
Abstract
Popular culture and medical lore have long postulated a connection between full moon and exacerbations of psychiatric disorders. We wanted to empirically analyze the hypothesis that suicides are increased during the period around full moons. We analyzed pre-COVID suicides from the Marion County Coroner’s Office (n = 776), and show that deaths by suicide are significantly increased during the week of the full moon (p = 0.037), with older individuals (age ≥ 55) showing a stronger effect (p = 0.019). We also examined in our dataset which hour of the day (3–4 pm, p = 0.035), and which month of the year (September, p = 0.09) show the most deaths by suicide. We had blood samples on a subset of the subjects (n = 45), which enabled us to look at possible molecular mechanisms. We tested a list of top blood biomarkers for suicidality (n = 154) from previous studies of ours 7, to assess which of them are predictive. The biomarkers for suicidality that are predictive of death by suicide during full moon, peak hour of day, and peak month of year, respectively, compared to outside of those periods, appear to be enriched in circadian clock genes. For full moon it is AHCYL2, ACSM3, AK2, and RBM3. For peak hour it is GSK3B, AK2, and PRKCB. For peak month it is TBL1XR1 and PRKCI. Half of these genes are modulated in expression by lithium and by valproate in opposite direction to suicidality, and all of them are modulated by depression and alcohol in the same direction as suicidality. These data suggest that there are temporal effects on suicidality, possibly mediated by biological clocks, pointing to changes in ambient light (timing and intensity) as a therapeutically addressable target to decrease suicidality, that can be coupled with psychiatric pharmacological and addiction treatment preventive interventions.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
“It is the very error of the moon:
She comes more nearer earth than she was wont,
And makes men mad.”
-. William Shakespeare
Full moon periods have historically and anecdotally been associated with mental illness and its exacerbations. Previous evidence has been mixed. A review study looking at a broad range of psychiatric behaviors (psychosis related admissions, suicide attempts, ER visits, and other indicators of psychiatric illness), found that these “abnormal behaviors” occurred at a greater frequency during the New Moon and Full Moon periods [1]. There has also been work that has shown the impact of the lunar phases on those diagnosed with bipolar disorder [2,3,4,5]. For example, subjects with rapid-cycling bipolar seemed to entrain on lunar cycles (noting potential for both the moon’s luminance and gravitational tidal cycles having impacts) [2, 5]. Clinically, it is known that those suffering from bipolar disorder typically struggle in regards to both seasonal and circadian rhythms, as well as the fact that age of onset of bipolar disorder varies based on distance from the equator [4]. In regards to suicide it has been shown that the variability and amount of total sunlight throughout the year can impact suicide rate in those with bipolar disorder, and those who experience large variations throughout the year in regards to sun exposure are at elevated risk for suicide [3]. This highlights that in addition to the impact of lunar cycles as noted above, seasonality, geography, and overall sun exposure seem to have relationship with psychiatric diseases. Additionally, although a Finnish study in 2021 showed lack of evidence for a broad relationship between suicidality and moon phase, there was shown to be a statistically significant correlation between suicide and the full moon, and further analysis revealed a peak of incidence of suicide during full moons during the winter for pre-menopausal women [6]. This highlights the fact that in conjunction with consideration of lunar phase, seasonal effect should be considered as well, as was mentioned earlier.
We wanted to examine empirically if the above effects of full moon on suicides are true. We also examined empirically other potential temporal effects, such as peak time of day and peak month of year. For that, we studied a pre-COVID cohort of suicide completers from an urban coroner’s office. We also conducted molecular blood biomarkers analyses on a subset of the subjects on which we had blood samples.
2 Materials and methods
2.1 Cohort
Marion County Coroner’s Office cases of deaths by suicide from January 1, 2012 to December 17, 2016 were collected from coroners log books and files. As these were post-mortem cases, the need for an active IRB protocol and informed consent for these cases was waived by the Indiana University IRB. The log books contained the date of death (or date found), case number, preliminary manner of death, name, age, sex, and race along with the name of the responding deputy coroner. If there was a question regarding the manner of death, the case numbers were marked and checked by a Deputy Coroner using their database. All data was entered into a spreadsheet in a de-identified fashion. In all, there were 210 completed suicides over a period of 626 days within the week of the full moon and 566 suicides over a period of 2006 days outside the week of the full moon. Completed suicides involving individuals aged 30 years and younger (n = 208) and 55 years and older (n = 232) were also analyzed separately (Table S1).
A subset of cases had blood samples collected as part of our INBRAIN initiative (Indiana Center for Biomarker Research in Neuropsychiatry) (Supplementary Table S2). We required a last observed alive postmortem interval of 24 h or less, and the cases selected had completed suicide by means other than overdose, which could affect gene expression. The 45 total samples consisted of 38 male and 7 female violent suicide completers (Table S1). 31 participants completed suicide by gunshot to head or chest, 12 by asphyxiation, 1 by slit wrist, and 1 by electrocution. Next of kin signed informed consent at the coroner’s office for donation of blood for research. We collected whole blood (10 ml) in two RNA-stabilizing PAXgene tubes, labeled with an anonymized ID number, and stored at −80 °C in a locked freezer until the time of future processing. Whole-blood RNA was extracted for microarray gene expression studies from the PAXgene tubes, as previously described [7].
2.2 Clock gene analysis
We annotated the suicide biomarker genes for involvement in the circadian clock. We compiled a database of genes associated with circadian function, by using a combination of review papers [8, 9] and searches of existing databases CircaDB (http://circadb.hogeneschlab.org), GeneCards (http://www.genecards.org), and GenAtlas (http://genatlas.medecine.univ-paris5.fr). Using the data we compiled from these sources we identified a total of 1468 genes that show circadian functioning. Using an estimate of about 21,000 genes in the human genome, that gives about 7% of genes having some circadian pattern. We further classified genes into “core” clock genes, i.e. those genes that are the main engine driving circadian function (n = 18), “immediate” clock genes, i.e. the genes that directly input or output to the core clock (n = 331), and “distant” clock genes, i.e. genes that directly input or output to the immediate clock genes (n = 1,119). Out of our 154 top biomarker genes [7], 18 had circadian evidence (11.7%) suggesting a 1.7 fold enrichment for circadian genes.
2.3 Literature databases search
Databases. We have established in our laboratory (Laboratory of Neurophenomics, www.neurophenomics.info) manually curated databases of the human gene expression/protein expression studies (postmortem brain, peripheral tissue/fluids: CSF, blood and cell cultures), human genetic studies (association, copy number variations and linkage), and animal model gene expression and genetic studies, published to date on psychiatric disorders. Only findings deemed significant in the primary publication, by the study authors, using their particular experimental design and thresholds, are included in our databases. Our databases include only primary literature data and do not include review papers or other secondary data integration analyses to avoid redundancy and circularity. These large and constantly updated databases have been used in our CFG cross validation and prioritization platform. For this study, data from papers on suicide were used for the primary analyses (Table 1), and on other disorders for co-morbidity analyses (Table S3).
2.4 Predicting temporal windows (full mood, peak hour of day, peak month of year)
The cohort (n = 45) for predicting temporal windows had whole-genome Affymetrix gene expression data [7] that was RMA normalized by gender. Predictions were performed using R-studio. A list of 154 top biomarkers for suicidality [7] was used. Receiver-operating characteristic (ROC) analyses were carried out between temporal window and outside of the temporal window. We used the pROC function of the R studio.
3 Results
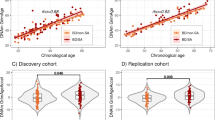
3.1 Phenomenology (Fig. 1)

Phenomics and Genomics. A,C, E. Phenomenological data during the peak time periods. T-tests and standard error of mean (SEM). B, D, F. Gene expression data during the peak time periods. Data in normalized (Z-scored) by gender. The genes whose expression is depicted are the clock genes from Table 1. Clock genes are enriched above baseline among the suicidality biomarkers that are significantly predictive of the peak time periods
Suicides deaths were increased during the week of the full moon (p = 0. 037), in particular in over 55 years old (p = 0.019). There was no statistically significant increase in under 30 years old (p = 0.132).
The peak hour of the day for suicides was 3 to 4 pm (p = 0.035). The peak month was September in all, with July being the peak month in over 55 years old and November being the peak month in under 30 years old. None of these reached statistical significance.
3.2 Genomics (Fig. 1 and Table 1)
Clock genes were enriched among suicidality biomarkers that were predictors of the temporal windows (Table 1), compared to the baselines of 7% of clock genes in the genome, and 11.7% of clock genes among the top suicidality biomarkers [7].
3.3 Co-morbidity, treatments, and biological roles (Table 2 and Table S4)
Depression and alcoholism were the top co-morbid disorders, lithium and valproate the top treatments, and Wnt and Errb signaling were the top biological pathways.
4 Discussion
An increase in suicides during the full moon could be due to the moonlight affecting vulnerable individuals at a time when there should be dark. Consistent with that, circadian clock genes are enriched for predicting this temporal interval. Moreover, the age differential may be consistent as well. For this data, primarily from prior to 2016, the nighttime exposure to light is arguably lower in those over 55 years old, as they were using less cell phones and going to sleep earlier than those under 30 years old. As such, the abnormal light from a full moon may be perceived by them more strongly, whereas it would be drowned by other sources of ambient light in the younger individuals.
The peak of suicides at 3–4 pm is intriguing, and again could have psycho-social and biological reasons. The psycho-social reasons may include day of event stressors such as work events triggering people to leave work early and complete suicides, at a time when they are alone at home. The biological reasons may be circadian clock related, with a decrease in light starting to occur at that time of day and a lower expression of circadian clock genes, as well as cortisol. Indeed, a decrease in gene expression of the clock genes GSK3B, AK2 and PRKCB was predictive in our data (Table 1).
The peak for suicides during September, incidentally, coinciding with Suicide Prevention Month, may be due as well to psycho-social and biological reasons. The psycho-social reasons may have to do with summer vacations being over, and work and school restarting, which may place stress on vulnerable individuals. The biological reasons may be circadian clock related seasonal affective disorder effects, with a decrease in daylight occurring at that time of year. Psycho-socially, the peaks in July for over 55 years old and in November for under 30 years old may be due to US holidays without or with relatives differentially affecting these age groups. Biologically, the increase daylight in July may give older people the energy to do something, and the decreased daylight in November may make younger people sad (they have in general sufficient energy at that age to do something regardless of time of year).
Previous work by us and others has shown that circadian clock abnormalities are related to mood disorders [9,10,11,12,13], and sleep abnormalities have been implicated in suicide [14]. The enrichment in, and putative involvement of, circadian clock genes in death by suicide in the peak temporal windows provides insights and opens the door to therapeutic interventions, whether chronobiological or pharmacological. The co-morbidity with depression and alcoholism may help in building a risk profile, and it is noted that lithium and valproate may be suitable drugs to prevent suicides during peak temporal risk times and beyond (Table 2).
In conclusion, our work is supportive of the full moon, fall season, and late afternoon being temporal windows of increased risk for suicide, where vigilance and preventive measures are warranted, particularly in individuals who suffer from depression and/or alcohol use disorders.
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Templer DI, Veleber DM. The moon and madness: a comprehensive perspective. J Clin Psychol. 1980;36(4):865–8.
Wehr TA. Bipolar mood cycles and lunar tidal cycles. Mol Psychiatry. 2018;23(4):923–31.
Bauer M, Glenn T, Alda M, Andreassen OA, Angelopoulos E, Ardau R, et al. Association between solar insolation and a history of suicide attempts in bipolar I disorder. J Psychiatr Res. 2019;113:1–9.
McCarty R, Josephs T, Kovtun O, Rosenthal SJ. Enlightened: addressing circadian and seasonal changes in photoperiod in animal models of bipolar disorder. Transl Psychiatry. 2021;11(1):373.
Wehr TA, Helferich-Forster C. Correction referring to: Longitudinal observations call into question the scientific consensus that humans are unaffected by lunar cycles. BioEssays. 2021;43(8):e2170083.
Meyer-Rochow VB, Hakko T, Hakko H, Riipinen P, Timonen M. Synodic lunar phases and suicide: based on 2605 suicides over 23 years, a full moon peak is apparent in premenopausal women from northern Finland. Mol Psychiatry. 2021;26(9):5071–8.
Niculescu AB, Le-Niculescu H, Levey DF, Phalen PL, Dainton HL, Roseberry K, et al. Precision medicine for suicidality: from universality to subtypes and personalization. Mol Psychiatry. 2017;22(9):1250–73.
Zhang EE, Liu AC, Hirota T, Miraglia LJ, Welch G, Pongsawakul PY, et al. A genome-wide RNAi screen for modifiers of the circadian clock in human cells. Cell. 2009;139(1):199–210.
McCarthy MJ, Welsh DK. Cellular circadian clocks in mood disorders. J Biol Rhythms. 2012;27(5):339–52.
Le-Niculescu H, Roseberry K, Gill SS, Levey DF, Phalen PL, Mullen J, et al. Precision medicine for mood disorders: objective assessment, risk prediction, pharmacogenomics, and repurposed drugs. Mol Psychiatry. 2021;26(7):2776–804.
Le-Niculescu H, McFarland MJ, Ogden CA, Balaraman Y, Patel S, Tan J, et al. Phenomic, convergent functional genomic, and biomarker studies in a stress-reactive genetic animal model of bipolar disorder and co-morbid alcoholism. Am J Med Genet B Neuropsychiatr Genet. 2008;147B(2):134–66.
Niculescu AB 3rd, Segal DS, Kuczenski R, Barrett T, Hauger RL, Kelsoe JR. Identifying a series of candidate genes for mania and psychosis: a convergent functional genomics approach. Physiol Genomics. 2000;4(1):83–91.
McGrath CL, Glatt SJ, Sklar P, Le-Niculescu H, Kuczenski R, Doyle AE, et al. Evidence for genetic association of RORB with bipolar disorder. BMC Psychiatry. 2009;9:70.
Goodwin RD, Marusic A. Association between short sleep and suicidal ideation and suicide attempt among adults in the general population. Sleep. 2008;31(8):1097–101.
Sequeira A, Morgan L, Walsh DM, Cartagena PM, Choudary P, Li J, et al. Gene expression changes in the prefrontal cortex, anterior cingulate cortex and nucleus accumbens of mood disorders subjects that committed suicide. PLoS ONE. 2012;7(4):e35367.
Labonte B, Suderman M, Maussion G, Lopez JP, Navarro-Sanchez L, Yerko V, et al. Genome-wide methylation changes in the brains of suicide completers. Am J Psychiatry. 2013;170(5):511–20.
Cabrera-Mendoza B, Fresno C, Monroy-Jaramillo N, Fries GR, Walss-Bass C, Glahn DC, et al. Sex differences in brain gene expression among suicide completers. J Affect Disord. 2020;267:67–77.
Pisanu C, Merkouri Papadima E, Melis C, Congiu D, Loizedda A, Orru N, et al. Whole genome expression analyses of miRNAs and mRNAs suggest the involvement of miR-320a and miR-155–3p and their targeted genes in lithium response in bipolar disorder. Int J Mol Sci. 2019;20(23):6040.
Hagihara H, Ohira K, Miyakawa T. Transcriptomic evidence for immaturity induced by antidepressant fluoxetine in the hippocampus and prefrontal cortex. Neuropsychopharmacol Rep. 2019;39(2):78–89.
Ogden CA, Rich ME, Schork NJ, Paulus MP, Geyer MA, Lohr JB, et al. Candidate genes, pathways and mechanisms for bipolar (manic-depressive) and related disorders: an expanded convergent functional genomics approach. Mol Psychiatry. 2004;9(11):1007–29.
Iaccarino HF, Singer AC, Martorell AJ, Rudenko A, Gao F, Gillingham TZ, et al. Gamma frequency entrainment attenuates amyloid load and modifies microglia. Nature. 2016;540(7632):230–5.
Le-Niculescu H, Case NJ, Hulvershorn L, Patel SD, Bowker D, Gupta J, et al. Convergent functional genomic studies of omega-3 fatty acids in stress reactivity, bipolar disorder and alcoholism. Transl Psychiatry. 2011;1:e4.
Cross-Disorder Group of the Psychiatric Genomics C, Lee SH, Ripke S, Neale BM, Faraone SV, Purcell SM, et al. Genetic relationship between five psychiatric disorders estimated from genome-wide SNPs. Nat Genet. 2013;45(9):984–94.
Cook IA, Congdon E, Krantz DE, Hunter AM, Coppola G, Hamilton SP, et al. Time course of changes in peripheral blood gene expression during medication treatment for major depressive disorder. Front Genet. 2019;10:870.
Nagy C, Suderman M, Yang J, Szyf M, Mechawar N, Ernst C, et al. Astrocytic abnormalities and global DNA methylation patterns in depression and suicide. Mol Psychiatry. 2015;20(3):320–8.
Schulpen SH, Pennings JL, Piersma AH. Gene expression regulation and pathway analysis after valproic acid and carbamazepine exposure in a human embryonic stem cell-based neurodevelopmental toxicity assay. Toxicol Sci. 2015;146(2):311–20.
Lee RS, Pirooznia M, Guintivano J, Ly M, Ewald ER, Tamashiro KL, et al. Search for common targets of lithium and valproic acid identifies novel epigenetic effects of lithium on the rat leptin receptor gene. Transl Psychiatry. 2015;5:e600.
Pandey GN, Dwivedi Y, Rizavi HS, Teppen T, Gaszner GL, Roberts RC, et al. GSK-3beta gene expression in human postmortem brain: regional distribution, effects of age and suicide. Neurochem Res. 2009;34(2):274–85.
Ren X, Rizavi HS, Khan MA, Dwivedi Y, Pandey GN. Altered Wnt signalling in the teenage suicide brain: focus on glycogen synthase kinase-3beta and beta-catenin. Int J Neuropsychopharmacol. 2013;16(5):945–55.
Roy B, Wang Q, Palkovits M, Faludi G, Dwivedi Y. Altered miRNA expression network in locus coeruleus of depressed suicide subjects. Sci Rep. 2017;7(1):4387.
Karege F, Perroud N, Burkhardt S, Fernandez R, Ballmann E, La Harpe R, et al. Protein levels of beta-catenin and activation state of glycogen synthase kinase-3beta in major depression. A study with postmortem prefrontal cortex. J Affect Disord. 2012;136(1–2):185–8.
Jimenez E, Arias B, Mitjans M, Goikolea JM, Roda E, Saiz PA, et al. Genetic variability at IMPA2, INPP1 and GSK3beta increases the risk of suicidal behavior in bipolar patients. Eur Neuropsychopharmacol. 2013;23(11):1452–62.
Palmos AB, Duarte RRR, Smeeth DM, Hedges EC, Nixon DF, Thuret S, et al. Lithium treatment and human hippocampal neurogenesis. Transl Psychiatry. 2021;11(1):555.
Breen MS, White CH, Shekhtman T, Lin K, Looney D, Woelk CH, et al. Lithium-responsive genes and gene networks in bipolar disorder patient-derived lymphoblastoid cell lines. Pharmacogenomics J. 2016;16(5):446–53.
Geoffroy PA, Curis E, Courtin C, Moreira J, Morvillers T, Etain B, et al. Lithium response in bipolar disorders and core clock genes expression. World J Biol Psychiatry. 2018;19(8):619–32.
Akkouh IA, Skrede S, Holmgren A, Ersland KM, Hansson L, Bahrami S, et al. Exploring lithium’s transcriptional mechanisms of action in bipolar disorder: a multi-step study. Neuropsychopharmacology. 2020;45(6):947–55.
Xiao Z, Cao Z, Yang J, Jia Z, Du Y, Sun G, et al. Baicalin promotes hippocampal neurogenesis via the Wnt/beta-catenin pathway in a chronic unpredictable mild stress-induced mouse model of depression. Biochem Pharmacol. 2021;190:114594.
Pandey GN, Ren X, Rizavi HS, Dwivedi Y. Glycogen synthase kinase-3beta in the platelets of patients with mood disorders: effect of treatment. J Psychiatr Res. 2010;44(3):143–8.
Jia S, Li B, Huang J, Verkhratsky A, Peng L. Regulation of glycogen content in astrocytes via Cav-1/PTEN/AKT/GSK-3beta pathway by three anti-bipolar drugs. Neurochem Res. 2018;43(8):1692–701.
Foo JC, Trautmann N, Sticht C, Treutlein J, Frank J, Streit F, et al. Longitudinal transcriptome-wide gene expression analysis of sleep deprivation treatment shows involvement of circadian genes and immune pathways. Transl Psychiatry. 2019;9(1):343.
Peng L, Zhang X, Cui X, Zhu D, Wu J, Sun D, et al. Paliperidone protects SK-N-SH cells against glutamate toxicity via Akt1/GSK3beta signaling pathway. Schizophr Res. 2014;157(1–3):120–7.
Fatemi SH, Reutiman TJ, Folsom TD. Chronic psychotropic drug treatment causes differential expression of Reelin signaling system in frontal cortex of rats. Schizophr Res. 2009;111(1–3):138–52.
Peng L, Zhu D, Feng X, Dong H, Yue Q, Zhang J, et al. Paliperidone protects prefrontal cortical neurons from damages caused by MK-801 via Akt1/GSK3beta signaling pathway. Schizophr Res. 2013;147(1):14–23.
Wong P, Sze Y, Chang CC, Lee J, Zhang X. Pregnenolone sulfate normalizes schizophrenia-like behaviors in dopamine transporter knockout mice through the AKT/GSK3beta pathway. Transl Psychiatry. 2015;5:e528.
Benton CS, Miller BH, Skwerer S, Suzuki O, Schultz LE, Cameron MD, et al. Evaluating genetic markers and neurobiochemical analytes for fluoxetine response using a panel of mouse inbred strains. Psychopharmacology. 2012;221(2):297–315.
Cabrera B, Monroy-Jaramillo N, Fries GR, Mendoza-Morales RC, Garcia-Dolores F, Mendoza-Larios A, et al. Brain gene expression pattern of subjects with completed suicide and comorbid substance use disorder. Mol Neuropsychiatry. 2019;5(1):60–73.
Cabrera-Mendoza B, Fresno C, Monroy-Jaramillo N, Fries GR, Walss-Bass C, Glahn DC, et al. Brain gene expression profiling of individuals with dual diagnosis who died by suicide. J Dual Diagn. 2019. https://doi.org/10.1093/schbul/sbaa030.405.
Pandey GN, Dwivedi Y, Rizavi HS, Ren X, Conley RR. Decreased catalytic activity and expression of protein kinase C isozymes in teenage suicide victims: a postmortem brain study. Arch Gen Psychiatry. 2004;61(7):685–93.
Flory JD, Donohue D, Muhie S, Yang R, Miller SA, Hammamieh R, et al. Gene expression associated with suicide attempts in US veterans. Transl Psychiatry. 2017;7(9):e1226.
McQuillin A, Rizig M, Gurling HM. A microarray gene expression study of the molecular pharmacology of lithium carbonate on mouse brain mRNA to understand the neurobiology of mood stabilization and treatment of bipolar affective disorder. Pharmacogenet Genomics. 2007;17(8):605–17.
Youngs RM, Chu MS, Meloni EG, Naydenov A, Carlezon WA Jr, Konradi C. Lithium administration to preadolescent rats causes long-lasting increases in anxiety-like behavior and has molecular consequences. J Neurosci. 2006;26(22):6031–9.
Koehn LM, Huang Y, Habgood MD, Kysenius K, Crouch PJ, Dziegielewska KM, et al. Effects of paracetamol (acetaminophen) on gene expression and permeability properties of the rat placenta and fetal brain. F1000Res. 2020;9:573.
Perlis RH, Huang J, Purcell S, Fava M, Rush AJ, Sullivan PF, et al. Genome-wide association study of suicide attempts in mood disorder patients. Am J Psychiatry. 2010;167(12):1499–507.
Le-Niculescu H, Balaraman Y, Patel S, Tan J, Sidhu K, Jerome RE, et al. Towards understanding the schizophrenia code: an expanded convergent functional genomics approach. Am J Med Genet B Neuropsychiatr Genet. 2007;144B(2):129–58.
Choi K, Le T, Xing G, Johnson LR, Ursano RJ. Analysis of kinase gene expression in the frontal cortex of suicide victims: implications of fear and stress. Front Behav Neurosci. 2011;5:46.
Acknowledgements
We would like to acknowledge the families who have lost loved ones to suicide, and the dedicated staff of the Marion County Coroner’s Office. This work was supported by NIH grants (R01MH117431) to ABN.
Author information
Authors and Affiliations
Contributions
ABN and GES designed the study, and ABN wrote the manuscript. RB, HLN, KR and CD analyzed the data. KK, AB, MY, and GES organized, collected and scored Coroner’s Office data. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
ABN is a co-founder of MindX Sciences.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Bhagar, R., Le-Niculescu, H., Roseberry, K. et al. Temporal effects on death by suicide: empirical evidence and possible molecular correlates. Discov Ment Health 3, 10 (2023). https://doi.org/10.1007/s44192-023-00035-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s44192-023-00035-4