
Abstract
Background
The social, cultural, and ethnic diversity of healthcare workers should match that of the U.S. population to improve health outcomes and decrease health disparities. The population’s diversity is increasing, though many health care professions lack diversity in their academic programs. The holistic admissions (HA) process considers an applicant’s unique experiences, achievements, and traits in addition to academic metrics when making admission decisions. HA has been shown to be an effective strategy to increase cohort diversity by considering the whole person instead of focusing on academic metrics.
Purpose
This study explored the extent to which U.S. Doctor of Physical Therapy (DPT) programs are implementing HA in their admissions process to diversify their admitted cohorts. The study further examined how programs defined diversity.
Methods
Using a cross-sectional, descriptive research design, 272 accredited DPT programs were invited to complete an online survey to collect data on admissions practices. Cross-tabulation was used to analyze coded responses. Inductive thematic analysis was used for open-ended responses.
Results
Thirty-five (71.4%) of the 52 respondents reported they were currently or were planning to use HA in their respective DPT program. Most respondents (88.6%) reported a positive experience, including an increase in student cohort diversity without a decrease in graduation rate. Four themes emerged as the definition of diversity: ethnicity (i.e., under-represented minorities), other demographics, life experiences, and challenges overcome.
Conclusion
Although this study represents a sample of DPT programs, the data show most programs using HA and have experienced increased diversity without a risk to academic performance.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
According to the 2020 Census report, the U.S. population is more diverse than ever [1]. As the diversity of the country’s population continues to increase, the need for a more diverse health care workforce also increases [2]. A diverse health care workforce is an effective strategy to reduce health disparities in underserved populations. When health care providers share the same characteristics with their patients, research shows that patients have a greater trust in their provider and report higher satisfaction rates [3,4,5]. Students from underserved populations who complete a health care program are likely to return to their home communities, serving such populations at risk for health disparities [6].
The Association of American Medical Colleges [7] first defined under-represented minorities (URM) as poorly represented racial and ethnic populations in the medical profession as compared to their respective numbers in the general population. To combat the lack of URM in medicine, the AAMC established the Holistic Review Project nearly 20 years ago. The project aimed to increase diversity in medicine by considering more than an applicant’s academic scores in the admissions process [8, 9].
1 Literature review
The Holistic Review Project has since become the driving factor for other health professions to successfully increase cohort diversity in their respective professions using holistic review as part of a holistic admissions (HA) process [3, 4, 6, 10,11,12,13,14]. Holistic review is defined as a method of reviewing an applicant’s information that considers the whole person instead of focusing on traditional academic metrics [15]. Medical schools, physician assistant programs, social work, nursing, speech-language pathology, and general undergraduate admissions demonstrated that holistic review is an effective strategy to evaluate an applicant as a whole and “read between the lines” of the application [16,17,18,19,20,21,22,23].
The AAMC enhanced the HA process by developing the Experiences-Attributes-Metrics (EAM) model, which increased diversity in the medical profession by focusing on the whole applicant, instead of on mainly academic metrics [5]. Other professions used the EAM model as a foundation for their HA process and subsequently, developed a list of noncognitive factors, or professional values. The presence of noncognitive factors helped determine if an applicant had the traits needed to graduate from a professional health program and successfully practice in their intended profession [3, 5, 9, 12, 14, 18, 19, 22, 25, 26]. Other characteristics, traits, and experiences assessed in a holistic review using an EAM model include the ability to work in a team, adaptability, cultural sensitivity, autonomy, integrity, and grit, all imperative qualities for health care workers [18, 19, 22, 24, 25].
Many authors used the AAMC’s definition of URM in their studies [3, 5, 9, 23, 25,26,27,28,29]. More recently, diversity has expanded to include socio-economic status, gender (identity), heritage, culture, family status, educational level, geographic location, military background, sexual orientation, age, religion, and disability [3,4,5, 9, 18, 23, 27,28,29].
Research supports the use of holistic review as an effective strategy to promote students from URM and other under-represented groups through the admissions process. As DPT programs consider holistic review as a part of HA, the importance of the Graduate Record Examination (GRE) score’s ability to predict passing the national board exam should not be ignored [3, 28, 30, 31]. Any change in admission criteria while transitioning to a holistic review should consider minimum scores needed to pass the national licensing exam [3, 6, 28, 32].
Despite research supporting the need for increased diversity in the PT profession, Doctor of Physical Therapy (DPT) programs have been slow to adopt holistic review in the admissions process [26, 28]. Wise et al. (2017) examined diversity in the PT profession and found it lacked representation of Black/African American and Hispanic/Latino as compared to their respective representation in the national population, while Whites and Asians were adequately represented. Like other professions, the racial distribution of PTs fails to mirror the U.S. population [26, 28].
2 Study purpose
Previous studies about HA recognized the need for further research across health care professional programs [4, 16, 19, 21, 26, 33]. Canham et al. [3] found that while HA helped increase the diversity in their admitted cohorts, more data, case reports, and research are needed to understand the effects on diversifying the PT profession. Current research supports using HA to increase diversity, though research lacks the examination of current DPT program practices. The purpose of this study was to explore the extent to which U.S. DPT programs are implementing holistic review in their admissions process to diversify their admitted cohorts.
3 Methods
3.1 Research design
This study was a cross-sectional, descriptive research design using an anonymous, online survey emailed to potential participants. Coplan et al. [10] conducted a survey for physician assistant schools that collected similar data about the use of holistic review in admissions and the matriculation of URM from physician assistant programs in a qualitative study. Guiberson and Vigil [21] completed a quantitative study using a survey to collect data on speech-language pathology graduate programs about their experiences with HA processes. This study was approved by A. T. Still University’s IRB and the University of Wisconsin—Milwaukee’s IRB through a reliance agreement overseen by A.T. Still University’s IRB.
3.2 Study participants
According to the Commission on Accreditation in Physical Therapy Education [34], 272 accredited or developing DPT programs were operating in the United States at the start of this study. Of the 272 programs, 34 admit a freshman cohort who advance to the professional phase if they maintain certain academic requirements throughout their undergraduate schooling [35]. The remaining schools typically have an admissions committee made up of faculty, staff, alumni, and other individuals who review applications and offer slots for each cohort. The chair or head of the admissions committee was the target participant for this project. A list of DPT program directors and contact information for individuals responsible for admissions was obtained from the centralized application service website [34], which provided a direct mechanism to reach targeted participants via email distribution.
3.2.1 Sampling methodology
Participants were selected using a non-probability, purposive sampling method. The sample exclusively targeted individuals involved in the admissions process. The recruitment email included transparent inclusion criteria requiring the person who took the survey to be employed in a U.S. DPT program with working knowledge of the admissions process.
3.3 Survey development
Guiberson and Vigil [21] conducted a similar study that examined HA in speech-language pathology programs using an adopted survey from two previous studies cited in their paper [11, 36]. With permission from Guiberson [21], a modified version of their survey was used in this study, consisting of seven sections and 35 multiple choice and short answer questions.
The survey modifications included changing all references of Graduate Speech and Language Pathologists used in the Guiberson and Vigil [21] survey to Doctor of Physical Therapy for this study. Additionally, nine options were added to the list of ‘non-academic attributes’ considered in the admission process question, making the list more inclusive.
The survey collected data on U.S. DPT programs, not the individual participant, including the region of the country and the size of the geographic location where the program resides, and the admissions committee make-up.
3.3.1 Validity and reliability
The survey instrument used was a modified version of one used in a previous study but was not validated [21]. The modified survey was beta tested by four DPT admission team members familiar with the admissions process to assure the questions were clear and aimed at the research question.
3.4 Data collection and analysis
The electronic survey was distributed via email on January 23, 2022 using a link for each participant. Data were collected over 10 weeks, through March 31, 2022, and stored on a secure server through ATSU’s Qualtrics program. The survey data required both quantitative and qualitative analysis. All questions were coded for analysis. IBM SPSS Statistics version 28.0.1.0 was used for statistical analysis. The sample characteristics included three nominal variables, all analyzed using descriptive analysis for frequencies. No composite scoring or scales were used in the survey, but one question involved an open-ended response, which required qualitative analysis.
The study collected descriptive data on admission processes, so analysis mainly involved frequencies, though cross-tabulation was used to explore possible relationships or trends across programs. Three variables were scale or ratio variables: appropriate for normality testing. The data analysis was divided into (a) demographic information, (b) applicant screening requirements, (c) application review processes, (d) applicant selection processes, (e) holistic admission use, (f) evaluation processes, and (g) program diversity.
The last survey question included a text response and was treated like qualitative data. Using inductive thematic analysis, themes were identified that captured the variability in how each DPT program defined diversity in the context of admissions. Since the majority of the survey variables were quantitative, other qualitative factors (e.g., trustworthiness, quotes) were not addressed in the data analysis.
4 Results
4.1 Sample characteristics
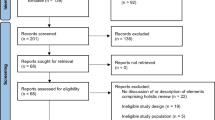
Of the 272 email invitations that were sent to fully accredited U.S. DPT programs, 58 respondents clicked on the survey link (21%). All 58 respondents met the inclusion criteria as the recruitment strategy was targeted, using purposive sampling. Six of the 58 respondent data were excluded for not meeting the requirement of completing at least 75% of the survey, which resulted in 52 respondent data used in the analysis, a 19% valid response rate.
The geographic location and population of the geographic location by the respondents represents where the program resides. Most of the programs represented in the survey data (48.1%) were from the South and are predominantly (67.3%) from urban areas (Table 1). The respondents represent a subset of the sample population. At the start of the study, 37% of DPT programs were located in the South and 77% were located in urban areas [37, 38].
The admissions committees of the represented programs were made up of a variety of individuals (Table 1). Most committees (98%) included representative(s) from the program’s core faculty. Additional committee members included staff with titles of administrative assistant or admissions coordinator (17%), faculty from other disciplines (15%), clinical community members (14%), adjunct faculty (14%), alumni (12%), and other members (10%).
4.2 Applicant screening requirements
Table 2 represents the academic metric screening requirements used to determine qualified applications. The United States uses a 4.0 grading scale, with 4.0 being the highest achievable grade point average (GPA). During application screening, 86% of programs reported using a minimum GPA, while only 28% reported using a minimum GRE score. Of the 43 programs using a minimum GPA, most programs (72.1%) required a 3.0 or higher cumulative GPA. Forty-two programs reported requiring a specific minimum pre-requisite GPA. Of those programs, most (76.2%) required at least a 3.0 or greater pre-requisite GPA.
The GRE is a standardized test often used in graduate admissions to assess applicants’ verbal reasoning, quantitative reasoning, and writing skills to predict success [30]. Fourteen respondents noted their program required a minimum GRE score for screening (Table 2). Of programs using a minimum GRE score for screening, most (64.3%) required a verbal score of at least 145 and (85.7%) a quantitative score of 140 (maximum possible score of 170). Twelve respondents noted their programs used a GRE writing minimum, requiring a mean of 3.042 (± 0.72) with a range of 1–3.5 (maximum possible score of 6).
4.3 Application review and applicant selection
Fifty respondents addressed the importance of academic metrics in the application review process (Table 3). Most respondents (80%) noted academic metrics were somewhat more important or the most important criteria, and 14% noted they were equally as important as other criteria. Similarly, for the non-academic attributes, nearly 33% reported socio-economic status, foreign language ability, ethnicity, underserved community origin, first generation, and experience with disadvantaged populations to be important factors. Less important factors included applicant’s geographic origin, gender, and others (Table 3). Other specific criteria related to program goals were found to be important to programs in the application selection process. Applicants with a focus on underserved areas (69.2%), both urban and rural, were more important than matching the program’s global health (13.5%) or research (3.8%) mission.
4.4 Use of holistic admissions
Thirty-five (71.4%) of the 52 respondents reported using or were planning to use holistic review, while 14 programs (28.6%) responded as not currently using or considering holistic review. Three programs did not respond and were marked as missing. Many programs did not get funding to implement HA (42.9%) or were unsure of any new resources (20%), while 34.3% of programs expected ongoing resources, and 2.9% only had resources to implement HA. One program did not report and was counted as missing. Table 4 represents the factors that motivated programs to implement HA. Most reported an interest in increasing the profession’s diversity (85.7%) and to shape admitted cohorts to align with the program’s mission and goals (77.1%).
Of the 35 respondents who reported using holistic review, two did not respond to the questions about changes in the admission process represented in Table 4. The main changes reported were adding non-academic criteria to the assessment (94.1%) and adding essays to identify students who faced barriers to academic success (70.6%). Chi-Square analysis did not show any significant association between DPT programs by geographic region or location.
4.4.1 Effect of holistic admissions
Most respondents reported a positive experience after implementing HA (88.6%). The positive outcomes and unintended consequences data were analyzed thematically. Sample responses included “recruiting passionate students,” increased diversity,” “more equitable process,” and “high graduation and licensure pass rates.” Three themes emerged from the positive outcomes: (a) increase in cohort diversity, (b) improved admissions process and applicant review, and (c) better prepared, successful, and employable students and graduates. Of respondents, 35% recorded unintended consequences in using a HA process. Using thematic analysis, three themes emerged: (a) academic struggles for students admitted holistically, (b) increased workload due to more complex review process, and (c) financial burden for students and programs due to other factors associated with the process. Of the 18 respondents, seven reported either no consequences or too early to tell.
Similar to the response on consequences, approximately one-third to one-half of the respondents noted it was too early to comment on any effects from implementing HA (Table 5). Of the respondents who noted an effect, 47.1% reported an increase in the program’s student diversity, and the majority noted either no change or an increase in average GPA of incoming class (54.3%) and graduation rate (51.5%).
4.4.2 Barriers
Of the 14 respondents who reported their program was not currently using or planning to use a holistic admission process, no programs were concerned with their national ranking (Table 6). Most programs (71.4%) were concerned that the students admitted may not be as prepared to succeed as those students admitted through the current admissions process.
4.5 Program evaluation processes
Of all respondents, the majority of programs track diversity of the incoming class and the average cumulative and pre-requisite GPAs of the incoming class (77.6%). Only 63.8% track the average GRE scores. The most common graduate outcomes tracked by programs were graduation rate (82.8%) and first time NPTE pass rate (79.3%). Most programs did not track the average GPA of graduating class (34.5%) or change in students' openness to ideas and perspectives different from their own (15.5%).
The mean number of applicants to the represented DPT programs was 392, with 45 participants responding. The mean total number of students enrolled in all phases of each DPT program represented was 116 (n = 46 programs). Of the 43 respondents who answered the question on number of CLD students currently enrolled, the majority of programs (51.2%) have fewer than 15% CLD students in their current cohorts (Fig. 1).

This figure demonstrates the total number of culturally and linguistically diverse (CLD) students enrolled in all phases of the participating DPT programs (n = 43). The x-axis represents the percent ranges of CLD students enrolled in programs and the y-axis represents the number of programs with CLD students in each percent range
4.6 Diversity defined
Programs defined the term diversity differently, as seen by the 27 survey responses. Participant definition of diversity included responses such as “Traditionally underrepresented minority groups,” “any member of a self-identified minority group,” “Life experiences, race, ethnicity, those of color, international, LGBTQ+, Appalachian,” and “racial and ethnic diversity, medically and economically underserved, first generation college, second language or ESL, Military status, second career.” Using inductive thematic analysis, the responses were coded, and four main themes emerged: (a) minority (ethnicity), (b) demographics (other than ethnicity), (c) life experiences/background, and (d) challenges faced/overcome. Four respondents did not provide a unique definition, did not know how their program defined diversity, or defaulted to another organization’s definition.
5 Discussion
The purpose of this study was to explore the use of holistic review in U.S. DPT programs as part of the admissions process to increase cohort diversity. The results provide a contribution to the PT profession demonstrating the current use of holistic review in the admissions process and the effect on diversity in student cohorts. The use of holistic review was slow to reach PT programs as compared to other health care professions [21, 26]. Study participants indicated that over 66% of the responding DPT programs are using or plan to use holistic review as part of the admissions process. The majority of DPT programs reported positive outcomes of holistic review, though not without challenges.
These findings are consistent with previous study outcomes. Implementing HA requires supportive leadership and a culture that encourages diversity and access to education [18, 20, 23, 39, 40]. The HA framework should align with program policies and mission statements, including a mechanism to evaluate and modify the process [3, 10, 13, 14, 18, 22, 23, 28]. Before implementing HA, reviewers should be adequately trained to ensure reliability throughout the holistic review process [3, 14, 20, 25, 41]. HA can be difficult to implement without adequate resources and support beyond the program level, which can be a barrier for some programs in adopting HA processes.
The U.S. Supreme Court’s ruling to ban the use of affirmative action practices in college admissions has many schools anxious about how to ensure their commitment to diversity in their programs [42, 43]. Affirmative action relies on a single metric from the application to determine the applicant’s ethic or cultural identity [42]. HA is more effective in identifying an applicant’s lived experiences that relate to their culture or ethnic identity from narrative portions of the application (e.g., essays, personal statements, and letters of recommendation). The review process then focuses on evaluating the applicant’s fit in the context of the program’s mission [43, 44]. Once a program determines what diversity means for them, using HA to evaluate applicants on metrics, attributes, and experiences provides a more comprehensive method to increase cohort diversity than affirmative action. The use of HA is a logical alternative to affirmative action to improve diversity of admitted students. As such, the new ruling should trigger an increase in HA use [42,43,44].
5.1 Limitations
This study targeted accredited U.S. DPT programs using contact information for admission questions that were available on the centralized application website and on program website pages. While the participants were targeted, only a small percentage of programs responded, with most responses representing urban programs from the South. The data may not be representative of all U.S. DPT programs. The survey questions purposely captured program demographic data and basic information about current admissions processes but did not collect any details or nuances about each program’s use of holistic review or their admissions process.
While the participants self-reported increases in student cohort diversity, consideration for other factors that may have led to such increases were not addressed in the survey.
Using validated surveys ensure reliability and validity. The use of a non-validated survey was a limitation in this study. The survey instrument used was chosen as a suitable option as no validated surveys were found to be specific for collecting information from DPT programs. As a result, using a modified version of a previously validated survey was the best option available.
Lastly, the data were from one point in time, not across time, making it difficult to discern outcomes from a diverse cohort, as compared to cohorts admitted through traditional admission processes. A longitudinal study examining the specific differences within programs could better predict the long-term effects of holistic review on cohort diversity and their respective student outcomes.
The results from this study describe the use of holistic review in a sample of U.S. DPT programs. As many programs strive to increase cohort diversity, each program’s working definition of diversity differs. The results from this study confirm that most programs successfully increased diversity, without compromising student outcomes. While programs experienced challenges implementing holistic review, many indicated positive outcomes.
6 Conclusion
Holistic review in a DPT program’s strategic admission initiative to increase cohort diversity can successfully meet the goal of matching the admitted cohort’s diversity to the general population. Holistic review considers applicants for all the qualities they can bring to a program, not only academic abilities. Future research is needed to compare the specific HA process used in programs having success with minimal barriers or consequences. Follow-up studies could be conducted to target schools represented in this study using a qualitative design to examine the details of their admission processes and outcomes. For holistic review to work in a HA process, the applicant pool itself needs to be diverse. Exploring recruitment practices may inform strategies to attract diverse students to the PT profession. While the results of this study superficially touched on the challenges, successes, and outcomes of participating programs, future studies could further examine best practices in the HA review process using an EAM model and provide guidance to programs hesitant to use HA.
Data availability
The data that support the findings of this study are not openly available due to reasons of sensitivity and are available from the corresponding author upon reasonable request. Data are located in controlled access data storage at A.T. Still University.
References
United States Census Bureau. 2020 U.S. population more racially and ethnically diverse than measured in 2010. 2021. https://www.census.gov/library/stories/2021/08/2020-united-states-population-more-racially-ethnically-diverse-than-2010.html#:~:text=1%20The%20most%20prevalent%20racial%20or%20ethnic%20group,non-Hispanic%20population%20was%20the%20third-largest%20group%20at%2012.1%25.
Goode CA, Landefeld T. The lack of diversity in healthcare: causes, consequences, and solutions. J Best Pract Health Prof Divers Educ Res Policy. 2019;11(2):73–95.
Canham L, Mañago M, Dannemiller L, Rapport M. Holistic review in doctor of physical therapy admissions can lead to enhanced diversity in admitted students. J Phys Ther Educ. 2021;35(3):195–202. https://doi.org/10.1097/JTE.0000000000000192.
James TG, Sullivan MK, Varnes JR. Improving representation of people with disabilities in health education. Pedagog Health Promot. 2020. https://doi.org/10.1177/2373379920978822.
Thomas B, Dockter N. Affirmative action and holistic review in medical school admissions: where we have been and where we are going. Acad Med. 2019;94(4):473–6. https://doi.org/10.1097/ACM.0000000000002482.
Raffoul M, Bartlett-Esquilant G, Phillips R. Recruiting and training a health professions workforce to meet the needs of tomorrow’s health care system. Acad Med. 2019;94(5):651–5. https://doi.org/10.1097/ACM.0000000000002606.
Association of American Medical Colleges (AAMC). Underrepresented in medicine: definition. 2004. https://www.aamc.org/initiatives/urm.
Diaz T, Huerto R, Weiss J. Making merit just in medical school admissions. AMA J Ethics. 2021;23(3):E223–8. https://doi.org/10.1001/amajethics.2021.223.
Witzburg RA, Sondheimer HM. Holistic review: shaping the medical profession one applicant at a time. N Engl J Med. 2013;368(17):1565–7. https://doi.org/10.1056/NEJMp1300411.
Coplan B, Todd M, Stoehr J, Lamb G. Holistic admissions and underrepresented minorities in physician assistant programs. J Physician Assist Educ. 2021;32(1):10–9. https://doi.org/10.1097/JPA.0000000000000337.
Glazer G, Danek J, Michaels J, Bankston K, Fair M, Johnson S, Nivet M. Holistic admissions in the health professions: findings from a national survey. Urban universities for health report. 2014. https://www.aplu.org/library/holistic-admissions-in-the-health-professions/File.
Scott LD, Zerwic J. Holistic review in admissions: a strategy to diversify the nursing workforce. Nurs Outlook. 2015;63(4):488–95. https://doi.org/10.1016/j.outlook.2015.01.001.
Snyder C, Frogner B, Skillman S. Facilitating racial and ethnic diversity in the health workforce. J Allied Health. 2018;47(1):58–65.
Wros P, Noone J. Holistic admissions in undergraduate nursing: one school’s journey and lessons learned. J Prof Nurs. 2018;34(3):211–6. https://doi.org/10.1016/j.profnurs.2017.08.005.
Association of American Medical Colleges (AAMC). Holistic review. n.d. https://www.aamc.org/services/member-capacity-building/holistic-review.
Bastedo MN, Bowman NA, Glasener KM, Kelly JL. What are we talking about when we talk about holistic review? Selective college admissions and its effects on low-SES students. J High Educ. 2018;89(5):782–805. https://doi.org/10.1080/00221546.2018.1442633.
Conrad S, Addams A, Young G. Holistic review in medical school admissions and selection: a strategic, mission-driven response to shifting societal needs. Acad Med. 2016;91(11):1472–4. https://doi.org/10.1097/ACM.0000000000001403.
Coplan B, Evans BC. How organizational culture influences holistic review: a qualitative multiple case study. Adv Health Sci Educ Theory Pract. 2021. https://doi.org/10.1007/s10459-021-10055-w.
Francis AM, Klein LB, Thomas SH, Kainz K, Blank Wilson A. Holistic admissions and racial/ethnic diversity: a systematic review and implications for social work doctoral education. J Soc Work Educ. 2021;58:1–18. https://doi.org/10.1080/10437797.2021.1895927.
Glazer G, Tobias B, Mentzel T. Increasing healthcare workforce diversity: urban universities as catalysts for change. J Prof Nurs. 2018;34(4):239–44. https://doi.org/10.1016/j.profnurs.2017.11.009.
Guiberson M, Vigil D. Speech-language pathology graduate admissions: implications to diversify the workforce. Commun Disord Q. 2021;42(3):145–55. https://doi.org/10.1177/1525740120961049.
Lancaster R, Baseman E, Smolinski L. A quality improvement project: defining and operationalizing a holistic admission selection policy. J Prof Nurs. 2020;36(4):259–63. https://doi.org/10.1016/j.profnurs.2020.01.003.
Morrow MR. Holistic admission: what is it? How successful has it been in nursing, and what are the possibilities? Nurs Sci Q. 2021;34(3):256–62. https://doi.org/10.1177/08943184211010431.
Hossler D, Chung E, Kwon J, Lucido J, Bowman N, Bastedo M. A study of the use of nonacademic factors in holistic undergraduate admissions reviews. J High Educ. 2019;90(6):833–59. https://doi.org/10.1080/00221546.2019.1574694.
Rosenberg L. A practical guide for implementing a holistic admissions review. J Nurs Educ. 2019;58(11):669–73. https://doi.org/10.3928/01484834-20191021-11.
Wise D, Dominguez J, Zoher K, Williams-York B, Moerchen V, Brooks S, Ross L. Defining underrepresented minorities and promoting holistic review admission strategies in physical therapist education. J Phys Ther Educ. 2017;31(4):8–13. https://doi.org/10.1097/JTE.0000000000000009.
Grabowski CJ. Impact of holistic review on student interview pool diversity. Adv Health Sci Educ. 2018;23(3):487–98. https://doi.org/10.1007/s10459-017-9807-9.
Greene R, Karavatas S. Increasing diversity in the physical therapy profession by addressing deficiencies in the performance of African Americans on the national physical therapy examination. J Best Pract Health Prof Divers Educ Res Policy. 2018;11(1):51–9.
Halpern-Felsher B, McLaughlin S. Need for advancing underrepresented minorities in the health sciences and medicine. J Health Disparities Res Pract. 2019;12(4):3–6.
Coleman-Salgado B, Barakatt E. Identifying demographic and preadmission factors predictive of success on the national physical therapy licensure examination for graduates of a public physical therapist education program. J Phys Ther Educ. 2018;32(1):8–16. https://doi.org/10.1097/JTE.0000000000000020.
Talamantes E, Henderson MC, Fancher TL, Mullan F. Closing the gap—making medical school admissions more equitable. N Engl J Med. 2019;380(9):803–5. https://doi.org/10.1056/NEJMp1808582.
Wilson MA, Odem MA, Walters T, DePass AL, Bean AJ. A model for holistic review in graduate admissions that decouples the GRE from race, ethnicity, and gender. CBE Life Sci Educ. 2019;18(1):ar7. https://doi.org/10.1187/cbe.18-06-0103.
Shulman J. The data we need for holistic admissions. Change. 2018;50(5):8–15. https://doi.org/10.1080/00091383.2018.1510256.
Commission on Accreditation in Physical Therapy Education. Welcome to the commission on accreditation in physical therapy education! 2020. https://www.capteonline.org/.
American Physical Therapy Association. Becoming a PT. n.d. https://www.apta.org/your-career/careers-in-physical-therapy/becoming-a-pt.
Bronheim S, Goode T. Climate of the learning environment: cultural and linguistic competence checklist for MCH training programs. National Center for Cultural Competence, Georgetown University Center for Child and Human Development. 2013. https://nccc.georgetown.edu/documents/NCCC-Climate-Checklist.pdf.
Commission on Accreditation in Physical Therapy Education. Aggregate program data: 2021 physical therapist education programs fact sheet. 2021. https://www.capteonline.org/globalassets/capte-docs/aggregate-data/archive/pts/2021-2022-aggregate-pt-program-and-salary-data.pdf.
Felter CE, Zalewski K, Jermann R, Palmer PL, Baier AE, Falvey JR. Rural health: the dirt road less traveled. Phys Ther. 2022;102(11): pzac112. https://doi.org/10.1093/ptj/pzac112.
Grbic D, Morrison E, Sondheimer HM, Conrad SS, Milem JF. The association between a holistic review in admissions workshop and the diversity of accepted applicants and students matriculating to medical school. Acad Med. 2019;94(3):396–403. https://doi.org/10.1097/ACM.0000000000002446.
Wilbur K, Snyder C, Essary A, Reddy S, Will K, Saxon M. Developing workforce diversity in the health professions: a social justice perspective. Health Prof Educ. 2020;6(2):222–9. https://doi.org/10.1016/j.hpe.2020.01.002.
Rideout BM. Variance and inter-rater reliability in holistic admissions review. College Univ. 2018;93(3):2–13.
Association of American Medical Colleges (AAMC). How can medical schools boost racial diversity in the wake of the recent Supreme Court ruling? 2023. https://www.aamc.org/news/how-can-medical-schools-boost-racial-diversity-wake-recent-supreme-court-ruling.
Kean N. Moving from affirmative action toward holistic admissions. 2023. https://www.clinicaladvisor.com/home/topics/practice-management-information-center/affirmative-action-holistic-admissions/.
Carlton G. Will holistic review replace affirmative action in the admissions process? 2023. https://nursejournal.org/articles/holistic-review-vs-affirmative-action/.
Funding
The authors declare they have no financial interests related to this paper and received no funding for writing it.
Author information
Authors and Affiliations
Contributions
All authors contributed to the drafting, editing, and reviewing of this manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Informed consent was obtained from all participants. No participants under 18 years of age were eligible to participate in the study.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Mazurek, R., Mathieson, K. Current holistic admission review practices of U.S. doctor of physical therapy programs. Discov Educ 3, 50 (2024). https://doi.org/10.1007/s44217-024-00134-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s44217-024-00134-6