
Abstract
Rate of force development (RFD) and impulse (IMP) are important mechanical measures of muscular performance but are relatively unused within the rehabilitation and performance community. Due principally to access to low-cost testing devices and understanding the utility of these measures. The aim of this study therefore was to quantify the reliability of various force–time variables using load-cell technology collected via isometric knee extension whilst constrained in an isokinetic device (CON90) or unconstrained on a physiotherapy plinth at 60 and 90 degree angles (UNCON60 and UNCON90). Thirty-two volunteers had their peak force (PF), RFD, peak RFD (PRFD), and IMP assessed across three protocols. For all variables, UNCON60 had the largest variability across all measures. PF and PRFD were found to have small variability (ICC > 0.67 and CV < 10%). With regards to RFD 2080 all three protocols were found to have moderate variability all ICCs above 0.75, however, all CVs were greater than 10% ranging from ~ 11%–22%. Finally, IMP 2080 was found to have moderate variability for both CON90 and UNCON90, the absolute consistency once more greater than 10% (~ 11%–25%). Using the constrained and unconstrained protocols, PF and PRFD can be measured reliably between trials with 90 degree knee position.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The innovation and evolution of medical management related to various orthopaedic injuries continues to progress. The concept of reintegration and readiness have garnered increasing attention in an attempt to diminish the risk of reinjury, and better profile a person’s relative capacity for a given task, skill, activity, or sport, than traditional testing strategies [16, 26, 29,30,31, 45, 47]. While readiness and reintegration are popular terms used in the athletic population, these concepts are equally as useful and important in the general population, when considering tasks such as the ability to recover balance during an unanticipated perturbation [28, 44, 48]. Regardless of the population, a subject’s performance profile should include a comprehensive battery of local and specific measures, such as muscular endurance or peak force production, as well as standardized functional movement tests, such as hop testing or single leg balance assessments [16, 26, 29,30,31, 45, 47]. These assessments typically include isolated tissue or joint performance objectified by a single maximal capacity of a contraction (peak force—PF) or the volume of repetitions completed at a given weight (muscular endurance). Such measures have been found of empirical value in evaluating a range of cohorts, from age-related strength changes in the lower extremity [22, 24, 25, 38, 39, 42, 43] to limb symmetry knee extension strength after anterior cruciate ligament reconstruction [22, 38, 39].
There is an emerging interest in investigating force–time characteristics as they are more closely correlated with tissue capacity and may provide better information about force production, than reporting maximal force alone [3, 8, 20, 25, 46, 48, 49]. In particular, rate of force development (RFD), the rate at which contractile elements of the muscle can develop force, and impulse (IMP), the time which force is exerted, are gaining clinical popularity. Measures of RFD and IMP have been shown to provide a more defined insight into neuromuscular characteristics, such as muscle–tendon unit (MTU) stiffness [8, 25], MTU physiology (such as arrangement and density of collagen fibers) [20, 48], nervous system capacity [3, 46, 49], and psychologic confidence [2, 11, 23, 29, 36]. Moreover, increases in rapid force production have been associated with improvements of performance in numerous tasks such as sprint speed and weightlifting [40, 41], along with activities of daily living, such as increases in walking speed or sit to stand actions [1, 6, 9]. Thus, RFD and IMP measurements may be more valuable both when describing risk and readiness post-injury, such as after anterior cruciate reconstruction [3], and when optimizing performance [4, 17,18,19].
Currently, RFD and IMP are relatively unused within rehabilitation and sports performance settings, primarily due to limited access to testing devices. The collection of RFD and IMP requires specialized equipment using particular hardware and software that analyses force in small-scale epochs. Devices such as force plates and isokinetic dynamometers are useful in collecting RFD and IMP, but have traditionally been available only in hospitals, research labs and human performance centres at a cost that is unfeasible for most clinicians. A more practical and cost-efficient approach to measuring force–time measures would be a load cell. Moreover, if this device is accurate in clinical testing scenarios such as on a physiotherapy plinth, it would further support its use in clinical environments. While a plethora of studies have examined the reliability of commercial isokinetic dynamometers [13, 33, 34], limited data exists concerning the reliability of knee extension RFD and IMP using a portable load cell [14]. Therefore, the primary aim of this study was to describe and compare the variability of an isometric knee extension test using a portable load-cell in two distinct layouts: (1) a constrained position with the rigid fixation using the seat and associated straps, and (2) an unconstrained position with no fixation on a physiotherapy plinth.
Methods
Participants
Thirty-two volunteers (14 males and 18 females: age: 31.8 ± 7.91 year, height: 170 ± 9.13 cm, body mass: 77.1 ± 23.9 kg) participated, and all reported their right limb as dominant (defined as the leg they would use to kick a ball). All individuals were deemed healthy according to their PAR-Q questionnaire, with no current health conditions that would limit strenuous exercise. Individuals were excluded if they had any prior surgical intervention that would limit maximal knee extension performance. All participants had the benefits and risks of the investigation explained to them verbally and in written form, and signed an informed consent before participation. The participants were informed that participation was voluntary and could withdraw at any time. Ethics approval for this study was obtained from the Auckland University of Technology Ethics Committee (19/447). Before testing all participants gave written informed consent.
Study Design
A cross-sectional, repeated measures design was used for comparative analysis of reliability for PF, RFD and IMP metrics during a maximal voluntary isometric contraction (MVIC) knee extension with a load cell device in constrained and unconstrained protocols. All participants attended a single testing session which consisted of three sequential rapid MVICs across three protocols. All data were collected by one researcher to reduce variability.
Load Cell Device
The load cell device was a wireless force measurement system comprising of a load cell device with wireless telemetry, with a relative affordability of ~ $1000 USD. Force data were collected at 1000 Hz via a custom-designed load cell device (Sports Performance Research Institute New Zealand Laboratories, Auckland University of Technology), interfaced with custom-designed data acquisition software (Matlab, Mathworks, USA).
Procedures
Data was collected using three ‘protocols’. These protocols involved varying degrees of knee flexion angle and constraint, or rigidity, the purpose of which was to simulate laboratory and clinical environments.
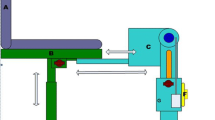
CON90 was defined as the Load Cell + Constrained + 90° (CON90—see Fig. 1a). The participant was seated upright in the chair of the isokinetic dynamometer (CSMi; Lumex, Ronkonkoma, NY) at a hip angle of 85°, with shoulder, waist, and thigh straps affixed to reduce body movement during contractions. The load cell was tethered to the isokinetic dynamometer and the individual’s lower leg ~ two cm superior to the lateral malleolus using a steel chain. The knee angle was measured using a goniometer and maintained at 90º flexion, throughout the set-up and trials, by shortening or lengthening the chain. The chair was adjusted to maintain both the centre of rotation just beyond the edge of the chair and that the line of force production was maintained in-line with the orientation of the load cell. The 60° knee flexion position, as seen and tested in Protocol-2 (description below), was not collected due to the inadequacy of appropriate angular fixation. There was no suitable fixation for the load cell by which the resistance to the force production was perpendicular to the attachment point on the shank, therefore only the 90° position was collected. The participant was instructed to place their non-testing limb behind the counterforce pad and hold the handles on both sides of the chair to further reduce instability. The computer, with software visible, was placed directly in front of the participant to be used for practice trials, feedback, and achieving the pretension threshold. The pretension mark for this device and protocol was 120 Newtons (N), while the collection threshold was 160 N (i.e., the trial initiation was established once the force produced was > 160 N).

Figures showing the constrained (CON90) and unconstrained (UNCON90). Note UNCON60 not shown
Participants were tested at 90° in both the constrained and unconstrained positions to assess if differences in reliability were due to restrictions of movement in the upper body. From a practical perspective, it would be far less practically viable in a practicing physiotherapy clinic if a more expensive system was needed to constrain the upper body movement. The second test looked at participants performing maximum extensions at 60° and 90° (both unconstrained) to allow for an analysis of the difference in variance between these angles. This was conducted as the preferred testing angle for maximal force is at 60°.
Protocols 2 and 3 both involved the use of a physiotherapy plinth (unconstrained), rather than the use of the isokinetic dynamometer chair. UNCON60 utilized the load cell + unconstrained + 60° knee position (UNCON60) while UNCON90 utilized the same load cell + unconstrained set up but at 90° (UNCON90). For both unconstrained protocols, the participant was seated on the edge of a clinical plinth (table), and allowed to self-select a position while meeting the following criteria: (1) the participant must maintain this position throughout the trials; (2) the participant must hold the sides of the table; and, (3) the participant must shift towards the side of the table being tested so that the line of force aligned to the fixation point which was previously located.
Once seated and comfortable, the participant was sat on the edge of the plinth two cm superior to the lateral malleolus using a low compliance, steel chain, and a towel was placed under the distal thigh between the thigh and table. The plinth had a very rigid, uncomfortable, surface edge which was found to be problematic in pilot testing. The participant was asked to create a submaximal force (to achieve the true testing position and remove any slack in the chain) and the knee angle was measured using a goniometer to either 60° or 90° respectively, according to the intended position. Every participant completed both knee joint angles positions; however, the order was varied from session to session and from participant to participant. Order was randomly assigned to the participant based on the order of enrolment. Note, the chain to table fixation was different for the two knee positions to accommodate for the different ranges of motion.
Throughout practice trials, the participant was allowed to move and change position, however, once the testing began, no further changes were allowed, and the participant’s position was recorded for future testing sessions. As with CON90, the computer monitor was placed within view of the participant for purposes of practice trials, pretension, and feedback. The pretension mark for this device and protocol was 120 N, while the collection threshold was 160 N.
Each participant warmed up by cycling at low to moderate resistance using a self-selected pace for three to five minutes. They were then placed in the constrained protocol for familiarization. Familiarization occurred at every session using the constrained protocol, regardless of the randomized testing order, and included a series of progressive, ascending force output isometric knee extension trials, which culminated with at least one trial at maximal effort. The participant was given verbal and visual feedback during these trials regarding performance and education was implemented in cases of confusion or to troubleshoot positioning. After familiarization trials were completed, the participant was asked to dismount the chair, and a five-minute rest commenced before the initiation of data collection. As part of the familiarization and practice trials, specific instruction and verbal cueing were explained and used. The term ‘fast’ in “fast and hard” was consistently emphasized throughout all testing occasions, which is necessary when collecting RFD and IMP metrics as opposed to maximal force [14]. The participant was given strong verbal encouragement throughout each trial.
After the familiarization trials and five-minute rest, the participant was then placed into a randomly allocated protocol and knee position. The participant was allowed up to five practice trials including verbal and visual feedback, and the participant was encouraged to complete at least one maximal effort contraction before finishing the practice trials. For testing trials, the participant was told to achieve the determined pretension state and hold at this level for two seconds by slowly extending the knee into the strap and visualizing the force line on the monitor. Once the force curve was steady at the pretension threshold, the primary investigator (PI) would begin a count down from 3 (“3–2-1-Go-Go-Go-Go-Go-Stop”). The participant was instructed to begin the MVIC at any point after “1” and maintain the contraction until told to “stop”.
Each participant completed three testing trials at each protocol. Due to the small testing domain, the rest between repetitions was set at 10 to 30 s based on participant preference as described by previous researchers [32]. The force–time curve was visually inspected for large deviations in force production (> 250 N from prior trials), or notable countermovement, or inconsistencies in the pretension state, as these would dramatically impact aspects of data analysis, such as onset of contraction and artificially inflated RFD metrics. If evident, these false contractions were removed, and the trial repeated with verbal and visual feedback to the participant. The testing order was dictated by random order assignments for each participant.
Data Processing
Force data were collected at 1000 Hz using the Load Cell device. Raw unfiltered force–time data was exported for subsequent analysis in CSV format. Only right leg (dominant leg) data were utilized for analysis. The data were then imported and analyzed in MATLAB (MathWorks, Natick, MA), using a custom algorithm. Each trial was trimmed to length to include a pretension period of at least 0.5 s, force onset, isometric contraction for at least one second, and a force offset (see Fig. 2). The onset of force was defined as an increase in force that was greater than three standard deviations (3 SD) of force calculated from the 350 ms pretension window within 1 s before the contraction [7, 12, 13, 29]. A modified version of this method was used; where the onset of force was calculated as the first 3 SD threshold crossing from the location of peak force working backwards. Outputs were visually assessed for methodological outliers, which were removed from the analysis. Peak force (PF) was determined as the absolute maximum force recorded during the entirety of the two-second contraction; and 20% and 80% of this peak force were calculated. All further variables of interest were then determined from within the time interval created by the 20%–80% peak force thresholds (time2080), as described previously [10, 15] (Fig. 2). This procedure was used to remove more volatile components of the contraction epoch (the first and last 20% of the contraction) in order to enhance stability and accuracy of the metric [10, 15]. Rate of force development (RFD2080) was the average slope over the epoch (F/t) and impulse (IMP2080) was the area under the force–time curve, during time2080. Peak rate of force development (PRFD) was calculated using a 10 Hz 4th order low-pass Butterworth filter.

Visual representation of the load cell force–time data
Statistical Analysis
All statistical analysis was conducted using RStudio IDE (Version 1.4.869, 2009 – 2020 RStudio, PBS). The statistical analysis explored the intrasession reliability of an isometric knee extension test using a portable load-cell in two distinct layouts. Each subject completed a series of at least three trials at each protocol. If less than three trials were conducted, the subject was removed from any further analysis. Outlier analysis was conducted using intrasession, intra-subject z-scores. Boxplots were used to visually check for outliers of the calculated z-scores (rstatix version: 0.6.0). Only extreme outliers were removed from the analysis. Normality of each intrasession variable was confirmed using Shapiro Wilks test. Mean and standard deviations were calculated. There was no gender bias and no significant inter-limb differences observed, during analysis, therefore analysis is of the right limb only, and genders were combined for all analyses. The within-subject coefficient of variation (CV), and intra-class correlation coefficient (ICC) (two-way mixed effects, absolute agreement, type = single) were used to explore systematic change, absolute and relative consistency respectively. ICC findings were interpreted based on the following: < 0.5 = poor; 0.5–0.75 = moderate; 0.75–0.90 = good; and > 0.90 = excellent [5, 27]. In terms of overall variability, an ICC < 0.67 and CV > 10% were deemed as having large variability, moderate variability when either the ICC > 0.67 or the CV < 10%, but not both, and small variability when ICC > 0.67 and CV < 10% [5, 27].
Results
In terms of the three trials there does not appear to be any systematic bias across variables and conditions (see Table 1). For all variables, UNCON60 was found to have the lowest ICC, and largest CV, values when compared to the other two protocols. PF was found to have “excellent” ICC magnitudes and small variability across all protocols (CV = 3.20%–4.50%). Excellent relative consistency and small variability was also observed for PRFD in the Trial 3–2 comparison for the CON90 and UNCON90 protocols. With regards to RFD2080 all three protocols were found to have moderate variability all ICCs above 0.75, however, all CVs were greater than 10% ranging from ~ 11%–22%. Finally, IMP2080 was found to have moderate variability for both CON90 and UNCON90, the absolute consistency once more, greater than 10% (~ 11%–25%).
Discussion
Of interest to the authors was the variability of an isometric knee extension test with load cell derived force–time variables as determined via three different protocols, which differed in terms of level of constraint and angle of assessment. The main findings were: 1) there was little evidence of systematic bias (familiarisation, learning effect, warm-up, etc.) using the described protocols; 2) PF and PFRD were found to have small variability; 3) RFD2080 and IMP2080 across all three protocols were found to have moderate variability all ICCs above 0.75, however, all CVs were greater than 10%; and, 4) UNCON60 was found to have the greatest variability compared to the other two protocols.
With regards to the assessment of PF, the low variability across all three protocols was not unexpected given the results of other researchers [21, 29, 37] and the inherent stability of the measure. However, an interesting finding was the low variability of the PRFD measure for both the CON90 and UNCON90, especially in light of the other RFD and impulse measures.
RFD2080 and IMP2080 were found to have moderate variability (CON90 and UNCON90) due to their ‘good’ and ‘excellent’ relative consistency, however, their absolute consistency was greater than 10% for both protocols (~ 11%–25%). These findings were similar to previously published research [35] investigating 70 degree and 100 degree positions, “good” relative consistency yet large absolute consistency for RFD (ICC = 0.82–0.87, CV 11.8%–14.9%) and IMP (ICC = 0.84–0.88, CV = 23.6%–29.6%) were associated with these testing positions. Based on the high typical error (CVs), it would seem that RFD2080 and IMP2080 are sensitive to system changes and the protocols used to quantify these measures need to be reviewed and refined further in order to better understand the variability associated with the measure i.e. biological or technological.
Finally, UNCON60 produced the largest variability (CV%) than both CON90 and UNCON90. Although the 60 degree position may be more useful for quantifying peak force data, the 60 degree position provided less rigidity due to the position, which could account for the larger variance in data across trials. Furthermore, it was subjectively reported that the UNCON60 position “felt” more unstable and less rigid by participants. From these finding it would seem that, knee angle should be considered when using the load cell for quantification of force capability.
Limitations
It is acknowledged that there are limitations to the current study. First, similar to previous reports, nuances and limitations in collecting RFD and other rapidly generated force variables are difficult to fully eliminate. These include the limitations associated with pretension prior to contraction onset. Previous researchers have identified reductions in force onset accuracy in performing isometric tests associated with a pretension state before the initiation of the force output [29]. Nonetheless, the study design and apparatus offered no other plausible solutions to this dilemma. It should also be noted that while a sample of convenience was recruited, an overwhelming majority of these individuals were very active regarding physical exercise, and may present different outcomes when compared to less active counterparts. Finally, it is worth acknowledging that the data analysis procedures used in this study also presented potential limitations to practical use. The method used to identify contraction onset and the subsequent 20–80% PF window was effective for the majority of testing sessions. However, in poor performance trials, specifically those with multiple force peaks within the testing window, the algorithm was occasionally less accurate than manual selection strategies, leading to a manual review of each trial for quality assurance. If this device is to be used in clinical medicine, it must be explored in situations that resemble such situations to enhance its potential.
Conclusion
The collection of PF and PRFD on a portable low budget/high utility load cell can be completed reliably between trials when using a constrained method (such as an isokinetic dynamometer fixation set up) or on an unconstrained protocol (such as a physiotherapy plinth) when the knee is tested at 90 degrees. However, RFD and IMP produced higher variabilities over all positions, these protocols therefore need to be reviewed and refined further in order to achieve acceptable reproducibility. Also, assessment range of motion needs to be considered when using the load cell for quantification of force capability given the 60 degree findings. Finally, given the high sampling frequency (1000 Hz), portability, and the relative affordability (~ $1000 USD), it would seem that a custom-designed load cell device, offers an effective alternative to more expensive dynamometry for measuring force capability during knee extension tasks.
Data Availability
The authors confirm the data supporting the findings of this study are available within the article. Raw data that support the findings of this study are available from the corresponding author, upon reasonable request.
References
Aagaard P, Magnusson PS, Larsson B, Kjaer M, Krustrup P. Mechanical muscle function, morphology, and fiber type in lifelong trained elderly. Med Sci Sports Exerc. 2007;39(11):1989.
Andersen LL, Aagaard P. Influence of maximal muscle strength and intrinsic muscle contractile properties on contractile rate of force development. Eur J Appl Physiol. 2006;96(1):46–52.
Angelozzi M, Madama M, Corsica C, Calvisi V, Properzi G, McCaw ST, Cacchio A. Rate of force development as an adjunctive outcome measure for return-to-sport decisions after anterior cruciate ligament reconstruction. J Orthop Sports Phys Therap. 2012;42(9):772–80.
Beckham G, Mizuguchi S, Carter C, Sato K, Ramsey M, Lamont H, Hornsby G, Haff G, Stone M. Relationships of isometric mid-thigh pull variables to weightlifting performance. J Sports Med Phys Fitness. 2013;53(5):573–81.
Bradshaw E, Hume P, Calton M, Aisbett B. Reliability and variability of day-to-day vault training measures in artistic gymnastics. Sports Biomech. 2010;9(2):79–97.
Brown M, Sinacore DR, Host HH. The relationship of strength to function in the older adult. J Gerontol Ser A Biol Sci Med Sci. 1995;50:55–9.
Buckthorpe M, Roi GS. The time has come to incorporate a greater focus on rate of force development training in the sports injury rehabilitation process. Muscles Ligaments Tendons J. 2017;7(3):435.
Burgess KE, Connick MJ, Graham-Smith P, PearsonSJ. Plyometric vs. isometric training influences on tendon properties and muscle output. J Strength Condition Res. 2007;21(3):986.
Clark DJ, Manini TM, Fielding RA, Carolynn Patten. Neuromuscular determinants of maximum walking speed in well-functioning older adults. Exp Gerontol. 2013;48(3):358–63.
Cobian DG, Koch CM, Amendola A, Williams GN. Knee extensor rate of torque development before and after arthroscopic partial meniscectomy, with analysis of neuromuscular mechanisms. J Orthopaed Sports Phys Therap. 2017;47(12):945–56.
Crameri R, Aagaard P, Qvortrup K, Langberg H, Olesen J, Kjaer M. Myofibre damage in human skeletal muscle: Effects of electrical stimulation versus voluntary contraction. J Physiol. 2007;583(1):365–80.
De Ruiter C, Kooistra RD, Paalman MI, de Haan A. Initial phase of maximal voluntary and electrically stimulated knee extension torque development at different knee angles. J Appl Physiol. 2004;97(5):1693–701.
De Ruiter CJ, Van Leeuwen D, Heijblom A, Bobbert MF, de Haan A. Fast unilateral isometric knee extension torque development and bilateral jump height. Med Sci Sports Exerc. 2006;38(10):1843–52.
Duchateau J, Baudry S. Maximal discharge rate of motor units determines the maximal rate of force development during ballistic contractions in human. Front Hum Neurosci. 2014;8:234.
Dudley-Javoroski S, Littmann AE, Iguchi M, Shields RK. Doublet stimulation protocol to minimize musculoskeletal stress during paralyzed quadriceps muscle testing. J Appl Physiol. 2008;104(6):1574–82.
Ellman MB, Sherman SL, Forsythe B, LaPrade RF, Cole BJ, Bach BR. Jr. Return to play following anterior cruciate ligament reconstruction. JAAOS. 2015;23(5):283–96.
Haff GG, Carlock JM, Hartman MJ, Kilgore JL, Kawamori N, Jackson JR, Morris RT, Sands WA, Stone MH. Force-time curve characteristics of dynamic and isometric muscle actions of elite women olympic weightlifters. J Strength Condition Res. 2005;19(4):741.
Haff GG, Jackson JR, Kawamori N, Carlock JM, Hartman MJ, Kilgore JL, Morris RT, Ramsey MW, Sands WA, Stone MH. Force-time curve characteristics and hormonal alterations during an eleven-week training period in elite women weightlifters. J Strength Condition Res. 2008;22(2):433–46.
Haff GG, Ruben RP, Lider J, Twine C, Cormie P. A comparison of methods for determining the rate of force development during isometric midthigh clean pulls. J Strength Condition Res. 2015;29(2):386–95.
Hakkinen K, Alen M, Kraemer WJ, Gorostiaga E, Izquierdo M, Rusko H, Mikkola J, Häkkinen A, Valkeinen H, Kaarakainen E, Romu S, Erola V, Ahtiainen J, Paavolainen L. Neuromuscular adaptations during concurrent strength and endurance training versus strength training. Eur J Appl Physiol. 2003;89(1):42–52.
Hernández-Davó JL, Sabido R. Rate of force development: reliability, improvements and influence on performance: a review. Eur J Hum Mov. 2014;33:46–69.
Ithurburn MP, Paterno MV, Ford KR, Hewett TE, Schmitt LC. Young athletes with quadriceps femoris strength asymmetry at return to sport after anterior cruciate ligament reconstruction demonstrate asymmetric single-leg drop-landing mechanics. Am J Sports Med. 2015;43(11):2727–37.
Jenkins N, Housh TJ, Traylor DA, Cochrane KC, Bergstrom HC, Lewis RW, Schmidt RJ, Johnson GO, Cramer JT. The rate of torque development: a unique, non-invasive indicator of eccentric-induced muscle damage? Int J Sports Med. 2014;35(14):1190–5.
Klass M, Baudry S, Duchateau J. Age-related decline in rate of torque development is accompanied by lower maximal motor unit discharge frequency during fast contractions. J Appl Physiol. 2008;104(3):739–46.
Kubo K, Kanehisa H, Ito M, Fukunaga T. Effects of isometric training on the elasticity of human tendon structures in vivo. J Appl Physiol. 2001;91(1):26–32.
Kyritsis P, Bahr R, Landreau P, Miladi R, Witvrouw E. Likelihood of ACL graft rupture: not meeting six clinical discharge criteria before return to sport is associated with a four times greater risk of rupture. Br J Sports Med. 2016;50(15):946.
Lenetsky S, Brughelli M, Nates RJ, Cross MR, Lormier AV. Variability and reliability of punching impact kinetics in untrained participants and experienced boxers. J Strength Condition Res. 2018;32(7):1838–42.
Maffiuletti NA. Assessment of hip and knee muscle function in orthopaedic practice and research. JBJS. 2010;92(1):220–9.
Maffiuletti NA, Aagaard P, Blazevich AJ, Folland J, Tillin N, Duchateau J. Rate of force development: physiological and methodological considerations. Eur J Appl Physiol. 2016;116(6):1091–116.
Manske R, Reiman M. Functional performance testing for power and return to sports. Sports Health. 2013;5(3):244–50.
Morris RC, Hulstyn MJ, Fleming BC, Owens BD, Fadale PD. Return to play following anterior cruciate ligament reconstruction. Clin Sports Med. 2016;35(4):655–68.
Noorkõiv M,Nosaka K, Blazevich AJ. Neuromuscular adaptations associated with knee joint angle-specific force change. Med Sci Sports Exerc. 2014;46(8):1525–37.
Oranchuk DJ, Nelson AR, Storey AG, Cronin JB. Variability of regional quadriceps architecture in trained men assessed by B-mode and extended-field-of-view ultrasonography. Int J Sports Physiol Perform. 2020;15(3):430–6.
Oranchuk DJ, Neville JG, Storey AG, Nelson AR, Cronin JB. Variability of concentric angle-specific isokinetic torque and impulse assessments of the knee extensors. Physiol Measur. 2020;41(1):1–2.
Oranchuk DJ, Storey AG, Nelson AR, Neville JG, Cronin JB. Variability of multiangle isometric force-time characteristics in trained men. J Strength Condition Res. 2022;36(1):284–288.
Peñailillo L, Blazevich A, Numazawa H, Nosaka K. Rate of force development as a measure of muscle damage. Scand J Med Sci Sports. 2015;25(3):417–27.
Rodríguez-Rosell D, Pareja-Blanco F, Aagaard P, González-Badillo JJ. Physiological and methodological aspects of rate of force development assessment in human skeletal muscle. Clin Physiol Funct Imaging. 2018;38(5):743–62.
Schmitt LC, Paterno MV, Hewett TE. The impact of quadriceps femoris strength asymmetry on functional performance at return to sport following anterior cruciate ligament reconstruction. J Orthop Sports Phys Therap. 2012;42(9):750–9.
Schmitt LC, Paterno MV, Ford KR, Myer GD, Hewett TE. Strength asymmetry and landing mechanics at return to sport after ACL reconstruction. Med Sci Sports Exerc. 2015;47(7):1426.
Slawinski J, Bonnefoy A, Levêque JM, Ontanon G, Riquet A, Dumas R, Chèze L. Kinematic and kinetic comparisons of elite and well-trained sprinters during sprint start. J Strength Condition Res. 2010;24(4):896–905.
Stone MH, Sands WA, Carlock J, Callan S, Dickie D, Daigle K, Cotton J, Smith SL, Hartman M. The importance of isometric maximum strength and peak rate-of-force development in sprint cycling. J Strength Condition Res. 2004;18(4):878–84.
Thompson BJ, Ryan ED, Sobolewski EJ, Smith DB, Conchola EC, Akehi K, Buckminster T. Can maximal and rapid isometric torque characteristics predict playing level in division I American collegiate football players? J Strength Condition Res. 2013;27(3):655–61.
Thompson BJ, Ryan ED, Herda TJ, Costa PB, Herda AA, Cramer JT. Age-related changes in the rate of muscle activation and rapid force characteristics. Age. 2014;36(2):839–49.
Tillin NA, Pain MTG, Folland J. Explosive force production during isometric squats correlates with athletic performance in rugby union players. J Sports Sci. 2013;31(1):66–76.
Undheim MB, Cosgrave C, King E, Strike S, Marshall B, Falvey É, Franklyn-Miller A. Isokinetic muscle strength and readiness to return to sport following anterior cruciate ligament reconstruction: is there an association? A systematic review and a protocol recommendation. Br J Sports Med. 2015;49(20):1305.
Van Cutsem M, Duchateau J, Hainaut K. Changes in single motor unit behaviour contribute to the increase in contraction speed after dynamic training in humans. J Physiol. 1998;513(1):295–305.
van Melick N, van Cingel RE, Brooijmans F, Neeter C, van Tienen T, Hullegie W, Nijhuis-van der Sanden MW. Evidence-based clinical practice update: practice guidelines for anterior cruciate ligament rehabilitation based on a systematic review and multidisciplinary consensus. Br J Sports Med. 2016;50(24):1506–15.
Ventura A, Muendle B, Friesenbichler B, Casartelli NC, Kramers I, Maffiuletti NA. Deficits in rate of torque development are accompanied by activation failure in patients with knee osteoarthritis. J Electromyogr Kinesiol. 2019;44:94–100.
Vila-Chã C, Falla D, Correia MV, Farina D. Changes in H reflex and V wave following short-term endurance and strength training. J Appl Physiol. 2012;112(1):54–63.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. Open Access funding enabled and organized by CAUL and its Member Institutions.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
On behalf of all authors, the corresponding author states that there is no conflict of interest. There are no competing interests to disclose.
Ethics Approval
Ethics approval for this study was obtained from the Auckland University of Technology Ethics Committee (19/447). Before testing all participants gave written informed consent.
Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Consent to Publish
The authors affirm that human research participants provided informed consent for publication of the images in Figs. 1a, b.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Juneau, C.M., Oranchuk, D.J., Cahill, M. et al. Reliability and Utility of Load-Cell Derived Force–Time Variables Collected During a Constrained and Unconstrained Isometric Knee Extension Task on a Plinth. J. of SCI. IN SPORT AND EXERCISE 6, 81–89 (2024). https://doi.org/10.1007/s42978-022-00215-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s42978-022-00215-8