
Abstract
This study reports about a new ion chromatography method for the detection of chloride ions in sweat as an alternative to the gold standard of the chloridometer. Information about necessary materials, required preparations, reference ranges, advantages and disadvantages of this method is provided. We finally demonstrate that this method is useful to screen for cystic fibrosis in sweat samples.
Article Highlights.
-
A new ion chromatography method for detection of chloride ions in sweat is described
-
References ranges for this method are given
-
Advantages and disadvantages are discussed
-
The usefulness of this method is shown in 145 sweat samples
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
Cystic fibrosis (CF) also termed mucoviscidosis is a monogenic autosomal recessive inherited disease within the Cystic Fibrosis Transmembrane Conductance Regulator (CFTR) gene affecting at least 100,000 people worldwide [1]. Actually, several newborn screening strategies are in use that either rely on the measurement of immunoreactive trypsinogen (IRT) from dried blood spots followed by genetic testing for CFTR mutations, or alternatively by performing a sweat chloride test that is considered as the gold standard for early diagnosis of CF [1]. Yet, the diagnosis of CF remains a challenge because different and more declines in IRT quantities are associated with more severe CFTR variants and the penetrance of the more than 2000 different CFTR mutations can result in different disease phenotypes that have promoted a reconsideration of the diagnosis criteria in the last years [2,3,4]. In addition, the sweat test shows a wide variability, which depends on age, sex, CFTR mutations, and the sweat sample collected [5].
Nevertheless, universal screening of newborn babies for CF using the sweat chloride test is done in many countries following approved procedural guidelines published by established, international Institutes such as the Clinical and Laboratory Standards Institute Guidelines [3, 6]. However, a cross-sectional cohort study using a standardized questionnaire administered in loco to the staff responsible for conducting sweat test in 14 centers in the state of Sao Paulo revealed that there is no uniformity in the sweat test procedure [7]. In particular, the quantification of chloride levels was done either by coulometry, flame photometry, conductivity, or manual titration in which obsolete noncertified clinical chemistry equipment was used during the measuring procedure resulting in adequately carried out sweat test [7].
To increase the reliability of the sweat test, we developed a novel method that relies on ion chromatography requiring only a micro sample of 5–10 µl of sweat. We demonstrate that this method is robust allowing us to measure chloride in the range between 2.82 and 141.0 mmol/l with an accuracy of < 0.3% standard deviation (SD). In the following we present a method that is a good alternative to the existing analytical methods.
2 Materials and methods
2.1 Sample storage and chemicals
All samples were stored at 2–8 °C and thawed at room temperature prior to analysis. A chloride standard stock of 1000 g/l was obtained from Bernd Kraft Laboratory Chemicals (Oberhausen, Germany). The sweat quality controls (QCs) for chloride at concentrations of 23, 49 and 100 mmol/l were obtained from Invicon Diagnostic Concepts GmbH (Munich, Germany). The chemicals for preparing the diluent and eluent were obtained from VWR International GmbH (Hanover, Germany) and prepared in deionized water. Double deionized water was prepared on a RO-1100ED integrated electro-deionization system (stakpure, Niederahr, Germany) and additionally purified on an ELGA PURELAB flex system (Veolia, Leipzig, Germany). All samples were retrospective analyzed in an anonymous fashion with the aim to increase the quality of diagnostics.
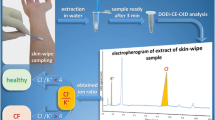
2.2 Sampling methodology
For weld sampling, the electrodes were directly attached to the patients’ arm before the sampling process starts, while in the iontophoresis the sweat was collected on a filter or disc containing 1.5% (w/w) pilocarpine (i.e. the pilogel) attached to two electrodes allowing optimal sweat transdermal stimulation with the sweat gland [8, 9]. The pilogel contains trisodium citrate, which is an excellent buffer in an acidic environment. At the cathode, the iontophoretic accumulation of alkali is reduced by increasing concentrations of pilocarpine that acts in a slightly alkaline environment as an effective buffer. Up to 30 µl of sweat was obtained in this way from each patient. In the results chapter, some more data on sweat analysis and patient’s characteristics are given.
2.3 Sample preparation and analytical conditions
10 µl of sweat was diluted in 3 ml of 2.5 mM NaOH in a tube and vortexed for 1 min. Subsequently, 20 µl of the sample was injected into the ion chromatography autosampler using the following instrumental setup: (i) Conductivity detector: Metrohm 882 Compact IC plus equipped with a Metrohm 771 IC Compact Interface and a Metrohm 863 Compact autosampler (Metrohm, Fiderstadt, Germany), (ii) Separation column: Metrosep A Supp 5–250/4.0 (Metrohm), (iii) Pre-column: Metrosep A Supp 1 Guard/4.6 (Metrohm), (iv) Column flow: 0.7 ml/min. The solutions used in chromatography were (i) Regeneration solution (5.32 ml H2SO4 dissolved in 1000 ml H2O), Stock eluent solution (16.96 g Na2CO3 and 4.20 g NaHCO3 dissolved in 500 ml H2O), and Eluents for anions separation (20 ml stock eluent were added to 1800 ml H2O).
2.4 Ethics
The samples of this study were taken due to a clinical indication and examined within the framework of quality management for the introduction of a new method. The use of leftover samples together with data from clinical routine submitted with the lab order is covered in North Rhine-Westphalia (NRW) by the Data Protection Act NRW §6 "Datenverarbeitung für wissenschaftliche Zwecke Abs. (2) und Abs. (3)“. During data handling, all personal information was anonymized. Therefore, no separate ethics vote is required for this study.
3 Results
3.1 Data of the ion chromatography method
The results of the validation for chloride in sweat are depicted in Fig. 1, showing that all parameters have the best fit to a polynomial curve over the entire measurement range.

Determination of chloride in sweat using ion chromatography
The most important characteristic analytical data for the separation of chloride in sweat are summarized in Table 1 and data on quality control accuracy from QC samples (low, medium, and high) are given in Table 2.
In a next step, we compared the results obtained by a standardized chloridometer measurement with our results obtained by ion chromatography methodology. We found that both methods are absolutely comparable (Fig. 2). There were no deviations or outliers. Linear regression showed a linear relationship of R2 = 0.996 between the two methods. The equation for calculation of chloride concentration by this method is y = 0.9962x–0.318 with r = 0.9964, DF = 3, and two-tailed p-value = 0.0003).

Comparison of measured chloride concentrations measured by chloridometer and ion chromatography (n = 13)
3.2 Testing of the ion chromatography method in daily routine
We next analysed the protocol for its routine use in a total of 145 samples that were collected from patients older than 6 months suspected to have CF (Fig. 3). The obtained values of each sample were subsequently scored for the presence of CF following a standardized reference scoring system, in which sweat chloride values during infancy are scored as: < 30 mmol/l considered normal; 30–59 mmol/l intermediate range for CF, and > 60 mmol/l diagnostic indicative for CF [1].

Measured chloride concentrations in 145 sweat samples taken from patients screened for cystic fibrosis
Another point is the selectivity of the analysis. The most important selectivity tests were carried out showing that the method has a good resolution without interference to F−, NO2, Br−, NO3− and SO42− that can potentially interfere with the measurement using chloridometer (Fig. 4), suggesting that the chromatography with the ion exchange column has indeed a diagnostic advantage.

Main possible chloridometer interferences are not present in ion chromatography
After the most important validation characteristics have been completed, the quality controls in the sweat matrix were determined, which is important in order to assess the robustness of the method (Fig. 5).

The course of the low sweat control in the quality interval, with the mean 23 mmol/l. In this analysis a total of 30 measurements were performed
4 Discussion
In newborn screening for CF, the sweat chloride test remains the gold standard for CF diagnosis since many years, but this test does not always give a clear answer to the question if a patient is affected by CF or not [3, 10]. In the ion chromatography method, this situation is rather similar because both methods rely on simple measurement of the analyte chloride. The method described here has a measuring range for chloride between 2.82 and 141.0 mmol/l (Table 1), while the measuring range of the chloridometer lies in the range of 9 and 139 mmol/l. The limit of quantification of 2.82 mmol/l is sensitive enough to reliably detect this analyte in sweat, while no interfering peaks are detected in the respective chromatographic retention time region (Fig. 1). The QC validation accuracy in all cases was found to be lower than 0.3% SD (Table 2), suggesting that the methodology is rather robust.
The longer term QC accuracy determined in 30 individual measurements showed that the method allows measurements with a SD of about 0.6% (Fig. 5). The method runs without internal standard, but it fully meets all accuracy criteria. Furthermore, the quantification limits of the ion chromatography are comparable to the chloridometer method (Fig. 2). The linearity of this method ranged between 2.82 and 141.0 mmol/l, thus fully meets all criteria necessary to perform meaningful CF analysis. In the comparative measurement we found no complaints in terms of quality between both methods (Fig. 2). Therefore, potential errors resulting from deviation due to the device can be ruled out.
Most important, the amount of material required for the measurement is far below the standard volume of 20 µl. The ion chromatography analysis established here can already be carried out in samples volumes from 10 µl down to 5 µl, in extreme cases even from 2.5 µl samples. The method is even sensitive enough to detect chloride in diluted samples.
Moreover, a decisive advantage over the chloridometer is its selectivity. The chloridometer is susceptible to errors resulting from oxidizing substances or interfering substances such as F− and Br−. These analytical interferences do not occur in the ion chromatography method reported here (Fig. 4). Therefore, compared to other methods used in CF analytics such as the chloridometer, inductively coupled plasma mass spectrometry (ICP-MS) [11], and capillary electrophoresis [12], the ion chromatographic method described here is a significant analytical add-on. However, the chloridometer is still the preferred method in point of care testing because the purchase of a typical ICP-MS work station requires an investment of approximately 180,000 US$ [13].
In the initial screening study, we have performed measurements in 145 patient samples, from which the majority of the samples (79%) were considered as normal (Fig. 3). 20% of all samples had chloride concentrations in the intermediate range for which a further diagnostic examination is necessary. In one case out of 145 samples, the presence of CF was made probable. In this case, a genetic examination is mandatory. Nevertheless, the method described here must be carried out by trained laboratory personnel, thus preventing the use of this method in point of care testing.
5 Study limitations
CF should be detected as early as possible in order to be able to initiate therapeutic steps as soon as possible. Therefore, simple accessible methods should be available, which allow conclusive testing for CF. Here we established a robust, selective, sensitive, and cost-effective alternative to the existing ICP-MS and chloridometer methods. However, further work will now be necessary to document the comparability of both methods thought external quality controls. Currently, we have only tested the method in sweat of 145 patients from which the majority of subjects were considered as normal. It would be of fundamental interest to measure samples from a defined cohort known to suffer from CF.
6 Conclusion
The ion chromatography method described here offers a reliable, selective and inexpensive way to measure chloride in sweat in a routine laboratory.
References
Shteinberg M, Haq IJ, Polineni D, Davies JC (2021) Cystic fibrosis. Lancet 397:2195–2211. https://doi.org/10.1016/S0140-6736(20)32542-3
Ooi CY, Sutherland R, Castellani C, Keenan K, Boland M, Reisman J, Bjornson C, Chilvers MA, van Wylick R, Kent S, Price A, Mateos-Corral D, Hughes D, Solomon M, Zuberbuhler P, Brusky J, Durie PR, Ratjen F, Gonska T (2019) Immunoreactive trypsinogen levels in newborn screened infants with an inconclusive diagnosis of cystic fibrosis. BMC Pediatr 19:369. https://doi.org/10.1186/s12887-019-1756-4
Farrell PM, White TB, Ren CL, Hempstead SE, Accurso F, Derichs N, Howenstine M, McColley SA, Rock M, Rosenfeld M, Sermet-Gaudelus I, Southern KW, Marshall BC, Sosnay PR (2017) Diagnosis of cystic fibrosis: consensus guidelines from the Cystic Fibrosis foundation. J Pediatr. https://doi.org/10.1016/j.jpeds.2016.09.064
Cystic Fibrosis Mutation Database. Available at: http://www.genet.sickkids.on.ca/cftr/app (last accessed 24 August, 2022).
Faria AG, Marson FAL, Gomez CCS, Servidoni MF, Ribeiro AF, Ribeiro JD (2017) Thirty years of sweat chloride testing at one referral center. Front Pediatr 5:222. https://doi.org/10.3389/fped.2017.00222
CLSI. Newborn Screening for Cystic Fibrosis. 2nd ed. CLSI guideline NBS05. Wayne, PA: Clinical and Laboratory Standards Institute; 2019. ISBN 978–1–68440–064–5 (Print); ISBN 978–1–68440–065–2 (Electronic).
Servidoni MF, Gomez CCS, Marson FAL, Toro AADC, Ribeiro MÂGO, Ribeiro JD, Ribeiro AF (2017) Grupo Colaborativo de Estudos em Fibrose Cística. Sweat test and cystic fibrosis: overview of test performance at public and private centers in the state of São Paulo, Brazil. J Bras Pneumol. 43:121–128. https://doi.org/10.1590/S1806-37562016000000076
De Boeck K, Vermeulen F, Dupont L (2017) The diagnosis of cystic fibrosis. Presse Med 46(6 Pt 2):e97–e108. https://doi.org/10.1016/j.lpm.2017.04.010
Souza SL, Graça G, Oliva A (2018) Characterization of sweat induced with pilocarpine, physical exercise, and collected passively by metabolomic analysis. Skin Res Technol 24(2):187–195. https://doi.org/10.1111/srt.12412
Farrell PM, Rosenstein BJ, White TB, Accurso FJ, Castellani C, Cutting GR, Durie PR, Legrys VA, Massie J, Parad RB, Rock MJ, Campbell PW 3rd (2008) Cystic fibrosis foundation guidelines for diagnosis of cystic fibrosis in newborns through older adults: cystic fibrosis foundation consensus report. J Pediatr 153:S4–S14. https://doi.org/10.1016/j.jpeds.2008.05.005
Marvelli A, Campi B, Mergni G, Di Cicco ME, Turini P, Scardina P, Zucchi R, Pifferi M, Taccetti G, Paolicchi A, la Marca G, Saba A (2020) Sweat chloride assay by inductively coupled plasma mass spectrometry: a confirmation test for cystic fibrosis diagnosis. Anal Bioanal Chem 412:6909–6916. https://doi.org/10.1007/s00216-020-02821-3
Dubot P, Liang J, Dubs J, Missiak Y, Sarazin C, Couderc F, Caussé E (2018) Sweat chloride quantification using capillary electrophoresis. Pract Lab Med 13:e00114. https://doi.org/10.1016/j.plabm.2018.e00114
Wilbur S. A Comparison of the relative cost and productivity of traditional metals analysis techniques versus ICP-MS in high throughput commercial laboratories. Agilent Technologies, Application. Available at: https://www.agilent.com/cs/library/applications/5989-1585EN.pdf (last accessed 24 August, 2022).
Funding
Open Access funding enabled and organized by Projekt DEAL. The authors have not disclosed any funding.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interest
The authors have nothing to declare.
Data availability
The original data files will be made are available on reasonable request.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Bertges, M., Weiskirchen, R. Quantification of chloride in sweat by using ion chromatography instead of chloridometer. SN Appl. Sci. 4, 273 (2022). https://doi.org/10.1007/s42452-022-05162-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s42452-022-05162-1