pdfs/ss6609.pdf)
Shaklai S, Peretz R, Spasser R, Simantov M, Groswasser Z (2014) Long-term functional outcome after moderate-to-severe paediatric traumatic brain injury. Brain Inj 28(7):915–921. https://doi.org/10.3109/02699052.2013.862739
Beers SR, Wisniewski SR, Garcia-Filion P et al (2012) Validity of a pediatric version of the Glasgow Outcome Scale-extended. J Neurotrauma 29(6):1126–1139. https://doi.org/10.1089/neu.2011.2272
McMillan T, Wilson L, Ponsford J, Levin H, Teasdale G, Bond M (2016) The Glasgow Outcome Scale-40 years of application and refinement. Nat Rev Neurol 12(8):477–485. https://doi.org/10.1038/nrneurol.2016.89
Anderson V, Godfrey C, Rosenfeld J V., Catroppa C (2012) Predictors of cognitive function and recovery 10 years after traumatic brain injury in young children. Pediatrics 129(2). https://doi.org/10.1542/peds.2011-0311
Herridge MS, Azoulay É (2023) Outcomes after critical illness. N Engl J Med 388(10):913–924. https://doi.org/10.1056/nejmra2104669
Alharfi IM, Stewart TC, Kelly SH, Morrison GC, Fraser DD (2013) Hypernatremia is associated with increased risk of mortality in pediatric severe traumatic brain injury. J Neurotrauma 30(5):361–366. https://doi.org/10.1089/neu.2012.2410
Friess SH, Kilbaugh TJ, Huh JW (2012) Advanced neuromonitoring and imaging in pediatric traumatic brain injury. Crit Care Res Pract 2012. https://doi.org/10.1155/2012/361310
Tasneem N, Samaniego EA, Pieper C, et al (2017) Brain multimodality monitoring: a new tool in neurocritical care of comatose patients. Crit Care Res Pract 2017. https://doi.org/10.1155/2017/6097265
Oddo M, Levine JM, MacKenzie L et al (2011) Brain hypoxia is associated with short-term outcome after severe traumatic brain injury independently of intracranial hypertension and low cerebral perfusion pressure. Neurosurgery 69(5):1037–1045. https://doi.org/10.1227/NEU.0b013e3182287ca7
Dellazizzo L, Demers SP, Charbonney E et al (2019) Minimal PaO2 threshold after traumatic brain injury and clinical utility of a novel brain oxygenation ratio. J Neurosurg 131(5):1639–1647. https://doi.org/10.3171/2018.5.JNS18651
Acknowledgements
None
Code availability
Data were analysed using SPSS v23.0 (IBM Statistical Package for the Social Sciences for Windows, Armonk, NY: IBM Corp.). The code shall not be shared because of restricted access.
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Author information
Authors and Affiliations
Contributions
Design of the study, GK and MK. Data collection, GK, SD. Analysis: GK, MK. Drafting of the manuscript: GK, MK. Revising it critically for important intellectual content: GK, MK, JB, HM. All the authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Institutional Review Board approved the study and waived the need for informed consent (Institutional Review Board UMCG, METc2021/534).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Supplemental figure 1.
In- and exclusion.
Additional file 2: Supplemental Table 1.
Definition of variables.
Additional file 3: Supplemental Table 2.
Radiological features of first Cranial Computed Tomography scan after trauma.
Additional file 4: Supplemental Table 3.
In hospital measurements on day 0-3.
Additional file 5: Supplemental Table 4.
Repeated measurements on day 0-1 and day 2-3 within Paediatric Cerebral Performance Category Scale ≤ 3 and ≥ 4.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Vlaam, G.Kd., Mulder, H.D., Dijkstra, S.K. et al. Characteristics and outcomes of critically ill children with moderate-to-severe traumatic brain injury. Intensive Care Med. Paediatr. Neonatal 2, 12 (2024). https://doi.org/10.1007/s44253-024-00033-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s44253-024-00033-6