
Abstract
Cancer is a leading cause of death, and its incidence is increasing, as reported in recent studies by GLOBOCAN. Cancer registry programs provide insights into currently trending tumors worldwide and aid in determining possible risk factors. This study was based on 7 years of cancer registry data recorded at NIMRA cancer hospital, Sindh, from 2015 to 2021. A total of 16,191 cancer patients were registered. In men, head and neck, lung, liver, colorectal and urinary tract cancers were most common. In women, breast cancer, head and neck cancer, gynecological tumors, esophageal cancer and colorectal cancer predominated. The overall data analysis indicated trending cancers in both sexes, including head and neck cancer (37.76%), breast cancer (13.83%), gynecological tumors (10.22%), esophageal cancer (5.18%), lung cancer (4.79%), colorectal cancer (4.27%), liver cancer (3.87%), lymphoma (3.16%), urinary tract cancer (3.11) and prostate cancer (1.53%). The mean age was 50.41 ± 11.78 years in men and 48.47 ± 11.88 years in women. Cancer prevalence has markedly increased worldwide, and is particularly alarming in developing countries. Various risk factors are involved in this increase, including the use of tobacco, areca nut, chewable tobacco, snuff or niswar. Current disease trends are substantially different from those in older studies at the institute.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
Cancer is a leading cause of mortality worldwide among people of all ages [1]. Globally, large expenditures are allocated to fighting against this disease. According to published research, in 2000, 6 million deaths occurred, and 22 million people were living with this deadly disease. That study predicted that, on the basis of the rates at the time, 15 million new cases and approximately 10 million deaths would occur in 2020 [2]. In fact, approximately 19.3 million new cancer cases were registered, and approximately 10 million deaths were reported worldwide in 2020. According to global cancer incidence (GLOBOCAN), the global burden of cancer is expected to be 28.4 million by 2040, a number 47% higher than that in 2020 [3].
The rapid increases in cancer incidence rates have become a serious public health issue in Pakistan and a focus of continuing governmental efforts. Cancer is a multigenic and multicellular disease that can arise from all cell types [4]. In developing countries, chronic infections are responsible for causing more than 22% of cancers, and the use of betel nuts and tobacco remains the most important risk factor [5]. For future policymaking regarding cancer prevalence, cancer registries have been found to be a valuable source of information on associated cancer risk factors in genetic, epigenetic and epidemiological studies. Cancer demographic data captured in registries change over time, under the influence of cancer screening programs; the availability of cancer treatment and diagnostic facilities; and variations in genetic, epigenetic and environmental risk factors. Epidemiological studies improve understanding of changing trends in cancer risk factors, thus aiding in interpretation and forecasting of future cancer incidence [6,7,8,9]. Cancer is a non-communicable deadly disease that has recently been found to be the leading cause of death [10, 11]. Asian developing countries must take immediate steps to prevent and detect cancer.
2 Materials and Methods
2.1 Inclusion of Data
The NIMRA cancer hospital is one of the oldest cancer hospital facilities built by the Pakistan Atomic Energy Commission (PAEC); it is located in the South Sindh province of Pakistan. Its scope includes diagnosis, nuclear medicine, and treatment of malignant cancers with chemotherapy and radiotherapy. NIMRA cancer hospital is capable of performing research studies to examine current cancer trends and forecast future trends. The center is equipped with a well-established cancer registry software hospital management information system (HMIS) for data analysis. Data were registered from January 1, 2015 to December 31, 2021, and included a total of 161,191 patients with biopsies treated at NIMRA cancer hospital. Each patient was registered with an automatically generated unique ID in HMIS software. Data were categorized by year, sex and type of cancer for 7 years. The data were divided into tabulated and graphical distributions for analysis.
2.2 Exclusion of Data
Miscellaneous diseases included pathologies present in low proportions and undefined primary cases, including melanoma, mesothelial, skin or soft tissue cases. Miscellaneous cases were excluded from the top ten trending cancer analyses.
3 Results
Cancer registry statistics of the reported cases for a period of 7 years (2015–2021) and the percentage incidence in both sexes are shown in Table 1. Almost on average cancer incidence reported ratio is about 50% between both sexes annually.
The graphical distribution of the reported cancer cases by year is shown in Fig. 1. The total number of registered cancer patients by year in Fig. 1 indicated the trends in reported cases over the past 4 years (2018–2021). The results indicated increased numbers of cancer patients per annum with respect to past data, except for the reported cancer cases in the year 2020 (because of the COVID-19 pandemic).

Graphical distribution of annually reported cases in both sexes
Reported cancer cases from 2015 to 2021 are categorized according to disease in Table 2. Cases in men and women were normalized to the most prevalent disease, which was predominantly head and neck cancer, in all annual data.
The normalized proportion graphs of incident disease are shown in Figs. 2, 3, 4, 5, 6, 7 and 8. Head and neck, breast and gynecological cancers had the most reported cases every year. Figure 2 shows that the top trending registered cancers in 2015 were head and neck cancer, breast cancer, gynecological tumors, lung cancer, colorectal cancer, liver cancer, urinary tract cancer, lymphoma, esophageal cancer and testicular tumors. Figure 3 shows that the top trending registered cancers in 2016 were head and neck cancer, breast cancer, gynecological tumors, lung cancer, liver cancer, esophageal cancer, colorectal cancer, lymphoma, urinary tract cancer and bone cancer. Figure 4 shows that the top trending registered cancers in 2017 were head and neck cancer, breast cancer, gynecological tumors, lung cancer, esophageal cancer, liver cancer, colorectal cancer, urinary tract cancer, lymphoma and bone cancer. Figure 5 shows that the top trending registered cancers in 2018 were head and neck cancer, breast cancer, gynecological tumors, esophageal cancer, lung cancer, liver cancer, colorectal cancer, lymphoma, urinary tract cancer and brain cancer. Figure 6 shows that the top trending registered cases in 2019 were head and neck cancer, breast cancer, gynecological tumors, esophageal cancer, lung cancer, colorectal cancer, lymphoma, liver cancer, urinary tract cancer and prostate cancer. Figure 7 shows that the top trending registered cases in 2020 were head and neck cancer, breast cancer, gynecological tumors, esophageal cancer, colorectal cancer, lung cancer, liver cancer, lymphoma, urinary tract cancer and testicular tumors. Figure 8 shows that the top trending registered cases in 2021 were head and neck cancer, breast cancer, gynecological tumors, esophageal cancer, colorectal cancer, liver cancer, urinary tract cancer, lung cancer, lymphoma and stomach cancer.

Graphical distribution of trending cancers registered in 2015

Graphical distribution of trending cancers registered in 2016

Graphical distribution of trending cancers registered in 2017

Graphical distribution of trending cancers registered in 2018

Graphical distribution of trending cancers registered in 2019

Graphical distribution of trending cancers registered in 2020

Graphical distribution of trending cancers registered in 2021
Among 16,191 registered cancer cases, 8107 were in men, and 8084 were in women. Table 3 depicts the overall distribution of 16,191 reported cases over the 7 years by sex. The aggregated cases in both sexes included 6113 (37.76%) head and neck cancer cases, 2239 (13.83%) breast cancer cases, 1654 (10.22%) gynecological tumor cases, 838 (5.18%) esophageal cancer cases, 776 (4.79%) lung cancer cases, 692 (4.27%) colorectal cancer cases, 626 (3.83%) liver cancer cases, 511 (3.16%) lymphoma cases, 503 (3.11%) urinary tract cancer cases, 248 (1.53%) prostate cancer cases, 232 (1.43%) bone cancer cases, 221 (1.36%) testicular tumor cases, 217 (1.34%) brain cancer cases, 191 (1.18%) stomach cancer cases, 106 (0.65%) gallbladder cancer cases, 85 (0.52%) leukemias, and 72 (0.44%) pancreatic cancer cases.
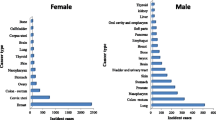
In men, the top trending cancers included head and neck cancer, lung cancer, liver cancer, colorectal cancer, urinary tract cancer, lymphoma, esophageal cancer, prostate cancer, testicular tumors and bone cancer, as shown in Fig. 9.

Top ten trending cancers in men
In women, the top trending cancers included breast cancer, head and neck cancer, gynecological tumors, esophageal cancer, colorectal cancer, lymphoma, lung cancer, urinary tract cancer, liver cancer and bone tumors, as shown in Fig. 10.

Top ten trending cancers in women
An overall analysis of the data indicated that the top trending cancers in men and women included head and neck cancer, breast cancer, gynecological tumors, esophageal cancer, lung cancer, colorectal cancer, liver cancer, lymphoma, urinary tract cancer and prostate cancer, as shown in Fig. 11.

Top ten trending cancers in both sexes
4 Discussion
The World Bank categorizes Pakistan as a low-middle-income country. Head and neck cancers are among the top ten cancers globally and are the top trending cancer reported in Pakistan. No national cancer registry data were available for comparison, and this was an institution-based study. Trending cancer data from our center indicated that the cancer incidence in both sexes was approximately 50%, and the predominant reported disease was head and neck cancer. Among 16,191 reported cases, the overall burden of head and neck cancers was 37.38%: 24.52% in men and 13.24% in women. The main factors contributing to these trends were the use of tobacco, areca nut, chewable tobacco, snuff, niswar, etc. [12,13,14,15]. Areca nut is used in numerous scented forms, and betel quid (including betel leaf, areca nut, sweeteners, condiments, slaked lime, and tobacco) is used in most areas of Pakistan and is the major source of carcinogenesis for head and neck cancers [16]. Various cancers are included in the head and neck region, whereas oral cancers are the most common squamous cell carcinomas. In developing countries, compared with the Western world, squamous cell carcinomas differ in disease sites, molecular biology and risk factors. In developing countries, owing to financial limitations, poverty, illiteracy and access to appropriate health care centers are the major barriers to diagnosis and treatment; consequently advanced stage presentation of the disease occurs in most cases [17,18,19].
Breast cancer is diagnosed in Pakistan a decade earlier than in Western countries [20]. From the overall data analysis, breast cancer is the second most common cancer overall and is the first most common cancer in women in Pakistan [21]. In this study, the breast cancer incidence was 13.62% in women. Breast cancer is heterogeneous in nature, and its subtypes include luminal A, luminal B, HER2 and basal-like triple-negative [22]. Reproductive factors and weight gain are associated with luminal A and luminal B [23].
Menarche at an early age, menopause at a late age, and full-term pregnancy at a late age are associated with a modest range of risk of breast cancer development. Enhanced use of estrogen and progestogen has been linked with early menarche, late menopause, and a shortened menstrual cycle. In addition, the use of oral contraceptives aggravates the risk factors of breast cancer [24]. The breast cancer prevalence is 2.5 times higher in Pakistan than in its neighboring countries. Much research remains necessary to establish cultural, socioeconomic, religious, psychosocial and psychological factors [25].
Gynecological malignancies were the third most common disease in the overall reported data analysis, at 10.22%. Numerous risk factors are associated with these malignancies, e.g., financial instability, compromised life (living in slums, early age menarche, treatment of infertility, use of oral contraceptives, etc. Financial limitations, and a lack of education and health awareness often cause patients to visit spiritual healers rather than physicians [26].
Esophageal cancer is an aggressive lethal disease with a high mortality rate. Worldwide, approximately 90% of biopsied cancers are classified as squamous cell cancer and adenocarcinoma [27]. Epidemiology studies can help understand the history and risk factors, thus aiding in early diagnosis and treatment of esophageal cancers [28]. In our study, the incidence of esophageal cancers was low, at 1.96%, in men but was 3.22% in women. The overall esophageal cancer burden recorded in this study was 5.18%. Esophageal malignancies have alarmingly increased in women with respect to previously reported values. Esophageal cancer shows geographic variation internationally, and high and increasing rates have been observed in some areas of Asia. Environmental factors, dietary habits (nutritional factors) and the use of tobacco are the major factors associated with the development of esophageal cancer, whereas rich diets in vegetables and fresh fruits can decrease the risk [29, 30].
Lung cancer is a common malignant neoplasm worldwide in both sexes. The overall burden of lung cancer in this study was 4.79%: 3.81% in men and 0.98% in women. The main etiological risk factor for lung malignancies is the use of tobacco. Other factors associated with lung cancers are genetic susceptibility, inappropriate diet, air pollution and occupational radiation exposure. Lung cancer is a highly preventable malignancy and remains the most common and deadly disease globally. Comprehensive research addressing all possible risk factors in the development of lung diseases must be performed to support future prevention and management efforts [31, 32].
In the Western world, colorectal malignancies are the fourth most common cancer. The trends in reported colorectal cancers in this study indicated that the overall burden of the disease was 4.27%: 2.61% in men and 1.66% in women. Possible risk factors associated with colorectal cancers include lifestyle; habits; age; chronic disease history; and mutations targeting oncogenes, genes associated with DNA repair mechanisms and tumor suppressor genes [33,34,35].
Liver malignancies, e.g., hepatocellular carcinoma (HCC), are the second leading cause of death globally. In Pakistan, HCC in men markedly increased in the past two decades and might become the most common malignancy in the future. The overall burden of liver malignancy was found to be 3.87%: 3.08% in men and 0.78% in women. Possible risk factors for lung malignancies are hepatitis-B and hepatitis-C, whereas in some regions in developing countries, the disease burden due to hepatitis-B has decreased because of vaccination. A substantial number of the cases reported in tertiary care hospitals treating hepatocellular diseases are hepatitis-C positive, and hepatitis-C is a well-established risk factor for liver carcinogenesis. A lack of awareness of liver diseases among the general public has substantially increased the incidence rate in Pakistan with respect worldwide incidence. The cancer registry database and screening framework allowed us to determine possible risk factors, and support prevention and education efforts for hepatitis and HCC. Owing to the lack of availability of health education and dedicated facilities, patients with liver diseases usually present in advanced stages and have no definitive treatment options [36, 37].
The overall burden of lymphomas was 3.16% in both sexes. Certain autoimmune and chronic inflammatory conditions, such as the immune system disorder Sjogren's syndrome and rheumatoid arthritis, have consistently been associated with an enhanced risk of malignant lymphomas [38]. In regions with endemic parasites, cancer is also associated with parasitic infection.
Urinary tract infections include the urinary system, bladder, urethra, ureters and kidneys [39]. The reported cases of urinary tract malignancies were 3.11% in both sexes: 2.20% in men and 0.91% in women. Urinary tract cancers range from small benign lesions to malignant neoplasms. Bladder malignancy is found predominantly in urinary tract cancers. Delayed diagnosis is associated with poor prognosis in the treatment of urinary tract malignancies. Early detection and follow-up pose major challenges in the management of the disease [40].
Prostate cancers have continually increased in recent years. Our overall data analysis indicated a 1.53% burden of prostate cancer. The causes of prostate cancers are more poorly understood than those of other tumors. Researchers continue to identify risk factors for prostate cancers. The known risk factors include familial and genetic factors. Understanding predictors will enable better control and prevention of the disease [41].
The top ten trending cancers accounted for 87.70% of the 16,191 total reported cases, whereas low proportion disease and miscellaneous tumors accounted for 12.30%.
5 Conclusion
Cancer is a leading cause of death globally, and its rate of incidence is increasing. Cancer trends differ between developing countries and the Western world. In this study, a substantial number of reported cases were head and neck (oral cavity) cancer, breast cancer, gynecological cancer, esophageal cancer, lung cancer, colorectal cancer and liver cancer. Various risk factors are involved in the increase in this deadly disease, e.g., use of tobacco, areca nut, chewable tobacco, snuff, niswar, etc. [12,13,14,15]. The observed disease trends have substantially changed with respect to older studies from our institute [42].
Availability of Data and Material
The raw data used in this study may be requested from the authors.
Abbreviations
- GLOBOCAN:
-
Global cancer incidence
- NIMRA:
-
Nuclear Institute of Medicine and Radiotherapy
- PAEC:
-
Pakistan Atomic Energy Commission
- HMIS:
-
Hospital Management and Information System
- HER2:
-
Human epidermal growth factor receptor 2
- HCC:
-
Hepatocellular carcinoma
References
Wu C, et al. Analysis of status and countermeasures of cancer incidence and mortality in China. Sci China Life Sci. 2019;62(5):640–7.
Parkin DM. Global cancer statistics in the year 2000. Lancet Oncol. 2001;2(9):533–43.
Sung H, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Cancer J Clinicians. 2021;71(3):209–49.
Baskar R, Lee KA, Yeo R, Yeoh K-W. Cancer and radiation therapy: current advances and future directions. Int J Med Sci. 2012;9(3):193.
Silas OA, et al. Changing patterns in trend of top 10 cancers in the Jos University Teaching Hospital’s (JUTH) cancer registry (1996–2018), Jos, north-central Nigeria. J Med Tropics. 2019;21(2):81.
Joshi P, Nair S, Chaturvedi P, Nair D, Agarwal J, D’Cruz A. Delay in seeking specialized care for oral cancers: experience from a tertiary cancer center. Indian J Cancer. 2014;51(2):95.
Olaleye O and Ekrikpo U. Epidemiology of cancers in sub-Saharan Africa. In: Cancer in Sub-Saharan Africa: Springer, 2017, p. 3–19.
C. R. UK, "Worldwide cancer statistics," ed, 2012.
Wild CP, Stewart BW, Wild C. World cancer report 2014. Geneva: World Health Organization; 2014.
Nishtar S, Bile KM, Ahmed A, Amjad S, Iqbal A. Integrated population-based surveillance of noncommunicable diseases: the Pakistan model. Am J Prev Med. 2005;29(5):102–6.
Park S, Bae J, Nam B-H, Yoo K-Y. Aetiology of cancer in Asia. Asian Pac J Cancer Prev. 2008;9(3):371–80.
Rozi S, Akhtar S. Prevalence and predictors of smokeless tobacco use among high-school males in Karachi, Pakistan. Eastern Mediterranean Health J. 2007;13(4):916–24.
Goldenberg D, et al. Habitual risk factors for head and neck cancer. Otolaryngology. 2004;131(6):986–93.
Mazahir S, et al. Socio-demographic correlates of betel, areca and smokeless tobacco use as a high risk behavior for head and neck cancers in a squatter settlement of Karachi, Pakistan. Substance Abuse Treat Prev Policy. 2006;1(1):1–6.
Maqbool S, Leghari MA, Ali S. The prevalence of use of areca nut and its effect on oral health in school going children in Gadap town, Malir, Karachi, Pakistan. World Journal of Dentistry. 2016;7(1):6–9.
Shah S, Merchant A, Luby S, Chotani R. Addicted schoolchildren: Prevalence and characteristics of areca nut chewers among primary school children in Karachi, Pakistan. J Paediatr Child Health. 2002;38(5):507–10.
Yeole BB. Trends in incidence of head and neck cancers in India. Asian Pac J Cancer Prev. 2007;8(4):607–12.
Bile K, Shaikh J, Afridi H, Khan Y. Smokeless tobacco use in Pakistan and its association with oropharyngeal cancer. EMHJ-Eastern Mediterranean Health J. 2010;16(Suppl):24–30.
Dhull AK, Atri R, Dhankhar R, Chauhan AK, Kaushal V. Major risk factors in head and neck cancer: a retrospective analysis of 12-year experiences. World J Oncol. 2018;9(3):80.
Soomro R, Faridi S, Khurshaidi N, Zahid N, Mamshad I. Age and stage of breast cancer in Pakistan: an experience at a tertiary care center. J Pak Med Assoc. 2018;68(11):1682–5.
Banning M, Hafeez H, Faisal S, Hassan M, Zafar A. The impact of culture and sociological and psychological issues on Muslim patients with breast cancer in Pakistan. Cancer Nurs. 2009;32(4):317–24.
Barnard ME, Boeke CE, Tamimi RM. Established breast cancer risk factors and risk of intrinsic tumor subtypes. Biochimica et Biophysica Acta (BBA). 2015;1856(1):73–85.
Tamimi RM, et al. Traditional breast cancer risk factors in relation to molecular subtypes of breast cancer. Breast Cancer Res Treat. 2012;131(1):159–67.
Kelsey JL, Gammon MD, John EM. Reproductive factors and breast cancer. Epidemiol Rev. 1993;15(1):36–47.
Asif HM, Sultana S, Akhtar N, Rehman JU, Rehman RU. Prevalence, risk factors and disease knowledge of breast cancer in Pakistan. Asian Pac J Cancer Prev. 2014;15(11):4411–6.
Wasim T, Mushtaq J, Wasim AZ. Gynecological malignancies at tertiary care hospital, Pakistan: a five-year review. Pakistan J Med Sci. 2021;37(3):621.
Klingelhöfer D, Zhu Y, Braun M, Brüggmann D, Schöffel N, Groneberg DA. A world map of esophagus cancer research: a critical accounting. J Transl Med. 2019;17(1):1–14.
Arnal MJD, Arenas ÁF, Arbeloa ÁL. Esophageal cancer: Risk factors, screening and endoscopic treatment in Western and Eastern countries. World J Gastroenterol. 2015;21(26):7933.
Blot WJ. Esophageal cancer trends and risk factors. Semin Oncol. 1994;21(4):403–10.
Zakiullah Z, et al. Genetic susceptibility to esophageal cancer due to CYP1A1 gene variant rs4646903 in tobacco addicted patients of Pashtun ethnicity: a case control study in Khyber Pakhtunkhwa province of Pakistan. Asian Pac J Cancer Prev. 2014;15(16):6715–20.
Malhotra J, Malvezzi M, Negri E, La Vecchia C, Boffetta P. Risk factors for lung cancer worldwide. Eur Respir J. 2016;48(3):889–902.
Akhtar N, Bansal JG. Risk factors of Lung Cancer in nonsmoker. Curr Probl Cancer. 2017;41(5):328–39.
Mármol I, Sánchez-de-Diego C, Pradilla Dieste A, Cerrada E, Rodriguez Yoldi MJ. Colorectal carcinoma: a general overview and future perspectives in colorectal cancer. Int J Mol Sci. 2017;18(1):197.
Stintzing S. Management of colorectal cancer. F1000prime Rep. 2014. https://doi.org/10.12703/P6-108.
Markowitz SD, Bertagnolli MM. Molecular basis of colorectal cancer. N Engl J Med. 2009;361(25):2449–60.
Hafeez-Bhatti AB, Dar FS, Waheed A, Shafique K, Sultan F, Shah NH. Hepatocellular carcinoma in Pakistan: national trends and global perspective. Gastroenterol Res Pract. 2016. https://doi.org/10.1155/2016/5942306.
Bosch FX, Ribes J, Díaz M, Cléries R. Primary liver cancer: worldwide incidence and trends. Gastroenterology. 2004;127(5):S5–16.
Smedby KEM, Baecklund E, Askling J. Malignant lymphomas in autoimmunity and inflammation: a review of risks, risk factors, and lymphoma characteristics. Cancer Epidemiol Biomark Prev. 2006;15(11):2069–77.
Foxman B. The epidemiology of urinary tract infection. Nat Rev Urol. 2010;7(12):653–60.
Yaxley JP. Urinary tract cancers: an overview for general practice. J Family Med Primary Care. 2016;5(3):533.
Patel AR, Klein EA. Risk factors for prostate cancer. Nat Clin Pract Urol. 2009;6(2):87–95.
Mangi F, Laghari N, Memon S, Zehra N. Top ten cancers’ incidence assessment in South Sindh’s Cancer Hospital. Int J Radiol Radiat Ther. 2017;2(2):00019.
Acknowledgements
We thank Dr. Rameez-Ul-Islam Raja for providing valuable guidance.
Funding
This study did not receive any external grants from government, private or commercial sources.
Author information
Authors and Affiliations
Contributions
FA and SH contributed to writing the manuscript and the literature review. FA designed the study/basic concept, wrote sections of the manuscript and analyzed the data. SA and SS wrote parts of the manuscripts, proofread the manuscript and provided insights in interpretation.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflicts of interest.
Ethical Approval and Consent to Participate
Not applicable.
Consent to Publication
Not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ali, F., Hussain, S., Memon, S.A. et al. Recently Top Trending Cancers in a Tertiary Cancer Hospital in Pakistan. Dr. Sulaiman Al Habib Med J 5, 42–49 (2023). https://doi.org/10.1007/s44229-023-00028-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s44229-023-00028-z