
Abstract
This study aims to analyse the impact of the 2006 Yogyakarta earthquake on the mental health and welfare of victims in Bantul and to examine whether disasters they experienced before might increase or decrease their mental health when facing indirect exposure to repeated disasters. This study employs several methods: descriptive analysis; logit; a combination of propensity score matching; and difference in differences. The results find that 7 people (1.78%) in 2007 and 31 people (7.89%) in 2014 have experienced symptoms of depression. Age is confirmed as a significant factor in increasing this probability. The results of this study reveal that direct exposure to the 2006 Yogyakarta earthquake increased the average mental disorder score and decreased the victims’ education expenditure 1 year after the disaster. The direct exposure to the 2006 Yogyakarta earthquake also affected the increase in mental disorder score and decrease in household expenditure of victims 1 year after the disaster, although the effects were insignificant.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
Indonesia is highly vulnerable to natural disasters, such as earthquakes, volcanoes and tsunamis, since it lies in the Ring of Fire. One of the large-scale natural disasters that occurred in Indonesia between 2005 and 2019 was the Yogyakarta earthquake in 2006. Bappenas [5] reports that this disaster killed 5700 people, injured more than 40,000–60,000 people, destroyed hundreds of thousands of houses, and lost people’s livelihoods. Losses caused by this earthquake amounted to 29.1 trillion (US$ 3.1 billion). Losses of lives, houses, and infrastructure have been a corollary of natural disasters [32]. Furthermore, natural disasters can give serious impact on victims’ welfare [31]. The exposure to disasters might affect the welfare negatively in short period through the declines in household income and household expenditure levels of the victims [3, 4, 22, 27]. However, natural disasters do not only remain the negative impact. Belasen and Polachek [7] and Kirchberger [31] find that natural disasters have positive impact on workers’ wage growth in short period. The renewal of productive assets apparently changes their calamity in short period into higher prosperity in long period compared with those that are not exposed by disasters [22].
In contrast, Caruso and Miller [11] find that the negative impact of natural disasters on welfare is resilient in long period. They reveal that natural disasters affect welfare through two channels. First, natural disasters give negative impacts on children's physical health, malnutrition, the spread of disease, and lack of health services. Second, disasters affect the mental health. Damage and losses caused by disasters are closely related to the impact of disasters on psychological conditions [9], then they have negative impact on work productivity [1, 8, 10] and welfare. The individuals exposed to natural disasters have opportunities to suffer from Post-Traumatic Stress Disorder (PTSD), depression, or other mental illness which previous studies have found [9, 12, 13, 15, 17, 23, 24]. For this reason, post-disaster management is needed to minimize the continuous negative impact or long-term negative impact on the physique, economy, and also mental health.
The government carried out several stages of post-disaster management to reduce the negative impacts of the 2006 Yogyakarta earthquake [6]. With regard to physical and economic recovery in post-disaster, the government carried out rehabilitation and reconstruction focused on three program components: housing and settlement restoration; public infrastructure restoration; and economic recovery of communities and regions. This restoration was completed 2 years following the earthquake. Afterwards, the government addressed victims’ psychological problems by executing psychological assistance and psychological rehabilitation within 7 months after the earthquake. Interventions are given to victims to ease their psychological burdens and prevent continuous psychological impacts caused by disasters that lead to mental disorders.
In response to continuous psychological impacts that lead to mental disorder, post-disaster management, particularly in mental health, should be accomplished appropriately. It is due to natural disasters impacts might persist less than a year [15, 23, 25, 29], but it might be more than a year [9, 13, 17, 23, 24]. Chen et al. [13] find that the Chi-Chi earthquake victims remained indications of PTSD (20.9%) and psychiatric morbidity (39.8%) 2 years after the disaster. Almost 65% of PTSD symptoms were found 3 years after the Pakistan earthquake [17]. Cénat and Derivois [12] also find that 36.93% of respondents were indicated the symptoms of PTSD, 46.21% suffered from depression, and 22.25% were comorbidities between PTSD and depression two and half years after the Haiti earthquake. Also, a survey conducted 8 years after the Wenchuan earthquake by Guo et al. [24] find that 11.8% of respondents had symptoms of PTSD and 24.8% had symptoms of depression.
The psychological recovery has been implemented by the government over less than a year while the previous studies reveal that the continuous psychological impacts, like PTSD and depression, probably emerge more than a year after the earthquake. What is more, Indonesia is a disaster-prone country that triggers the victims to experience repeated trauma whenever natural disasters strike. Bland et al. [9] analyse the impacts of repeated experiences of similar disasters in Italy. They find that people who experienced two disasters and had evacuated from earthquake damage were indicated having a higher level of stress. They also suggest that previous disasters that people experienced could be a significant factor in triggering similar stress. Geng et al. [21] also find similar finding that there is a detrimental addictive effect on adolescent mental health due to repeated disaster experiences.
On the contrary, Norris and Murrell [38] find that people who experienced previous disasters were not influenced by trait anxiety and not stressed by particular weather. They emphasize that it ensued since experience might role as an excellent preventive measure for victims. Moreover, Seery et al. [39] conclude that those who have bad experiences with disasters will have lower levels of global distress, functional impairment, and post-traumatic stress symptoms. Then, they will have a higher level of life satisfaction than those who do not experience as bad experiences can build an individual’s resilience. Not only direct exposure to repeated disasters, but indirect exposure might also trigger mental disorders, such as mass media exposure [20, 40]. Acute stress is positively yielded from cumulative direct and indirect experiences and exposure to media from previous disasters [20]. Media exposure also negatively affects mental and physical health [40].
Studies of the long-term impacts of disasters on mental health are still limited, particularly in Indonesia. Therefore, the study of the long-term impacts of disasters on mental health is urgently needed for several reasons. First, several studies cited in the previous paragraphs indicate certain possibilities of disasters’ impact on mental health in a protracted period. Second, there is a linkage between natural disasters and welfare caused by mental health. Third, it is not certain whether experience will influence people’s preparedness for dealing with disasters or instead, they will be more sensitive and easier to get stressed. Due to the fact that Indonesia lies in the Ring of Fire thus disasters possibly occur repeatedly. Therefore, this study aims to investigate the impact of the 2006 Yogyakarta earthquake on the mental health of victims in Bantul. In addition, it will analyse the impact of the 2006 Yogyakarta earthquake on the welfare of victims in Bantul. Lastly, it will also examine whether disasters they experienced before might increase or decrease their mental health when facing indirect exposure to repeated disasters, the 2010 Merapi eruption.
2 Literature review
Mental disorders are evidently caused by exposure to disasters [35]. Mental disorders that victims may experience include PTSD, depression and other mental disorders. PTSD is a psychiatric disorder in individuals who have witnessed or experienced traumatic events, such as natural disasters and accidents. The intensity of exposure to disasters depends on the duration of the negative impacts on mental health. Besides, gender and age also could be significant factors that determine how long survivors are successfully recovered from their traumatic experiences. Several studies have revealed that women and children are highly vulnerable to mental disorders [13, 24, 26, 41]. Children might be the most vulnerable group since they are unable to escape from danger, identify themselves, make important decisions, and depend on themselves. They are at the highest risk to release a negative stress reaction when disasters affect them directly, such as losing a loved person or pet [33]. Other groups who are vulnerable to mental disorders when facing disasters are those who are poorly educated, have bad perceptions about health, have other traumatic experiences after disasters [24], reside in prefabricated houses, and have serious damage to their properties [13]. When these groups cannot solve their problems quickly and efficiently, the mental disorders can persist over several years after disasters, as reported by Guo et al., Cénat and Derivois [12, 24], and Chen et al. [13]. Furthermore, survivors with direct exposure to disasters have two conflicting possibilities. On the one hand, previous disaster experiences can significantly generate stress when survivors face repeated disasters [9]. Moreover, repeated disaster experiences might give a detrimental addictive effect on mental health, especially among adolescents [21].
On the other side, survivors can use previous disaster experiences as a preventive measure to minimize anxiety and stress [38]. Afterwards, Seery et al. [39] summarize that individuals’ resilience will build when they have disaster experiences or bad experiences. Yet, this resilience is built and developed through bad experiences at low or moderate levels. Individuals who completely do not have bad experiences cannot build resilience as they have no challenge in managing stress. On the contrary, having many challenges in managing stress (individuals with many bad experiences) will damage this resilience.
Several factors are believed can recover mental disorders after disasters. They are genetic, neurobiological, cognitive, cultural, psychosocial, and personal factors, as explained by Feder et al. [17]. Their study in Pakistan finds that life goals are one of the psychosocial factors that might reduce PTSD symptoms and increase positive emotions. In addition, an increase of positive emotions is associated with higher social support while a high level of symptoms and negative emotions are associated with negative religious coping (for instance, they feel being punished by God for sins or less religious personality). Besides psychosocial, culture is an essential factor in dealing negative impacts of disasters, related to victims’ psychological disorders. Masykur [37] explains that Javanese culture gave good contribution to managing stress caused by the 2006 Yogyakarta earthquake, one of them is tatag (being tough). Individuals with tatag will be a sincere, tough, and wise person in facing disasters. People with these personalities will be happier than those who refuse the reality.
Mental disorders and trauma from natural disasters are also believed may affect productivity. Then, an implication has been found that decrease of welfare is associated with the decrease in income. Bubonya et al. [10] reveal that mental illness is relatively expensive and vast. Individuals who suffered from mental illness tend to have a decline in work productivity. The survivors with poor mental health tend to have higher rates of absenteeism [10] and have worse work performance [1]. They also potentially have less opportunity to participate in labour market and have higher unemployment rates. It does not only give negative impacts on labour market and productivity, but Bubonya et al. [10] also mention that two costs emerge due to this mental illness. They are direct cost (costs of health care, disability payments, and provision of support services) and indirect cost (imposed to caregivers, family members, and society).
In addition, impact of natural disasters such as typhoons which occurred simultaneously during the COVID-19 pandemic caused an even deeper decline in welfare for individuals and communities. This is also further complicated by restrictions on population mobility which causes mental health to decline, especially stress and anxiety levels [14]. These findings regarding multiple disasters are also in line with Leppold et al. [34] which states that the potential risk of several disaster exposures exceeds the potential risk of one disaster exposure. Apart from that, there are also indirect implications due to changes in health service facilities, changes in community risk perceptions and government responses to various disasters. Lindert et al. [36] added that the COVID-19 pandemic period has provided many lessons that the impact of natural disasters will get worse, so it is necessary to develop new response models in dealing with disasters in the future. This model requires collaborative efforts from the public health sector, medical services, and emergency systems.
Furthermore, welfare is one of serious impacts that individuals might experience when natural disasters occur [31]. Losses of lives or human resources and private physical capital (such as productive assets and infrastructure) affect loss of income, decreased consumption, and reduced accumulation of human capital [4]. Losses and damage caused by disasters also give a change in local labour market [22]. In short term, the disruptions in local labour market caused by disasters have double impacts (positive and negative) on welfare. Gignoux and Menéndez [22] explains that it depends on the survivor’s position in labour market (as a supplier or a user of labor) and the ongoing business sector (for instance, construction sector will have an increase in workforce after disasters). These two factors subsequently affect the increase and decrease of workers’ wage that give impacts on consumption and welfare. It does not only give short-term impacts but also long-term impacts on welfare. The long-term impacts comprise two sides. First, welfare is at a significant disadvantage by the loss of assets. Second, welfare gains more benefits due to the renewal of lost assets.
Survivors who trapped in poverty for longer periods are caused by: the loss of productive assets [4, 22]; the diversion of current consumption investments; and reduced investment in human capital [4]. In addition, Gignoux and Menéndez [22] reveal that the poverty trap occurs when the return on assets locally increases. It is due to minimum requirements for the replacement of old production technology with a more productive one and the variation of input and output prices. They also confirm that poor regions that do not receive relief or get insufficient relief after disasters have a high probability to be stuck in poverty trap. On the contrary, an inflow of national or international resources that distributed as reconstruction attempt will positively affect the stock of public and private capital, revive and even increase several dimensions of welfare [4]. Afterwards, Gignoux and Menéndez [22] explain that renewals in capital stock, reliefs, and reconstructions after disasters potentially increase productivity in long period so that survivors’ income and welfare will increase.
3 Research methodology
3.1 Data
This study employed longitudinal survey data from the Indonesian Family Life Survey (IFLS) which was originally taken from the RAND Corporation. IFLS wave 3 (2000), 4 (2007), and 5 (2014) were used as the source of data. The sample used in this study were individuals between the ages of 15 and 70 in 2000, resided in Bantul before, during, and after the 2006 Yogyakarta earthquake (2000–2014), and experienced the 2006 Yogyakarta earthquake. Because of the fact that Indonesia is a vast archipelago and its high heterogeneity in geography, income, and population density, thus not all individuals in the IFLS sample are used in this research [31].
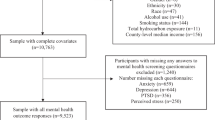
After cleaning and combining data of IFLS wave 3, 4, and 5, a sample of 393 individuals was obtained for each wave used in this study (see Fig. 1). After that, the data used included mental health, per capita household expenditure, the intensity of earthquake exposure, age, gender, marital status, education, and region.

Source: IFLS (processed)
Research sample.
3.2 Research variable
Mental health is measured by using the Center for Epidemiological Studies Depression Scale (CESD-10) 10-item questionnaire. There are 10-item questions that ask what the respondents feel within the past week. The questions include: I am bothered by things that usually would not bother me; I have difficulty concentrating on doing things; I feel depressed; I feel that what I do requires much effort; I feel hopeful about the future; I feel scared; I have trouble sleeping; I feel happy; I feel alienated; I cannot start anything. The scale for each question is 0–3 (0 = rarely or never, 1 = a little, 2 = sometimes, 3 = often).
Two proxies are used for mental health. First, mental disorder is measured by the total score of 6 CESD-10 questions, i.e. I feel bothered by things that usually do not bother me; I have difficulty concentrating on doing things; I feel what I do requires much effort; I feel scared; I have trouble sleeping; and I feel alienated. This study only uses 6 out of 10 questions because there are differences in the questions between batch 3 and waves 4 and 5. In addition, the scale used for each question is 0–2 (0 = never, 1 = sometimes, and 2 = often). Second, depression symptoms are measured by using a cut-off value of 10 and above, in which a person is confirmed to have significant depression symptoms if the total score of the ten questions in the CESD-10 is 10 and above [2].
Welfare outcomes are proxied through household expenditure per month per capita. Per capita household expenditure was divided into two parts, namely per capita food expenditure and per capita non-food expenditure. Per capita non-food expenditures were broken down into: per capita expenditures for frequently purchased goods and services (electricity/water/telephone, personal toiletries, household goods, domestic services, recreation and entertainment, transportation, and sweepstakes); per capita expenditure on goods and services that were rarely purchased (such as clothing, furniture, medicines, ceremony, and taxes); and per capita education expenditure for children living in the household (such as school fee, uniforms, and transportation).
Direct exposure to the earthquake refers to individuals who experienced the 2006 Yogyakarta earthquake and reported the death of their family members, suffered from severe injury or illness, had a direct financial loss or had family members who had been displaced. This study included people aged between 15 and 70 in 2000. Gender uses a dummy takes a value of 1 for men and 0 for other. Marital status is also represented with a dummy takes a value of 1 for married and 0 for other.
Education means the education length that each individual spent in formal school or education institution. Finally, the regional variables used in this study are the city dummy which has a value of 1 if individuals reside in urban areas and 0 otherwise. Then, the sub-district dummy has a value of 1 if they reside in Sewon District and 0 otherwise. Sewon District was chosen as the control variable since they had the largest number of residents who experienced direct exposure to earthquake. Based on IFLS 4 data, out of 355 people who were directly exposed to the earthquake, Sewon took the highest position with 100 victims, followed by Jetis with 92 people, Pandak with 59 people, and 104 others spread across several sub-districts in Bantul. Variable details are shown as the following (Table 1).
3.3 Analysis technique
This study employs three analytical methods to analyse the impact of natural disasters on mental health and welfare in Bantul: descriptive analysis; logit; a combination of propensity score matching; and difference in differences (PSM-DD). Descriptive analysis was used to investigate the number of Bantul residents who had depression symptoms in a year and 8 years after the 2006 Yogyakarta earthquake. The analysis was presented in cross-tabulation. Next, a logit regression was performed to determine certain factors that influenced depressive symptoms. This analysis used cross-sectional data only for wave 4, with samples taken from the combination of wave 3 and 4. The samples used in this analysis were individuals who resided in Bantul before, during, and 1 year after the 2006 Yogyakarta earthquake (2000 until 2007) and experienced the 2006 Yogyakarta earthquake. A sample of 507 individuals in wave 4 was obtained by cleaning and merging data, which was used in this logit analysis.
Logit model or logistic estimation method is a model that its dependent variable is the log of the odds ratio (a linear function of the independent variables). The probability function that underlies the logit model is the logistic distribution. The probability equation that represents the logistic distribution function is formulated as follows:
If Pi is the success category of Y, then (1 − Pi), the probability of failure is expressed as
so it can be written as
The value of Pi/(1 − Pi) refers to the odds ratio. It is the ratio between the probability of a successful event and the probability of a failure.
If its natural logarithm value is taken from the equation above, then the equation will change to
and it demonstrates that the natural logarithm of the odds ratio is not only linear with X, but also linear with the parameter. By using the symptoms of depression as the dependent variable, so it has a value of 1 if depression symptoms were found and 0 otherwise. The logistic regression model in this study is written as follows:
Finally, the difference in differences (DD) method was used to investigate the impact of direct exposure to earthquakes on mental health and welfare. DD method is a method that compares the change of outcome between treatment group and comparison group over time. This method combines two comparison methods, namely before-and-after and with-and-without comparisons.
The treatment group used in this study were individuals who experienced the 2006 Yogyakarta earthquake and reported the death of their family members, suffered from severe injury or illness, had a direct financial loss, or had family members who had been displaced. For the comparison group, this study used individuals who solely experienced the 2006 Yogyakarta earthquake but did not report the death of their family members, suffered from severe injuries or illness, had a direct financial loss, or had family members who had been displaced. The treatment group will have a value of 1 if they are exposed to direct exposure and 0 if they are not or the comparison group.
There are two DD models in this study. First, a model used to analyse the impact of earthquake on mental health and welfare 1 year after the 2006 Yogyakarta earthquake. This model was analysed by employing the combination data of waves 3 and 4 with 786 observations (393 individuals for each wave). Second, a model used to analyse the impact of earthquake on mental health and welfare 8 years after the 2006 Yogyakarta earthquake and 4 years after the 2010 Merapi eruption. The data used to estimate this model is waves 3–5 panel data with 1179 observations (393 individuals for each wave).
The difference in differences model in this study can be written as follows:
Outcome is income value of each dependent variable (mental disorder score and spending per capita), y07 is a dummy year which has a value of 1 if it is 2007 and 0 if it is 2000, y0714 is a dummy year which has a value of 1 if it is 2007 and 2014 and 0 if it is 2000, direct is a dummy of direct exposure or treatment with a value of 1 if it is exposed to direct exposure and 0 otherwise, and y07*direct and y0714*direct are interaction variables which are the average of DD effects of the 2006 Yogyakarta earthquake.
Afterwards, to minimize the estimation bias, models 6 and 7 were developed by adding individual characteristic variables, such as age, gender, marital status, education, and regional variables. Thus, modification of the difference in differences model which also used in this study is formulated as follows:
Khandker et al. [30] revealed that three conditions should be met first before DD regression is performed. First, model equation is specified correctly. Second, error term is not correlated with other variables in equation. Third, the existence of parallel-trend assumption (the most essential one), namely an assumption that unobserved characteristics that affect program participation do not vary over time. Therefore, to ensure that the parallel-trend assumption is fulfilled, the propensity score matching analysis is combined with difference in differences (PSM-DD).
PSM is performed to obtain a comparison group based on the probability of participating in a treatment group. It is implemented by using observed characteristics before the program period [30]. After the right match was found, the impacts of the 2006 Yogyakarta earthquake on mental health and spending were estimated by using the DD, based on samples in common support area. The equation to count the DD effect in common support as formulated as follows:
w(i, j) is the result of PSM weighting that are given to individuals in j-comparison group who have paired with individuals in treatment group.
4 Result and discussion
4.1 Descriptive statistics result
Table 9 (see appendix) presents descriptive statistics of individual characteristics in the base period or in 2000, based on IFLS 3 data. In this analysis, individuals were divided into two groups, namely treatment group (individuals who experienced the 2006 Yogyakarta earthquake and reported the death of their family members, suffered from severe injury or illness, had a direct financial loss, or had family members who had been displaced) and comparison group (individuals who solely experienced the 2006 Yogyakarta earthquake but did not report the death of their family members, suffered from severe injury or illness, had a direct financial loss, or had family members who had been displaced). In addition, Table 9 also shows p-value that is generated from the average results of the t-test between treatment and comparison groups.
The average age of individuals was 37 years for treatment group and 31 years for comparison group. The majority of the samples in treatment group were women (around 53%), yet the majority of the samples in comparison group are men (around 53%). Samples in both groups were dominated by individuals in marital status, around 73% for treatment group and around 66% for comparison group. The average length of education in treatment group was 8.5 years (2nd grade junior high school equivalent). It was lower than the comparison group, i.e., around 10 years (1st high school equivalent). The majority of individuals in both groups resided in urban areas. About 27% of individuals in treatment group and about 63% of individuals in comparison group resided in Sewon District.
For outcome characteristics, the average score of mental disorders in treatment group was 1.5 points out of a total score of 12 points, and this figure was lower than the comparison group amounted to 2 points. Moreover, the total of both food and non-food expenditures in the treatment group was also lower than in the comparison group. Based on the average results of the t-test there were several different characteristics found between the treatment and comparison groups. To deal with this difference problem, this study controlled all observed characteristics in model and used propensity score matching to obtain the right group pair.
Furthermore, Table 10 (see appendix) provides the descriptive statistics of victims’ condition when the 2006 Yogyakarta earthquake occurred. It has been reported that out of 355 people who experienced direct exposure to earthquake, 162 people reported their losses of business assets. The average loss of business assets was IDR2,523,006. Then, 336 out of 355 victims reported that the average loss of household assets was IDR18,400,000. Beside the loss of assets, 14 victims had revealed that they lost their family members and 38 people stated that 1 family member on average had suffered from injury or serious problem. The average medical expenses incurred by 353 out of 355 victims of direct exposure to the earthquake amounted to IDR5,804,703. The victims received relief amounted to IDR12,900,000 on average. The relief was obtained from various sources, namely 318 people received relief from the central government, 4 people from the central government and foreign governments/foreign NGOs/donors, 3 people from local governments, 7 people from other local NGOs, 1 person from individuals, 1 person from companies, 7 people from foreign governments/foreign NGOs/donors, and 12 people did not receive the relief. Subsequently, it has been reported that 318 out of 355 people resided in temporary shelters when the earthquake occurred, with an average duration of 119 days. Out of 318 people, 135 took refuge in shelters, 151 took refuge in tents outside the shelter, and the rest were spread in family-dwelling homes, friends’/neighbors’ homes, other dwellings, and open spaces.
In addition, the 2006 Yogyakarta earthquake also changed the asset ownership of many houses. Table 11 (see appendix) shows that the number of households who owned particular assets, such as houses and occupied land, houses/other buildings, land/area not used for farming/non-agricultural, vehicles, jewelry and household equipment, has dropped drastically from 2007 until 2014. However, there was no significant difference between husbands and wives in status or percentage of ownership. A high difference between wives and husbands was found for goods, such as houses and land people occupied, and savings/deposits/shares in 2014. The ownership percentage of assets was highly found in wives rather than in husbands. It indicates that husbands tend to sacrifice their assets during the economic recovery process after the 2006 Yogyakarta earthquake.
This study also demonstrates the number of victims who developed depression symptoms over 1 year and 8 years after the 2006 Yogyakarta earthquake by using the CESD-10 questionnaire with a cut-off point of 10 and above, as shown in Table 12 (see appendix). It also has been reported that 7 individuals (1.78%) developed significant depression symptoms in 2007 or 1 year after the earthquake. They were the ones who experienced the 2006 Yogyakarta earthquake and reported the death of their family members, suffered from severe injury or illness, had a direct financial loss, or had family members who had been displaced. Those who developed significant depression symptoms were divided into: 4 men and 3 women; 4 married, and 3 not married; 2 aged 16–35 years and 5 aged 36–55 years; 3 elementary graduates, 1 junior high school graduate, 1 senior high school graduate, and 2 above high school graduates; 5 reside in city and 2 reside in village; 2 reside in Sewon sub-district and 5 reside in other sub-districts.
It has been reported that 31 people developed significant depression symptoms in 2014 or 8 years after the 2010 Merapi eruption. Only 25 out of 30 people were confirmed as the direct exposure victims of the 2006 Yogyakarta earthquake whereas 6 people were not. In addition, there was only 1 of 7 people with significant depressive symptoms in 2007 whose depression symptoms persisted until 2014. These 31 people comprise: 15 men and 15 women; 23 married and 8 not married; 7 aged 16–35 years, 16 aged 36–55 years, 8 aged 56 years and above; 1 uneducated, 10 elementary graduates, 6 junior high school graduates, and 14 senior high school graduates; 30 reside in urban areas and 1 in rural areas; 11 reside in Sewon sub-district and 20 in other sub-districts.
4.2 Impact of earthquakes on depression symptoms
After obtaining the number of victims with significant depressive symptoms in 2007, the analysis was continued with logit regression to analyse certain risk factors which caused depressive symptoms. The regression used in this study was IFLS 4 data with a sample of 507 individuals. The estimation results are shown in Table 2.
The estimation results show that individuals who experienced direct exposure (OR = 1.230) and were men (OR = 2.641) are more likely to develop depression symptoms. Then, those who were married (OR = 0.461), had older age (OR = 0.949), had higher education level (OR = 0.935), resided in cities (OR = 0.433) and Sewon (OR = 0.993) were found less likely to develop depression symptoms. In addition, coefficient alpha for CESD itself (ceteris paribus) was OR = 0.558. However, age was simply found as a significant factor of all these risk factors that significantly affect the probability of depression symptoms. Somehow, through a more practical and clinical approach, according to Ferguson [18], several factors driving the probability of experiencing depression have a relatively modest impact, and even tend to have no effect as they are below the cut-off of 2.0. Only the male factor inclines to have a higher impact since it has OR of 2.641, though it still tends to be in a position approaching moderate effect.
4.3 Impact of earthquakes on mental disorders
The impact analysis was conducted by combining the propensity score matching and difference in differences (PSM-DD) methods through several stages. First, we entail observations in both treatment and comparison groups by relying on the observed characteristics in base period through the propensity score calculation. It was intended to find observations that located in common area. Second, the data in base period was subsequently paneled with the following data. Then, by using panel data and observations in common support, the analysis was continued by employing DD method. PSM results were listed in Appendix 2. Besides, this study also used fixed effects (FE) method to check the consistency of results and robustness.
The impact of the 2006 Yogyakarta earthquake on mental health was analysed using two different periods: 1 year after the 2006 earthquake and 8 years after the 2006 earthquake; and 4 years after the 2010 Merapi eruption. Table 3 shows the results of the estimated impact 1 year after the 2006 earthquake by employing a model without control variable and with control variable. On average, the 2006 Yogyakarta earthquake that caused individuals experienced direct exposure tends to have a 1.102 higher mental disorder score than the ones who experienced indirect exposure.
By including the control variable in the model, the mean of mental disorders score in treatment group was still higher than the comparison group, which was 1.076 and significant at the 5% level. A similar result was also found in fixed effects analysis and it confirmed that the model built was robust.
Furthermore, from 6 control variables used, 4 variables had a negative and significant correlation with mental disorder score while the other 2 variables had a negative and insignificant correlation. The four variables were age, gender, marital status, and residing in the city. A negative coefficient of 0.0200 in age variable defined that the average age increase over a year would reduce the mental disorder score by 0.0200 points and be significant at the 1% level. Gender was negatively and significantly correlated with a coefficient value of 0.270 which indicated that men on average had lower mental disorders score than women with a difference of 0.270 points and being significant at the 5% level. Moreover, those in marital status and residing in cities were also found had lower significant average mental disorder scores than those who were not married and residing in villages, with each individual difference: 0.537 points (significant at the 1% level) and 0.434 points (significant at the 5% level). The length of education and residing in Sewon District were confirmed had no significant relationship with mental disorders. Meanwhile, coefficient alpha for CESD was 3.666 points (significant at the 1% level).
Table 4 suggests the estimation results of the 2006 Yogyakarta earthquake’s impact on mental disorders 8 years after the 2006 earthquake and 4 years after the 2010 Merapi eruption. On average, the 2006 Yogyakarta earthquake has prompted individuals with direct exposure to have higher mental disorders score than individuals with indirect exposure, with a difference of 0.519. Similar figures were also obtained when regression was conducted by entering control variables into the DD model and the regression was conducted by using fixed effects. However, the findings confirm that the 2006 earthquake had no significant impact on mental disorder scores 8 years after the event and 4 years after the 2010 Merapi eruption.
Age and marital status were variables that significantly influenced the mental disorder score 8 years after the 2006 earthquake and 4 years after the 2010 Merapi eruption, while other variables were not. The age coefficient was negative at 0.0200, which defined that the age increase in a year would reduce the mental disorder score by 0.0200 points and be significant at the 1% level. Marital status was also negatively correlated with a coefficient value of 0.431 which indicated that married people on average had lower mental disorders score than unmarried people with a difference of 0.431 points and being significant at the 1% level. Furthermore, coefficient alpha for CESD was 3.123 points (significant at the 1% level).
4.4 Impact of earthquakes on per capita household expenditure
The analysis of the 2006 earthquake’s impact on per capita household expenditure was also estimated by employing the PSM-DD combination and the consistency of its results was checked by using fixed effects. The periods used were also the same: 1 year after the 2006 earthquake (Tables 5 and 6) and 8 years after the 2006 earthquake; and 4 years after the 2010 Merapi eruption (Tables 7 and 8).
Table 5 shows that the 2006 Yogyakarta earthquake has caused the treatment group has a IDR29,994.9 lower average household expenditure per capita than comparison group. In addition, when per capita household expenditure was broken down into per capita food expenditure and per capita non-food expenditure, it has found that the treatment group has lower average household expenditure per capita than comparison group, with a difference of IDR2685 and IDR30,267.9, respectively. The interesting results were found when per capita non-food expenditure was broken down into expenditure per capita for frequently purchased goods and services, rarely purchased goods and services, and education. The estimation results show that the 2006 Yogyakarta earthquake has caused the treatment group for frequently purchased goods and services and rarely purchased goods and services has higher average household expenditure per capita than comparison group, with a difference of IDR6703.1 and IDR12,478.1, respectively. On the contrary, the 2006 earthquake has caused the treatment group for lower education level has an IDR24,047.5 lower average household expenditure per capita than comparison group. However, the significant impact of the 2006 earthquake was only found in household education expenditure per capita and it was significant at the 5% level. Similar results were also found in fixed effects regression as shown in Table 6.
The findings confirm that age, gender, and length of education were the control variables that significantly influenced household expenditure per capita. Age has a positive coefficient of 3744.4 which defines that the average age increase in a year will raise household expenditure per capita by IDR3744.4 and be significant at the 1% level. Gender has a negative coefficient of 67,576.8, which indicates that men on average have lower household expenditure per capita than women by IDR67,576.8 and is significant at the 1% level. The length of education also has a positive coefficient of 30,254.7 which defines that the average length of education increase in a year will raise household expenditure per capita by IDR30,254.7 and be significant at the 1% level.
In addition, Table 7 illustrates the estimation results of the 2006 Yogyakarta earthquake’s impact on household per capita expenditure 8 years after the earthquake and 4 years after the 2010 Merapi eruption. The results show that the 2006 earthquake did not cause significant differences in per capita household expenditure between the two groups. When spending was split or not, even though the average household expenditure per capita in treatment group was lower than the comparison group, both treatment and comparison groups did not show significant differences. Similar results were found in the estimation of fixed effects in Table 8.
Age, gender, marital status, and length of education were confirmed as certain factors that might significantly affect per capita household expenditure 8 years after the event. Age significantly and positively influenced per capita household expenditure at the 1% level, with a coefficient value of 11,579.7. It indicates that the average age increase in a year will raise per capita household expenditure by IDR11,579.7.
A positive correlation is also found in the length of education with a coefficient value of 51,517.1, which indicates that the average increase of length of education in a year will raise per capita household expenditure by IDR51,517.1 and be significant at the 1% level. In addition, the findings confirm that those who are male and married have lower per capita household expenditures than those who are female and unmarried with a difference of IDR63,937.4 (significant at the 10% level) and IDR75,525.2 (significant at the 10% level), respectively.
4.5 Discussion
With regard to the results of descriptive analysis, logit analysis, and DD analysis of victims’ mental health 1 year after the 2006 Yogyakarta earthquake, the results suggest that the shock caused by direct exposure to the 2006 Yogyakarta earthquake had significantly increased mental disorder score, but this increase did not cause the victims to develop significant depressive symptoms. This phenomenon possibly occurs due to the low average score of mental health in Bantul before the earthquake. In terms of the happiness index, the low score of mental disorders might due to the high happiness index in D.I. Yogyakarta. Based on Statistics Indonesia (BPS) data in Socioeconomic Data Monthly Report Book, D.I. Yogyakarta in April 2018, D.I. Yogyakarta had high happiness index (ranked eighth in Indonesia), although its income inequality was highest in Indonesia. It indicates that D.I. Yogyakarta is a unique province that their residents are happy although they are in hardship. This high happiness index is attributed to the culture of Yogyakarta which mainly concerns with social capital, such as beliefs to others and cooperation.
The second factor that caused the victims did not develop depression symptoms is related to relative status. People tend to compare their actual conditions with other people in assessing their happiness [16]. Due to the fact that most of Bantul residents did not experience the direct exposure to the 2006 earthquake, the consideration of relative status would minimalize the negative impact of direct exposure to the earthquake toward depression symptoms. The estimation results of the earthquake's impact on household expenditure 1 year after the 2006 earthquake show that direct exposure to earthquake completely had caused individuals reduced their household expenditure, yet it was not significant. However, for education expenditure, in particular, the victims with direct exposure tend to reduce their education expenditure significantly 1 year after the earthquake. This decrease might be due to educational scholarships for earthquake victims, from elementary to tertiary education, as well as assistance from Hiroshima University, Kyoto Sangyo University, and others. This education aid is associated with the decrease in household expenditure since 100 individuals in Bantul in 2007 aged 35 or under. If we assume that they got married at 20–25 years old, thus their children were 10–15 years at the event in which they were at school age. With the scholarship, the household may replace the allocation for education with the consumption of goods and services, such as clothing and household furnishing.
On the contrary, Karim and Noy [28] find that poor households tend to reduce their consumption for education and health when a disaster occurs. It is intended to facilitate their food consumption. A decrease in investment in human capital [4] or the diversion of education consumption to other consumptions might cause the households to be trapped in poverty for a long period [4, 28].
Furthermore, the analysis of the earthquake's impact on mental disorders 8 years after the 2006 earthquake and 4 years after the 2010 Merapi eruption shows that the treatment group had higher mental disorders score on average than the comparison group, but the difference was not significant. It indicates that previous disaster experiences might give a detrimental addictive effect that subsequently may harm the victims [21] and become a factor in generating stress [9] so that the victims of previous disaster will be more sensitive when hearing disasters recur. This insignificant difference, however, confirms that the previous disasters experience apparently was not sufficient to generate the stress of the 2006 earthquake victims back when they faced direct exposure (by media or others) of the 2010 Merapi eruption. This study has considered the possibility of migration of the 2006 Yogyakarta earthquake victims in Bantul to Sleman (location of the 2010 Merapi eruption), in order to observe the impact of direct exposure to repeated disasters. But, the impact of direct exposure could not be analysed subsequently as the number of victims who migrated from Bantul to Sleman was less (based on existing data).
An insignificant impact was also found on per capita household expenditure 8 years after the 2006 earthquake and 4 years after the 2010 Merapi eruption. On average, per capita household expenditure in treatment group was lower than the comparison group. Then, age and marital status were the control variables that significantly influenced the mental disorder score 1 and 8 years after the 2006 earthquake. Individuals with young age belong to the prone-mental health group caused by exposure to disasters [19, 23]. Emotional and psychological recovery for the younger group is more complicated than the older group due to different levels of social networks and previous disaster experiences [29]. Those who are married are classified as the stronger group in dealing with disasters than those who are not married. It dues to the fact that they can share the hardship in the aftermath of disaster with their partners and do not face it alone so that the negative impact of mental health dwindles.
The control variables that significantly affected per capita household expenditure 1 and 8 years after the 2006 earthquake were age, gender, and years of education. As people get older, they will have more necessities so that their expenditures are higher than the younger ones. The higher level of education also affects the higher expenditure since higher education means the higher income they earn, which eventually affects the increase of lifestyle. Women are confirmed have higher expenditure than men due to the different lifestyles between women and men.
5 Concluding remarks
5.1 Conclusion
By considering the analysis and discussion above, certain conclusions can be drawn. First, direct exposure to the 2006 Yogyakarta earthquake only significantly increased the mental disorder score of victims, but this increase did not cause the victims to develop significant depression symptoms 1 year after the earthquake. Second, direct exposure to the 2006 Yogyakarta earthquake decreased the average per capita household expenditure as a whole. After 1 year of the disaster, the victims with direct exposure tended to reduce their education expenditures significantly and divert them to the consumption of goods and services, such as clothing and household furnishing. In addition, after 8 years of the 2006 earthquake, the individuals with direct exposure still possibly faced economic problems dealing with the increase of mental disorders and the loss of productive assets which compounded the low per capita household expenditure. Third, previous disaster experiences possibly give a detrimental addictive effect that subsequently may harm the victims and become a factor in generating stress so that the victims of previous disasters will be more sensitive when hearing disasters recur. However, a significant relationship between previous disaster experience and generating the stress of the 2006 earthquake victims back when they faced direct exposure (by media or others) of the 2010 Merapi eruption was not found.
5.2 Implication
Treatment of psychological problems, such as psychological assistance and rehabilitation, must be designed appropriately. It is also necessary to set priority treatment for young victims. Certain assessments and periodic rehabilitation should be implemented until mental disorders symptoms are tackled based on the assessment results so that the possibility of people generating stress back when facing direct exposure to disasters might be very minimum. Furthermore, education aids for victims should be a priority when facing a disaster because there is a possibility that household expenditure for human capital will be diverted to other expenditures, such as clothing and household furnishings.
5.3 Research limitation
There are several limitations of this study. First, mental health was assessed by using the CESD-10 questionnaire which only explained the depression symptoms, not PTSD symptoms which was the appropriate one concerning the impact of disaster exposure. Second, different questions about mental health among the 3, 4, and 5 waves had compounded several adjustments in questions and scores which caused measurement errors. Third, direct exposure to an earthquake did not distinguish the loss of lives and goods or assets whereas different impacts from these two things might exist. Fourth, this study did not observe the impact of direct exposure toward numerous food expenditures, such as meat, vegetables and others. Finally, the sample used in this study focuses on adults.
5.4 Future direction
Based on these limitations, we suggest future research to use PTSD as the outcome of mental disorders caused by earthquakes. Second, future research can divide direct exposure into two types: loss of life and loss of objects or property. Third, food expenditure can be divided into smaller categories, such as meat and vegetables, in order to minimize heterogeneity, Finally, future research can concentrate more on analysing the earthquake's impact on children, who are the most vulnerable group in experiencing mental health disorders.
Data availability
The data that support the findings of this study are available from the corresponding author upon request.
References
Adler D. Job performance deficits due to depression. Am J Psychiatry. 2006;163(9):1569. https://doi.org/10.1176/appi.ajp.163.9.1569.
Andersen EM, Malmgren JA, Carter WB, Patrick DL. Screening for depression in well older adults: evaluation of a short form of the CES-D. Am J Prev Med. 1994;10(2):1–8.
Arouri M, Nguyen C, Youssef AB. Natural disasters, household welfare, and resilience: evidence from rural Vietnam. World Dev. 2015;70:59–77. https://doi.org/10.1016/j.worlddev.2014.12.017.
Baez JE, Santos IV. On shaky ground: the effects of earthquakes on household income and poverty. New York: UNDP; 2008.
Bappenas. Preliminary damage and loss assessment: Yogyakarta and central java natural disaster. Washington: World Bank Publication; 2006.
Bappenas. Laporan Pemantauan dan Evaluasi Dua Tahun Pelaksanaan Rehabilitasi dan Rekonstruksi Pascabencana Gempa Bumi 27 Mei di Wilayah Provinsi DI Yogyakarta dan Provinsi Jawa Tengah. 2008.
Belasen AR, Polachek SW. How hurricanes affect wages and employment in local labor markets. Am Econ Rev. 2008;98(2):49–53. https://doi.org/10.1257/aer.98.2.49.
Belleville G, Marchand A, St-Hilaire MH, Martin M, Silva C. PTSD and depression following armed robbery: patterns of appearance and impact on absenteeism and use of health care services. J Trauma Stress. 2012;25(4):465–8. https://doi.org/10.1002/jts.21726.
Bland SH, Farinaro E, Jossa F, Trevisan M. Long-term psychological effects of natural disasters. Psychosomatic. 1996;58:18–24.
Bubonya M, Cobb-Clark DA, Wooden M. Mental health and productivity at work: does what you do matter? Labour Econ. 2017;46:150–65. https://doi.org/10.1016/j.labeco.2017.05.001.
Caruso G, Miller S. Long run effects and intergenerational transmission of natural disasters: a case study on the 1970 Ancash earthquake. J Dev Econ. 2015;117:134–50. https://doi.org/10.1016/j.jdeveco.2015.07.012.
Cénat JM, Derivois D. Long-term outcomes among child and adolescent survivors of the 2010 Haitian earthquake. Depress Anxiety. 2015;32(1):57–63. https://doi.org/10.1002/da.22275.
Chen CH, Tan HKL, Liao LR, Chen HH, Chan CC, Cheng JJS, Chen CY, Wang TN, Lu ML. Long-term psychological outcome of 1999 Taiwan earthquake survivors: a survey of a high-risk sample with property damage. Compr Psychiatry. 2007;48(3):269–75. https://doi.org/10.1016/j.comppsych.2006.12.003.
Cueto LJ, Agaton CB. Pandemic and typhoon: positive impacts of a double disaster on mental health of female students in the Philippines. Behav Sci. 2021. https://doi.org/10.3390/bs11050064.
Dwidiyanti M, Hadi I, Wiguna RI, Eka H, Ningsih W. Gambaran Risiko Gangguan Jiwa pada Korban Bencana Alam Gempa di Lombok Nusa Tenggara Barat. J Holistic Nurs Health Sci. 2018;1(2):82. https://doi.org/10.14710/hnhs.1.2.2018.82-91.
Easterlin RA. Does economic growth improve the human lot? Cambridge: Academic Press; 1974.
Feder A, Ahmad S, Lee EJ, Morgan JE, Singh R, Smith BW, Southwick SM, Charney DS. Coping and PTSD symptoms in Pakistani earthquake survivors: purpose in life, religious coping and social support. J Affect Disord. 2013;147(1–3):156–63. https://doi.org/10.1016/j.jad.2012.10.027.
Ferguson CJ. An effect size primer: a guide for clinicians and researchers. Prof Psychol Res Pract. 2009;40(5):532–8. https://doi.org/10.1037/a0015808.
Frankenberg E, Friedman J, Gillespie T, Ingwersen N, Pynoos R, Rifai IU, Sikoki B, Steinberg A, Sumantri C, Suriastini W, Thomas D. Mental health in Sumatra after the tsunami. Am J Public Health. 2008;98(9):1671–7. https://doi.org/10.2105/AJPH.2007.120915.
Garfin DR, Holman EA, Silver RC. Cumulative exposure to prior collective trauma and acute stress responses to the Boston marathon bombings. Psychol Sci. 2015;26(6):675–83. https://doi.org/10.1177/0956797614561043.
Geng F, Zhou Y, Liang Y, Fan F. A longitudinal study of recurrent experience of earthquake and mental health problems among Chinese adolescents. Front Psychol. 2018. https://doi.org/10.3389/fpsyg.2018.01259.
Gignoux J, Menéndez M. Benefit in the wake of disaster: long-run effects of earthquakes on welfare in rural Indonesia. J Dev Econ. 2016;118:26–44. https://doi.org/10.1016/j.jdeveco.2015.08.004.
Gissurardóttir ÓS, Hlodversdóttir H, Thordardóttir EB, Pétursdóttir G, Hauksdóttir A. Mental health effects following the eruption in Eyjafjallajökull volcano in Iceland: a population-based study. Scand J Public Health. 2019;47(2):251–9. https://doi.org/10.1177/1403494817751327.
Guo J, He H, Qu Z, Wang X, Liu C. Post-traumatic stress disorder and depression among adult survivors 8 years after the 2008 Wenchuan earthquake in China. J Affect Disord. 2017;210:27–34. https://doi.org/10.1016/j.jad.2016.12.009.
Hamama-Raz Y, Palgi Y, Leshem E, Ben-Ezra M, Lavenda O. Typhoon survivors’ subjective wellbeing—a different view of responses to natural disaster. PLoS ONE. 2017. https://doi.org/10.1371/journal.pone.0184327.
Hlodversdottir H, Thorsteinsdottir H, Thordardottir EB, Njardvik U, Petursdottir G, Hauksdottir A. La salud a largo plazo de los niños después de la erupción volcánica del Eyjafjallajökull—Un estudio prospectivo de cohorte prospectivo. Eur J Psychotraumatol. 2018. https://doi.org/10.1080/20008198.2018.1442601.
Karim A. The household response to persistent natural disasters: evidence from Bangladesh. World Dev. 2018;103:40–59. https://doi.org/10.1016/j.worlddev.2017.10.026.
Karim A, Noy I. Poverty and natural disasters: a regression meta-analysis. Rev Econ Instit. 2016;7(2):26. https://doi.org/10.5202/rei.v7i2.222.
Kato H, Asukai N, Miyake Y, Minakawa K, Nishiyama A. Post-traumatic symptoms among younger and elderly evacuees in the early stages following the 1995 Hanshin-Awaji earthquake in Japan. Acta Psychiatr Scand. 1996;93(6):477–81. https://doi.org/10.1111/j.1600-0447.1996.tb10680.x.
Khandker SR, Koolwal GB, Samad HA. Handbook on impact evaluation: quantitative methods and practices. Washington: World Bank Publication; 2010.
Kirchberger M. Natural disasters and labor markets. J Dev Econ. 2017;125:40–58. https://doi.org/10.1016/j.jdeveco.2016.11.002.
Kokai M, Fujii S, Shinfuku N, Edwards G. Natural disaster and mental health in Asia. Psychiatry Clin Neurosci. 2004. https://doi.org/10.1111/j.1440-1819.2003.01203.x.
Koplewicz HS, Cloitre M, McClough J, Gurian A, Kamboukos D, Levine E, Pearlman M, Wasser R. Caring for kids after trauma, disaster and death: a guide for parents and professionals. New York: New York University Child Study Center; 2006.
Leppold C, Gibbs L, Block K, Reifels L, Quinn P. Public health implications of multiple disaster exposures. Lancet Public Health. 2022;7(3):e274–86. https://doi.org/10.1016/S2468-2667(21)00255-3.
Liang Y, Cheng J, Ruzek JI, Liu Z. Posttraumatic stress disorder following the 2008 Wenchuan earthquake: a 10-year systematic review among highly exposed populations in China. J Affect Dis. 2019;243:327–39. https://doi.org/10.1016/j.jad.2018.09.047.
Lindert J, Jakubauskiene M, Bilsen J. The covid-19 disaster and mental health-assessing, responding and recovering. Eur J Public Health. 2021;31:IV31–5. https://doi.org/10.1093/eurpub/ckab153.
Masykur AM. Potret Psikososial Korban Gempa 27 Mei 2006 (Sebuah Studi Kualitatif di Kecamatan Wedi dan Gantiwarno, Klaten). J Psikologi Universitas Diponegoro. 2006;3(1):36–44.
Norris FH, Murrell SA. Prior experience as a moderator of disaster impact on anxiety symptoms in older adults 1. Am J Community Psychol. 1988;16(5):665–83. https://doi.org/10.1007/BF00930020.
Seery MD, Holman EA, Silver RC. Whatever does not kill us: cumulative lifetime adversity, vulnerability, and resilience. J Pers Soc Psychol. 2010;99(6):1025–41. https://doi.org/10.1037/a0021344.
Silver RC, Holman EA, Andersen JP, Poulin M, McIntosh DN, Gil-Rivas V. Mental- and physical-health effects of acute exposure to media images of the September 11, 2001, attacks and the Iraq War. Psychol Sci. 2013;24(9):1623–34. https://doi.org/10.1177/0956797612460406.
Sulistyaningrum E. The impact of earthquake on child test score. J Indones Econ Bus. 2017;32(2):104–20.
Acknowledgements
Not applicable.
Funding
This paper does not receive any research funding.
Author information
Authors and Affiliations
Contributions
All authors have contributed equally to designing the research, the process of data collection and calculation, and drafting and revision of the manuscript. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study is not submitted to an ethics committee as it employs secondary data from Indonesian Family Life Survey.
Informed consent
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix
Appendix
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Trisilia, M.S., Sugiyanto, C. & Rifa’i, A. Impact of natural disasters on mental health and welfare: the case of the 2006 Yogyakarta earthquake. Discov Psychol 4, 7 (2024). https://doi.org/10.1007/s44202-023-00112-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s44202-023-00112-3