
Abstract
Migrants and refugees are likely to be under-immunised according to the host country's national immunisation schedule and may remain under-immunised post-resettlement for various reasons. In Australia and Aotearoa New Zealand, primary health care professionals including general practitioners and nurses provide the majority of routine and catch-up immunisations for migrants and refugees. However, immunisation service delivery for migrants and refugees is complex, with evidence that unmet training needs for immunisation providers, particularly in the development of catch-up plans, is a significant barrier to immunisation service delivery for this group. Targeted professional development opportunities for immunisation providers are essential to improve their awareness, confidence, and capability to improve immunisation service delivery for migrants and refugees. We developed an educational program to support learning for immunisation providers and equip them with the requisite knowledge and confidence to improve immunisation service delivery for refugees and migrants. The development of the multi-module online educational program drew on evidence-based web design principles, adult learning theories, and its content aimed to complement general immunisation training and align with the continuing professional development standards of Australian and New Zealand general practice and nursing colleges. Input from experts and feedback from a few selected providers in Australia and New Zealand added to the robustness of the program. This program has the potential to improve the understanding and capacity of immunisation providers, to improve vaccination experiences and increase overall vaccine uptake among migrants and refugees.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Background
International migration has been increasing over time, there are currently an estimated 281 million migrants globally in 2020 [1]. The United Nations Department of Economic and Social Affairs (UN DESA) adopts a definition of an international migrant as a person who moves away from their usual country of residence [2], and this may be voluntarily or forced. In 2022, there were approximately 0.35 million refugees and 5 million asylum seekers [3]. Refugees, as defined by the United Nations Convention relating to the Status of Refugees (1951), are “individuals who reside in another country and who are unable to return to their country of origin due to fear of being persecuted on account of race, religion, nationality, political affiliation or because they are a member of a particular social group” [4]. More than half of all refugees originated from just three countries: the Syria, Ukraine and Afghanistan [3].
1.1 Migrants and refugees as priority groups for equity in immunisation
Immunisation is one of the most cost-effective public health interventions, yet some population groups who experience inequities due to social disadvantage are likely to have limited or poor access to immunisation services [5]. Migrants and refugees are a subgroup with disparities in immunisation coverage and generally experience a higher burden of vaccine-preventable-diseases (VPDs) compared to non-migrants worldwide [6]. Since the onset of the COVID-19 pandemic, global immunisation coverage substantially declined and has yet to return to pre-pandemic levels, exacerbating immunisation inequities [7]. As outlined in the World Health Organization’s (WHO) Immunization Agenda 2030, equity of immunisation access and achieving national immunisation targets can only be achieved through implementation of contextualised evidence-based interventions aimed at under-immunised populations [8]. The notion of “leave no one behind” underpins the importance of specific efforts to improve vaccine uptake among migrant and refugee background populations.
In Australia and Aotearoa New Zealand, refugees and migrants have lower reported immunisation rates [9, 10]. Refugees are likely to be underimmunised due to differences in immunisation schedules between their countries of origin and the host countries, and barriers in accessing immunisations in their countries of origin, while in transit, and upon resettlement. Language, cultural, financial, and logistical barriers, lack of familiarity with the host country’s health care system, limited literacy, and health literacy are some barriers that further impede their access to immunisations upon resettlement [11]. Even when they access health services, structural complexities around providing care impede access to immunisation. These include the lack of readily available interpreter services, logistical issues, such as long waiting times, and sociocultural differences occurring during client-provider interactions affecting communication and trust between refugees and service providers [12]. There are still gaps in knowledge about migrant vaccination. Studies conducted in Australia and New Zealand have also indicated inadequate uptake of various adult vaccines among migrant communities [9, 13,14,15]. Language barriers, misinformation, low-risk perception and limited health literacy are key factors contributing to under-immunisation among migrants [15]. Compounding these are provider-specific barriers that impact on immunisation service delivery for both groups [5].
1.2 Immunising migrant and refugee background communities from service providers’ perspectives
In Australia and New Zealand, primary care providers including General Practitioners (GPs) and practice nurses are the main providers of immunisations for migrants and refugees. A good level of understanding around vaccines and their potential benefits has been reported among migrants and refugees and positive recommendations from providers are significant predictors of vaccine uptake [16, 17]. However, immunisation providers may be less likely to recommend immunisation if they lack training around the specific needs of at-risk populations [18].
Immunisation service delivery for migrants and refugees is complex, with evidence that unmet training needs for immunisation providers, particularly in the development of catch-up plans, is a significant barrier to immunisation service delivery for this group. Specifically, gaps in relevant skills and knowledge in implementing complex catch-up immunisation schedules, lack of adequate support and resources to assist with provision of immunisation to migrants and refugees including effective use of reminders, recall systems, and other information management systems have been shown to be major barriers in service delivery for this group [19]. In addition, cultural differences between migrants, refugees, and service providers are a significant barrier resulting in culturally inappropriate services and ultimately impacting on health care utilisation among this group [10]. Consequently, strategies aimed at improving cross-cultural care and health care utilisation for people from culturally and linguistically diverse backgrounds, particularly newly arrived migrants and refugees, emphasise the need for training on cross-cultural awareness and communication skills among service providers to improve service delivery for this group [20]. Insufficient training on immunisation-specific needs for refugees among GPs has been reported to result in missed opportunities for vaccination and in some cases over-immunisation [19]. Such findings demonstrate the need for implementing multi-level (policy, provider, and community) strategies aimed at systematically increasing vaccine uptake for migrant and refugees [9].
At a provider level, while training on immunisation is available for GPs and practice nurses, current training focuses on certifying immunisers, and providing annual updates on changes to the National Immunisation Schedule mainly related to childhood immunisation. To our knowledge, there is currently no widely available education program for immunisation providers that aims at reducing provider-specific barriers in Australia and New Zealand specifically focusing on the immunisation needs for migrants and refugees. To address this need, an online educational program targeting authorised immunisation providers (e.g., GPs, nurses) across Australia and New Zealand was developed. This article presents the development approach as a case study.
2 Case study: ‘Catching up providers on catch-up immunisation’—an intervention to improve immunisation service delivery for migrants and refugees in Australia and New Zealand
Targeted professional development opportunities for immunisation providers are essential to increase their awareness, confidence, and capability to improve immunisation service delivery for migrants and refugees. We developed a multi-module online educational program to support learning for immunisation providers (e.g., GPs, primary care nurses) and equip them with the requisite knowledge and skills for improving immunisation service delivery for refugees and migrants. The development of this educational program was underpinned by several bodies of knowledge to ensure it effectively delivered the training needs required for the target audience, was evidence-based, and was aligned to the Continuous Professional Development (CPD) needs of Australian and New Zealand general practice and nursing colleges.
2.1 Web-design principles and adult learning theories
Casebeer et al. developed a set of twelve key principles for the design of online training for clinicians, based on learning and change theories [21]. These principles are derived from renowned learning and change theories (including Schon’s model [22]) and have been identified to positively influence GPs’ preventive practices such as screening for infectious diseases [23]. Schon’s model highlights the importance of providers’ reflections on their daily practice as a component of their learning process, a key component featured in the training program [22]. We designed our educational program using this framework, as its principles are evidence-based, they conform to key principles for designing CMEs that are more likely to improve physician performance and patient health outcomes as identified by Cervero and Gaines [24]. In addition, CME trainings designed using this framework have been evaluated in clinical practice, providing evidence of improved physicians’ preventive practices [25, 26].
The design of our educational program considered nine of these principles: (i) needs assessment; (ii) multimodal strategies, (iii) tailoring and interactivity, (iv) credible evidence-base content, (v) contextual learning in the form of clinical cases, (vi) audit and feedback, (vii) credibility of the hosting organisation and the website host, (viii) enabling materials, and (ix) ease of use and navigation. Below we describe the application of the learning theories and the evidence-based web design principles in the development of our educational program:
-
i)
Needs assessment
Two needs assessment analyses conducted among key immunisation stakeholders including GPs in Victoria [27], and in New South Wales and the Australian Capital Territory [20] highlighted a need for additional educational support in the form of training on catch-up immunisation for refugees. These findings were similarly echoed in our study that explored provider-specific challenges in immunisation service delivery across all states and territories in Australia [19] and more recently by studies conducted among GP immunisation providers for migrant children in Victoria [28] and immunisation providers for refugee children across New Zealand [29]. Collectively, findings from these studies informed the contents of this educational program.
-
ii)
Multimodal strategies
A single module when compared to a series of multiple modules, is less likely to alter providers’ behaviours and its effects are likely to reduce over time [30]. This online program was therefore designed as a series of modules that are adaptable and flexible to allow providers to learn at their own pace. To further enhance the learning process, each module uses a multimodal approach containing lessons informed by learning theories such as constructivism [31] (problem-based learning and reflective practice) and behaviourism [32] (reinforcement mechanisms at the completion of each module, video clips of experts in the field sharing real-life scenarios in practice for authenticity and fostering an engaging learning experience, and feedback mechanisms). Figure 1 provides an overview of the four modules that reflect the domains and learning outcomes aligned to the competency outcomes of the RACGP, and the Nurses Council of New Zealand.
-
iii)
Tailoring and interactivity
Fig. 1 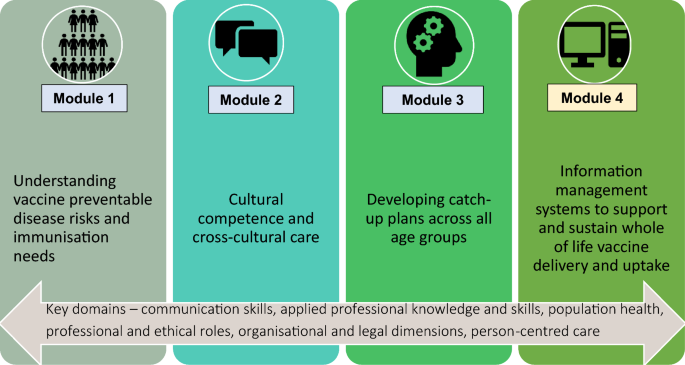
Overview of the ‘Catching up providers with catch-up immunisation’ educational program
Tailoring, which is prominently featured in health communication and behavioural change theories, allows for the content to be individualised and responsive to the specific needs of the learners [33, 34]. The immunisation providers can repeat modules several times until they master the content allowing them to tailor the content to meet their individual learning needs. The post-module questions also allow the learners to self-assess and repeat as required.
Interactive learning stimulates the learner by providing an active learner-centred environment, maintaining the learner's interest which further reinforces individual development [32]. Active learning strategies underpinned by constructivist and social cognitive theories, and adult learning principles were used to tailor the content specific to the learning needs of the target audience (i.e., immunisation providers). Table 1 provides an overview of education techniques, theoretical underpinnings, their relevance, and application in the program development.
Table 1 Overview of practical education techniques, theoretical underpinnings, their relevance and application in the program development Interactive features in this program include reflection activities before and after the commencement of each module, interactive maps and figures, downloadable summary tables and hyperlinked resources including research articles, immunisation guidelines, catch-up immunisation calculators and other relevant websites, drag and drop activities, matching circumstances and outcomes related to migrant and refugee health, and video clips containing tips for supporting immunisation service delivery for migrants and refugees in clinical practice.
-
iv)
Credible evidence-base content
The educational program has been developed based on a range of evidence-based resources. Five authors (AM, IA, NC, HS, AH) have extensive knowledge and a track record in refugee and migrant health research. To ensure the program content is relevant, appropriately pitched, and addresses the education needs of immunisation providers, expert input from two GPs and two nurse immunisers with extensive experience in providing primary health care to refugees and migrants was also sought. Scrutiny by the expert providers ensured the content was relevant to the target audience, met the stated outcomes, and was of the highest possible ethical, clinical, and educational standards.
-
v)
Contextual learning in the form of clinical cases
Three clinical cases were developed, which focused on key issues raised in the literature, and drew on real-life experiences raised by two practicing GPs and an academic with extensive experience in teaching, research, and practice in refugee and migrant health. These cases addressed the following critical considerations for immunisation providers in assessing immunisation needs of migrants and refugees: the need for proactive screening for hepatitis B carriage of newly arrived migrants and refugees (Module 1); the importance of general practices offering culturally sensitive and appropriate services (Module 2); and the nuanced implementation of catch-up immunisation for migrants and refugees (Module 3). These case studies have been designed with open-ended, reflective questions for providers to consider the circumstances in their own practices and considerations for the application of what they learn to their own practice. Upon completion, feedback about the best practice approaches for such cases and an explanation of what an expert would do under such circumstances accompanies the case studies for the providers to reflect on. Figure 2 is a snapshot of one of the case studies included in the program.
-
vi)
Audit and feedback
Fig. 2 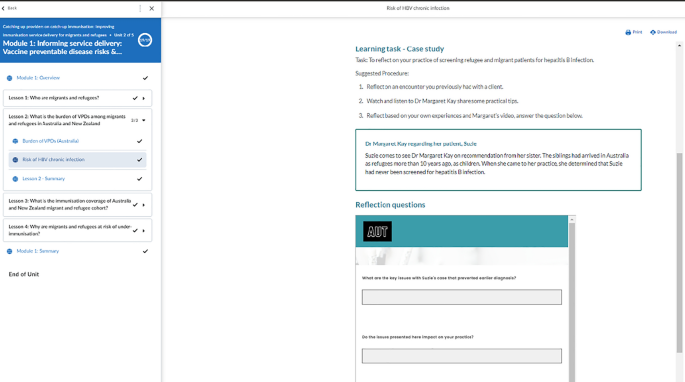
A snapshot of a case study on screening for hepatitis B carriage in general practice
Feedback given to providers, coupled with their ability to compare their performance against internal or external sources, has been shown to improve clinical care and facilitate changes in clinical practice [30, 35, 36]. Each module contains knowledge questions, case studies and reflection activities with immediate feedback through pop-up icons, additional slides, or video clips, enabling providers to benchmark their responses against good practice provided by experts. All the activities are evidence-based and were reviewed by expert immunisation providers with the aim of improving the quality of immunisation services offered to refugees and migrants.
-
vii)
Credibility of the hosting organisation and the website host
The education program is developed and offered via in-house learning management system provided by The Immunisation Advisory Centre (IMAC) in New Zealand. IMAC has been training New Zealand’s vaccinators for more than fifteen years, providing information and training for health professionals, national immunisation coordination and policy advice and research into many aspects of vaccines and vaccine-preventable diseases. IMAC also has a portal for immunisation education familiar to NZ immunisers.
-
viii)
Enabling materials
As learning is a continuous process, enabling materials (educational resources) are crucial in supporting the translation of skills and knowledge gained into everyday practice [21]. Useful resources for equipping and supporting providers with immunisation service delivery for refugees and migrants, such as comprehensive screening guidelines, translation and interpreter resources, catch-up calculators and planning tools, and tables containing evidence-based literature have been made available as links and attached PDF documents within each module for easy access when required.
-
ix)
Ease of use and navigation
While e-learning is advantageous in providing a unique opportunity for self-directed learning, evidence shows that technological issues such as low competence in using computer-based technologies among GPs may severely hamper its use [37]. As such, this program has been designed using a learning management system that is easy for adult learners and has been previously used to deploy online educational programs for nurses [38]. This learning platform is flexible and adaptable, providing an interface whereby learners can easily navigate the program, sign out and continue where they left off upon signing back in, restart a lesson and re-visit the module content multiple times. Table 2 provides an overview of the four modules that reflect the domains and learning outcomes aligned to the competency outcomes of these professional bodies.
Table 2 Overview of the module contents and curriculum mapping based on the RAGGP and Nurses Council on New Zealand domains and key competencies


2.2 Online active learning approach
Considering the need for widely accessible educational resources for immunisation providers, in both Australia and New Zealand, including those practicing in rural and remote locations, this program was designed as an online active learning module. Online CME (e-learning), which entails the delivery of structured, scheduled educational sessions via the internet, increased exponentially in 2020 due to the COVID-19 pandemic. Compared to the traditional CME approaches, such as face-to-face refresher courses that tend to be didactic and passive, e-learning has multiple advantages including greater flexibility and allowing healthcare providers to learn at their own pace, which is important considering the busy nature of their work [37].
The benefits of e-learning such as increased accessibility, flexibility, and adaptivity render this modality invaluable, particularly in our case where we target health professionals across two countries. Due to low screening and immunisation rates among refugee clients attending a primary care clinic in the USA, Waldorf et al. [39] reiterate the usefulness of e-learning educational programs for primary care providers to potentially improve health outcomes in this population through improved utilisation of guidelines [38]. In the context of the COVID-19 pandemic, delivering online, interactive, multimedia-based training is of utmost importance to facilitate continuous professional development. Implications for developing migrant- and refugee-specific immunisation resources and training for immunisation providers.
This evidence-based education program aims to support learning for immunisation providers and equip them with the requisite knowledge and confidence to improve immunisation service delivery for refugees and migrants, which may improve immunisation coverage rates and experiences for those with migrants and refugee backgrounds. To increase the potential of effectuating changes in clinical practice, the framework by Casebeer et al. [21] that applies evidence-based behaviour and learning theories in online education has been used in the design of the program. The program is also aligned to current vaccine recommendations and the continuing professional development needs of General Practitioners and registered nurses in Australia and New Zealand.
Our training program takes a holistic approach by filling in training gaps on migrant and refugee immunisation for providers in Australia and New Zealand. Module one provides background information on the demographics, the epidemiology of vaccine preventable diseases and immunisation needs of refugees and migrants. This module informs immunisation providers of the factors associated with low immunisation coverage for this group and outlines evidence-based strategies to reduce the risks of under-immunisation.
Module two focuses on the elements of cultural competence and cross-cultural communication with the aim of supporting the delivery of culturally competent services in primary care. There is a plethora of literature in Australia, New Zealand and overseas highlighting sociocultural differences occurring during client-provider interactions to severely hamper on health care utilisation for this group. This module fills this gap by equipping immunisation providers with practical tools and best practice approaches to facilitate cross-cultural communication and support the delivery of culturally appropriate immunisation services.
Module three provides practical issues to consider when assessing immunisation needs for refugees and migrants, and equips immunisation providers with an understanding of relevant procedures and approaches for planning and implementation of catch-up immunisation for migrants and refugees across all age groups. This module addresses a crucial training gap that is yet to be filled. As an interactive, practical module, this module includes evidence-based best practice approaches in immunisation service delivery for refugees and migrants across the continuum of care, that is, history taking, examination, investigations (serological tests for hepatitis B) and management (catch-up planning, implementation, and recording of vaccines on immunisation registers/vaccine records). Using clinical case studies in developing clinical proficiencies has been shown to improve physicians’ knowledge, confidence, and decision-making skills in clinical practice [26]. This module integrates clinical case studies on implementation of catch-up immunisation for refugees and migrants hence addressing the gaps among providers on contextualisation of catch-up immunisation for overseas-born individuals [28, 29]. This module also equips providers with relevant resources including online catch-up calculators and catch-up guides to assist in developing catch-up schedules, which is critical in ensuring migrants and refugees across all age groups receive their catch-up immunisations as required.
Module four provides an overview of the use of information management systems in general practice. This module is aligned with domains in general practice and nursing that encompass organisational skills such as effective use of information technology, records, reporting, and practice management. This module focuses on the use of information management systems including the recall and reminder systems, the immunisation register, and reporting of adverse events following immunisation to enhance patient safety. Standardised and consistent data collection on immunisation allows for efficient monitoring of vaccine uptake and identification of potential predictors of uptake which can be useful in developing targeted approaches aimed at improving vaccine uptake among this group [40]. Implementation of recall and reminder systems in clinical practice is essential for ensuring continuity of care and may result in better clinical outcomes [41]. Reminder systems, when used appropriately, have been proven to be effective in improving uptake of preventive services including immunisation [42].
3 Next steps
Before launching in early 2024, this program will be pilot tested with GPs and nurse immunisers in November 2023 and revised accordingly. The educational program will be pilot tested and evaluated using a convergent parallel mixed method design involving the collection of both quantitative and qualitative data. Quantitative data will be collected online as participants complete the course. The online program contains predisposing and reinforcing activities and embedded activities within the program to enrich the learning space. These activities include a reflection on their baseline knowledge on implementing catch-up plans (predisposing); practice assessing immunisation needs for refugees and migrants including history taking, investigating, and planning a catch-up schedule for all age groups; and upgrading their skills on understanding vaccine eligibility criteria (embedded). Participant responses on predisposing and reinforcing activities will be captured on the IMAC platform, which will then be downloaded and saved by the researchers. In addition, a survey to compare baseline knowledge and confidence pre- versus post-program will in included. In this study, for the pilot and evaluation, the education program will be developed and offered via IMAC and survey data will be collected through links to Qualtrics survey management software. To reach the target sample size (n = 80–100) across Australia and New Zealand, we anticipate that data will be collected over 3 months after implementation. Analysing the survey responses to the predisposing and reinforcing activities will allow us to assess the impact of the intervention on levels of knowledge and confidence towards providing immunisation services to migrants and refugees among research participants. The before-and-after design is most useful when demonstrating the immediate impacts of short-term programs, such as a short educational intervention [43].
At the end of the online education program, participants will be invited to provide their email address if they are interested in participating in the qualitative interviews. In-depth interviews will be undertaken online via video teleconference, or face-to-face with 15–20 participants across Australia and New Zealand who have completed the program. The purpose of these interviews is to explore the receptiveness of the online program focusing on the attitudes, experiences, and acceptability of the participants towards the new educational program so that feedback can be used to make improvements. The Auckland University of Technology Ethics Committee has provided ethical approval for both quantitative and qualitative research (22/118).
Beyond this, consideration needs to be given regarding the content of the modules and ensuring that they remain consistent with current vaccine recommendations and the published peer-review literature. As with any training program in immunisation, there will be a need for constant review of the content to ensure that it aligns with government policies and immunisation provider guidelines across the two countries.
4 Conclusions
We have outlined the development of an online educational program for immunisation providers across Australia and New Zealand focused on delivering immunisations to migrants and refugees which will fill an important gap in immunisation provider training. This program is aligned with the CPD needs for immunisation providers in both countries, based on relevant theories and models pertaining to web-based design principles and adult learning, and fills a known gap in immunisation in our countries. The program has the potential to improve immunisation providers’ understanding of refugee and migrant immunisation needs, with the ultimate aim of increasing overall vaccine uptake amongst these communities. Future research examining its impact on improving immunisation practices for migrants and refugees will be undertaken following its implementation.
4.1 Lessons for practice
-
Immunisation service delivery for migrants and refugees is complex necessitating the need for contextualised training among providers.
-
Targeted professional development opportunities for immunisation providers are essential to improve their awareness, confidence, and capability to improve immunisation service delivery for migrants and refugees.
-
An evidence based-designed online educational program aligned with the CPD needs of general practitioners and nurses may help address training gaps on migrant and refugee-specific immunisation needs.
Data availability
Not applicable.
Abbreviations
- CME:
-
Continuous Medical Education
- CPD:
-
Continuous Professional Development
- GP:
-
General Practitioner
References
International Organisation for Migration (IOM). World migration report 2022. Grand-Saconnex: IOM; 2021. https://worldmigrationreport.iom.int/. Accessed 15 Oct 2022.
Department of Economic and Social Affairs (DESA). Recommendations on statistics of international migration [Internet]. New York: DESA; 1998. https://unstats.un.org/unsd/publication/seriesm/seriesm_58rev1e.pdf. Accessed 21 Nov 2022.
United Nations High Commissioner for Refugees (UNHCR). Figures at a glance. Geneva: UNHCR; 2023. https://www.unhcr.org/figures-at-a-glance.html. Accessed 9 Sep 2023.
United Nations High Commissioner for Refugees (UNHCR). Convention Relating to the Status of Refugees, 1951, and Protocol Relating to the Status of Refugees, 1967 [Internet]. Geneva: UNHCR; 2010. www.unhcr.org/protect/PROTECTION/3b66c2aa10.pdf. Accessed 28 July 2022.
Heywood AE, López-Vélez R. Reducing infectious disease inequities among migrants. J Travel Med. 2019;26(2): tay131.
Charania NA, Gaze N, Kung JY, Brooks S. Vaccine-preventable diseases and immunisation coverage among migrants and non-migrants worldwide: a scoping review of published literature, 2006 to 2016. Vaccine. 2019;37(20):2661–9.
World Health Organization (WHO). Immunization coverage. Geneva: WHO; 2022. https://www.who.int/news-room/fact-sheets/detail/immunization-coverage. Accessed 25 Oct 2022.
World Health Organisation (WHO). Immunization agenda 2030: A global strategy to leave no one behind. Geneva: WHO; 2020. https://www.who.int/teams/immunization-vaccines-and-biologicals/strategies/ia2030. Accessed 25 Oct 2022.
Charania NA, Paynter J, Lee AC, Watson DG, Turner NM. Exploring immunisation inequities among migrant and refugee children in New Zealand. Hum Vaccin Immunother. 2018;14(12):3026–33.
Chaves NJ, Paxton GA, Biggs BA, Thambiran A, Gardiner J, Williams J, Smith MM, Davis JS. The Australasian Society for Infectious Diseases and Refugee Health Network of Australia recommendations for health assessment for people from refugee-like backgrounds: an abridged outline. Med J Aust. 2017;206(7):310–5.
Kpozehouen E, Heywood AE, Kay M, Smith M, Paudel P, Sheikh M, MacIntyre CR. Improving access to immunisation for migrants and refugees: recommendations from a stakeholder workshop. Aust N Z J Public Health. 2017;41(2):118.
Correa-Velez I, Barnett AG, Gifford SM, Sackey D. Health status and use of health services among recently arrived men with refugee backgrounds: a comparative analysis of urban and regional settlement in South-east Queensland. Aust J Prim Health. 2011;17(1):66–71.
Kong KL, Chu S, Giles ML. Factors influencing the uptake of influenza vaccine vary among different groups in the hard-to-reach population. Aust N Z J Public Health. 2020;44(2):163–8.
Karki S, Dyda A, Newall A, Heywood A, MacIntyre CR, McIntyre P, Banks E, Liu B. Comparison of influenza vaccination coverage between immigrant and Australian-born adults. Vaccine. 2016;34(50):6388–95.
Abdi I, Menzies R, Seale H. Barriers and facilitators of immunisation in refugees and migrants in Australia: an east-African case study. Vaccine. 2019;37(44):6724–9.
Krishnaswamy S, Cheng AC, Wallace EM, Buttery J, Giles ML. Understanding the barriers to uptake of antenatal vaccination by women from culturally and linguistically diverse backgrounds: a cross-sectional study. Hum Vaccin Immunother. 2018;14(7):1591–8.
Tung IL, Machalek DA, Garland SM. Attitudes, knowledge and factors associated with human papillomavirus (HPV) vaccine uptake in adolescent girls and young women in Victoria, Australia. PLoS ONE. 2016;11(8): e0161846.
Paxton GA, Spink PC, Danchin MH, Tyrrell L, Taylor CL, Casey S, Graham HR. Catching up with catch-up: a policy analysis of immunisation for refugees and asylum seekers in Victoria. Aust J Prim Health. 2019;24(6):480–90.
Mahimbo A, Seale H, Smith M, Heywood A. Challenges in immunisation service delivery for refugees in Australia: a health system perspective. Vaccine. 2017;35(38):5148–55.
Duncan G, Harding C, Gilmour A, Seal A. GP and registrar involvement in refugee health: a needs assessment. Aust Fam Physician. 2013;42(6):405.
Casebeer LL, Strasser SM, Spettell CM, Wall TC, Weissman N, Ray MN, et al. Designing tailored Web-based instruction to improve practicing physicians’ preventive practices. J Med Internet Res. 2003;5(3): e20.
Schon DA. The reflective practitioner. How professionals think in action. 1983. Schon DA, DeSanctis V. The reflective practitioner: How professionals think in action. J Contin High Educ. 1986;34(3):29.
Allison JJ, Kiefe IC, Wall T, Casebeer L, Ray NM, Spettell MC, et al. Multicomponent Internet continuing medical education to promote chlamydia screening. Am J Prev Med. 2005;28(3):285–90.
Cervero RM, Gaines JK. The impact of CME on physician performance and patient health outcomes: an updated synthesis of systematic reviews. J Contin Educ Health Prof. 2015;35(2):131–8.
Bonevski B, Magin P, Horton G, Bryant J, Randell M, Kimlin GM. An internet based approach to improve general practitioners’ knowledge and practices: The development and pilot testing of the “ABC’s of vitamin D” program. Int J Med Inform. 2015;84(6):413–22.
Harris JM, Salasche SJ, Harris RB. Can internet-based continuing medical education improve physicians’ skin cancer knowledge and skills? J Gen Intern Med. 2001;16(1):50–6.
Paxton G, Spink P, Casey S, Graham H. A needs analysis of catch-up immunisation in refugee-background and asylum seeker communities in Victoria. Melbourne: Victorian Refugee Health Network; 2014.
Overmars I, Kaufman J, Holland P, Danchin M, Tuckerman J. Catch-up immunisation for migrant children in Melbourne: a qualitative study with providers to determine key challenges. Vaccine. 2022;40(47):6776–84.
Cavit L, Charania NA. Exploring factors that influence vaccination uptake for children with refugee backgrounds: An interpretive description study of primary healthcare providers' perspectives. Vaccine. 2023. https://doi.org/10.1016/j.vaccine.2023.09.055
Davis DA, Thomson MA, Oxman AD, Haynes RB. Changing physician performance: a systematic review of the effect of continuing medical education strategies. JAMA. 1995;274(9):700–5.
Biggs J. Enhancing teaching through constructive alignment. Higher Ed. 1996;32(3):347–64.
Spence KW. Behavior theory and learning: Selected papers. 1960.
Kreuter MW, Farrell DW, Olevitch LR, Brennan LK. Tailoring health messages: customizing communication with computer technology. Milton Park: Routledge; 2013.
Oxman AD, Thomson MA, Davis DA, Haynes RB. No magic bullets: a systematic review of 102 trials of interventions to improve professional practice. CMAJ. 1995;153(10):1423.
Goebel LJ. A peer review feedback method of promoting compliance with preventive care guidelines in a resident ambulatory care clinic. Jt Comm J Qual Improv. 1997;23(4):196–202.
Hayes R, Ballard D. Feedback about practice patterns for measurable improvements in quality of care–a challenge for PROs under the Health Care Quality Improvement Program. Clin Perform Qual Health Care. 1995;3(1):15–22.
Sandars J, Walsh K. E-learning for general practitioners: lessons from the recent literature Work Based Learning in Primary Care. Milton Park: Taylor and Francis Ltd; 2004. p. 305–14.
Immunisation Advisory Centre. Welcome to our e-learning centre. 2023. https://www.immune.org.nz/education/e-learning. Accessed 9 Sep 2023.
Waldorf B, Gill C, Crosby SS. Assessing adherence to accepted national guidelines for immigrant and refugee screening and vaccines in an urban primary care practice: a retrospective chart review. J Immigr Minor Health. 2014;16(5):839–45.
Moller SP, Hjern A, Andersen A-MN, Norredam M. Differences in uptake of immunisations and health examinations among refugee children compared to Danish-born children: a cohort study. Eur J Paediatr. 2016;175(4):539–49.
Free C, Phillips G, Watson L, Galli L, Felix L, Edwards P, et al. The effectiveness of mobile-health technologies to improve health care service delivery processes: a systematic review and meta-analysis. PLoS Med. 2013;10(1): e1001363.
Grol R, Grimshaw J. From best evidence to best practice: effective implementation of change in patients’ care. Lancet. 2003;362(9391):1225–30.
Thiese MS. Observational and interventional study design types; an overview. Biochemia medica. 2014;24(2):199–210.
Acknowledgements
We would like to acknowledge the contribution of Dr. Margaret Kay and Professor Nick Zwar in the development of the program resources including case studies and video clips, and the review of the whole program. We would also like to acknowledge Dr. Shamila Ginige, Dr. Sarah McGuinness, Diane McIrvine, and Trish Wells Morris for their constructive feedback and input on the modules of the educational program.
Funding
This work was supported by an Independent Medical Education program grant from GSK and a grant from the Health Research Council of New Zealand (18/586).
Author information
Authors and Affiliations
Contributions
AM was responsible for the design, drafting, and editing of the manuscript. PT was responsible for the drafting and editing of the manuscript. IA was responsible for drafting and editing of the manuscript. HS was responsible for the reviewing and editing the manuscript. NC was responsible for reviewing and editing the manuscript and contributing to the design of the manuscript. AEH was responsible for reviewing and editing the manuscript and contributing to the design of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
A/Prof Anita Elizabeth Heywood has received honoraria from MSD (2022) and Pfizer (2021) unrelated to this manuscript. A/Prof Holly Seale has received funding from drug companies for investigator-driven research and consulting fees to present at conferences/workshops and develop resources (bio-CSL/Sequiris, GSK and Sanofi Pasteur). Dr Abela Mahimbo, Dr Preeti Tiwari, Dr Ikram Abdi, and Dr Nadia Charania have no conflicts to declare.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Mahimbo, A., Tiwari, P., Abdi, I. et al. Designing an online educational program to improve immunisation service delivery for migrants and refugees in Australia and New Zealand. Discov Health Systems 2, 28 (2023). https://doi.org/10.1007/s44250-023-00043-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s44250-023-00043-9