
Abstract
The Self-compassion Scale-Short Form (SCS-SF) was developed as an economical alternative for the Self-compassion Scale (SCS), one of the few scales to assess self-compassion. Despite the active use of the SCS-SF, a psychometric evaluation of this scale remains limited. This study analysed the factor structure, reliability, and construct validity of the SCS-SF in UK university student populations. Of 365 students approached, 333 completed the SCS-SF and other measures including negative psychological constructs (mental health problems, self-criticism, and mental health shame) and positive psychological constructs (self-reassurance, resilience, and well-being). Data were analysed through confirmatory factor analyses and correlations. CFA revealed that the six-factor structure, reported in the validation paper, was not replicated. The positive factor, consisting of the three positive subscales, was not strongly related to any variable but moderately related to reassured-self, resilience, well-being, and inadequate-self. The negative factor, consisting of the three negative subscales, was strongly related to inadequate-self and moderately related to resilience, reassured-self, stress, well-being, depression, and internal shame. Coefficients in the negative factor were in general larger than those in the positive factor. The total SCS-SF score was most strongly related to inadequate-self, followed by resilience. Inter-correlations of the six subscales did follow neither Neff’s [1] theoretical model of self-compassion nor the full-scale factor solution. Findings do not accord with the common use of the global SCS-SF score as an assessment of six factors of self-compassion and suggest a two-factor solution assessing self-criticism and self-compassion.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Self-compassion—being understanding and accepting of one’s weaknesses and inadequacies [2]—has been receiving increasing attention [3], particularly in the fields of mental health and psychology [4,5,6,7,8,9]. A meta-analysis of 20 studies reported large (as defined [10]) associations between self-compassion and various types of mental distress including depression and anxiety [11]. Further, intervention studies found that enhancing self-compassion also improved various outcomes including mental health [12], well-being [13], and life satisfaction [14]. These studies reported that practicing compassion towards one’s inadequacies and life challenges can counter shame and self-criticism, which otherwise might lead to poor mental health and well-being [15].
Self-compassion is most commonly regarded [3] as a healthful formulation of self-acceptance, based upon (i) self-kindness: an understanding of oneself when facing inadequacy, rather than self-criticism and self-judgement; (ii) common humanity: a notion that suffering is an unavoidable human condition, as opposed to viewing it as a source of isolation (e.g. ‘Why me?’); and (iii) mindfulness: being presently aware of hurtful thoughts, instead of over-identifying with them [1, 2]. These three components are theorised to interplay with each other: improvement in one element can lead to improvement in another [1]. Self-compassion, therefore, is based on positive constructs of self-kindness, common humanity, and mindfulness and the absence of their opposites, the negative constructs of self-judgement, isolation, and over-identification [2]. The positive constructs may be explained by significant relationships between self-compassion and positive affects (e.g. happiness and optimism) and personality traits (e.g. agreeableness) [16]. On the other hand, the negative constructs may be explained by the strong associations with mental health problems (e.g. depression, anxiety, stress) and shame [2, 6,7,8,9, 17, 18].
The Self-compassion Scale (SCS; [2]) is the most commonly used measure of self-compassion in research [3], although other self-compassion scales have been developed recently (e.g. [19,19,21]). However, this 26-item scale has been criticised for its limited reliability; in Lopez et al.’s study (2015) of 1643 Dutch participants aged 20–97 years, confirmatory factor analyses (CFAs) could not replicate the original six-factor structure of the SCS. Indeed, exploratory factor analyses (EFAs) indicated a two-factor solution with the positive components (self-kindness, common humanity, and mindfulness) and the negatives ones (self-judgement, isolation, and over-identification), as the best fit model with good internal consistency. Similar results were also yielded in other studies, reporting a best and good fit of a two-factor solution [22,22,24]. Neff [25] attributed these poor fits with the six-subscale model to the language translation and the specific study contexts, in line with her previous research into differences of self-compassion in different cultures [26]. However, the generalisability of SCS needs to be refined. Recently, following other research supporting the validity of SCS (Cleare et al., 2017; [27]), Neff et al. [28] conducted more comprehensive analyses (n = 11,685) which confirmed the reliability of the six-factor model of the SCS.
In order to reduce the time and effort for participants, a brief version of SCS, the 12-item Self-compassion Scale-Short Form (SCS-SF; [18]) was developed; this was particularly desirable in clinical research where patients often have to complete large batteries of assessments. The global score of SCS-SF was almost perfectly correlated with the global score of SCS [18]. Raes et al. recruited two Dutch samples (271 undergraduate psychology students and 185 from general population), using the Dutch version of SCS, and one American sample (415 students), using the original English version of SCS. Raes et al. selected two items from each subscale that were strongly correlated with the global score of SCS and their intended subscale score (recommended by [29]), while qualitatively considering the breadth of the original subscale contents (to counter the risk of suboptimal content domain coverage; [30]). While the global SCS-SF score was almost perfectly correlated with the global SCS score (r ≥ .97), the internal consistencies of the subscales in the SCS-SF (the English version) were less good, varying between .54 and .75; hence, only the global SCS-SF score, and not the subscales, was recommended for use [18].
The validity of the SCS-SF has been tested in various populations. Among 594 randomly recruited elder participants, the Swedish SCS-SF did not yield reliable results. Good reliability was only found in the group of 66-year-olds (α > .70), and only the negative components of the two-factor model (self-judgement, isolation, and over-identification) showed good internal consistency, both in the entire sample and in the 66-year-old group [31]. Likewise, Hayes, Lockard, Janis, and Locke (2016) explored the factor structure and construct validity of the SCS-SF for a clinical population (1609 American university students who have mental health problems), and could not replicate the six-subscale model, but identified a two-factor model: self-disparage and self-care. These were similar results to Costa et al. [23], who noted the two-factor model for the full SCS from other clinical populations. Lastly, Sutten, Schonert-Reichl, Wu, and Lawlor (2018) investigated 406 Canadian children between 8 and 12 years old, using the Self-compassion Scale for Children (SCS-C), an adjusted brief version of the SCS-SF to more children-friendly language, which, again, supported the two-factor model. Despite the significant differences of the levels of self-compassion in different cultures [26], the SCS-SF to date has not been evaluated in UK populations. Indeed, high internal consistency of SCS-SF in UK populations has been reported in recent studies (e.g. α = .90–.92 in n = 105; [32]; α = .84 in n = 145; Kotera, Green & Sheffield, 2019); however, these studies did not recruit a large sample and did examine neither the factor structure nor the construct validity of the scale. Accordingly, this study aimed to explore the factor structure, reliability, and construct validity of the SCS-SF in UK students. First, the factor structure was examined using CFA: whether we could replicate the hierarchical six-factor structure (as reported by [18]). Second, the reliability of the SCS-SF (internal consistency) was calculated. Lastly, the relationships between the SCS-SF and self-report measures regarding mental health, self-criticism, self-reassurance, mental health shame, emotional resilience (hereafter ‘resilience’), and mental well-being (hereafter ‘well-being’) were explored, in order to appraise construct validity of the SCS-SF.
Method
Sample and Procedure
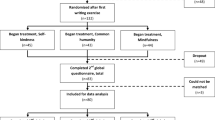
This is part of a research project where the mental health of students in the UK was explored. Ethical approval was granted by the university’s research ethics committee. Student participants, who were aged 18 years old or older and were studying at a UK university, were recruited from healthcare and social care programmes at a UK university in the East Midlands via opportunity sampling. Students who were on a study break at the time of the study were excluded. No incentives were offered for participation. Of 365 students approached, 333 (Mage = 29.28, SDage = 9.06 years old) completed the SCS-SF and other self-report measures about mental health, self-criticism, self-reassurance, shame, resilience, and well-being. There were 287 females, 45 males, and 1 unanswered; 281 undergraduates and 52 postgraduates; 299 home students; and 34 international students including 14 other Europeans, 13 Africans, 4 Asians, 2 North Americans, and 1 unanswered.
Measures
The Self-compassion Scale-Short Form (SCS-SF; [18]) is a 12-item on five-point Likert scale (0 = ‘Almost never’ to 5 = ‘Almost always’) to record how often you behave kindly and caringly towards yourself in difficult life situations. The global SCS-SF score had high internal consistency (α = .86; [18]). As with the original 26-item Self-compassion Scale [2], Raes et al. calculated internal consistency for all the six subscales (self-kindness, self-judgement, common humanity, isolation, mindfulness, and over-identification); however, it was not high (α = .54–.75; self-kindness had the lowest, and over-identification had the highest α values). Therefore, they recommended only using the global score in the SCS-SF. Six items are positively worded (e.g. ‘When something painful happens I try to take a balanced view of the situation’), and the other six are negatively worded (e.g. ‘When I fail at something that’s important to me, I tend to feel alone in my failure’), thus inversely rated.
The Depression, Anxiety, and Stress Scale 21 (DASS 21), a shortened version of DASS 42 [33], was used to measure mental health. Reflecting on the past week, participants respond to these 21 items on four-point Likert scale (0 = ‘Did not apply to me at all’ to 3 = ‘Applied to me very much or most of the time’), relating to the levels of depression (e.g. ‘I found it difficult to work up the initiative to do things’), anxiety (e.g. ‘I felt I was close to panic’) and stress (e.g. ‘I was intolerant of anything that kept me from getting on with what I was doing’) (seven items each). These subscales had good reliability (α = .87–.94; [34]).
Self-criticism and self-reassurance were examined employing the Forms of Self-criticising/attacking and Self-reassuring Scale (FSCRS; [35]), entailing 22 items on five-point Likert scale (0 = ‘Not at all like me’ to 4 = ‘Extremely like me’). FSCRS appraises how people treat themselves in challenging times, referring to self-criticalness (inadequate-self and hated-self) and self-reassurance (reassured-self). Inadequate-self considers a sense of personal inadequacy (e.g. ‘I feel beaten down by my own self-critical thoughts.’; nine items), hated-self considers a desire to persecute the self (e.g. ‘I have a sense of disgust with myself.’; five items), and reassured-self considers a sense of supporting the self (e.g. ‘I find it easy to forgive myself.’; eight items). These subscales had high internal consistency (α = .86–.90; [35]).
Mental health shame was appraised using the Attitudes Towards Mental Health Problems (ATMHP) scale [36], consisting of 35 items on four-point Likert scale (0 = ‘Do not agree at all’ to 3 = ‘Completely agree’), dividing into four sections. The first section gauges the perception of their community and family towards mental health problems (e.g. ‘My community/family would tend to look down on somebody with mental health problems’; eight items). The second section appraises the perception of their community and family towards them, if they had a mental health problem (i.e. external shame; e.g. ‘I think my family/community would see me as inadequate’; ten items). The third section considers their own perception towards themselves if they have a mental health problem, namely, internal shame (e.g. ‘I would see myself as a weak person’, five items). The fourth section comprising 12 items relates to reflected shame: (a) worries of reflected shame on their family, if they had a mental health problem (family-reflected shame; e.g. ‘I would worry about the effect on my family’), and (b) worries of reflected shame on themselves, if a close relative had a mental health problem (self-reflected shame; e.g. ‘I would worry that if this were known I would lose status the community’). All of the subscales had high internal consistency (α = .85–.97; [36]).
Brief Resilience Scale (BRS), a six-item on five-point Likert scale measure (1 = ‘Strongly Disagree’ to 5 = ‘Strongly Agree’) assessing the ability to bounce back from difficulties [37], was used to measure resilience (e.g. ‘It does not take me long to recover from a stressful event’). Items 2, 4, and 6 are inversely scored. BRS demonstrated high internal consistency (α ≧ .80; [37]).
Lastly, well-being was measured using the Short Warwick–Edinburgh Mental Well-being Scale (SWEMWBS; [38]), a seven-item scale, shortened from the original 14-item version [39]. Participants reflect on the past 2 weeks to respond to items including ‘I’ve been feeling optimistic about the future’, on a five-point Likert scale (‘1’ being ‘None of the time’ to ‘5’ being ‘All of the time’). SWEMWBS had high internal consistency (α = .85; [38]).
Data Analysis
First, the factor structure of the SCS-SF was examined through CFA using RStudio version 1.1.463 [40]. The goodness of fit of the models was checked using the chi-squared to degrees of freedom ratio (χ2/df), the comparative fit index (CFI), the Tucker–Lewis Index (TLI), the root mean square error of approximation (RMSEA), and the standardised root mean residual (SRMR). χ2/df values less than 5.00 are considered an acceptable fit of the model, and values close to or less than 2.00 are considered a good fit [41]. CFI and TLI values greater than .90 are interpreted as an acceptable, and values greater than .95 are interpreted as a good model fit. Lastly, RMSEA and SRMR values between .06 and .08 indicate an acceptable model fit, and values smaller than .06 indicate a good fit (Hu and Bentler, 2009). Recent studies reported that these fit indices can be affected by sample size and data normality [42, 43]; a satisfactory model fit was determined when all assessments assured either an acceptable or a good fit.
None of the 12 items in the SCS-SF was deemed to have severe non-normal distribution, which was assessed from the skewness (< 2) and kurtosis (< 7) values [44]. Internal consistency was determined with Cronbach’s alpha statistic (α): α ≧ .80 was considered as good/high [45]. Pearson correlations were performed to examine the associations between the SCS-SF and other psychological constructs; correlations coefficients below .19 were interpreted as ‘very weak’, .20–.39 as ‘weak’, .40–.59 as ‘moderate’, .60–.79 as ‘strong’, and .80–1.0 as ‘very strong’ [46].
Results
Descriptive Statistics
Table 1 presents the mean scores and standard deviations of all the study variables.
SCS-SF subscales were strongly inter-correlated with each other and the total score, with most of the coefficients greater than .3; these correlations are presented in Table 2.
Confirmatory Factor Analysis
A model with six correlated factors, reported by Raes et al. [18], was tested. The fit indices computed that the model fit the data to an acceptable to good degree: χ2 = 89.324 (df = 39, p < .000), χ2/df = 2.29 (i.e. < 3 indicating an acceptable fit), CFI = .96 (i.e. > .95 indicating a good fit), TLI = .94 (i.e. > .90 indicating an acceptable fit), RMSEA = .062 (i.e. < .08 indicating an acceptable fit), and SRMR = .046 (i.e. < .06 indicating a good fit). However, the covariance matrix of latent variables was not positive definite; therefore, the results did not replicate the six-factor model [47].
Further, as re-appraisal research of the original SCS has reported (e.g. Lopez et al., 2015), we examined the model fit of the two-factor model of the SCS-SF. This time, the covariance matrix of latent variables was not a concern, and an acceptable model fit was calculated: χ2 = 150.335 (df = 53, p < .000), χ2/df = 2.84 (i.e. < 3 indicating an acceptable fit), CFI = .93 (i.e. > .90 indicating an acceptable fit), TLI = .91 (i.e. > .90 indicating an acceptable fit), RMSEA = .074 (i.e. < .08 indicating an acceptable fit), and SRMR = .061 (i.e. < .08 indicating an acceptable fit). Table 3 summarises the factor loadings of each item. In general, the negative factor yielded higher loadings than the positive one.
Exploratory factor analyses performed using principal components analysis also supported the two-factor model (see Appendix Table 5).
Reliability: Internal Consistency
Internal consistencies of the items related to negative subscales and positive subscales were calculated. Internal consistency for the negative subscale items was high (α = .86) and acceptable for the positive subscale items (α = .79). The SCS-SF total score also demonstrated good internal consistency (α = .85).
Construct Validity: Correlations with Other Self-report Measures
Overall, the positive factor, negative factor, and total of SCS-SF were broadly related to other psychological variables, apart from community attitudes (Table 4). The positive factor was moderately related to reassured-self, resilience, well-being, and inadequate-self (r > .4; [46]). No variable was strongly related to the positive factor. The negative factor was strongly related to inadequate-self (r = − .66) and moderately related to resilience, reassured-self, stress, well-being, depression, and internal shame (r > .4). Coefficients in the negative factor were, in general, larger than those in the positive factor. The total SCS-SF score was especially strongly related to inadequate-self, resilience, and reassured-self (r ≧ .6) and moderately related to well-being, stress, depression, and hated-self (r > .4).
Discussion
This study evaluated the psychometric properties of the Self-compassion Scale-Short in a large student sample in the UK. Results did not confirm the six-factor structure, as proposed by Raes et al. [18]. Contrarily, a two-factor model was identified; the positively formulated items and negatively formulated items, both with high internal consistency. These two factors were differently related to other variables, implying that the meaning of each factor was different. The positive factor was moderately, but not strongly, related to reassured-self, resilience, well-being, and inadequate-self: three of them were positive constructs. The negative factor was strongly related to inadequate-self, and moderately related to resilience, reassured-self, stress, well-being, depression, and internal shame.
One of the unique findings from this study is that the SCS-SF was deemed to have a two-factor structure of the positively and negatively formulated items, instead of the six-factor model as reported by Raes et al. [18]. This was consistent with other studies that explored the psychometric properties of the SCS-SF, which failed to replicate the six-factor model but identified a two-factor model ([31, 48]; Sutten et al., 2018). Our CFA did not replicate the six-factor model but did replicate the two-factor model: the negative factor as the primary factor and the positive factor as the secondary factor. This may suggest that the SCS-SF was psychometrically more fit to measure the negative aspects of self-compassion (e.g. self-criticism) than the positive aspects. Although the title of ‘self-compassion’ suggest a positive psychological construct, the SCS-SF may be more suited to measure the negative construct of self-criticism, as the factor loadings in this factor indicated a higher contribution to the total SCS-SF score than the positive factor. This may suggest a renaming of this scale: Self-inadequacy and Resilience Scale.
Relatedly, our findings using SCS-SF did not support Neff’s theoretical model of self-compassion (2003), where the three positive subscales contribute to self-compassion, and each positive subscale corresponds to the opposing negative subscale (e.g. self-judgement is an opposing construct to self-kindness). Common humanity was most strongly related to self-judgement, not isolation among the three negative subscales, and over-identification was most strongly related to self-kindness, not mindfulness among the three positive subscales. Moreover, the SCS-SF was more firmly associated with the negative psychological variables than the positive psychological ones. Both the negative factor and the total score were most strongly related to inadequate-self, suggesting that the utility of this scale may be better expressed using constructs such as ‘self-inadequacy’ in the title. Considering that it is a two-factor model with the positive items and negative ones, the positive aspects may be expressed using positive constructs such as ‘resilience’, contrasting to the negative ‘self-inadequacy’. These words may better inform researchers and practitioners about what this scale primarily assesses, avoiding participants and patients’ misinterpretation (which could cause serious consequences). This may be similar to the recent overuse of the word ‘resilience’. Because this word has been used so frequently in diverse contexts, sometimes educators and students use it incorrectly, causing psychological damage to students [49]. The structure of the SCS-SF may need to be re-evaluated to better capture the original six factors that were recently confirmed in a large multi-country study [28].
Several limitations need to be considered. First, this study only considered a student sample at a UK university via opportunity sampling, which limits the generalisability of the findings. Therefore, the findings may not be generalisable to clinical populations in the UK, while noting that there was no difference in self-compassion between a clinical sample and non-clinical sample [50]. Moreover, it is unclear whether the findings would be replicated in samples from other countries, in addition to Sweden [31], the USA [48], and Canada (Sutten et al., 2018). Second, there might have been other scales to be included to assess the convergent and divergent validity of the SCS-SF. However, the scales included were strongly related to the SCS-SF, which included self-reassurance in the FSCRS, a relatively similar construct to self-compassion. Likewise, this paper did not compare SCS-SF with other newly developed compassion scales such as the Sussex-Oxford Compassion Scale (SOCS; Gu et al., 2019). Future research needs to compare these compassion scales to identify their characteristics to help practitioners and researchers to discern the most appropriate compassion scale to be used in their population and context. Third, the dropout rate was not insignificant (9%). This may be due to the length of the entire battery of the survey, implying that the response accuracy may be limited (i.e. even students who have completed all the questionnaires might have felt tired towards the end of the survey). Future research can benefit from using such short and reliable scales.
In conclusion, our results did not accord with the proposed six-factor model of the SCS-SF but did support the two-factor model, where the negative factor had more bearing on the total score than the positive factor. These results differ from the full SCS, which replicated the six-factor model but did not replicate the two-factor model across 20 samples (n = 11,685; [28]). Considering the SCS-SF’s higher relevancy to the negative constructs than the positive ones, the current title of self-compassion—a rather positive construct—may be misleading. To acknowledge the positive factor, a title such as ‘self-inadequacy and resilience’ (or self-criticism and self-compassion) may capture the characteristics of the scale more accurately. More research is needed to re-appraise the structure of the SCS-SF in a range of populations.
References
Neff KD. The development and validation of a scale to measure self-compassion. Self Identity. 2003b;2(3):223–50. https://doi.org/10.1080/15298860309027.
Neff K. Self-compassion: an alternative conceptualization of a healthy attitude toward oneself. Self Identity. 2003a;2(2):85–101. https://doi.org/10.1080/15298860309032.
López A, Sanderman R, Smink A, Zhang Y, van Sonderen E, Ranchor A, et al. A reconsideration of the Self-Compassion Scale’s total score: self-compassion versus self-criticism. PLoS One, e0132940. 2015;10(7). https://doi.org/10.1371/journal.pone.0132940.
Barnard LK, Curry JF. Self-compassion: conceptualizations, correlates, and interventions. Rev Gen Psychol. 2011;15(4):289–303. https://doi.org/10.1037/a0025754.
Kotera Y, Conway E, Van Gordon W. Ethical judgement in UK business students: relationship with motivation, self-compassion and mental health. International Journal of Mental Health and Addiction. 2018a;17:1–15. https://doi.org/10.1007/s11469-018-0034-2.
Kotera Y, Green P, Van Gordon W. Mental wellbeing of caring profession students: relationship with caregiver identity, self-compassion, and intrinsic motivation. Mindfulness & Compassion. 2018b;3(2):7–30.
Kotera Y, Green P, Sheffield D. Mental health attitudes, self-criticism, compassion, and role identity among UK social work students. Br J Soc Work. 2018c;49:351–70. https://doi.org/10.1093/bjsw/bcy072.
Kotera Y, Conway E, Van Gordon W. Mental health of UK university business students: relationship with shame, motivation and self-compassion. J Educ Bus. 2019a;94(1):11–20. https://doi.org/10.1080/08832323.2018.1496898.
Kotera Y, Green P, Sheffield D. Mental health of therapeutic students: relationships with attitudes, self-criticism, self-compassion, and caregiver identity. Br J Guid Couns. 2019b:1–12. https://doi.org/10.1080/03069885.2019.1704683.
Cohen J. Statistical power analysis for the behavioral sciences. New York: Lawrence Erlbaum; 1988.
MacBeth A, Gumley A. Exploring compassion: a meta-analysis of the association between self-compassion and psychopathology. Clin Psychol Rev. 2012;32(6):545–52. https://doi.org/10.1016/j.cpr.2012.06.003.
Gilbert P, Procter S. Compassionate Mind Training for people with high shame and self-criticism: overview and pilot study of a group therapy approach. Clinical Psychology and Psychotherapy. 2006;13:353–79. https://doi.org/10.1002/cpp.507.
Mantelou A, Karakasidou E. The effectiveness of a brief self-compassion intervention program on self-compassion, positive and negative affect and life satisfaction. Psychology. 2003;8:590–610. https://doi.org/10.4236/psych.2017.84038.
Neff KD, Germer CK. (2013) A Pilot Study and Randomized Controlled Trial of the Mindful Self-Compassion Program. J Clin Psychol. 69(1):28–44. https://doi.org/10.1002/jclp.21923.
Gilbert P. Introducing compassion-focused therapy. Adv Psychiatr Treat. 2009;15(3):199–208. https://doi.org/10.1192/apt.bp.107.005264.
Neff KD, Rude SS, Kirkpatrick KL. An examination of self-compassion in relation to positive psychological functioning and personality traits. J Res Pers. 2007;41(4):908–16. https://doi.org/10.1016/J.JRP.2006.08.002.
Leary MR, Tate EB, Adams CE, Batts Allen A, Hancock J. Self-compassion and reactions to unpleasant self-relevant events: the implications of treating oneself kindly. J Pers Soc Psychol. 2007;92(5):887–904. https://doi.org/10.1037/0022-3514.92.5.887.
Raes F, Pommier E, Neff KD, Van Gucht D. Construction and factorial validation of a short form of the Self-Compassion Scale. Clinical Psychology and Psychotherapy. 2011;18(3):250–5. https://doi.org/10.1002/cpp.702.
Gilbert P, Catarino F, Duarte C, Matos M, Kolts R, Stubbs J, et al. The development of compassionate engagement and action scales for self and others. Journal of Compassionate Health Care. 2017;4(4). https://doi.org/10.1186/s40639-017-0033-3.
Gu J, Baer R, Cavanagh K, Kuyken W, Strauss C. Development and psychometric properties of the Sussex-Oxford Compassion Scales (SOCS). Assessment. 2020;27(1):3–20. https://doi.org/10.1177/1073191119860911.
Smith BW, Guzman A, Erickson K. The Unconditional Self-Kindness Scale: assessing the ability to respond with kindness to threats to the self. Mindfulness. 2018;9(6):1713–22. https://doi.org/10.1007/s12671-018-0912-5.
Coroiu A, Kwakkenbos L, Moran C, Thombs B, Albani C, Bourkas S, et al. Structural validation of the Self-Compassion Scale with a German general population sample. PLoS One. 2018;13(2):e0190771. https://doi.org/10.1371/journal.pone.0190771.
Costa J, Marôco J, Pinto-Gouveia J, Ferreira C, Castilho P. Validation of the psychometric properties of the Self-Compassion Scale. Testing the factorial validity and factorial invariance of the measure among borderline personality disorder, anxiety disorder, eating disorder and general populations. Clinical Psychology and Psychotherapy. 2016;23(5):460–8. https://doi.org/10.1002/cpp.1974.
Phillips WJ, Ferguson SJ. Self-compassion: a resource for positive aging. J Gerontol Ser B Psychol Sci Soc Sci. 2013;68(4):529–39. https://doi.org/10.1093/geronb/gbs091.
Neff KD. The Self-Compassion Scale is a valid and theoretically coherent measure of self-compassion. Mindfulness. 2016;7(1):264–74. https://doi.org/10.1007/s12671-015-0479-3.
Neff KD, Pisitsungkagarn K, Hsieh Y-P. Self-compassion and self-construal in the United States, Thailand, and Taiwan. J Cross-Cult Psychol. 2008;39(3):267–85. https://doi.org/10.1177/0022022108314544.
Zhang H, Dong L, Watson-Singleton NN, Tarantino N, Carr ER, Niles-Carnes LV, et al. Psychometric properties of the Self-Compassion Scale (SCS) in an African American clinical sample. Mindfulness. 2019;10:1395–405. https://doi.org/10.1007/s12671-019-01099-6.
Neff KD, Tóth-Király I, Yarnell LM, Arimitsu K, Castilho P, Ghorbani N, et al. Examining the factor structure of the Self-Compassion Scale in 20 diverse samples: support for use of a total score and six subscale scores. Psychol Assess. 2019;31(1):27–45. https://doi.org/10.1037/pas0000629.
Stöber J, Joormann J. Worry, procrastination, and perfectionism: differentiating amount of worry, pathological worry, anxiety, and depression. Cogn Ther Res. 2001;25(1):49–60. https://doi.org/10.1023/A:1026474715384.
Thompson ER. Development and validation of an internationally reliable short-form of the Positive and Negative Affect Schedule (PANAS). J Cross-Cult Psychol. 2007;38(2):227–42. https://doi.org/10.1177/0022022106297301.
Bratt A, Fagerström C. Self-compassion in old age: confirmatory factor analysis of the 6-factor model and the internal consistency of the Self-Compassion Scale-Short Form. Aging Ment Health. 2019;24:1–7. https://doi.org/10.1080/13607863.2019.1569588.
Ivtzan I, Young T, Lee HC, Lomas T, Daukantaitė D, Kjell ONE. Mindfulness based flourishing program: a cross-cultural study of Hong Kong Chinese and British participants. J Happiness Stud. 2018;19(8):2205–23. https://doi.org/10.1007/s10902-017-9919-1.
Lovibond S, Lovibond P. Manual for the depression anxiety stress scales. Sydney: Psychology Foundation; 1995.
Antony M, Bieling P, Cox B, Enns M, Swinson R. Psychometric properties of the 42-item and 21-item versions of the Depression Anxiety Stress Scales in clinical groups and a community sample. Psychol Assess. 1998;10(2):176–81. https://doi.org/10.1037/1040-3590.10.2.176.
Gilbert P, Clarke M, Hempel S, Miles J, Irons C. Criticizing and reassuring oneself: an exploration of forms, styles and reasons in female students. Br J Clin Psychol. 2004;43(1):31–50. https://doi.org/10.1348/014466504772812959.
Gilbert P, Bhundia R, Mitra R, McEwan K, Irons C, Sanghera J. Cultural differences in shame-focused attitudes towards mental health problems in Asian and non-Asian student women. Mental Health, Religion & Culture. 2007;10(2):127–41. https://doi.org/10.1080/13694670500415124.
Smith BW, Dalen J, Wiggins K, Tooley E, Christopher P, Bernard J. The brief resilience scale: assessing the ability to bounce back. International Journal of Behavioral Medicine. 2008;15(3):194–200. https://doi.org/10.1080/10705500802222972.
Stewart-Brown S, Tennant A, Tennant R, Platt S, Parkinson J, Weich S. Internal construct validity of the Warwick-Edinburgh Mental Well-being Scale (WEMWBS): a Rasch analysis using data from the Scottish Health Education Population Survey. Health Qual Life Outcomes. 2009;7(1):15. https://doi.org/10.1186/1477-7525-7-15.
Stewart-Brown S, Janmohamed K. Warwick-Edinburgh Mental Well-being Scale (WEMWBS) user guide version 1. Warwick: Warwick Medical School; 2008.
RStudio Team. RStudio: integrated development for R. Boston: RStudio, Inc.; 2015.
Watkins D. The role of confirmatory factor analysis in cross-cultural research. International Journal of Psychology. 1989;24(2–6):685–701. https://doi.org/10.1080/00207598908247839.
DiStefano C, Liu J, Jiang N, Shi D. Examination of the weighted root mean square residual: evidence for trustworthiness? Struct Equ Model Multidiscip J. 2018;25(3):453–66. https://doi.org/10.1080/10705511.2017.1390394.
Nye CD, Drasgow F. Assessing goodness of fit: simple rules of thumb simply do not work. Organ Res Methods. 2011;14(3):548–70. https://doi.org/10.1177/1094428110368562.
Fabrigar LR, Wegener DT, MacCallum RC, Strahan EJ. Evaluating the use of exploratory factor analysis in psychological research. Psychol Methods. 1999;4(3):272–99. https://doi.org/10.1037/1082-989X.4.3.272.
Nunnally JC. Psychometric theory. New York: McGraw-Hill; 1978.
Evans JD. Straightforward statistics for the behavioral sciences. Pacific Grove: Brooks/Cole; 1996.
Beaujean AA. Latent variable modeling using R. New York: Routledge; 2014.
Hayes JA, Lockard AJ, Janis RA, Locke BD. Construct validity of the Self-Compassion Scale-Short Form among psychotherapy clients. Couns Psychol Q. 2016;29(4):405–22. https://doi.org/10.1080/09515070.2016.1138397.
Traynor M. Guest editorial: what’s wrong with resilience. J Res Nurs. 2018;23:5–8. https://doi.org/10.1177/1744987117751458.
Williams MJ, Dalgleish T, Karl A, Kuyken W. Examining the factor structures of the Five Facet Mindfulness Questionnaire and the Self-Compassion Scale. Psychol Assess. 2014;26(2):407–18. https://doi.org/10.1037/a0035566.
Schönrock-Adema J, Heijne-Penninga M, Van Hell EA, Cohen-Schotanus J, Schönrock J, Schönrock-Adema S. Medical teacher necessary steps in factor analysis: enhancing validation studies of educational instruments. The PHEEM applied to clerks as an example. Medical Teacher. 2009;31:226–32. https://doi.org/10.1080/01421590802516756.
Cattell R. The scree test for the number of factors. Multivar Behav Res. 1966;1(2):245–76. https://doi.org/10.1207/s15327906mbr0102_10.
Kaiser HF. An index of factorial simplicity. Psychometrika. 1974;39(1):31–6. https://doi.org/10.1007/BF02291575.
Thurstone LL. Multiple factor analysis: a development and expansion of vectors of the mind. Chicago: University of Chicago Press; 1947.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical Approval
This study was approved by the research ethics committee of the University of Derby. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Conflict of Interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Medicine
Appendix
Appendix
Exploratory factor analyses were performed on SPSS 25.0 to examine the factor structure of the SCS-SF, conducting a principal components analysis (PCA). The suitability of PCA was tested before analysis: the correlation matrix demonstrated that all variables had at least one correlation coefficient greater than .30. The overall Kaiser–Meyer–Olkin (KMO) measure was .88 with individual KMO measures all greater than .83, demonstrating ‘meritorious’ to ‘marvelous’ values [51]. Bartlett’s test of sphericity was statistically significant (p < .0005), indicating that the data were likely factorisable.
PCA revealed two components that had eigenvalues above one, and those components explained 38.08% and 16.65% of the total variance each. Visual inspection of the scree plot indicated that two components should be retained [52]. Moreover, a two-component solution met the interpretability criterion [53]. Based on those inspections, two components were retained.
The two-component solution explained 54.73% of the total variance. A varimax orthogonal rotation was employed to aid interpretability. The rotated solution exhibited ‘simple structure’ [54], except for item 6. The interpretation of this two-component solution revealed that all the items related to the negative subscales (self-judgement, isolation, and over-identification) were categorised as component 1 (explaining 38.08% of the total variance), whereas all the items related to the positive subscales (self-kindness, common humanity, and mindfulness) were categorised as component 2 (explaining 16.65% of the total variance).
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kotera, Y., Sheffield, D. Revisiting the Self-compassion Scale-Short Form: Stronger Associations with Self-inadequacy and Resilience. SN Compr. Clin. Med. 2, 761–769 (2020). https://doi.org/10.1007/s42399-020-00309-w
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s42399-020-00309-w