
Abstract
Objective
Frequent users to emergency departments (EDs) are a diverse group of patients accounting for a disproportionate number of ED presentations. This study examined sociodemographic and ED visit characteristics of adult high-system users in two Canadian provinces.
Methods
Cohorts of high-system users were created for Alberta and Ontario including patients with the top 10% of presentations in the National Ambulatory Care Reporting System (April 2015–March 2016). Controls were random samples of non-high-system user patients. Sociodemographic and ED visits data were used to predict high-system user group membership in a multivariable logistic regression model.
Results
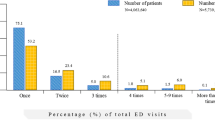
There were 579,674 high-system users and 2,115,960 controls. High-system users were more likely to be female [odds ratio (OR) = 1.1, 95% confidence interval (CI) 1.1,1.1], older (OR 1.02 per 5 years, 95% CI 1.02,1.02), from the lowest-income quintile (OR 1.8, 95% CI 1.7,1.8), and more rural (OR 1.6, 95% CI 1.6,1.6) than controls. High-system users had a higher proportion of presentations by ambulance (OR 1.1 per 0.25 increase, 95% CI 1.1,1.1) and disposition was admission/transfer (OR 1.1 per 0.25 increase, 95% CI 1.1,1.1), left without being seen (OR 1.1, 95% CI 1.1,1.1), or left against medical advice (OR 1.1, 95% CI 1.1,1.1) more often than controls.
Conclusion
High-system users were more likely to be female, older, live in rural areas and within the lowest-income quintile compared to controls. Their heterogeneity in acuity, comorbid chronic diseases, and limited access to primary care suggests that interventions referring high-system users to primary care may be fruitful in reducing ED utilization by high-system users.
Résumé
Objectif
Les utilisateurs fréquents des services d'urgence sont un groupe diversifié de patients qui représentent un nombre disproportionné de présentations aux services d'urgence. Cette étude a examiné les caractéristiques sociodémographiques et les visites aux urgences de grands utilisateurs adultes du système de santé dans deux provinces canadiennes.
Méthode
Des cohortes de grands utilisateurs du système de santé ont été créées pour l'Alberta et l'Ontario, y compris les patients ayant fait l'objet des 10 % de présentations les plus importantes dans le système national d'information sur les soins ambulatoires (avril 2015-mars 2016). Les contrôles étaient des échantillons aléatoires des patients ne faisant pas partie des grands utilisateurs. Les données sociodémographiques et les données sur les visites aux urgences ont été utilisées pour prédire l'appartenance à un groupe de grands utilisateurs du système dans un modèle de régression logistique multivariable.
Résultats
Il y avait 579 674 de grands utilisateurs et 2 115 960 témoins. Les grands utilisateurs de système étaient plus susceptibles d'être des femmes (rapport des cotes [RC] = 1,1, intervalle de confiance à 95 % (IC) 1,1, 1,1), plus âgés (RC = 1,02 tous les 5 ans, IC à 95 % 1,02, 1,02), d'après quintile de revenu le plus bas (RC = 1,8, IC à 95 % 1,7,1,8), et plus rural (RC = 1,6, IC à 95 % 1,6,1,6) que les témoins. Les grands utilisateurs du système avaient une proportion plus élevée de présentations par ambulance (RC = 1,1 pour une augmentation de 0,25, IC à 95 % 1,1, 1,1) et la disposition était l'admission / transfert (RC = 1,1 pour une augmentation de 0,25, IC à 95 % 1,1, 1,1), parti sans être vu (OR = 1,1, IC à 95% 1,1, 1,1), ou parti contre l'avis médical (OR = 1,1, IC à 95 % 1,1, 1,1) plus souvent que les témoins.
Conclusions
Les grands utilisateurs du système étaient plus susceptibles d'être des femmes, des personnes âgées, vivant dans des zones rurales et se situant dans le quintile de revenu le plus bas, par rapport aux témoins. Leur hétérogénéité en termes d'acuité, de comorbidité des maladies chroniques et d'accès limité aux soins primaires suggère que les interventions qui orientent les grands utilisateurs du haut système vers les soins primaires peuvent être fructueuses pour réduire l'utilisation des urgences par les grands utilisateurs du système



Similar content being viewed by others


References
Affleck A, Parks P, Drummond A, Rowe B, Ovens H. Emergency department overcrowding and access block. CJEM. 2013;15(6):59–67.
LaCalle E, Rabin E. Frequent users of emergency departments: the myths, the data, and the policy implications. Ann Emerg Med. 2010;56(1):42–8.
Giannouchos TV, Kum H-C, Foster MJ, Ohsfeldt RL. Characteristics and predictors of adult frequent emergency department users in the United States: a systematic literature review. J Eval Clin Pract. 2019;25(3):420–33.
van Tiel S, Rood PPM, Bertoli-Avella AM, Erasmus V, Haagsma J, van Beeck E, et al. Systematic review of frequent users of emergency departments in non-US hospitals: state of the art. Eur J Emerg Med. 2015;22(5):306–15.
Burns TR. Contributing factors of frequent use of the emergency department: a synthesis. Int Emerg Nurs. 2017;35:51–5.
Chan BTB, Ovens HJ. Frequent users of emergency departments. Do they also use family physicians’ services? Can Fam Physician. 2002;48:1654–60.
Doupe MB, Palatnick W, Day S, Chateau D, Soodeen R-A, Burchill C, et al. Frequent users of emergency departments: developing standard definitions and defining prominent risk factors. Ann Emerg Med. 2012;60(1):24–32.
Gaulin M, Simard M, Candas B, Lesage A, Sirois C. Combined impacts of multimorbidity and mental disorders on frequent emergency department visits: a retrospective cohort study in Quebec, Canada. CMAJ. 2019;191(26):E724–32.
Geurts J, Palatnick W, Strome T, Sutherland KA, Weldon E. Frequent users of an inner-city emergency department. CJEM. 2012;14(5):303–13.
Palmer E, Leblanc-Duchin D, Murray J, Atkinson P. Emergency department use: is frequent use associated with a lack of primary care provider? Can Fam Physician. 2014;60:e223–9.
Rowe BH, Bond K, Ospina MB, Blitz S, Friesen C, Schull M, et al. Emergency department overcrowding in Canada: what are the issues and what can be done? [Technology overview no 21]. Ottawa: Canadian Agency for Drugs and Technologies in Health; 2006.
Rowe BH, McRae A, Rosychuk RJ. Temporal trends in emergency department volumes and crowding metrics in a western Canadian province: a population-based, administrative data study. BMC Health Serv Res. 2020;20:356.
Morley C, Unwin M, Peterson GM, Stankovich J, Kinsman L. Emergency department crowding: a systematic review of causes, consequences and solutions. PLoS One. 2018;13(8):e0203316.
Canadian Institutes of Health Research, Canadian Institute for Health Information. Dynamic Cohort of Complex, High System Users—2011–2015: A CIHR-CIHI Collaboration. Ottawa, ON: Canadian Institutes of Health Research and Canadian Institute for Health Information; 2017.
Canadian Institute for Health Information. National Ambulatory Care Reporting System (NACRS). Ottawa, ON: Canadian Institute for Health Information.
Canadian Institute for Health Information. Data Quality Documentation, National Ambulatory Care Reporting System—Current-Year Information, 2015–2016. https://www.cihi.ca/sites/default/files/document/nacrs-dataquality_2015-2016_en.pdf. Ottawa, ON: Canadian Institute for Health Information; 2016.
Canadian Institute for Health Information. National Ambulatory Care Reporting System Open-Year Data Quality Test Specifications, 2017–2018. https://www.cihi.ca/sites/default/files/document/nacrs-2017-2018-oydq-specs.pdf. Ottawa, ON: Canadian Institute for Health Information; 2017.
Bullard MJ, Unger B, Spence J, Grafstein E, CTAS National Working Group. Revisions to the Canadian Emergency Department Triage and Acuity Scale (CTAS) adult guidelines. CJEM. 2008;10(2):136–51.
Canadian Institute for Health Information. The Canadian Enhancement of ICD-10 (International Statistical Classification of Diseases and Related Health Problems, Tenth Revision). Ottawa: Canadian Institute for Health Information; 2001.
Quan H, Sundararajan V, Halfon P, Fong A, Burnand B, Luthi J-C, et al. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med Care. 2005;43(11):1130–9.
Guttmann A, Schull MJ, Vermeulen MJ, Stukel TA. Association between waiting times and short term mortality and hospital admission after departure from emergency department: population based cohort study from Ontario. Canada. BMJ. 2011;342:d2983.
Sanmartin C, Khan S, LHAD Research Team. Hospitalizations for Ambulatory Care Sensitive Conditions (ACSC): the factors that matter. Ottawa: Statistics Canada; 2011.
Statistics Canada. Postal Codes Conversion File (PCCF), Reference Guide, May 2011 Postal Codes. Statistics Canada Catalogue no. 92-153-G. Ottawa; 2011.
Moe J, Kirkland S, Ospina MB, Campbell S, Long R, Davidson A, et al. Mortality, admission rates and outpatient use among frequent users of emergency departments: a systematic review. Emerg Med J. 2016;33(3):230–6.
Oliveira A. Hyperusers and emergency. Acta Med Port. 2009;21(6):6.
Ruger JP, Richter CJ, Spitznagel EL, Lewis LM. Analysis of costs, length of stay, and utilization of emergency department services by frequent users: implications for health policy. Acad Emerg Med. 2004;11(12):1311–7.
Althaus F, Paroz S, Hugli O, Ghali WA, Daeppen J-B, Peytremann-Bridevaux I, et al. Effectiveness of interventions targeting frequent users of emergency departments: a systematic review. Ann Emerg Med. 2011;58(1):41–52.
Acknowledgements
The authors thank Prof. Howard Ovens MD from the University of Toronto for helping to secure grant funding and for insightful comments. The authors thank the Canadian Institute for Health Information for providing health datasets. Parts of this material are based on data and information provided by the Canadian Institute for Health Information. However, the analyses, conclusions, opinions and statements expressed herein are those of the author and not those of the Canadian Institute for Health Information.
Funding
This study was supported by a grant from the Canadian Institutes of Health Research (#394223). The funding source had no direct involvement in the study design, analysis, interpretation or decision to submit this work.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The author declares that there is no competing interest.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Chen, A., Ospina, M., McRae, A. et al. Characteristics of frequent users of emergency departments in Alberta and Ontario, Canada: an administrative data study. Can J Emerg Med 23, 206–213 (2021). https://doi.org/10.1007/s43678-020-00013-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s43678-020-00013-7