
Abstract
Introduction
It is a well-established fact that concomitant diseases can affect the outcome of total hip arthroplasty (THA). Therefore, careful preoperative assessment of a patient's comorbidity burden is a necessity, and it should be a part of routine screening as THA is associated with a significant number of complications. To measure the multimorbidity, dedicated clinical tools are used.
Methods
The article is a systematic review of instruments used to evaluate comorbidities in THA studies. To create a list of available instruments for assessing patient's comorbidities, the search of medical databases (PubMed, Web of Science, Embase) for indices with proven impact on revision risk, adverse events, mortality, or patient's physical functioning was performed by two independent researchers.
Results
The initial search led to identifying 564 articles from which 26 were included in this review. The measurement tools used were: The Charlson Comorbidity Index (18/26), Society of Anesthesiology classification (10/26), Elixhauser Comorbidity Method (6/26), and modified Frailty Index (5/26). The following outcomes were measured: quality of life and physical function (8/26), complications (10/26), mortality (8/26), length of stay (6/26), readmission (5/26), reoperation (2/26), satisfaction (2/26), blood transfusion (2/26), surgery delay or cancelation (1/26), cost of care (1/26), risk of falls (1/26), and use of painkillers (1/26). Further research resulted in a comprehensive list of eleven indices suitable for use in THA outcomes studies.
Conclusion
The comorbidity assessment tools used in THA studies present a high heterogeneity level, and there is no particular system that has been uniformly adopted. This review can serve as a help and an essential guide for researchers in the field.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Total hip arthroplasty (THA) is performed in 200 patients per 100,000 population in Organisation for Economic Cooperation and Development (OECD) countries yearly, which makes it one of the most common orthopedic surgeries [1]. The number of patients undergoing THA is continually increasing, and THA's efficiency is on the rise [2]. One of the causes of increasing effectiveness is a better assessment of a patient's health status to provide more personalized treatment based on their risk factors. According to research, 83.7% of patients undergoing hip surgery suffer from comorbidities [3]. Researchers indicate that concomitant diseases can affect the outcome of THA, including postoperative complications, risk of reoperation, cost of patient's treatment, future mobility of the patient, and outcomes represented by joint-specific measures including: Western and McMaster Universities Osteoarthritis Index (WOMAC), the Hip Disability and Osteoarthritis Outcome Score (HOOS), the Harris Hip Score (HHP), the Oxford Hip Score (OHS) and the Mayo Hip Score (MHS) [4]. Hence, the in-depth evaluation of comorbidities is vital for predicting THA outcomes [5]. The comorbidity index used for clinical practice should have simple computation, and data used for estimating should be easy to obtain. Most comorbidity indices are based on the International Statistical Classification of Diseases and Related Health Problems (ICD-10) coding, which provides better data assembling. ICD-10 codes are also collected in medical databases, which could be helpful for population-based or retrospective studies. Data for creating comorbidity indices could be obtained from a patient's exam, medical history, or prescription data, and the diseases used for estimating comorbidity indices should have a high prevalence and proven impact on THA outcome. There are also attempts to quantify comorbidities' influence by using weights assigned to each comorbidity to provide better risk assessment. Demographic factors such as age, body mass index (BMI) are often included in comorbidity indices [6].
Methods
The systemic search of medical databases Embase, PubMed, and Web of Science was conducted by two independent researcher’s MP and WK. To find the most valuable and recent data, we estimated the following search criteria: articles must be written in English, published between 2016 and 2020, and contain the following keywords: "HIP," "ARTHROPLASTY", "REPLACEMENT" linked with the keyword "COMORBIDITY INDEX" using the operator "AND". Articles in which THA was performed for femoral neck or acetabular fracture were excluded from research using the operator "NOT" and phrase "FRACTURE" in search criteria. Animal studies were also excluded using the operator "NOT" and the phrase "ANIMAL" and "ANIMALS". From the obtained literature collection, initial titles and abstracts selection were performed. The second step was to screen full texts and exclude publications that do not measure comorbidities' impact on THA outcomes and review articles. The last step was to choose publications that discuss the impact of comorbidity in clinical practice, including predicting postoperative complications, adverse events, physical status, quality of life revision rate, length of hospitalization, risk of readmission, and mortality in different periods. Data from the last collection was extracted into Table 1 to present a comprehensive overview of the most recent assessment tools. A search of reference lists of identified articles was performed to identify other relevant studies. This additional search aimed to find other, less often used indices, which could be a valuable tool for patient's health assessment.
Results
The search resulted in the identification of 564 publications suitable for initial criteria. A further selection of the final 26 publications is presented in Fig. 1. In this review, the majority of publications (23/26) were retrospective studies. This systematic review's primary purpose was to find recently used tools for assessing a patient's comorbidity. The investigation revealed the following indices, presented with the frequency of their appearance: The Charlson Comorbidity Index (18/26), Society of Anesthesiology classification (10/26), Elixhauser Comorbidity Method (6/26), and modified Frailty Index (5/26). The following outcomes were measured: quality of life and physical function (8/26), complications (10/26), mortality (8/26), length of stay (6/26), readmission (5/26), reoperation (2/26), satisfaction (2/26), blood transfusion (2/26), surgery delay or cancelation (1/26), cost of care (1/26), risk of falls (1/26), and use of painkillers (1/26). The selected articles are listed in Table 1.

Summary of search and review process
A Further examination of reference lists of 26 identified articles and combining them with systemic research resulted in creating a list of 11 indices suitable for predicting THA's outcome. The background information on the creation of each clinical tool and its essential characteristics is summarized in Table 2. The indices are subdivided into four categories depending on the tool’s scope. The index can be based on diagnosis, medical and demographic factors, prescription data, or general health status. The scoring method can vary between authors for the same clinical tool; in Table 3, the recommended scoring methods are described. Table 4 shows a detailed description of each instrument assessed in this review in the aspect of THA. The clinical conditions rated in each of the comorbidity indices are listed in Table 5. This systematic review revealed high heterogeneity in the methods used to assess THA patients' comorbidity, resulting from a lack of clinical guidelines.
Discussion
The THA is one of the most common surgeries worldwide that 1–3% of patients aged over 65 years will undergo in their lifetime [12]. Due to the high effectiveness in improving patients functioning and quality of life, the procedure was described in 2007 in "The Lancet" as "Operation of the Century" [80]. Currently, the age of patients undergoing THA increases, as is the comorbidity burden [81]. In a systematic review conducted by Buirs et al. [82], 11 out of 13 studies (84.62%) showed a significant negative relationship between comorbidities and postoperative hip function. In another review by Olthof et al. [83], multimorbidity predisposed to the longer hospital stay after THA, and in 8 out of 9 studies, the relationship was statistically significant. In all out of two eligible studies, comorbidities were associated with a higher cost of care. Also, cognitive status and mental health before surgery can affect the functioning after THA. Psychiatric disorders are associated with less satisfactory functional outcomes and less improvement in life quality, pain and satisfaction after surgery, prolonged hospitalization, complications, and increased mortality [84, 85]. Undeniably, the coexisting diseases can impact THA results, both traditional outcomes like mortality, risk of adverse events, or revision, and patient-oriented outcomes such as quality of life, physical function, and satisfaction [4]. Identifying patients at high risk of complications can lead to adequate qualification for the procedure and initiation of more rigorous prophylaxis. On the other hand, low-risk patients could be subjected to fast-track surgery, reducing the length of stay and care-related costs [58]. The current methods used to assess health status among patients qualified for THA are very diverse among the authors, making it difficult to compare individual results in a pooled analysis. This review is intended to facilitate the selection of the appropriate tool and its proper application. Table 6 represents the summary of the strengths and limitations of included comorbidity assessment methods.
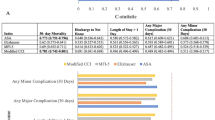
The most commonly used comorbidity measure in THA patients is the ASA classification, and the second one is the CCI. These clinical tools often serve as a reference point for measuring other indices' performance, including mFI and ECM. Both ASA and CCI can successfully predict the THA outcomes such as quality of life, physical function, complications, mortality, length of stay, and hospital readmission. Nevertheless, the ASA classification was more predictive than CCI when indices were compared in terms of adverse events (any, minor and serious), length of stay, and discharge to the higher level facility after THA. The ASA could better reflect patients' health status because of its dynamic assessment of comorbidities, while indices like CCI only note the presence of the disease. The CCI, an objective, diagnose-based measure, has less predictive power than a subjective tool like ASA. However, the ASA class had less discriminative ability than age in all the aforementioned outcomes. The available variants of CCI are presented in Table 7 [12, 57].
The recent publications demonstrate that the ASA score has a good predictive value, but it could present significant discrepancies over time because of its dynamic and subjective nature [12]. That is why other indices like ECM are still under investigation. The ECM is based on ICD codes, which can be acquired from administrative data, unlike the ASA score, collected and assessed prospectively. The ECM is the third most commonly used comorbidity index in THA studies. It outperformed CCI and mFI to predict serious complications, e.g., sepsis, myocardial infarction, bleeding, mortality, mechanical complications, infection, extended length of stay, and discharge to the facility [28]. Also, comparing to ASA, it can be a better predictor of outcome after orthopedic surgery [86]. However, the complexity of 30 variables that could provide a broad perspective of the patient’s preoperative health status could lead to data collection difficulties. Using scores consisting of many variables could provide a situation when comorbidities with different impacts on THA are put on equal. That is why creating appropriate weights was made, but studies do not prove the additional utility of weighted scores [28].
Another example of an index that should also be considered in THA patients is the modified Frailty Index (mFI). With aging, the comorbidities burden increases, catabolic processes exacerbate, and the physiological reserve and resistance to stressors such as surgery declines. This state of organism exhaustion is referred to as frailty. The mFI is used to assess multimorbidity and frailty, and it is available in a version containing eleven components (mFI-11) and in a shortened version consisting of five items ("mFI-5"). Both versions effectively predict increased risk of prolonged hospitalization, complications, and reoperation after THA [61]. Due to its easy estimation, objectivity, and good predictive value of surgery outcomes, mFI is a promising clinical practice tool. It can be obtained retrospectively from medical records ICD coding. Previous studies have shown that mFI is a stronger predictor than age or ASA in predicting the length of hospitalization, complications, reoperation, and mortality after THA [17]. The mFI was recently proven to predict long-term functional outcomes (WOMAC) and length of hospital stay in patients after THA [18].
Other, less frequently used indices deliver a more diverse image of a patient's health status and provide additional predictive value than the beforementioned clinical tools. For example, the Functional Comorbidity Index (FCI) can predict postoperative patients' physical function and quality of life after THA. It includes aspects like obesity or mental status and focuses on physical function limitation. However, its predictive ability does not find reflection in recent studies, and it is not widely used in clinical practice. Moreover, The FCI, compared to CCI, has a worse predicting ability of mortality after THA [27]. Another less-commonly used index is RxRisk-V, a proven predictor of THA outcome with a unique calculation method based on a patient’s prescription data. The RxRisk-V provides good predictive value, as well as easy data collection. However, a medication-based index can lead to misclassifications when one medication is given to cure two comorbid diseases or medicament is given “off label” [42]. The Index of Coexistent Disease (ICED) is an example of an index considering both physical and functional status, but it is rarely used in orthopedic literature [32]. The Cumulative Illness Rating Scale (CIRS) differs from other indices because it rates each separate human body system. It could be a reliable and valid instrument for assessing comorbidity in THA patients. As a fast, objective, and easily quantified index, it is well suited to various research uses. [25]. As well as some lesser-known indices we presented in this review, demographic factors have a significant ability to predict the outcome of THA. Measurement tools like RRATHR and CMS-HCC combine demographic factors like age with comorbidities to create a more comprehensive reflection of a patient's health status. However, RRATHR was found to have no proven predictive value in THA, according to recent literature. Furthermore, their overwhelming complexity excludes them from everyday clinical practice instruments and adjusting care for patients' needs [54].
Studies discussing comorbidity indices' effectiveness highlighted that indices used in everyday practice should remain as easy as possible. Too many factors included in the index could lead to errors and hinder data assembling. Additionally, the index should be legible and straightforward for clinicians to provide a convenient and fast evaluation. That is why ASA and CCI are still widely used even though they do not precisely reflect a patient's health status. In opposition to more specific ones, general indices help assess which patient should receive more intensive peri/postoperative care. Using general indices also avoids the risk of equalizing different conditions in patients with the same comorbid disease [32]. Despite the variety of comorbidity assessment methods and measured outcomes, the majority of recent studies presented in this systemic review confirm the predicting ability of different comorbidity indices and convince that assessing patients' comorbid diseases is vital in clinical practice. This study does not contain all available comorbidity indices like Chronic disease score (CDS), Kaplan Feinstein Classification (KFC), Health-related Quality of Life Comorbidity Index (HRQL-CI) due to their absence in the orthopedic literature [87, 88].
Conclusions
-
1.
The most commonly used comorbidity indices in THA studies are CCI and ASA.
-
2.
Currently, researchers focus not only on mortality and complications but also on the quality of life, function, and patient satisfaction after THA.
-
3.
There is high heterogeneity in the methods used to assess the health status of THA patients.
-
4.
Comorbidity indices should be an integral part of clinical practice because it allows predicting the risk of complications and the THA's functional outcome.
-
5.
Less common comorbidity indices may also prove useful for researchers in THA studies.
References
Pabinger, C., & Geissler, A. (2014). Utilization rates of hip arthroplasty in OECD countries. Osteoarthritis Cartilage, 22(6), 734–741.
Barros, A. A. G., et al. (2017). Efficacy evaluation of a protocol for safe hip surgery (total hip arthroplasty). Revista Brasileira de Ortopedia, 52(Suppl 1), 29–33.
Hustedt, J. W., et al. (2017). Calculating the cost and risk of comorbidities in total joint arthroplasty in the United States. Journal of Arthroplasty, 32(2), 355-361.e1.
Pulik, Ł, et al. (2020). An update on joint-specific outcome measures in total hip replacement. Reumatologia, 58(2), 107–115.
Jain, N. B., et al. (2005). Comorbidities increase complication rates in patients having arthroplasty. Clinical Orthopaedics and Related Research, 435, 232–238.
Soohoo, N. F., et al. (2010). Factors that predict short-term complication rates after total hip arthroplasty. Clinical Orthopaedics and Related Research, 468(9), 2363–2371.
Charlson, M. E., et al. (1987). A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. Journal of Chronic Diseases, 40(5), 373–383.
Voskuijl, T., Hageman, M., & Ring, D. (2014). Higher Charlson Comorbidity Index Scores are associated with readmission after orthopaedic surgery. Clinical Orthopaedics and Related Research, 472(5), 1638–1644.
Sharabiani, M. T., Aylin, P., & Bottle, A. (2012). Systematic review of comorbidity indices for administrative data. Medical Care, 50(12), 1109–1118.
Armitage, J. N., & van der Meulen, J. H. (2010). Identifying co-morbidity in surgical patients using administrative data with the Royal College of Surgeons Charlson Score. British Journal of Surgery, 97(5), 772–781.
Austin, S. R., et al. (2015). Why summary comorbidity measures such as the Charlson Comorbidity Index and Elixhauser Score Work. Medical Care, 53(9), e65-72.
Ondeck, N. T., et al. (2018). Predicting adverse outcomes after total hip arthroplasty: a comparison of demographics, the american society of anesthesiologists class, the modified Charlson Comorbidity Index, and the Modified Frailty Index. The Journal of the American Academy of Orthopaedic Surgeons, 26(20), 735–743.
Menendez, M. E., et al. (2014). The Elixhauser comorbidity method outperforms the Charlson index in predicting inpatient death after orthopaedic surgery. Clinical Orthopaedics and Related Research, 472(9), 2878–2886.
Rockwood, K., et al. (2005). A global clinical measure of fitness and frailty in elderly people. CMAJ, 173(5), 489–495.
Farhat, J. S., et al. (2012). Are the frail destined to fail? Frailty index as predictor of surgical morbidity and mortality in the elderly. The Journal of Trauma and Acute Care Surgery, 72(6), 1526–1530. (discussion 1530–1).
Searle, S. D., et al. (2008). A standard procedure for creating a frailty index. BMC Geriatrics, 8(1), 24.
Bellamy, J. L., et al. (2017). Modified Frailty Index is an effective risk assessment tool in primary total hip arthroplasty. Journal of Arthroplasty, 32(10), 2963–2968.
Pulik, Ł, et al. (2020). Modified frailty index as a predictor of the long-term functional result in patients undergoing primary total hip arthroplasty. Reumatologia, 58(4), 213–220.
Elixhauser, A., et al. (1998). Comorbidity measures for use with administrative data. Medical Care, 36(1), 8–27.
Greene, M. E., et al. (2015). Standard comorbidity measures do not predict patient-reported outcomes 1 year after total hip arthroplasty. Clinical Orthopaedics and Related Research, 473(11), 3370–3379.
van Walraven, C., et al. (2009). A modification of the Elixhauser comorbidity measures into a point system for hospital death using administrative data. Medical Care, 47(6), 626–633.
Kim, C.-Y., et al. (2018). Predicting adverse events, length of stay, and discharge disposition following shoulder arthroplasty: A comparison of the Elixhauser Comorbidity Measure and Charlson Comorbidity Index. Journal of shoulder and elbow surgery, 27(10), 1748–1755.
Ondeck, N. T., et al. (2018). Discriminative ability of elixhauser’s comorbidity measure is superior to other comorbidity scores for inpatient adverse outcomes after total hip arthroplasty. Journal of Arthroplasty, 33(1), 250–257.
Bülow, E., et al. (2017). Comorbidity does not predict long-term mortality after total hip arthroplasty. Acta Orthopaedica, 88(5), 472–477.
Linn, B. S., Linn, M. W., & Gurel, L. (1968). Cumulative illness rating scale. Journal of the American Geriatrics Society, 16(5), 622–626.
Conwell, Y., et al. (1993). Validation of a measure of physical illness burden at autopsy: The Cumulative Illness Rating Scale. Journal of the American Geriatrics Society, 41(1), 38–41.
Groll, D. L., et al. (2006). Assessment of long-term physical function in acute respiratory distress syndrome (ARDS) patients: comparison of the Charlson Comorbidity Index and the Functional Comorbidity Index. American Journal of Physical Medicine and Rehabilitation, 85(7), 574–581.
Mahomed, N. N., et al. (2002). The importance of patient expectations in predicting functional outcomes after total joint arthroplasty. The Journal of Rheumatology, 29(6), 1273.
Resnik, L., Gozalo, P., & Hart, D. L. (2011). Weighted index explained more variance in physical function than an additively scored functional comorbidity scale. Journal of Clinical Epidemiology, 64(3), 320–330.
Mariconda, M., et al. (2011). Quality of life and functionality after total hip arthroplasty: a long-term follow-up study. BMC Musculoskeletal Disorders, 12, 222.
Greenfield, S., et al. (1993). The importance of co-existent disease in the occurrence of postoperative complications and one-year recovery in patients undergoing total hip replacement. Comorbidity and outcomes after hip replacement. Medical Care, 31(2), 141–154.
de Groot, V., et al. (2003). How to measure comorbidity. A critical review of available methods. Journal of Clinical Epidemiology, 56(3), 221–229.
Miskulin, D. C., et al. (2001). Comorbidity assessment using the index of coexistent diseases in a multicenter clinical trial. Kidney International, 60(4), 1498–1510.
Li, P., Kim, M. M., & Doshi, J. A. (2010). Comparison of the performance of the CMS Hierarchical Condition Category (CMS-HCC) risk adjuster with the Charlson and Elixhauser comorbidity measures in predicting mortality. BMC Health Services Research, 10, 245.
Ellimoottil, C., et al. (2016). Medicare’s new bundled payment for joint replacement may penalize hospitals that treat medically complex patients. Health Affairs (Millwood), 35(9), 1651–1657.
Kumar, A., et al. (2017). Current Risk Adjustment and Comorbidity Index underperformance in predicting post-acute utilization and hospital readmissions after joint replacements: implications for comprehensive care for joint replacement model. Arthritis Care Research (Hoboken), 69(11), 1668–1675.
Siracuse, B. L., & Chamberlain, R. S. (2016). A preoperative scale for determining surgical readmission risk after total hip replacement. JAMA Surgery, 151(8), 701–709.
White, R. S., et al. (2018). Readmission rates and diagnoses following total hip replacement in relation to insurance payer status, race and ethnicity, and income status. Journal of Racial and Ethnic Health Disparities, 5(6), 1202–1214.
Sloan, K. L., et al. (2003). Construction and characteristics of the RxRisk-V: a VA-adapted pharmacy-based case-mix instrument. Medical Care, 41(6), 761–774.
Inacio, M. C., et al. (2015). Comparing co-morbidities in total joint arthroplasty patients using the RxRisk-V, Elixhauser, and Charlson Measures: a cross-sectional evaluation. BMC Musculoskeletal Disorders, 16, 385.
Pratt, N. L., et al. (2018). The validity of the Rx-Risk Comorbidity Index using medicines mapped to the Anatomical Therapeutic Chemical (ATC) Classification System. British Medical Journal Open, 8(4), e021122.
Inacio, M. C. S., et al. (2016). Evaluation of three comorbidity measures to predict mortality in patients undergoing total joint arthroplasty. Osteoarthritis Cartilage, 24(10), 1718–1726.
Charnley, J. (1972). The long-term results of low-friction arthroplasty of the hip performed as a primary intervention. Journal of Bone and Joint Surgery: British Volume, 54(1), 61–76.
Charnley, J., & Halley, D. K. (1975). Rate of wear in total hip replacement. Clinical Orthopaedics and Related Research, 112, 170–179.
Dunbar, M. J., Robertsson, O., & Ryd, L. (2004). What’s all that noise? The effect of co-morbidity on health outcome questionnaire results after knee arthroplasty. Acta Orthopaedica Scandinavica, 75(2), 119–126.
Malchau, H., et al. (2005). Presidential guest address: the Swedish Hip Registry: increasing the sensitivity by patient outcome data. Clinical Orthopaedics and Related Research, 441, 19–29.
Münger, P., et al. (2006). Patient-related risk factors leading to aseptic stem loosening in total hip arthroplasty: a case-control study of 5,035 patients. Acta Orthopaedica, 77(4), 567–574.
Foote, J., et al. (2009). Length of stay following primary total hip replacement. Annals of the Royal College of Surgeons of England, 91(6), 500–504.
Schaeffer, J. F., et al. (2015). The Association of ASA class on total knee and total hip arthroplasty readmission rates in an Academic Hospital. Journal of Arthroplasty, 30(5), 723–727.
Saklad, M. M. D. (1941). Grading of patients for surgical procedures. Anesthesiology, 2(3), 281–284.
Ranta, S., Hynynen, M., & Tammisto, T. (1997). A survey of the ASA physical status classification: significant variation in allocation among Finnish anaesthesiologists. Acta Anaesthesiologica Scandinavica, 41(5), 629–632.
Ferguson, R. J., et al. (2019). ASA class is associated with early revision and reoperation after total hip arthroplasty: An analysis of the Geneva and Swedish Hip Arthroplasty Registries. Acta orthopaedica, 90(4), 324–330.
Jolles, B. M., Zangger, P., & Leyvraz, P. F. (2002). Factors predisposing to dislocation after primary total hip arthroplasty: A multivariate analysis. Journal of Arthroplasty, 17(3), 282–288.
Singh, J. A., et al. (2011). Cardiac and thromboembolic complications and mortality in patients undergoing total hip and total knee arthroplasty. Annals of the Rheumatic Diseases, 70(12), 2082–2088.
Ridgeway, S., et al. (2005). Infection of the surgical site after arthroplasty of the hip. Journal of Bone and Joint Surgery: British Volume, 87(6), 844–850.
Hailer, N. P., et al. (2016). Early mortality, and morbidity after total hip arthroplasty in patients with femoral neck fracture. Acta Orthopaedica, 87(6), 560–566.
Mannion, A. F., et al. (2020). The association between comorbidity and the risks and early benefits of total hip arthroplasty for hip osteoarthritis. Journal of Arthroplasty, 35(9), 2480–2487.
Petersen, P. B., et al. (2020). Improvement in fast-track hip and knee arthroplasty: a prospective multicentre study of 36,935 procedures from 2010 to 2017. Scientific Reports, 10(1), 21233.
Snell, D. L., et al. (2020). Associations between comorbidity and quality of life outcomes after total joint replacement. Quality of Life Research.
Rajamäki, T. J., et al. (2020). Predictors of the use of analgesic drugs 1 year after joint replacement: a single-center analysis of 13,000 hip and knee replacements. Arthritis Research and Therapy, 22(1), 89.
Traven, S. A., et al. (2019). New 5-factor modified frailty index predicts morbidity and mortality in primary hip and knee arthroplasty. Journal of Arthroplasty, 34(1), 140–144.
Traven, S. A., et al. (2019). Frailty predicts medical complications, length of stay, readmission, and mortality in revision hip and knee arthroplasty. Journal of Arthroplasty, 34(7), 1412–1416.
Ryan, S. P., et al. (2019). Predicting costs exceeding bundled payment targets for total joint arthroplasty. Journal of Arthroplasty, 34(3), 412–417.
Goltz, D. E., et al. (2019). A weighted index of elixhauser comorbidities for predicting 90-day readmission after total joint arthroplasty. Journal of Arthroplasty, 34(5), 857–864.
Singh, J. A., et al. (2016). Validation of the Mayo Hip Score: construct validity, reliability and responsiveness to change. BMC Musculoskelet Disord, 17, 39.
Poitras, S., et al. (2018). Predicting hospital length of stay and short-term function after hip or knee arthroplasty: are both performance and comorbidity measures useful? International Orthopaedics, 42(10), 2295–2300.
Glassou, E. N., et al. (2018). Is gain in health-related quality of life after a total hip arthroplasty depended on the comorbidity burden? Acta Orthopaedica, 89(4), 374–379.
Triantafyllopoulos, G. K., et al. (2018). Rate and risk factors for periprosthetic joint infection among 36,494 primary total hip arthroplasties. Journal of Arthroplasty, 33(4), 1166–1170.
Riddle, D. L., & Golladay, G. J. (2018). Preoperative risk factors for postoperative falls in persons undergoing hip or knee arthroplasty: A longitudinal study of data from the osteoarthritis initiative. Archives of Physical Medicine and Rehabilitation, 99(5), 967–972.
Glassou, E. N., Pedersen, A. B., & Hansen, T. B. (2017). Is decreasing mortality in total hip and knee arthroplasty patients dependent on patients’ comorbidity? Acta Orthopaedica, 88(3), 288–293.
Lakomkin, N., et al. (2017). Higher modified charlson index scores are associated with increased incidence of complications, transfusion events, and length of stay following revision hip arthroplasty. Journal of Arthroplasty, 32(4), 1121–1124.
Loth, F. L., et al. (2017). Impact of comorbidities on outcome after total hip arthroplasty. Journal of Arthroplasty, 32(9), 2755–2761.
Slover, J., et al. (2017). Incidence and risk factors for blood transfusion in total joint arthroplasty: analysis of a statewide database. Journal of Arthroplasty, 32(9), 2684-2687.e1.
Messina, G., et al. (2017). Risk adjusted mortality after hip replacement surgery: a retrospective study. Annali dell Istituto Superiore di Sanita, 53(1), 40–45.
Phruetthiphat, O. A., et al. (2016). Incidence of and preoperative risk factors for surgical delay in primary total hip arthroplasty: Analysis from the American College of Surgeons National Surgical Quality Improvement Program. Journal of Arthroplasty, 31(11), 2432–2436.
Deyo, R. A., et al. (1992). Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. Journal of Clinical Epidemiology, 45(6), 613–619.
Halfon, P., et al. (2002). Measuring potentially avoidable hospital readmissions. Journal of Clinical Epidemiology, 55(6), 573–587.
Romano, P. S., et al. (1993). Adapting a clinical comorbidity index for use with ICD-9-CM administrative data: Differing perspectives. Journal of Clinical Epidemiology, 46(10), 1075–1079.
Schneeweiss, S., et al. (2003). Improved comorbidity adjustment for predicting mortality in Medicare populations. Health Services Research, 38(4), 1103–1120.
Learmonth, I. D., et al. (2007). The operation of the century: Total hip replacement. The Lancet, 370(9597), 1508–1519.
Cram, P., et al. (2011). Clinical characteristics and outcomes of medicare patients undergoing total hip arthroplasty, 1991–2008. JAMA, 305(15), 1560–1567.
Buirs, L. D., et al. (2016). Predictors of physical functioning after total hip arthroplasty: a systematic review. British Medical Journal Open, 6(9), e010725.
Olthof, M., et al. (2014). The association between comorbidity and length of hospital stay and costs in total hip arthroplasty patients: a systematic review. The Journal of Arthroplasty, 29(5), 1009–1014.
Hofstede, S. N., et al. (2016). Preoperative predictors for outcomes after total hip replacement in patients with osteoarthritis: A systematic review. BMC Musculoskeletal Disorders, 17(1), 212.
Buller, L. T., et al. (2015). The Influence of psychiatric comorbidity on perioperative outcomes following primary total hip and knee arthroplasty; a 17-year analysis of the National Hospital Discharge Survey Database. The Journal of Arthroplasty, 30(2), 165–170.
Rasouli, M., et al. (2016). ASA Physical Status, Charlson and Elixhauser Comorbidity Scores for Predicting Outcome after Orthopedic Surgery. American Society of Anesthesiologists 2016. Annual meeting abstract book.
Ou, H.-T., et al. (2012). Comparative performance of comorbidity indices in predicting health care-related behaviors and outcomes among Medicaid enrollees with type 2 diabetes. Population Health Management, 15(4), 220–229.
Hall, S. F. (2006). A user’s guide to selecting a comorbidity index for clinical research. Journal of Clinical Epidemiology, 59(8), 849–855.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
On behalf of all authors, the corresponding author ŁP states that there is no conflict of interest.
Ethical standard statement
This article does not contain any studies with human or animal subjects performed by the any of the authors.
Informed consent
For this type of study informed consent is not required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Pulik, Ł., Podgajny, M., Kaczyński, W. et al. The Update on Instruments Used for Evaluation of Comorbidities in Total Hip Arthroplasty. JOIO 55, 823–838 (2021). https://doi.org/10.1007/s43465-021-00357-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s43465-021-00357-x