
Abstract
The study aims to compare the accuracy and reliability of tooth width measurements and Bolton ratios among plaster models (PM), cone beam computed tomography (CBCT), and intraoral scanner (IOS). This three-way comparison has not been previously conducted in existing studies. Seventy-two patients (aged 19–36) were selected from the University of Duhok clinic. PM, CBCT, and IOS images were obtained. Tooth widths and Bolton ratios were measured on plaster models and digital models (CBCT and IOS mages). Reliability was assessed by repeating all measurements after one month by the same examiner. The measurement accuracy and reliability were assessed through Repeated Measures ANOVA and ICC analysis. ICC results showed reliable measurements of tooth widths for PM, CBCT, and IOS (R = 0.90, 0.98, and 0.99 respectively). P-values for tooth widths and Bolton ratios between groups were all > 0.05. The ICC analysis revealed a strong correlation between the measurements of tooth widths and Bolton ratios obtained through the three distinct methods. PM, CBCT, and IOS can be used interchangeably in orthodontic diagnosis for accurate and reliable measurement of tooth widths and Bolton ratios (anterior and overall).
Article highlights
-
Accurate measurements The study confirms CBCT and IOS accuracy in measuring tooth widths, comparable to plaster models.
-
Tri-method consistency A unique comparison of CBCT, IOS, and plaster models demonstrates their strong agreement, ensuring reliable diagnostics.
-
Orthodontic application CBCT and IOS are reliable options for precise orthodontic assessments of tooth dimensions and Bolton ratios.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Introduction
Differences in tooth widths within the same jaw or between the upper and lower jaws can impact occlusion during orthodontic treatment [1]. However, this issue typically becomes apparent only in the final stages of treatment [2]. Tooth widths, especially in the anterior region, are considered crucial variables and have been identified as the seventh key to occlusion [3]. Multiple approaches have been suggested to evaluate disparities in tooth widths, although their utilization remains limited [4]. Studies conducted in the United States indicate that orthodontists frequently employ the Bolton ratio during the initial diagnosis of orthodontic cases [4]. This ratio plays a crucial role before orthodontic treatment, serving as a direct and significant indicator for assessing dental harmony and detecting irregularities in the upper or lower jaw, as well as the anterior or posterior regions [5].
The Bolton ratio directly affects overjet, overbite, crowding, and spacing [5]. Traditionally, this ratio has been manually calculated based on tooth widths (anterior/posterior width) using plaster models [6]. However, researchers are increasingly exploring modern digital alternatives and conducting tests and comparisons to determine their accuracy [7]. Digital methods are also favored for their ease, speed, and efficient image and data storage capabilities [7].
In orthodontic diagnosis, high-quality 3D digital models allow for the measurement of tooth widths and subsequent calculation of the Bolton ratio [8]. Several published studies have analyzed tooth widths using cone-beam computed tomography (CBCT), with plaster models (by alginate impressions) [9] or 2D/3D images serving as the gold standard for comparison [10], applied to either patients [10] or skulls [11]. The standardized orientation method, which involves measuring all teeth in the occlusal plane of the entire jaw, has been adopted [12]. However, the custom orientation method, based on the sagittal axis of each tooth individually, has not been used to accurately determine the anterior/posterior width.
The intraoral scanner (IOS) represents the latest innovation in dentistry for generating assessable 3D images [13]. Numerous tests have been conducted to determine the accuracy and reliability of this scanner in measuring tooth widths and the Bolton ratio, using plaster models [14] or 2D images as the gold standard [15]. However, no study has compared the accuracy and reliability of measuring tooth width and the Bolton ratio using CBCT and IOS images, with plaster models by C-silicone impressions (the gold standard) for comparison.
This study aims to be the first in the medical literature to conduct a three-way comparison of these methods.
2 Materials and methods
The study was conducted at the Department of Preventive, Orthodontic & Pedodontics, College of Dentistry, University of Duhok, from November 2021 to December 2022. It was a comparative study with three groups: the plaster model group [G(PM)], CBCT group [G(CBCT)], and the IOS group [G(IOS)]. Local Research Ethics Committee Approval was obtained from the Directorate of Health in Duhok governorate, Ministry of Health, Kurdistan Region (ID = 21082023-7-9), and the study was registered on the clinical trials database (www.clinicaltrials.gov) (ID = NCT05711160).
2.1 Sample size calculation
The sample size was determined using G*power 3.1.9.4 software (Universität Düsseldorf, Düsseldorf, Germany) with a power of 80%, and an effect size of 0.38 (based on a previous study [16]). The statistical analysis included a Repeated Measures ANOVA followed by a Bonferroni post hoc test to compare the different measurement methods. Therefore, a sample size of 72 patients was required, and informed consent was obtained from each participant.
2.2 Participants
A total of 200 patients at the Department of Preventive, Orthodontic & Pedodontics in the College of Dentistry, University of Duhok underwent examination. Out of these patients, 90 individuals who met the inclusion criteria received a detailed explanation of the study project. Information sheets were then distributed, and those patients who expressed their willingness to participate were asked to sign consent forms. Eventually, a total of 80 patients agreed to take part in the study.
Using a random selection process based on the predetermined sample size, the study selected a total of 72 patients. Each group consisted of 72 plaster models, 72 CBCT images, and 72 IOS images (Fig. 1). CBCT and IOS images, acquired from orthodontic patients at the Department of Preventive, Orthodontic & Pedodontics, College of Dentistry, University of Duhok, serve as diagnostic records for treatment initiation, extending beyond their research applications.

Diagram of the study groups
The inclusion criteria for participants included being between the ages of 19 and 36, having a complete set of permanent teeth, and not currently undergoing orthodontic treatment. On the other hand, exclusion criteria encompassed tooth agenesis or extractions, large restorations, anomalous tooth shapes, severe carious lesions or enamel defects, and severe crowding in the dentition (> 6 mm).
2.3 Participant’s preparation
All patients underwent scaling and polishing to ensure records of clean teeth, and all diagnostic records were taken by the same trained co-authors (M.A.M).
For plaster models, impressions of the upper and lower arches were recorded using C-silicone impression material (Zetaplus, Zhermack, Italy), and Orthodontic stone class III (Orthokal, Kalabhi®, Gujarat, India) was used to create the plaster models. CBCT scans of both jaws were taken using the Smart 3D apparatus (LARGEV, China) to obtain 3D images with the following parameters: voxel size of 100 μm, tube voltage of 100 kV, tube current 3 mA, and an exposure time of 13 s. Intraoral scans of the patient’s dentition were performed using the Intraoral scanner (Trios®, 3Shape dental systems, Copenhagen, Denmark) according to the manufacturers’ instruction.
2.4 Measurement of teeth widths and Bolton’s ratios
All maximum mesiodistal width measurements were taken from the left first molar to the right first molar for both the upper and lower jaw by the trained first author (S.K).
Tooth widths were measured using a digital electronic caliper for plaster models (Fisher Scientific International Inc., Hampton, NH, USA) [17] (Fig. 2).

Taking measurements of the tooth width on the plaster model
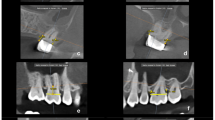
CBCT images were examined using smartV2-CD® software (LARGEV™, China). Images were carefully oriented for accuracy [18]. Each tooth was individually oriented, and sections were adjusted to ensure perpendicularity with the tooth’s longitudinal axis (Fig. 3). This orientation method allowed precise measurement of tooth width regardless of its position in the dental arch.


Measuring the tooth width on the digital model obtained from the IOS. a lower jaw, b upper jaw
Bolton’s ratios were calculated for each patient using Bolton’s formula to assess the anterior and overall ratios [20].
The minimum measurable value on a digital electronic caliper is 0.01 mm, for CBCT images it is 0.1 mm, and for intraoral scanner (IOS) images, it ranges from 0.1 to 0.2 mm.
2.5 Intra-observer reliability of measurements
To determine intra-observer reliability, all measurements were repeated after one month by the same examiner (S.K).
2.6 Blinding
In this trial, the concept of participant blindness did not apply. Consequently, the only instance where blindness was implemented was during the data analysis stage, specifically by one of the co-authors (M.R.S). To maintain the assessor’s blindness, the patients’ CBCTs, IOS, and plaster models were assigned unique serial numbers, and the allocation of data was kept concealed from the investigator throughout the statistical analysis phase.
2.7 Statistical analysis
Statistical analysis was performed using 2011 IBM SPSS Statistics software (IBM©, Version 20.0, Armonk, USA). Measurement reliability (intra-observer) was assessed using the intercorrelation coefficient (ICC). Kolmogorov–Smirnov Normality tests showed normal distributions of the collected data. Repeated Measures ANOVA was used to compare the three groups, followed by post hoc tests with Bonferroni correction. The Intraclass Correlation Coefficient type2 was employed to assess the agreement among measurements across groups.
3 Results
A total of 72 participants (29 females and 43 males) with an age range of 19–36 years (mean age 26.49 ± 1.16 years) were included in the study. All patients completed the study, and data analysis was performed for all participants. Table 1 presents the basic characteristics of the patients.
Tooth width measurements were taken from the left first molar to the right first molar in the upper and lower jaws. A total of 5184 tooth width measurements (1728 per group) were recorded for all participants.
3.1 Intra-observer reliability of measurements
Regarding the intra-observer reliability of measurements, strong associations were found between the initial measurements and those taken after one month for tooth width and Bolton’s ratios in each of the three study groups (Table 2).
3.2 Assessing tooth width differences among three groups
A Repeated Measures ANOVA test was conducted to evaluate the differences in mean values for teeth widths among the three groups: G(PM), G(CBCT), and G(IOS). The comparison showed no statistically significant differences in tooth widths among the groups (Tables 3 and 4).
Further analysis revealed no significant differences in mean tooth widths between the G(PM) and G(CBCT) groups or between the G(PM) and G(IOS). Similarly, no significant differences were found between the G(CBCT) and G(IOS) (Table 5).
Evaluation of agreement among the plaster models, CBCT, and IOS images using ICC is presented in Tables 3 and 4
3.3 Assessing Bolton ratio differences among three groups
Assessing the Bolton ratios, the G(CBCT) had slightly lower mean values compared to the plaster models group, but the differences were not statistically significant. The G(IOS) showed slightly higher mean values for the Bolton ratios, but again, no significant differences were observed (Table 6). Additional analysis indicated that there were no statistically significant differences in the mean Bolton ratios when comparing the G(PM) with the G(CBCT) or the G(PM) with the G(IOS). Likewise, there were no significant differences between the G(CBCT) and the G(IOS) (Table 7). Evaluation of agreement among the plaster models, CBCT, and IOS images using ICC is presented in Table 6.
4 Discussion
In the modern era, orthodontics plays a significant role in enhancing oral health and overall appearance [4]. One of the important advancements in orthodontic treatment is the utilization of CBCT and IOS technologies [8]. CBCT provides 3D imaging of the jaws and teeth, allowing for precise assessment and treatment planning [12]. IOS, on the other hand, utilizes digital scanning to capture accurate intraoral images without the need for traditional impressions [13]. Both CBCT and IOS offer numerous advantages in terms of diagnostic accuracy, treatment efficiency, patient comfort, and improved outcomes [8]. These advanced technologies have revolutionized the field of orthodontics by providing orthodontists with valuable tools for precise diagnosis, treatment planning, and monitoring progress [7].
The current study investigated the accuracy and reliability of using CBCT and IOS in measuring tooth widths and Bolton ratios, which are essential diagnostic elements in orthodontics. A comparison was made between the results obtained from these two techniques and the gold standard, which is plaster models by C-silicone. Plaster models, created from impressions using elastomeric materials, have been widely used as a benchmark in orthodontics due to their ability to accurately reproduce dental anatomy. These models offer a tangible and reproducible representation of the dentition, allowing for precise measurements of tooth dimensions and ratios. Over the years, they have been accepted as a reliable method for assessing tooth widths and Bolton’s ratio in orthodontic studies.
The utilization of plaster models as a gold standard in this comparative study ensures a robust foundation for evaluating the accuracy and reliability of modern imaging techniques, namely CBCT and IOS. Plaster models serve as a reference point against which the measurements obtained from CBCT and IOS images can be evaluated. This approach allows for a comprehensive assessment of the diagnostic potential and clinical applicability of these contemporary imaging methods.
The results of the present study showed that there were no statistically significant differences among the average tooth widths of the three study groups G(PM), G(CBCT), and G(IOS). When comparing G(PM) with G(CBCT), the largest difference between the mean widths was 0.03 mm, when comparing G(PM)with G(IOS), the maximum disparity between the mean widths was 0.02 mm. Additionally, when comparing G(CBCT) with G(IOS) the largest difference between the mean widths was 0.06 mm.
When comparing CBCT images with plaster models, slightly smaller mean tooth widths were observed in the CBCT images, which can be attributed to CBCT’s direct recording method without intraoral factors affecting the measurements. On the other hand, IOS images showed slightly larger mean tooth widths, possibly due to the effect of intraoral factors on scanning. However, these differences were not statistically or clinically significant. The ICC analysis of tooth widths’ results indicates a strong level of agreement among the plaster models, CBCT, and IOS images.
The results of this study suggest that the mean values of Anterior Bolton ratio did not exhibit any statistically significant differences among the three groups. A comparison of G(PM) and G(CBCT) yielded a mean difference of − 0.07%, whereas G(PM) and G(IOS) had a mean difference of − 0.01%. On the other hand, when comparing G(CBCT) and G(IOS), the mean difference was 0.05%. The results showed that there were no significant differences between the mean values of the Overall Bolton ratio among the three study groups. When comparing G(PM) with G(CBCT), the mean difference was − 0.07%. In the comparison between G(PM) and G(IOS), the mean difference was 0.001%. Lastly, when comparing G(CBCT) with G(IOS), the mean difference was 0.07%. The ICC analysis of the Bolton ratio results reveals a robust level of concordance among the plaster models, CBCT, and IOS images.
Previous studies in the medical literature compared diagnostic data extracted from CBCT or IOS images to a gold standard. No study conducted a three-way comparison of diagnostic data (tooth widths and Bolton ratios) among CBCT, IOS, and a gold standard (plaster models by C-silicon).
4.1 Comparison with CBCT studies
Regarding tooth widths, the present study agreed with the research conducted by Celikoglu et al.[21] and Kumar et al.[22], which compared CBCT with plaster models. Both studies concluded that CBCT can provide accurate tooth width values for all the groups studied. This is attributed to CBCT’s ability to directly capture data from the patient’s mouth, eliminating the influence of intraoral factors and impression materials that may impact data transfer from the patient to the diagnostician.
The present study differed from Hernandez et al.[23] and José et al. [24], which compared CBCT with 2D scanned plaster models, Furthermore, our results deviated from Kim et al.’s study [25], which compared CBCT with 3D scanned plaster models and plaster models. Although statistically significant differences were observed among the study groups, these differences were not clinically significant. The discrepancies can be attributed to the lack of clarification on their inclusion criteria in their studies. Additionally, they used a different measurement method on CBCT images compared to the present study, and Hernandez and José did not specify the Impression material used for obtaining the 2D scanned plaster models. Furthermore, Kim’s 3D models were derived from alginate impressions.
Regarding Bolton ratios, the present study aligned with Tarazona et al.’s [10] and Celikoglu et al.’s [21] studies, which compared CBCT with plaster models, as well as with Kumar et al.’s [22] and Kim et al.’s [26] studies, which compared CBCT with 3D scanned plaster models and plaster models. Both studies demonstrated that CBCT can accurately determine the anterior and overall Bolton ratios in all the groups studied. This alignment can be attributed to the use of plaster models as a gold standard for comparison with CBCT images.
4.2 Comparison with IOS studies
Regarding tooth widths, the results of the current study were consistent with the findings of Naidu et al. [19], Wiranto et al. [16], and Zhang et al. [27] who compared IOS with plaster models. They also agreed with Grünheid et al. [28] who compared IOS with 3D scanned plaster models and plaster models, and with Anne’s et al. [14] who compared IOS with stereolithographic models. These studies found no statistically significant difference in tooth width measurements between IOS and the other study groups. The agreement was attributed to the direct transfer of data from the patient’s mouth to the diagnosing doctor, as well as the confocal microscopy technology of the IOS.
Flügge et al. [29] and Camardella et al. [30] reported that IOS provides less accurate tooth width values compared to scanned plaster models and plaster models. They attributed this difference to factors related to the oral cavity, such as saliva, soft tissues, and the small size of the oral cavity. On the other hand, Tomita et al. [15] suggested that IOS is more accurate than plaster models in terms of tooth width measurements, but they used plaster models by alginate as a means of comparison.
Regarding the anterior and overall Bolton ratios, the results of the current study were in agreement with the studies by Naidu et al. [19] and Wiranto et al. [16]. These studies also found no statistically significant difference in Bolton ratio measurements between IOS and plaster models. This concurrence can be attributed to the use of the same gold standard in the current study, which is the plaster models.
In elucidating the equivalence in accuracy and reliability of dental measurements and Bolton’s ratio among traditional plaster models, CBCT images, and IOS images, we underscore the credibility of modern diagnostic methodologies. While plaster models offer limited orthodontic diagnostic insights, they impose substantial time constraints and storage demands. Additionally, transferring data between practitioners is cumbersome. In the context of IOS images, although they share a diagnostic role akin to plaster models, they present a significant advantage in terms of time efficiency and storage optimization.
CBCT images, on the other hand, assume a pivotal diagnostic role. They facilitate panoramic and cross-sectional imagery, cephalometric analyses, and diagnosis of impacted teeth. CBCT images afford meticulous precision, reliability, swift diagnosis, streamlined storage, and seamless data transfer, thereby encapsulating comprehensive orthodontic diagnostic information within a single acquisition.
Concerning the cost disparities across these diagnostic approaches, a dedicated study evaluating various devices and brands is requisite. This evaluation would provide a nuanced perspective on the financial considerations associated with each methodology, further enhancing our understanding of their practical implications.
In summation, the confluence of CBCT’s extensive diagnostic capacity, coupled with its precision, reliability, efficient time utilization, and data management, underscores its prominence. While acknowledging the diagnostic potential of IOS and the essential role of traditional plaster models, CBCT emerges as a singularly comprehensive tool for orthodontic diagnosis. Future endeavors, aimed at dissecting cost differentials among diagnostic modalities, necessitate meticulous examination across multiple devices and brands to yield an accurate assessment.
5 Limitations of the study
The study excluded teeth with composite or metal restorations, as well as prosthetic crowns or bridges. The width, depth, and length of the dental arch or the amount of overjet and overbite were not investigated. Blinding of the patients was not possible in this trial. However, this limitation is not expected to introduce bias since no patient-centered self-assessed outcomes were evaluated. The inter-examiner reliability was not assessed, and the evaluation of the impact of various CBCT imaging types or IOS devices on the extracted data quality was not undertaken.
6 Conclusions
The study demonstrates the comparable accuracy and reliability of tooth width measurements and Bolton ratios between plaster models (PM), cone beam computed tomography (CBCT), and intraoral scanner (IOS) methods. No significant differences were found among the three methods for both tooth widths and Bolton ratios. These results validate the diagnostic potential of CBCT and IOS as effective alternatives to traditional plaster models in orthodontic practice, providing clinicians with advanced tools for precise measurements. The findings encourage the integration of CBCT and IOS technologies into orthodontic diagnostics and treatment planning. Further research could focus on cost-effectiveness and device-specific considerations to enhance their practical implementation.
Data availability
Corresponding author M.R.S. For any additional data or any inquiries about the current data.
Abbreviations
- G:
-
Group
- ICC:
-
Intraclass Correlation Coefficient
- IOS:
-
Intraoral scanner
- PM:
-
Plaster models
- SD:
-
Standard deviation
- SPSS:
-
Statistical package for the social sciences
References
Proffit WR, Fields HW, Sarver DM (2019) Contemporary orthodontics. Elsevier, Philadelphia
Camardella LT, Ongkosuwito EM, Penning EW, Kuijpers-Jagtman AM, Vilella OV, Breuning KHJT (2020) Accuracy and reliability of measurements performed using two different software programs on digital models generated using laser and computed tomography plaster model scanners. Korean J Orthod 50:13–25. https://doi.org/10.4041/kjod.2020.50.1.13
Amuk NG, Karsli E, Kurt GJIO (2019) Comparison of dental measurements between conventional plaster models, digital models obtained by impression scanning and plaster model scanning. Int Orthod 17:151–158. https://doi.org/10.1016/j.ortho.2019.01.014
Alqahtani H (2023) A study to estimate tooth size discrepancy values specific to Saudi orthodontic patients: a systematic review and meta-analysis. Saudi Dental J. 35:270–274. https://doi.org/10.1016/j.sdentj.2023.03.006
Kong L, Li Y, Liu ZJCOI (2022) Digital versus conventional full-arch impressions in linear and 3D accuracy: a systematic review and meta-analysis of in vivo studies. Clin Oral Investig 26:5625–5642. https://doi.org/10.1007/s00784-022-04607-6
Roos Y (2018) Bolton comparison between Caucasian and Chinese populations. Volume Master of science. Dissertation, The University of Manitoba.
Tandon D, Rajawat J, Banerjee MJ (2020) Present and future of artificial intelligence in dentistry. J Oral Biol Craniofac Res 10:391–396. https://doi.org/10.1016/j.jobcr.2020.07.015
Majstorović NV, Živković SP, Glišić BR (2019) Dental arch monitoring by splines fitting error during orthodontic treatment using 3D digital models. Vojnosanit Pregl 76:233–240. https://doi.org/10.2298/VSP190515051E
Kau CH, Littlefield J, Rainy N, Nguyen JT, Creed BJAO (2010) Evaluation of CBCT digital models and traditional models using the Little’s index. Angle Orthod 80:435–439. https://doi.org/10.2319/083109-491.1
Tarazona B, Llamas JM, Cibrián R, Gandía JL, Paredes VJ (2012) Patología Oral y Cirugía Bucal: evaluation of the validity of the Bolton index using cone-beam computed tomography (CBCT). Med Oral Patol Oral Cir Bucal 17:e878. https://doi.org/10.4317/medoral.18069
Baumgaertel S, Palomo JM, Palomo L, Hans MG (2009) Reliability and accuracy of cone-beam computed tomography dental measurements. Am J Orthod Dentofacial Orthoped 136:19–25. https://doi.org/10.1016/j.ajodo.2007.09.016
Alam MK, Shahid F, Purmal K, Khamis MF (2015) Cone-beam computed tomography evaluation of Pont’s index predictability for Malay population in orthodontics. J Nat Sci Biol Med 6:S113. https://doi.org/10.4103/0976-9668.166106
Afrashtehfar KI, Alnakeb NA (2022) Accuracy of intraoral scanners versus traditional impressions: a rapid umbrella review. J Evid Based Dent Pract. 22(3):101719. https://doi.org/10.1016/j.jebdp.2022.101719
Cuperus AMR, Harms MC, Rangel FA, Bronkhorst EM, Schols JGJH (2012) Dental models made with an intraoral scanner: a validation study. Am J Orthod Dentofacial Orthop 142:308–313. https://doi.org/10.1016/j.ajodo.2012.03.031
Tomita Y, Uechi J, Konno M, Sasamoto S, Iijima M (2018) Accuracy of digital models generated by conventional impression/plaster-model methods and intraoral scanning. Dent Mater J 37(4):628–633. https://doi.org/10.4012/dmj.2017-208
Wiranto MG, Engelbrecht WP, Nolthenius HET, van der Meer WJ, Ren YJ (2013) Validity, reliability, and reproducibility of linear measurements on digital models obtained from intraoral and cone-beam computed tomography scans of alginate impressions. Am J Orthod Dentofacial Orthop 143:140–147. https://doi.org/10.1016/j.ajodo.2012.06.018
Mullen SR, Martin CA, Ngan P, Gladwin MJA (2007) Accuracy of space analysis with emodels and plaster models. Am J Orthod Dentofacial Orthop 132:346–352. https://doi.org/10.1016/j.ajodo.2005.08.044
Tonea M, Ivanciu C, Trascu C et al (2016) Comparative dimensional study between panoramic X-ray (OPG) and cone beam CT (CBCT). ARS Med Tomitana 22:196–202. https://doi.org/10.1515/arsm-2016-0033
Naidu D, Freer TJ (2013) Validity, reliability, and reproducibility of the iOC intraoral scanner: a comparison of tooth widths and Bolton ratios. Am J Orthod Dentofacial Orthop. 144(2):304–310. https://doi.org/10.1016/j.ajodo.2013.04.011
Bolton WAJ, Wainright WA (1958) Disharmony in tooth size and its relation to the analysis and treatment of malocclusion. Angle Orthod 28(2):113–130. https://doi.org/10.1043/0003-3219(1958)028%3c0113:DITSAI%3e2.0.CO;2
Celikoglu M, Nur M, Kilkis D, Sezgin OS, Bayram M (2013) Mesiodistal tooth dimensions and anterior and overall Bolton ratios evaluated by cone beam computed tomography. Aust Orthod J 29:153–158. https://doi.org/10.3316/informit.915237045181596
Kumar AA, Phillip A, Kumar S et al (2015) Digital model as an alternative to plaster model in assessment of space analysis. J Pharm Bioallied Sci 7:S465. https://doi.org/10.4103/0975-7406.16350
Hernandez Y, Tarazona B, Zamora N, Cibrian R, Gandia JL, Paredes VJOR (2015) Comparative study of reproducibility and accuracy in measuring mesiodistal tooth sizes using three different methods: 2D digital, 3D CBCT, and 3D CBCT segmented. Oral Radiol 31:165–172. https://doi.org/10.1007/s11282-015-0204-x
San José V, Bellot-Arcís C, Tarazona B et al (2017) Dental measurements and Bolton index reliability and accuracy obtained from 2D digital, 3D segmented CBCT, and 3D intraoral laser scanner. J Clin Exp Dent 9:e1466. https://doi.org/10.4317/jced.54428
Kim J, Heo G, Lagravère MO (2014) Accuracy of laser-scanned models compared to plaster models and cone-beam computed tomography. Angle Orthod 84:443–450. https://doi.org/10.2319/051213-365.1
Kim J, Lagravére MO (2016) Accuracy of Bolton analysis measured in laser scanned digital models compared with plaster models (gold standard) and cone-beam computer tomography images. Korean J Orthod 46:13–19. https://doi.org/10.4041/kjod.2016.46.1.13
Zhang F, Suh K-J, Lee K-M (2016) Validity of intraoral scans compared with plaster models: an in-vivo comparison of dental measurements and 3D surface analysis. PLoS One 11:e0157713. https://doi.org/10.1371/journal.pone.0157713
Grünheid T, McCarthy SD, Larson BE (2014) Clinical use of a direct chairside oral scanner: an assessment of accuracy, time, and patient acceptance. Am J Orthod Dentofacial Orthop 146:673–682. https://doi.org/10.1016/j.ajodo.2014.07.023
Flügge TV, Nelson K, Schmelzeisen R, Metzger MC (2013) Three-dimensional plotting and printing of an implant drilling guide: simplifying guided implant surgery. J Oral Maxillofac Surg 71:1340–1346. https://doi.org/10.1016/j.joms.2013.04.010
Camardella LT, Vilella OV, van Hezel MM et al (2017) Accuracy of stereolithographically printed digital models compared to plaster models. J Orofac Orthop 78:394–402. https://doi.org/10.1007/s001090000086
Acknowledgements
Not applicable.
Funding
This research received no external funding.
Author information
Authors and Affiliations
Contributions
Conceptualization, SKK, and AMM; methodology, MRS, and AMM; Statistical analysis, MRS; validation, SKK, AMM, and MRS; formal analysis MRS; investigation, SKK; resources, SKK; data curation, MRS; writing original draft preparation, AMM, and MRS; writing review and editing, SKK; visualization, MRS; supervision, SKK; project administration, AMM All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no relevant financial or non-financial interests to disclose.
Institutional review board statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Local Research Ethics Committee from the Directorate of Health in Duhok governorate, Ministry of Health, Kurdistan Region (ID = 21082023-7-9)).
Informed consent
Informed consent was obtained from all subjects involved in the study.
Consent for publication
Not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Khalil, S.K., Mudhir, A.M. & Sirri, M.R. Accuracy of CBCT and intraoral scanner images for measuring tooth widths and Bolton’s ratio: a comparative study with gold standard (plaster models) in Duhok’s adult population. SN Appl. Sci. 5, 257 (2023). https://doi.org/10.1007/s42452-023-05483-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s42452-023-05483-9