
Abstract
Substance use disorder (SUD) is a chronic brain condition, with compulsive and uncontrollable drug-seeking that leads to long-lasting and harmful consequences. The factors contributing to the development of SUD, as well as its treatment settings, are not fully understood. Alterations in brain glutamate homeostasis in humans and animals implicate a key role of this neurotransmitter in SUD, while the modulation of glutamate transporters has been pointed as a new strategy to diminish the excitatory glutamatergic transmission observed after drugs of abuse. N-acetylcysteine (NAC), known as a safe mucolytic agent, is involved in the regulation of this system and may be taken into account as a novel pharmacotherapy for SUD. In this paper, we summarize the current knowledge on the ability of NAC to reduce drug-seeking behavior induced by psychostimulants, opioids, cannabinoids, nicotine, and alcohol in animals and humans. Preclinical studies showed a beneficial effect in animal models of SUD, while the clinical efficacy of NAC has not been fully established. In summary, NAC will be a small add-on to usual treatment and/or psychotherapy for SUD, however, further studies are required.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Substance use disorder (SUD) is a chronic brain condition, with compulsive and uncontrollable drug-seeking that leads to long-lasting and harmful consequences. SUD also evokes relapse that is triggered after (re)exposure to the drug, drug-associated cues or stressors [1]. As far as public health and safety are concerned, SUD remains an unsolved issue. Several drugs can produce addictive behavior in humans and animals, including psychostimulants, opioids, cannabinoids, nicotine, and alcohol. The factors contributing to the development of SUD, as well as its treatment settings, are not fully understood.
Although the primary behavioral outcomes of addictive substances are realized through distinct effector mechanisms, such as neurotransmitter transporters, ion channels, and receptor proteins, the common feature of these drugs is concerned with increased dopamine neurotransmission within the mesocorticolimbic circuitry of the brain from the ventral tegmental area to the nucleus accumbens and prefrontal cortex [1].
Literature studies indicate that neuroadaptations within prefrontal cortical-hippocampal-striatal circuits, interconnected via glutamatergic signaling, are dysfunctional in SUD and may represent common mechanisms triggered in the case of chronic use of drugs of abuse and relapse [2]. In fact, preclinical research demonstrates that repeated exposure to several addictive substances evokes a drop in basal concentrations of extracellular glutamate [3,4,5]. The above change is associated with long-lasting decreases in the expression of the glial glutamate transporter 1 (GLT-1) and the cystine-glutamate exchange system/antiporter (system xc−) within the nucleus accumbens and/or prefrontal cortex related to downregulation of the genes encoding the latter system [6,7,8,9,10,11]. The system xc− is a glycoprotein-associated amino acid transporter that catalyzes Na+-independent exchange of extracellular cystine for intracellular glutamate in a 1:1 stoichiometric ratio [12], and in the brain is functionally expressed as a heterodimer [13]; its catalytic unit is called xCT. Further, it influences glutamate neurotransmission by maintaining the basal level of extracellular glutamate followed by local stimulation of group II metabotropic glutamate autoreceptors. GLT-1 (also known as EAAT2) is responsible for the largest proportion of glutamate transport and control over glutamate clearance. Furthermore, in rodents drug-seeking reinstatement raises extracellular accumbal glutamate levels [14]. In line with animal research, clinical data using tailored proton magnetic resonance spectroscopy demonstrated that people with cocaine use disorder have reduced basal glutamate concentrations and increased glutamate levels in the nucleus accumbens during cue-induced craving [15]. This finding is supported by another proton magnetic resonance spectroscopy trial involving the dorsal anterior cingulate cortex, where glutamate levels were significantly higher in cocaine-dependent patients compared with healthy controls [16]. Alterations in brain glutamate homeostasis in humans and animals implicate a key role of this neurotransmitter in SUD. Additionally, the modulation of cystine-glutamate exchange via the system xc− has been suggested as a new strategy to diminish the excitatory glutamatergic transmission observed after drugs of abuse, while drugs that influence that system—such as N-acetylcysteine (NAC)—were considered as promising targets for the development of novel pharmacotherapies of SUD.
NAC
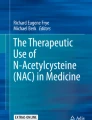
NAC is an acetyl derivative of a semi-essential amino acid. After oral administration, NAC is rapidly absorbed from the gastrointestinal tract, and in the liver, it is transformed through deacetylation to cysteine, which (1) is used for glutathione (GSH) production, (2) enters the bloodstream and crosses the blood–brain barrier [17, 18] using a sodium-dependent transport system. However, NAC has low bioavailability in contrast to its amide derivative [19]. In the brain, cysteine is metabolized to cysteine and it modulates the synaptic release of glutamate through the plasma membrane-localized system xc− (Fig. 1) [20]. This process activates the metabotropic glutamate receptors group II on presynaptic neurons, responsible for inhibiting the synaptic release of glutamate and thereby restoring local extracellular glutamate levels in the nucleus accumbens [10, 21]. Cysteine is the rate-limiting substrate for an important antioxidant—GSH—and, along with cystine, it also forms a key redox couple on its own. The highest plasma concentrations of NAC were detected up to 1 h following oral administration with the terminal t1/2 of about 6 h [22, 23].

Mechanism of action and summary of N-acetylcysteine effects in preclinical and clinical studies. ∅ no changed, ↓ decreased, GLT-1 glutamate transporter 1, GSH glutathione, system xc− cystine/glutamate antiporter
NAC was approved for the treatment of potentially hepatotoxic doses of acetaminophen and pulmonary complications of cystic fibrosis. Apart from hepatoprotective, mucolytic, antioxidant, and anti-inflammatory activities, it has been shown that this drug exerts neurochemical effects in SUD.
The preclinical and clinical use of NAC
This literature review summarizes research results concerning the efficacy of NAC in SUD. In the beginning, a set of conditions of searching for all experiments on animals, as well as preclinical and clinical trials (controlled and uncontrolled clinical trials, open-label cases), reported until 2020 was developed to determine the eligibility of a study using several databases, including Web of Science, Pub Med, Medline, Clinical trials and Google. All results were obtained by searching for specific keywords, as indicated in brackets, related to treatment (N-acetylcysteine—acetylcysteine), substances (marijuana/cannabinoids—tobacco/nicotine—morphine/heroin/opioid—cocaine/amphetamine/methamphetamine—alcohol) and their results (efficacy—effectiveness—outcomes—evaluation). Additionally, preclinical and clinical search terms were combined with the type of animal model (self-administration—conditioned place preference) or disorders (substance use disorders—addiction—substance abuse—dependence). Recent reviews have become increasingly focused on the potential clinical use of NAC [24, 25] in patients suffering from several psychiatric disorders, including SUD. However, this manuscript will provide a brief outline of the potential role of NAC in pharmacotherapy and examine all preclinical and clinical studies on NAC in the treatment of SUD.
NAC and preclinical research
The first study showing the beneficial effects of NAC in SUD was published in 2003 [10]. Findings from Dr. Peter Kalivas’s laboratory indicate that systemic NAC treatment in rats evoked a dose-dependent decrease in the reinstatement of cocaine-seeking that was linked to restoring accumbal extracellular glutamate and the xc− system [10]. From that time more than 40 research papers aimed to determine whether NAC alters reward, abstinence or reinstatement of drugs of abuse and whether the restoration of the xc− system is accompanied by such changes were released (Table 1).
In rodent models of alcohol use disorder (AUD), NAC given in acute doses or repeatedly (during abstinence period) reduced alcohol intake [26,27,28], and was responsible for the development of alcohol sensitization [29], extinction responding [30], alcohol relapse [27, 28, 31], alcohol withdrawal-induced anxiety and depression [32, 33] (Table 1). These changes were examined in male rats or mice. However, a recent paper by Quintanilla et al. also demonstrated inhibitory actions of NAC towards alcohol intake or relapse in female rats [28]. Interestingly, reductions seen after NAC treatment in behavioral studies were accompanied by either restoration in the accumbal xc− system [29] or no changes [30]. Although the changes in the xc− system following NAC in AUC are not resolved, further examinations of glutamate-related neuroadaptations in animal alcohol models revealed a decrease in the drug-related enhanced hippocampal oxidized/reduced glutathione ratio levels in both male [27] and female [28] rats. Additionally, NAC attenuated neuroinflammation expressed by the glial fibrillary acidic protein immunohistochemistry in the rat hippocampus, showing for the first time a new target for NAC treatment [28].
NAC effects in cannabinoid use disorder were addressed in a separate paper. Thus, Spencer et al. indicated that daily treatment with NAC attenuated cue-induced reinstatement of Δ9-tetrahydrocannabinol and cannabidiol seeking in rats [34].
Considering nicotine use disorder (NUD), there are several data supporting beneficial effects of acute or chronic NAC treatment on nicotine reward assessed in self-administration or conditioned place preference rodent models [27, 35,36,37] (Table 1). Importantly, no indication of tolerance development was observed after chronic NAC treatment toward nicotine reward [37]. Furthermore, NAC blocked mouse behaviors associated with nicotine somatic withdrawal signs, but not anxiety developed during nicotine withdrawal [36]. Other proofs that NAC may have high clinical utility in NUD were provided in reports showing the drug reducing efficacy in models assessing nicotine seeking and reinstatement behaviors [35, 38,39,40,41,42] (Table 1). Of note, subchronic NAC administration (< 4 days) was found as ineffective in reducing cue-induced reinstatement and in restoring nicotine-evoked disruption in dendritic spine morphology and glutamatergic transcripts in the accumbal core region [42]. In other molecular and neurochemical assays combined with behavioral evaluations, it was found that NAC effectively reversed a drop in the accumbal xc− system and GLT-1, seen 7 or 50 days after cue-induced reinstatement, respectively [39, 40]. The latter paper even reports the anti-relapse activity of NAC with cue exposure therapy that persisted 50 days after drug treatment, supporting the idea of adopting a combined strategy for treating NUD. Interestingly, NAC did not alter cue-induced reinstatement in female rats regardless of their estrous cycle phase, which may suggest NAC sex-specific efficacy and some limitation in its use [41]. However, based on a separate report, it is difficult to draw the final conclusion and more data addressing both genders are required.
Four reports addressed the effects of NAC in rodent models of opioid use disorder (Table 1). In rats extinguishing from heroin self-administration, NAC reduced cue- or drug-evoked reinstatement precipitated after 10–40 days of heroin withdrawal [43, 44]. NAC used as an add-on drug attenuated the development of morphine tolerance and dependence in mice and associated biochemical alterations, such as reduced GSH level and GSH peroxidase activity [45, 46].
Considering amphetamines use in rats and nonhuman primates (Table 1), NAC neither changed amphetamine or cocaine reward, cocaine relapse [47], re-expression of amphetamine sensitization [48], methamphetamine reward nor reinstatement [49].
On the other hand, there is no doubt that in rat models of cocaine use disorder (CUD), NAC did not change cocaine reward, but effectively reduced escalation of drug intake, cocaine-seeking, and reinstatement behaviors [8, 10, 14, 19, 21, 50,51,52,53,54,55,56,57] (Table 1). The latter effects were observed after systemic or intra-accumbens NAC administration. Furthermore, the behavioral attenuation of cocaine actions appeared together with NAC-induced restoration of the xc− system, GLT-1, and AMPA/NMDA ratio in accumbal or striatal brain regions [8, 21, 57, 58]. Taken together, preclinical works have supported the role of imbalances in the accumbal glutamatergic system as a driver of addictive behaviors in rodents. However, in this context, it should be added that NAC did not show efficacy in monkeys toward cocaine-induced reinstatement [47]. Since people with cocaine use disorder suffer from depression, such comorbidity was evaluated using cocaine self-administration/extinction/reinstatement procedures in the rat model of depression based on the removal of the olfactory bulbs [19]. In the latter paper it was shown that repeated treatment with NAC did not alter reinstatement of cocaine-seeking behavior, while its amide derivative, that is AD4, effectively blocked cue- or cocaine-induced reinstatement [19].
To summarize, studies on male rats show that NAC is able to significantly diminish the propensity to seek drugs of abuse (Table 1). The molecular or neurochemical mechanisms underlying such NAC effects are not fully recognized as the xc system was found as unnecessary to reduce cocaine-seeking [58]. New—and independent of the xc− system—mechanisms of NAC, such as restoring GLT-1 [58] or GSH levels [27, 28] or influencing immunomodulatory markers (the nuclear factor kappa-light-chain-enhancer of activated B cells signaling pathway) [38] were proposed.
NAC and clinical research
Apart from pre-clinical studies, also clinical trials addressed the role of NAC therapy in diminishing relapse to addictive drug use. To date, NAC demonstrated promising results in subjects with cocaine, heroin, and tobacco addiction.
About 30% effectiveness of NAC on alcohol consumption was shown in adults during cannabis cessation [59]. One study regarded co-occurrence of AUD and post-traumatic stress disorder [60]; however, further studies are required for the determination of NAC effectiveness on alcohol consumption in patients suffering from AUD (Table 2).
Mixed results on the NAC efficacy have been shown in humans with cannabis dependency (Table 2). In fact, an open-label study showed that NAC reduced self-reported marijuana use without differences in the urine cannabis toxicology in young people [61]. During randomized placebo-controlled trials in young people with cannabis dependence after 8 weeks of NAC treatment combined with behavioral therapy, the odds of negative urine toxicology were twice higher as compared to placebo [62], while NAC treatment did not change the cannabis craving in these adolescents in a secondary analysis from that clinical trial [63]. Additionally, the reduced craving was observed in both groups, suggesting that marijuana craving probably is not involved in NAC cessation effects [63]. An intent-to-treat analysis showed the relation between low pretreatment impulsivity, NAC efficacy, and negative urine toxicology for cannabinoids [64]. On the contrary, another clinical trial involving 12-week NAC therapy in adults with cannabis use disorder, did not show differences in cannabis abstinence and urine cannabinoid tests compared to the placebo-treated group [65]. However, the analysis of a subgroup of adults with co-occurring depressive symptoms and cannabis dependence found an association between higher baseline depression and decreased abstinence rates during the trial, and neither NAC nor placebo attenuated the depressive symptoms [66]. It should be emphasized that while subgroup analyses can be suggestive, they do not give strong evidence that the drug actually helped to a specific subgroup. Taken together, the co-occurrence of the behavioral therapy and NAC treatment seems to contribute to decreased cannabis use in individuals, however, further studies are required to clarify these beneficial effects.
Despite the fact that several preclinical studies confirmed the beneficial effects of NAC treatment on nicotine reward, the clinical studies are not that convincing (Table 2). Healthy individuals with NUD treated with NAC reported a reduction in the number of cigarettes smoked, however, there were no differences in craving, withdrawal, and biochemical verification of smoking [67]. Three-and-a-half day treatment with NAC (3.6 g daily) during short-term abstinence in heavy smokers did not evoke significant effects on craving and withdrawal symptoms; however, individuals treated with NAC experienced less pleasure from smoking the first cigarette posttreatment [68]. On the contrary, the positive effect of NAC at a lower dose (2.4 g daily) during 3.5-day monetary-incentivized smoking abstinence on nicotine abstinence, craving, and resting-state functional connectivity in frontostriatal areas was presented [69]. Four-week co-administration of varenicline (an α4β2 nicotinic receptor antagonist) and NAC reduced the number of cigarettes per day in adult smokers, however, a low abstinence score at the study end was presented [70]. In patients with co-occurring NUD and gambling, NAC treatment with augmented behavioral therapy during the first 6 weeks was beneficial but returned to baseline in the 3-month follow-up [71]. Eight-week NAC administration did not change daily cigarettes smoked and withdrawal [72]. Twelve-week NAC treatment at a dose of 3 g daily evoked a reduction in the number of cigarettes smoked, exhaled CO, and depression severity [73]. Adjunctive NAC at lower doses (1.8 g daily) significantly reduced abstinence score and inflammation state (soluble tumor necrosis factor receptor 2 levels) without the effect on anxiety and depression, as well as on the metabolism components [74]. Additionally, a larger study consisting of 8 and 16 weeks NAC treatment (1.8 g daily) with a 42-week post-discontinuation follow-up has been started [75]. In conclusion, a recommendation for NAC use for NUD cannot be made at this time, as further research is required.
The effects of NAC on cocaine-seeking behavior have been well studied in animal studies. In healthy cocaine-dependents, 4-day NAC treatment reduced the withdrawal symptoms and craving [76]. A follow-up study showed that NAC administered during two 3-day inpatient hospitalizations separated by 4 days reduced the desire for cocaine use induced by drug-related cues, as well as decreased interest and time for a view cue [77]. At the same time, 4-day NAC treatment reduced craving and the motivational qualities of a cocaine challenge injection but did not affect euphoric properties in individuals with CUD [78]. In an open-label study, a reduction in the self-reported cocaine use was reported in NAC-treated cocaine-dependent patients after 4-week treatment [79]. Higher glutamate levels in the dorsal anterior cingulate cortex associated with higher impulsivity were detected in patients with CUD compared to healthy controls, that were reduced after a single administration of 2.4 g NAC [16]. It should be noted that increased glutamate levels are typical during cocaine relapse, what suggests that NAC may have potentially positive effects in CUD [5, 80]. Moreover, 25-day NAC treatment increased cognitive control without the effect on working memory in cocaine-using men [81]. Eight-week NAC treatment did not reduce cocaine use in patients with CUD, however, it was shown that NAC prevented cocaine relapse rather than promoted initial drug-abstinence [82]. Attenuation of cocaine-cue attentional bias and reduced intranasal cocaine self-administration were observed after NAC treatment [83] (Table 2). It should be mentioned that according to the latest systematic review and meta-analysis performed by Duailibi et al., NAC was superior to placebo in diminishing craving symptoms in SUD [84]. However, this meta-analysis was based on seven randomized control trials with heterogeneous methodology and a small sample size (n = 245) and further studies are necessary to determine the potential impact of NAC on craving symptoms in SUD.
Eight-week co-administration of NAC and naltrexone in adults with methamphetamine use disorder did not affect cravings, drug use, urine toxicology, depression, anxiety, disability, and quality of life at different points of the study, compared to the placebo group [85]. On the contrary, another clinical study showed that 8-week NAC administration reduced methamphetamine craving [86] (Table 2). However, further investigation in a larger population is required to demonstrate the exact NAC efficacy.
Summary
This review provides proof for NAC efficacy in SUD in animal models (Fig. 1). As far as beneficial effects of NAC are concerned, the modulation of GLT-1 seems to be crucial for diminishing the excitatory glutamatergic transmission observed after drugs of abuse. However, the efficacy of NAC in different drug dependencies has not been established yet. It should be emphasized that in preclinical studies the experimental conditions are stable, where no other sources of variance exist beyond the experimental variables and even a small effect of NAC may be detected using animal models. On the other hand, in human studies, more factors are implicated and the clinical efficacy is more difficult to investigate. NAC is safe and well-tolerated, but the most likely outcome, even with more studies, larger samples, and better designs, is that NAC will be a small add-on to usual treatment and/or psychotherapy for SUD. While preclinical studies have shown promise, further clinical studies and trials concerning the exact effects of NAC on SUD will be required before including this drug in general clinical practice and to point to potential groups that can actually benefit from the drug.
Abbreviations
- AUD:
-
Alcohol use disorder
- CUD:
-
Cocaine use disorder
- GLT-1:
-
Glutamate transporter 1
- GSH:
-
Glutathione
- NAC:
-
N-acetylcysteine
- NUD:
-
Nicotine use disorder
- SUD:
-
Substance use disorder
- System xc − :
-
Cystine/glutamate antiporter
- xCT:
-
Catalytic subunit of system xc−
References
Kalivas PW. Recent understanding in the mechanisms of addiction. Curr Psychiatry Rep. 2004;6(5):347–51.
Smaga I, Sanak M, Filip M. Cocaine-induced changes in the expression of NMDA receptor subunits. Curr Neuropharmacol. 2019;17:1039.
Pierce RC, Bell K, Duffy P, Kalivas PW. Repeated cocaine augments excitatory amino acid transmission in the nucleus accumbens only in rats having developed behavioral sensitization. J Neurosci. 1996;16(4):1550–60.
McFarland K, Lapish CC, Kalivas PW. Prefrontal glutamate release into the core of the nucleus accumbens mediates cocaine-induced reinstatement of drug-seeking behavior. J Neurosci. 2003;23(8):3531–7.
Wydra K, Golembiowska K, Zaniewska M, Kaminska K, Ferraro L, Fuxe K, et al. Accumbal and pallidal dopamine, glutamate and GABA overflow during cocaine self-administration and its extinction in rats. Addict Biol. 2013;18(2):307–24.
Bechard AR, Hamor PU, Wu L, Schwendt M, Knackstedt LA. The effects of clavulanic acid and amoxicillin on cue-primed reinstatement of cocaine seeking. Behav Neurosci. 2019;133(2):247–54.
Knackstedt LA, Kalivas PW. Glutamate and reinstatement. Curr Opin Pharmacol. 2009;9(1):59–64.
Knackstedt LA, Melendez RI, Kalivas PW. Ceftriaxone restores glutamate homeostasis and prevents relapse to cocaine seeking. Biol Psychiatry. 2010;67(1):81–4.
Smaga I, Fierro D, Mesa J, Filip M, Knackstedt LA. Molecular changes evoked by the beta-lactam antibiotic ceftriaxone across rodent models of substance use disorder and neurological disease. Neurosci Biobehav Rev. 2020;115:116–30.
Baker DA, McFarland K, Lake RW, Shen H, Tang XC, Toda S, et al. Neuroadaptations in cystine-glutamate exchange underlie cocaine relapse. Nat Neurosci. 2003;6(7):743–9.
Smaga I, Gawlińska K, Frankowska M, Wydra K, Sadakierska-Chudy A, Suder A, et al. Extinction training after cocaine self-administration influences the epigenetic and genetic machinery responsible for glutamatergic transporter gene expression in male rat brain. Neuroscience. 2020;451:99–110.
McBean GJ. Cerebral cystine uptake: a tale of two transporters. Trends Pharmacol Sci. 2002;23(7):299–302.
Sato H, Tamba M, Okuno S, Sato K, Keino-Masu K, Masu M, et al. Distribution of cystine/glutamate exchange transporter, system x(c)-, in the mouse brain. J Neurosci. 2002;22(18):8028–33.
Kau KS, Madayag A, Mantsch JR, Grier MD, Abdulhameed O, Baker DA. Blunted cystine-glutamate antiporter function in the nucleus accumbens promotes cocaine-induced drug seeking. Neuroscience. 2008;155(2):530–7.
Engeli EJE, Zoelch N, Hock A, Nordt C, Hulka LM, Kirschner M et al. Impaired glutamate homeostasis in the nucleus accumbens in human cocaine addiction. Mol Psychiatry. 2020.
Schmaal L, Veltman DJ, Nederveen A, van den Brink W, Goudriaan AE. N-acetylcysteine normalizes glutamate levels in cocaine-dependent patients: a randomized crossover magnetic resonance spectroscopy study. Neuropsychopharmacology. 2012;37(9):2143–52.
Smaga I, Pomierny B, Krzyżanowska W, Pomierny-Chamioło L, Miszkiel J, Niedzielska E, et al. N-acetylcysteine possesses antidepressant-like activity through reduction of oxidative stress: behavioral and biochemical analyses in rats. Prog Neuropsychopharmacol Biol Psychiatry. 2012;39(2):280–7.
Deepmala, Slattery J, Kumar N, Delhey L, Berk M, Dean O, et al. Clinical trials of N-acetylcysteine in psychiatry and neurology: a systematic review. Neurosci Biobehav Rev. 2015;55:294–321.
Jastrzębska J, Frankowska M, Filip M, Atlas D. N-acetylcysteine amide (AD4) reduces cocaine-induced reinstatement. Psychopharmacology. 2016;233(18):3437–48.
Smaga I, Frankowska M, Filip M. N-acetylcysteine as a new prominent approach for treating psychiatric disorders. Br J Pharmacol. 2021;1–26.
Madayag A, Lobner D, Kau KS, Mantsch JR, Abdulhameed O, Hearing M, et al. Repeated N-acetylcysteine administration alters plasticity-dependent effects of cocaine. J Neurosci. 2007;27(51):13968–76.
Massie A, Boillee S, Hewett S, Knackstedt L, Lewerenz J. Main path and byways: non-vesicular glutamate release by system xc(-) as an important modifier of glutamatergic neurotransmission. J Neurochem. 2015;135(6):1062–79.
Lewerenz J, Hewett SJ, Huang Y, Lambros M, Gout PW, Kalivas PW, et al. The cystine/glutamate antiporter system x(c)(-) in health and disease: from molecular mechanisms to novel therapeutic opportunities. Antioxid Redox Signal. 2013;18(5):522–55.
Scofield MD, Kalivas PW. Astrocytic dysfunction and addiction: consequences of impaired glutamate homeostasis. Neuroscientist. 2014;20(6):610–22.
Brown RM, Kupchik YM, Kalivas PW. The story of glutamate in drug addiction and of N-acetylcysteine as a potential pharmacotherapy. JAMA Psychiat. 2013;70(9):895–7.
Ferreira Seiva FR, Amauchi JF, Ribeiro Rocha KK, Souza GA, Ebaid GX, Burneiko RM, et al. Effects of N-acetylcysteine on alcohol abstinence and alcohol-induced adverse effects in rats. Alcohol. 2009;43(2):127–35.
Quintanilla ME, Morales P, Ezquer F, Ezquer M, Herrera-Marschitz M, Israel Y. Commonality of ethanol and nicotine reinforcement and relapse in Wistar-derived UChB rats: inhibition by N-Acetylcysteine. Alcohol Clin Exp Res. 2018;42(10):1988–99.
Quintanilla ME, Ezquer F, Morales P, Ezquer M, Olivares B, Santapau D, et al. N-Acetylcysteine and acetylsalicylic acid inhibit alcohol consumption by different mechanisms: combined protection. Front Behav Neurosci. 2020;14:122.
Morais-Silva G, Alves GC, Marin MT. N-acetylcysteine treatment blocks the development of ethanol-induced behavioural sensitization and related ΔFosB alterations. Neuropharmacology. 2016;110(Pt A):135–42.
Lebourgeois S, González-Marín MC, Antol J, Naassila M, Vilpoux C. Evaluation of N-acetylcysteine on ethanol self-administration in ethanol-dependent rats. Neuropharmacology. 2019;150:112–20.
Cano-Cebrián MJ, Fernández-Rodríguez S, Hipólito L, Granero L, Polache A, Zornoza T. Efficacy of N-acetylcysteine in the prevention of alcohol relapse-like drinking: study in long-term ethanol-experienced male rats. J Neurosci Res. 2021;99(2):638–48.
Schneider R Jr, Santos CF, Clarimundo V, Dalmaz C, Elisabetsky E, Gomez R. N-acetylcysteine prevents behavioral and biochemical changes induced by alcohol cessation in rats. Alcohol. 2015;49(3):259–63.
Yawalkar R, Changotra H, Gupta GL. Protective influences of N-acetylcysteine against alcohol abstinence-induced depression by regulating biochemical and GRIN2A, GRIN2B gene expression of NMDA receptor signaling pathway in rats. Neurochem Int. 2018;118:73–81.
Spencer S, Neuhofer D, Chioma VC, Garcia-Keller C, Schwartz DJ, Allen N, et al. A model of Δ(9)-Tetrahydrocannabinol self-administration and reinstatement that alters synaptic plasticity in nucleus accumbens. Biol Psychiatry. 2018;84(8):601–10.
Rao KN, Sentir AM, Engleman EA, Bell RL, Hulvershorn LA, Breier A, et al. Toward early estimation and treatment of addiction vulnerability: radial arm maze and N-acetyl cysteine before cocaine sensitization or nicotine self-administration in neonatal ventral hippocampal lesion rats. Psychopharmacology. 2016;233(23–24):3933–45.
Bowers MS, Jackson A, Maldoon PP, Damaj MI. N-acetylcysteine decreased nicotine reward-like properties and withdrawal in mice. Psychopharmacology. 2016;233(6):995–1003.
Ramirez-Niño AM, D’Souza MS, Markou A. N-acetylcysteine decreased nicotine self-administration and cue-induced reinstatement of nicotine seeking in rats: comparison with the effects of N-acetylcysteine on food responding and food seeking. Psychopharmacology. 2013;225(2):473–82.
Namba MD, Kupchik YM, Spencer SM, Garcia-Keller C, Goenaga JG, Powell GL, et al. Accumbens neuroimmune signaling and dysregulation of astrocytic glutamate transport underlie conditioned nicotine-seeking behavior. Addict Biol. 2020;25(5):e12797.
Moro F, Orrù A, Marzo CM, Di Clemente A, Cervo L. mGluR2/3 mediates short-term control of nicotine-seeking by acute systemic N-acetylcysteine. Addict Biol. 2018;23(1):28–40.
Moro F, Giannotti G, Caffino L, Marzo CM, Di Clemente A, Fumagalli F, et al. Lasting reduction of nicotine-seeking behavior by chronic N-acetylcysteine during experimental cue-exposure therapy. Addict Biol. 2020;25(4):e12771.
Goenaga J, Powell GL, Leyrer-Jackson JM, Piña J, Phan S, Prakapenka AV, et al. N-acetylcysteine yields sex-specific efficacy for cue-induced reinstatement of nicotine seeking. Addict Biol. 2020;25(1):e12711.
Powell GL, Leyrer-Jackson JM, Goenaga J, Namba MD, Piña J, Spencer S, et al. Chronic treatment with N-acetylcysteine decreases extinction responding and reduces cue-induced nicotine-seeking. Physiol Rep. 2019;7(1):e13958.
Hodebourg R, Murray JE, Fouyssac M, Puaud M, Everitt BJ, Belin D. Heroin seeking becomes dependent on dorsal striatal dopaminergic mechanisms and can be decreased by N-acetylcysteine. Eur J Neurosci. 2019;50(3):2036–44.
Zhou W, Kalivas PW. N-acetylcysteine reduces extinction responding and induces enduring reductions in cue- and heroin-induced drug-seeking. Biol Psychiatry. 2008;63(3):338–40.
Abdel-Zaher AO, Abdel-Rahman MS, Fahmy EL. Blockade of nitric oxide overproduction and oxidative stress by Nigella sativa oil attenuates morphine-induced tolerance and dependence in mice. Neurochem Res. 2010;35(10):1557–65.
Abdel-Zaher AO, Mostafa MG, Farghaly HS, Hamdy MM, Abdel-Hady RH. Role of oxidative stress and inducible nitric oxide synthase in morphine-induced tolerance and dependence in mice. Effect of alpha-lipoic acid. Behav Brain Res. 2013;247:17–26.
Bauzo RM, Kimmel HL, Howell LL. The cystine-glutamate transporter enhancer N-acetyl-L-cysteine attenuates cocaine-induced changes in striatal dopamine but not self-administration in squirrel monkeys. Pharmacol Biochem Behav. 2012;101(2):288–96.
Taracha E, Kaniuga E, Chrapusta SJ, Boguszewski PM, Lehner M, Krząścik P, et al. N-acetyl cysteine does not modify the sensitization of the rewarding effect of amphetamine as assessed with frequency-modulated 50-kHz vocalization in the rat. Behav Brain Res. 2015;280:141–8.
Charntikov S, Pittenger ST, Pudiak CM, Bevins RA. The effect of N-acetylcysteine or bupropion on methamphetamine self-administration and methamphetamine-triggered reinstatement of female rats. Neuropharmacology. 2018;135:487–95.
Moran MM, McFarland K, Melendez RI, Kalivas PW, Seamans JK. Cystine/glutamate exchange regulates metabotropic glutamate receptor presynaptic inhibition of excitatory transmission and vulnerability to cocaine seeking. J Neurosci. 2005;25(27):6389–93.
Moussawi K, Pacchioni A, Moran M, Olive MF, Gass JT, Lavin A, et al. N-Acetylcysteine reverses cocaine-induced metaplasticity. Nat Neurosci. 2009;12(2):182–9.
Reichel CM, Moussawi K, Do PH, Kalivas PW, See RE. Chronic N-acetylcysteine during abstinence or extinction after cocaine self-administration produces enduring reductions in drug seeking. J Pharmacol Exp Ther. 2011;337(2):487–93.
Kupchik YM, Moussawi K, Tang XC, Wang X, Kalivas BC, Kolokithas R, et al. The effect of N-acetylcysteine in the nucleus accumbens on neurotransmission and relapse to cocaine. Biol Psychiatry. 2012;71(11):978–86.
Murray JE, Everitt BJ, Belin D. N-Acetylcysteine reduces early- and late-stage cocaine seeking without affecting cocaine taking in rats. Addict Biol. 2012;17(2):437–40.
Frankowska M, Jastrzębska J, Nowak E, Białko M, Przegaliński E, Filip M. The effects of N-acetylcysteine on cocaine reward and seeking behaviors in a rat model of depression. Behav Brain Res. 2014;266:108–18.
Kangas BD, Doyle RJ, Kohut SJ, Bergman J, Kaufman MJ. Effects of chronic cocaine self-administration and N-acetylcysteine on learning, cognitive flexibility, and reinstatement in nonhuman primates. Psychopharmacology. 2019;236(7):2143–53.
Ducret E, Puaud M, Lacoste J, Belin-Rauscent A, Fouyssac M, Dugast E, et al. N-acetylcysteine facilitates self-imposed abstinence after escalation of cocaine intake. Biol Psychiatry. 2016;80(3):226–34.
Reissner KJ, Gipson CD, Tran PK, Knackstedt LA, Scofield MD, Kalivas PW. Glutamate transporter GLT-1 mediates N-acetylcysteine inhibition of cocaine reinstatement. Addict Biol. 2015;20(2):316–23.
Squeglia LM, Tomko RL, Baker NL, McClure EA, Book GA, Gray KM. The effect of N-acetylcysteine on alcohol use during a cannabis cessation trial. Drug Alcohol Depend. 2018;185:17–22.
Back SE, Gray K, Santa Ana E, Jones JL, Jarnecke AM, Joseph JE, et al. N-acetylcysteine for the treatment of comorbid alcohol use disorder and posttraumatic stress disorder: design and methodology of a randomized clinical trial. Contemp Clin Trials. 2020;91:105961.
Gray KM, Watson NL, Carpenter MJ, Larowe SD. N-acetylcysteine (NAC) in young marijuana users: an open-label pilot study. Am J Addict. 2010;19:187–9.
Gray KM, Carpenter MJ, Baker NL, DeSantis SM, Kryway E, Hartwell KJ, et al. A double-blind randomized controlled trial of N-acetylcysteine in cannabis-dependent adolescents. Am J Psychiatry. 2012;169(8):805–12.
Roten AT, Baker NL, Gray KM. Marijuana craving trajectories in an adolescent marijuana cessation pharmacotherapy trial. Addict Behav. 2013;38(3):1788–91.
Bentzley JP, Tomko RL, Gray KM. Low pretreatment impulsivity and high medication adherence increase the odds of abstinence in a trial of N-acetylcysteine in adolescents with cannabis use disorder. J Subst Abuse Treat. 2016;63:72–7.
Gray KM, Sonne SC, McClure EA, Ghitza UE, Matthews AG, McRae-Clark AL, et al. A randomized placebo-controlled trial of N-acetylcysteine for cannabis use disorder in adults. Drug Alcohol Depend. 2017;177:249–57.
Tomko RL, Baker NL, Hood CO, Gilmore AK, McClure EA, Squeglia LM, et al. Depressive symptoms and cannabis use in a placebo-controlled trial of N-Acetylcysteine for adult cannabis use disorder. Psychopharmacology. 2020;237(2):479–90.
Knackstedt LA, LaRowe S, Mardikian P, Malcolm R, Upadhyaya H, Hedden S, et al. The role of cystine-glutamate exchange in nicotine dependence in rats and humans. Biol Psychiatry. 2009;65(10):841–5.
Schmaal L, Berk L, Hulstijn KP, Cousijn J, Wiers RW, van den Brink W. Efficacy of N-acetylcysteine in the treatment of nicotine dependence: a double-blind placebo-controlled pilot study. Eur Addict Res. 2011;17(4):211–6.
Froeliger B, McConnell PA, Stankeviciute N, McClure EA, Kalivas PW, Gray KM. The effects of N-Acetylcysteine on frontostriatal resting-state functional connectivity, withdrawal symptoms and smoking abstinence: a double-blind, placebo-controlled fMRI pilot study. Drug Alcohol Depend. 2015;156:234–42.
McClure EA, Baker NL, Gipson CD, Carpenter MJ, Roper AP, Froeliger BE, et al. An open-label pilot trial of N-acetylcysteine and varenicline in adult cigarette smokers. Am J Drug Alcohol Abuse. 2015;41(1):52–6.
Grant JE, Odlaug BL, Chamberlain SR, Potenza MN, Schreiber LR, Donahue CB, et al. A randomized, placebo-controlled trial of N-acetylcysteine plus imaginal desensitization for nicotine-dependent pathological gamblers. J Clin Psychiatry. 2014;75(1):39–45.
McClure EA, Baker NL, Gray KM. Cigarette smoking during an N-acetylcysteine-assisted cannabis cessation trial in adolescents. Am J Drug Alcohol Abuse. 2014;40(4):285–91.
Prado E, Maes M, Piccoli LG, Baracat M, Barbosa DS, Franco O, et al. N-acetylcysteine for therapy-resistant tobacco use disorder: a pilot study. Redox Rep. 2015;20(5):215–22.
Machado R, Vargas HO, Baracat MM, Urbano MR, Verri WA Jr, Porcu M, et al. N-acetylcysteine as an adjunctive treatment for smoking cessation: a randomized clinical trial. Braz J Psychiatry. 2020;42(5):519–26.
Arancini L, Bortolasci CC, Dodd S, Dean OM, Berk M. N-acetylcysteine for cessation of tobacco smoking: rationale and study protocol for a randomised controlled trial. Trials. 2019;20(1):555.
LaRowe SD, Mardikian P, Malcolm R, Myrick H, Kalivas P, McFarland K, et al. Safety and tolerability of N-acetylcysteine in cocaine-dependent individuals. Am J Addict. 2006;15(1):105–10.
LaRowe SD, Myrick H, Hedden S, Mardikian P, Saladin M, McRae A, et al. Is cocaine desire reduced by N-acetylcysteine? Am J Psychiatry. 2007;164(7):1115–7.
Amen SL, Piacentine LB, Ahmad ME, Li SJ, Mantsch JR, Risinger RC, et al. Repeated N-acetyl cysteine reduces cocaine seeking in rodents and craving in cocaine-dependent humans. Neuropsychopharmacology. 2011;36(4):871–8.
Mardikian PN, LaRowe SD, Hedden S, Kalivas PW, Malcolm RJ. An open-label trial of N-acetylcysteine for the treatment of cocaine dependence: a pilot study. Prog Neuropsychopharmacol Biol Psychiatry. 2007;31(2):389–94.
Smaga I, Wydra K, Frankowska M, Fumagalli F, Sanak M, Filip M. Cocaine self-administration and abstinence modulate NMDA receptor subunits and active zone proteins in the rat nucleus accumbens. Molecules. 2020;25(15):3480.
Schulte MHJ, Wiers RW, Boendermaker WJ, Goudriaan AE, van den Brink W, van Deursen DS, et al. The effect of N-acetylcysteine and working memory training on cocaine use, craving and inhibition in regular cocaine users: correspondence of lab assessments and Ecological Momentary Assessment. Addict Behav. 2018;79:24–31.
LaRowe SD, Kalivas PW, Nicholas JS, Randall PK, Mardikian PN, Malcolm RJ. A double-blind placebo-controlled trial of N-acetylcysteine in the treatment of cocaine dependence. Am J Addict. 2013;22(5):443–52.
Levi Bolin B, Alcorn JL 3rd, Lile JA, Rush CR, Rayapati AO, Hays LR, et al. N-Acetylcysteine reduces cocaine-cue attentional bias and differentially alters cocaine self-administration based on dosing order. Drug Alcohol Depend. 2017;178:452–60.
Duailibi MS, Cordeiro Q, Brietzke E, Ribeiro M, LaRowe S, Berk M, et al. N-acetylcysteine in the treatment of craving in substance use disorders: systematic review and meta-analysis. Am J Addict. 2017;26(7):660–6.
Grant JE, Odlaug BL, Kim SW. A double-blind, placebo-controlled study of N-acetyl cysteine plus naltrexone for methamphetamine dependence. Eur Neuropsychopharmacol. 2010;20(11):823–8.
Mousavi SG, Sharbafchi MR, Salehi M, Peykanpour M, Karimian Sichani N, Maracy M. The efficacy of N-acetylcysteine in the treatment of methamphetamine dependence: a double-blind controlled, crossover study. Arch Iran Med. 2015;18(1):28–33.
Acknowledgements
This study was supported by statutory funds from the Maj Institute of Pharmacology Polish Academy of Sciences, Kraków, Poland.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Smaga, I., Frankowska, M. & Filip, M. N-acetylcysteine in substance use disorder: a lesson from preclinical and clinical research. Pharmacol. Rep 73, 1205–1219 (2021). https://doi.org/10.1007/s43440-021-00283-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s43440-021-00283-7