
Abstract
Background
Nowadays, liver cancer is the second leading cause of cancer death in the world. Therefore, it is very important to understand tumor progression and evaluate tumor microcirculation for treatment strategy.
Objective
To explore the application of MRI quantitative hemodynamic parameter histogram analysis in the development of a rabbit VX2 liver cancer.
Methods
Five New Zealand white rabbits were randomly selected each time for liver Dynamic contrast- enhanced MR perfusion (DCE-MRI) imaging at the 1st, 2nd, 3rd, 4th and 5th weeks after liver tumor implantation. The dynamic changes and the significant differences between the tumor volume and related derived parameters during tumor progression were compared and analyzed.
Results
In the development of the VX2 liver cancer model, the tumor volume between the end of 1 ~ 5w group (F = 44.11; P = 0.000) was statistically significant (P < 0.01), and the significant differences were found between the 5th week and the 1st, 2nd, 3rd, 4th week, the 4th week and the 1st, 2nd week, the 3rd week and the 5th week (P < 0.01), respectively. The skewness and kurtosis of the volume transport constant (Ktrans) value, the maximum, 90th percentile and skewness of the reverse reflux rate constant (Kep) value, and the skewness, kurtosis, 75th and 90th percentiles of the plasma fraction (Vp) value were statistically significant (P < 0.05) at the end of each week. The 10th, 25th, 50th percentiles of the Kep value, the 10th, 25th percentiles of the extracellular space (EES) fraction (Ve) value, the 10th percentile of the Vp value was positively correlated with tumor volume (r > 0, P < 0.05). The expression of α-smooth muscle actin (α-SMA) was negatively correlated with the mean, 75th percentile of the Ktrans value, the 50th, 75th percentiles of the Kep value, the mean, minimum of the Vp value (r < 0, P<0.05). It was positively correlated with the skewness, kurtosis of the Ktrans value, the skewness of the Vp value (r > 0, P<0.05).
Conclusions
MRI quantitative hemodynamic parameter histogram analysis can reflect the progress of the rabbit VX2 liver cancer. In particular, the skewness, kurtosis and percentiles of Ktrans, Kep and Vp can reflect the microvascular information and can be used as biomarkers to assess the development of Hepatocellular Carcinoma(HCC).
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The incidence rate of primary liver cancer ranks fourth in China, and the rate of tumor-related death ranks second. The survival rate in China and the United States is only 3–5% [1, 2]. Previous studies have reported the importance of angiogenesis in the development of hepatocellular carcinoma [3]. Recent studies have shown that angiogenesis is critical for tumor growth, invasion and metastasis. The occurrence and development of tumors are not only determined by cancer cells but also by tumor microcirculation (also known as tumor angiogenesis), which also plays an important role in the growth, invasion and metastasis of cancer cells [4, 5]. The CD34, α-smooth muscle actin (α-SMA) reflect the biological behavior of liver cancer to a certain extent and is closely related to tumor progression and microcirculation, but it is limited by living tissue. Therefore, understanding the molecular and cellular mechanisms regulating the occurrence and development of hepatocellular carcinoma is crucial, and comprehensively evaluating tumor angiogenesis and microcirculation state changes is warranted to formulate treatment strategies and prognosis prediction.
Three-dimensional dynamic contrast-enhanced MR perfusion (DCE-MRI) two-compartment model analysis can be used to quantify the microcirculation function of liver cancer. By introducing low-molecular exogenous contrast agent, the whole liver can be scanned many times. After the pharmacokinetic two-compartment model calculation, hemodynamic information, such as the local tissue blood volume, blood flow and capillary permeability, is obtained, and the contrast molecules are dynamically tracked from time to time [6]. The whole dynamic process of intravascular leakage to the extracellular space and from the extravascular to intravascular space generated the quantitative parameters Ktrans (volume transport constant), Kep (reverse reflux rate constant), Ve (extracellular space (EES) fraction) and VP (plasma fraction). These parameters require additional calculations to generate parametric maps obtained after a pixel-by-pixel curve fitting process of the region under analysis [7, 8]. Thus, they are more computationally technical to obtain than the semi-quantitative ones. After generating parametric maps, the mean or median values within region of interests are usually calculated to represent tumor microvasculature [9].
However, many studies using DCE-MRI quantitative hemodynamic parameters to predict the tumor response apply central trend parameters, such as the average or median of the single slice region of interest (ROI), to determine the longitudinal changes in the tumor tissue before and after treatment [10]. But due to the diversity of etiology and genetic background, as well as the long-term development of liver cancer, the pathological changes in liver cancer show inherent heterogeneous tumor components, which cannot represent the exact tumor status [10]. Presently, a new imaging analysis method, histogram analysis of different radiation parameters, is in development [11]. Histogram analysis can provide more quantitative indicators than the average value, can better reflect several morphological characteristics of different malignant tumors [12], and quantitatively reflect the heterogeneity of tumor pathological changes, without additional hardware and additional sequences. At present, there are few studies on this image post-processing method in liver cancer.
The biological behavior of the rabbit VX2 liver cancer model is similar to that of human tumors in location, tissue type, etiology and pathogenesis [13]. Therefore, this study mainly mimics the rabbit VX2 liver cancer model, which is closest to the human liver cancer model, which aimed to explore microquantitative histogram analysis of tumor microcirculation and tumor functional imaging in the process of tumor progression as well as the application of MRI quantitative hemodynamic parameters histogram analysis to develop a rabbit VX2 liver cancer model to evaluate the progression and prognosis of liver cancer in vivo and provide an imaging basis for clinical treatment.
Materials and methods
Establishment of the tumor-bearing rabbit model
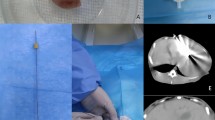
Twenty-eight New Zealand white rabbits aged 2 ~ 3 weeks, male, weighing (2.3 ± 0.4) kg, which were provided by the Experimental Animal Center of Xinjiang Medical University. This study was approved by the animal protection and ethics committee of The First Affiliated Hospital of Shihezi University School of Medicine (No: A2021-052-01). The VX2 rabbit anaplastic epidermal squamous cell carcinoma strain was obtained from Beijing Shangcheng Beina Chuanglian Biotechnology Co. Ltd. (No: 341749). After thawing the VX2 tumor samples, the number of dead and living cells was counted by Trypan blue staining. The activity of the living cells was more than 95%, and the concentration of living cells was 106/mL. In the suspension, 0.5- mL of the tumor suspension was mixed with 1:1 phosphate buffer solution and inoculated into the subcutaneous or muscular space of the groin area of three healthy New Zealand white rabbits. Three weeks later, the solid mass could be found at the inoculation site, which was further confirmed as squamous cell carcinoma by pathology. Under aseptic conditions, the tumor was peeled off, and the tumor tissue with vigorous growth at the edge of the mass was cut and placed in normal saline. The tumor tissue was cut into multiple 1-mm3 tissue blocks by eye scissors for liver implantation.
Twenty-five healthy New Zealand white rabbits were anesthetized with fasting water for 12 h (general anesthesia with 3% pentobarbital sodium 30 mg/kg via the ear vein in the supine position and fixed, with the left side of the xiphoid process sheared). A vertical incision was made under the xiphoid process for approximately 2 cm, and the left liver lobe was exposed with smooth forceps. A 15 G needle was inserted into the visceral surface of the left liver lobe, and then 0.5-mL tumor fragments were injected with a 5-mL syringe and removed. After the acupuncture, the puncture site was covered with a gelatin sponge. After the confirmation of no obvious bleeding, the incision was sutured with a layer of 2 − 0 absorbable suture, and the abdomen was sutured with a layer of 1 − 0 absorbable suture. After the operation, the animals awakened and were returned to the cage. Each experimental rabbit was injected with penicillin (800,000 u) within three days after the operation. The incision was disinfected to prevent infection. Wound healing and appetite were monitored daily. At the end of 1w, 2w, 3w, 4w and 5w after tumor implantation, 5 rabbits were randomly selected for DCE-MRI imaging. After the MRI, 25 New Zealand white rabbits were killed by air embolism under anesthesia.
Instruments and inspection methods
The senior engineer of GE company plans to scan the experimental rabbit model and standardize its scanning parameters. All the experimental animals were subjected to the GE discovery MR750 3.0T MRI scanner, 8 ~ 12 h before fasting, using an 8-channel phased-array orthogonal head and neck coil, in the “prone position, head advanced” position and with the scanning range approximately 2 cm from the top of the diaphragm to the bottom of the kidney. The scanning sequence was Cor T2WI-SSFSE, Ax T2WI-FSE, DCE-MRI. The Cor T2WI-SSFSE parameters were as follows: FOV, 24 × 24 cm; TR, 4488; TE, 70; flip angle, 90°; Nex, 1; thickness, 3.0 mm; matrix, 288 × 288. The Ax T2WI-FSE parameters were as follows: FOV, 24 × 24 cm; TR, 8114; TE, 72; Flip angle, 110°; Nex, 1; thickness, 3.0 mm; matrix, 192 × 192. In the DCE-MRI sequence, five groups of T1-vibe sequences were scanned before examination, and the T1-vibe parameters were as follows: FOV, 24 × 24 cm; TR, 3.0; TE, 1.5; flip angles, 3°, 6°, 9°, 12°, and 15°. Thereafter, DCE-MRI was performed, and the T1-twis parameters were as follows: FOV, 24 × 24 cm; TR, 3.0; TE, 1.4; flip angle, 12°; Nex, 0.69; thickness, 3 mm; matrix, 128 × 128; phase acquisition, 23. At the end of the third phase acquisition image, gadolinium diethylenetriamine was injected through the ear vein at a flow rate of 2.0 mL/s and a dose of 0.1 mmol/kg. After the contrast medium group injection, 20 ~ 30 mL of normal saline was injected into the tube, and then 20 temporal images were continuously or repeatedly collected, approximately 5 ~ 6 min.
Image analysis and postprocessings
All the DCE-MRI images were imported into OmniKinetics Version V2.1.0.R software provided by GE pharmaceutical company in the DICOM format for analysis. The original data were corrected by the registration program, and then the image was imported into the perfusion program. The region of interest (ROI) was placed in the main artery of the abdominal aorta and portal vein, and the time density curve (TDC) and perfusion pseudocolor map were obtained.
Region of interest (ROI) mapping was performed by two radiologists (with 7 years and 3 years of imaging experience in liver diseases, respectively) using the double-blind method. With reference to the axial T2WI image, the focus boundary was drawn layer by layer from the top to bottom on the calibrated image. The ROI should include as much tumor information as possible at every level, including bleeding, necrosis and cystic components, to better evaluate tumor heterogeneity. Additionally, considering the partial volume effect, the ROI area should be slightly smaller than the actual area of the focus. The software combines the ROI of each layer to obtain the 3D-ROI of the whole tumor. For each lesion, the the 3D-ROI of the whole tumor was measured 5 times to take the average value. In the DCE-MRI image, the perfusion parameters(Ktrans, Kep, Ve, Vp; unit: min− 1) and the corresponding parameters of the perfusion pseudo color image were obtained. Finally, the values of quantitative parameters were analyzed by histogram. Histogram parameters include the minimum, maximum, mean, skewness, kurtosis, 10th, 25th, 50th, 75th, and 90th percentiles.
Pathological examinations and analysis
The specimens were fixed with formalin, embedded in paraffin and sectioned continuously. The parenchyma tissues of the liver cancer was selected for the pathological histological and immunohistochemistry evaluation by hematoxylin and eosin staining. The expressions of CD34, α-SMA in the rabbit VX2 implanted tumor were examined immunohistochemically using respective primary antibodies by Elivision TMS-P System. Using Image-Pro Plus 6.0 software for CD34, α-SMA count, Immunohistochemical indicators were recorded 3 times in each pathological, and take its average value as the final result of the slice, and divide it into (-), (+), (++), (+++) according to the result. The pathological materials of the lesions must be consistent with the MRI-ROI delineation of the lesions. Histopathological analysis was performed by a senior pathologist.
Statistical analysis
SPSS 19.0 statistical software was used to analyze the data. Quantitative variables were expressed as the mean ± standard deviation, and categorical variables were expressed as frequencies or percentages. The Shapiro–Wilk method was used to test the normality of the measurement data. For example, to conform to the normal distribution, The ANOVA was used for comparison among groups, and the LSD-t was used for comparison between two groups; if not, the Kruskal–Wallis H test was used for comparison between groups. The Kruskal–Wallis U test was used to compare two groups. The Spearman rank correlation was used to analyze the correlation the tumor volume, quantitative parameters of DCE-MRI histograms and the CD34, α-SMA. P < 0.05 was statistically significant.
Results
-
(1)
Focus and related pathological results.
In 25 rabbits transplanted with VX2 tumor cells, 30 lesions were detected, of which two lesions (one each in the left and right lobes of the liver and two in the left lobes of the liver) were found in the rabbits scanned at the end of 1 and 2 weeks, respectively, and one in the rabbits scanned at the end of 3 weeks was found in two lesions (two in the left lobes of the liver). The 30 lesions of 25 rabbits were confirmed as squamous cell carcinoma by pathology.
-
(2)
Comparison of the tumor volume among the groups and the correlation between tumor volume and DCE-MRI quantitative parameters histogram analysis in the development of the VX2 hepatoma model in rabbits.
-
(2–1)
In the development of the VX2 liver cancer model, at the end of 1 ~ 5w group, between the average tumor volume of the randomly selected 5 experimental rabbit tumors in each weekly group was statistically significant (F = 44.11; P = 0.000) (P < 0.01). The significant differences were found between the 5th week and the 1st, 2nd, 3rd, 4th week, the 4th week and the 1st, 2nd week, the 3rd week and the 5th week, respectively (P < 0.01). (Figure 1).

The average tumor volume between the end of 1 ~ 5w group was statistically significant in the development of the VX2 liver cancer model (P < 0.01). The significant differences were found between the 5th week and the 1st, 2nd, 3rd, 4th week, the 4th week and the 1st, 2nd week, the 3rd week and the 5th week, respectively (P < 0.01)
-
(2–2)
The 10th, 25th, 50th percentiles of the Kep value was positively correlated with tumor volume (r = 0.804, r = 0.699, r = 0.495, P < 0.01); The 10th, 25th percentiles of the Ve value was positively correlated with tumor volume (r = 0.920, r = 0.475, P < 0.05); The 10th percentile of the Vp value was positively correlated with tumor volume (r = 0.412, P < 0.05); There was no significant correlation between Ktrans and tumor volume. (Table 1)
-
(3)
Comparison of the results of DCE-MRI quantitative parameter histogram analysis in the groups in the development of the VX2 hepatoma model in rabbits.
During the development of VX2 liver cancer in rabbits, the skewness, kurtosis of the Ktrans value were statistically significant (P < 0.05), the maximum, skewness, kurtosis and 90th percentile of the Kep value were statistically significant (P < 0.05), and the skewness, kurtosis, 75th, 90th percentiles of the Vp value were statistically significant (P < 0.05) in the groups. No significant difference was found in all the histogram parameters of the Ve value in the groups. (Fig. 2-i, ii, iii, iv)

During the development of VX2 liver cancer in rabbits, the skewness, kurtosis of the Ktrans value were statistically significant (P < 0.05) (Fig. 2-i), the maximum, skewness, kurtosis and 90th percentile of the Kep value were statistically significant (P < 0.05) (Fig. 2-ii), and the skewness, kurtosis, 75th, 90th percentiles of the Vp value were statistically significant (P < 0.05) in the groups (Fig. 2-iv). No significant difference was found in all the histogram parameters of the Ve value in the groups (Fig. 2-iii)
-
(4)
Correlation between immunohistochemistry and quantitative parameters of DCE-MRI histograms in the rabbit VX2 implanted tumor.
The expression of ɑ-SMA was negatively correlated with the mean, 75th percentile of the Ktrans value (r=-0.369, r=-0.385, P < 0.05), the 50th, 75th percentiles of the Kep value (r=-0.377, r=-0.472, P < 0.05), the mean, minimum of the Vp value (r=-0.459, P < 0.05). The expression of ɑ-SMA was positively correlated with the skewness, kurtosis of the Ktrans value (r = 0.399, r = 0.415, P < 0.05), the skewness of the Vp value (r = 0.367, P < 0.05). There was no correlation between CD34 and DCE-MRI quantitative parameters (P > 0.05) (Table 2). The DCE-MRI imaging and pathological immunohistochemical expressions of 1 case of implanted tumor in the left lobe of rabbit liver at the end of 3 weeks were shown in Fig. 3-i, ii, iii, iv, v, vi.

The DCE-MRI imaging and pathological immunohistochemical expressions of 1 case of implanted tumor in the left lobe of rabbit liver at the end of 3 weeks. There are the T1-weighted contrast-enhanced (Fig. 3-i), the Ktrans (Fig. 3-ii), the Kep (Fig. 3-iii) and the Ve (Fig. 3-iv) and the Vp (Fig. 3-v) value of the tumor, respectively, the staining area is the ROI of tumor. HE staining(×40): Fig. 3-vi. Immunohistochemical staining (×400): CD34 (Fig. 3-vii), ɑ-SMA (Fig. 3-viii)
Discussion
This study aimed to explore the application of Mr quantitative hemodynamic parameter histogram analysis in the development of a rabbit VX2 liver cancer model. During the development of the rabbit VX2 liver cancer model, the tumor volume change between the groups was statistically significant, and the significant differences were found between the 5th week and the 1st, 2nd, 3rd, 4th week, the 4th week and the 1st, 2nd week, the 3rd week and the 5th week, which intragroup comparison of the tumor volume change, respectively. The cause may be that, when the tumor volume is small, the new blood vessels have not been induced, so the tumor cannot continue to grow in size, and the growth of tumor volume is not significant at this time, confirming no significant difference in the tumor volume in the first three weeks in this study. The nutrient supply of the rabbit liver transplantation tumor model mainly comes from hepatic blood sinuses. Because the tumor nutrient supply comes from the newly formed tumor blood vessels and hepatic blood sinuses, over time, the tumor and peripheral blood vessels show exponential growth, and the tumor volume increases significantly [13, 14]. Wedam et al [15] showed that for phase III clinical trials, DCE-MRI can be used asalternative biomarkers to evaluate the efficacy of drugs before tumor volume changes. The results show that the 10th, 25th, 50th percentiles of the Kep value, the 10th, 25th percentiles of the Ve value, the 10th percentile of the Vp value was positively correlated with tumor volume; while the Ktrans value was no significant correlation with the tumor volume. Among them, the 10th percentile of the Ve are the most correlated, which indicates that in the process of tumor progression, in the lower than the 25th percentile range, which can best reflect the hemodynamic changes of microcirculation in tumor.
This study shows that the 10th, 25th, 50th percentile of the Kep value, the 10th, 25th percentile of the Ve value, and the 10th percentile of the Vp value are positively correlated with tumor volume, indicating that the values of the Kep, Ve and Vp value can reflect the hemodynamic changes of microcirculation in the process of tumor progression in the range of less than 50 percentile. However, there is no significant correlation between Ktrans value and tumor volume, indicating that tumor progression can not be measured only by observing the longitudinal changes of tumor volume, and tumor progression can not fully represent the hemodynamic changes within the tumor [16, 17]. At the same time, DCE-MRI quantitative parameter histogram analysis can better explain it.
In this study, the tumor volume was taken as a reference, and the skewness of the histogram-based DCE-MRI parameters Ktrans, Kep, and Vp was significantly different among the groups, peaking at 4w, and declining at the end of 5w, reflecting the increased skewness in the values of Ktrans, Kep, Vp in the DCE-MRI data. According to some studies [18], the higher is the heterogeneity of tumor, the higher is the skewness value. The lower is the degree of differentiation, the higher is the number of cells. The closer is the arrangement of cells, the less is the amount of the extracellular matrix. The more limited is the vascular permeability, the more limited is the degree of blood flow into the tissue and flow back process of contrast agent from EES to the intravascular space. The higher is the volume fraction of plasma in a single pixel, the greater is the skewness value. These findings demonstrate the complexity of the internal structure of the tumor, resulting in a straight grayscale and the square is not evenly distributed. And in this study, the conventional T2WI sequence, it showed the central region of the high signal and the peripheral ring area of the low signal in the process of rapid growth of the rabbit VX2 tumor [19]. It corresponds to the DCE-MRI showed that the components such as cystic degeneration, necrosis and bleeding increased gradually, and the enhancement mode of hepatocellular carcinoma obtained by DCE-MRI changed from rapid enhancement to slow enhancement or even no enhancement in the central area (Figure 3-i, ii, iii, iv), and the growth, progression and abnormal enhancement mode of this malignant tumor were related to the formation of tumor neovascularization [16]. The results are consistent with those of Moon j et al [20]. Additionally, Woo S et al [21] and others also showed that the degree of skewness better reflected the heterogeneity of liver cancer.
The CD34 can reflect the invasive biological behavior of malignant tumor [22], ɑ-SMA can promote the proliferation of tumor cells as stromal cells around the tumor [23]. The results of this study showed that the expression of ɑ-SMA was positively correlated with the skewness, kurtosis of the Vp value,and the skewness of the Vp value. Related studies have shown that the changes of skewness and kurtosis can be reflected as tumor heterogeneity. In other words, for the heterogeneity in the process of tumor progression, due to the high malignant degree of tumor, the high expression of ɑ-SMA and the increase of tumor vascular permeability, ɑ-SMA promotes tumor progression by releasing growth factors, extracellular matrix proteins and angiogenic factors, so that the kurtosis value is discrete and the skewness value is higher [22, 23]. This study also found that the expression of ɑ-SMA was negatively correlated with the mean and 75th percentile of the Ktrans value, the 50th and 75th percentile of the Kep value, the mean and minimum of the Vp value, indicating that with the enhancement of tumor heterogeneity, the reflux process of contrast medium from EES to intravascular space was limited, and the plasma volume fraction in a single pixel decreased, resulting in the complexity of its internal structure and biological behavior, resulting in uneven gray histogram distribution [24]. In the MRI of the corresponding phase, the signal is uneven, and the tumor is prone to cystic degeneration and necrosis, while the skewness, kurtosis, higher percentile (50th, 75th) and mean of the Ktrans, Kep, Vp value can best reflect tumor heterogeneity, which is consistent with the results of Moon J et al [20].
However, in this study, it was found that there was no significant correlation between CD34 and histogram parameters of DCE-MRI quantitative parameters. The reason may be that with the increase of tumor heterogeneity, cystic degeneration and necrosis in the tumor were more common, angiogenesis was significantly decreased, while the vascular endothelial cells around the tumor were reactive hyperplasia [25]. MRI showed obvious enhancement in the periphery of the tumor but no enhancement in the center. In addition, the repeatability of DCE-MRI imaging parameters is affected by the location of the lesions. Although the repeatability of intrahepatic parameters is significantly higher than that of other organs or tissues [26], when quantitative DCE-MRI imaging parameters are used to evaluate diseases, the parameters obtained by the pharmacokinetic model may not be accurate enough for clinical application [27, 28].
Our research has some limitations. First, the sample size was relatively small, producing a certain selection bias, and more samples are needed for further investigation on the heterogeneity of tumors in the future when necessary. Second, In this study, ROI is based on the maximum cross-sectional area manually sketched, software synthesis of the tumor volume and measured the average value many times, which has a slight error with the actual tumor volume; however, our method is simple, fast and more practical. Third, the motion artifacts caused by breathing and heart movement can affect Image quality of the DCE-MRI. ECG gating technology can effectively reduce the cardiac artifacts; however, because the heart rate of New Zealand white rabbits is very fast (180–250 BPM), this study did not use this technology. To reduce the impact of respiratory artifacts, we used two methods: (1) pentobarbital anesthesia, which can inhibit the respiratory movement of New Zealand white rabbits to a certain extent; (2) non-rigid registration method of the total dynamics program to perform the motion correction of medical imaging alignment to reduce the motion artifacts. Using the above two methods, the respiratory artifacts of New Zealand white rabbits were effectively controlled.
Conclusions
This study showed that the MRI quantitative hemodynamic parameter histogram analysis can reflect the progress of the rabbit VX2 liver cancer. In particular, the skewness, kurtosis and percentiles of Ktrans, Kep and Vp can reflect the microvascular information and can be used as biomarkers to assess the development of HCC.
Data availability
All data generated or analysed during this study are included in this published article.
References
Liu Y, Zheng J, Hao J, et al. Global burden of primary liver cancer by five etiologies and global prediction by 2035 based on global burden of disease study 2019. Cancer Med. 2022;11(5):1310–23. https://doi.org/10.1002/cam4.4551.
Torre LA, Bray F, Siegel RL, et al. Global cancer statistics, 2012. Cancer J Clin. 2015;65(2):87–108. https://doi.org/10.3322/caac.21262.
Neeman M, Perspectives. MRI of angiogenesis. J Magn Reson. 2018;292:99–105. https://doi.org/10.1016/j.jmr.2018.04.008.
Liu K, Zhang X, Xu W, et al. Targeting the vasculature in hepatocellular carcinoma treatment: starving versus normalizing blood supply. Clin Transl Gastroenterol. 2017;8(6):e98–e101. https://doi.org/10.1038/ctg.2017.28.
Chong HH, Yang L, Sheng RF, et al. Multi-scale and multi-parametric radiomics of gadoxetate disodium-enhanced MRI predicts microvascular invasion and outcome in patients with solitary hepatocellular carcinoma ≤ 5 cm. Eur Radiol. 2021;31(7):4824–38. https://doi.org/10.1007/s00330-020-07601-2.
Chen BB, Lin ZZ, Shao YY et al. Early changes in DCE-MRI biomarkers may predict survival outcomes in patients with advanced hepatocellular carcinoma after Sorafenib failure: two prospective phase II trials. Cancers (Basel). 2021;13(19):4962. https://doi.org/10.3390/cancers13194962.
Mu X, Zhong Y, Zhang X, Qu C. Early diagnosis value of DCE-MRI hemodynamic parameters in hepatocellular carcinoma. J Oncol. 2022;2022:9556589. https://doi.org/10.1155/2022/9556589.
Brix G, Griebel J, Kiessling F, et al. Tracer kinetic modelling of tumour angiogenesis based on dynamic contrastenhanced CT and MRI measurements. Eur J Nucl Med Mol Imaging. 2010;37(Suppl 1):30–S51. https://doi.org/10.1007/s00259-010-1448-7.
Chen BB, Shih TT. DCE-MRI in hepatocellular carcinoma-clinical and therapeutic image biomarker. World J Gastroenterol. 2014;20(12):3125–34. https://doi.org/10.3748/wjg.v20.i12.3125.
Just N. Improving tumour heterogeneity MRI assessment with histograms. Br J Cancer. 2014;111:2205–13. https://doi.org/10.1038/bjc.2014.512.
Surov A, Meyer HJ, Leifels L, et al. Histogram analysis parameters of dynamic contrast-enhanced magnetic resonance imaging can predict histopathological findings including proliferation potential, cellularity, and nucleic areas in head and neck squamous cell carcinoma. Oncotarget. 2018;9(30):21070–7. https://doi.org/10.18632/oncotarget.24920.
Meyer HJ, Leifels L, Schob S, et al. Histogram analysis parameters identify multiple associations between DWI and DCE MRI in head and neck squamous cell carcinoma. Magn Reson Imaging. 2018;45:72–7. https://doi.org/10.1016/j.mri.2017.09.015.
Pascale F, Pelage JP, Wassef M, et al. Rabbit VX2 liver tumor model: a review of Clinical, Biology, Histology, and Tumor Microenvironment characteristics. Front Oncol. 2022;12:871829. https://doi.org/10.3389/fonc.2022.871829.
Korean Liver Cancer Association. National Cancer Center 2019 2018 Korean Liver Cancer Association-National Cancer Center Korea Practice guidelines for the management of Hepatocellular Carcinoma. Gut Liver 13 3 227–99 https://doi.org/10.5009/gnl19024.
Wedam SB, Low JA, Yang SX, et al. Antiangiogenic and antitumor effects of bevacizumab in patients with inflammatory and locally advanced breast cancer. J Clin Oncol. 2006;24:769–77. https://doi.org/10.1200/JCO.2005.03.4645.
Jajamovich GH, Huang W, Besa C, et al. DCE-MRI of hepatocellular carcinoma: perfusion quantification with Tofts model versus shutter-speed model–initial experience. MAGMA. 2016;29(1):49–58. https://doi.org/10.1007/s10334-015-0513-4.
Zhu AX, Duda DG, Sahani DV, et al. HCC and angiogenesis: possible targets and future directions. Nat Rev Clin Oncol. 2011;8:292–301. https://doi.org/10.1038/nrclinonc.2011.30.
Zhu YJ, Feng B, Wang S, et al. Model-based three-dimensional texture analysis of contrast- enhanced magnetic resonance imaging as a potential tool for preoperative prediction of microvascular invasion in hepatocellular carcinoma. Oncol Lett. 2019;18(1):720–32. https://doi.org/10.3892/ol.2019.10378.
Keller S, Chapiro J, Brangsch J, et al. Quantitative MRI for assessment of treatment outcomes in a rabbit VX2 hepatic tumor model. J Magn Reson Imaging. 2019;52(3):668–85. https://doi.org/10.1002/jmri.26968.
Moon J, Kim JH, Choi D, et al. Correlation of quantitative dynamic contrast-enhanced MRI with microvascular density in necrotic, partial necrotic, and viable liver tumors in a rabbit model. J Appl Clin Med Phys. 2016;17(5):418–27. https://doi.org/10.1120/jacmp.v17i5.
Woo S, Cho JY, Kim SY, et al. Histogram analysis of apparent diffusion coefficient map of diffusion-weighted MRI in endometrial cancer: a preliminary correlation study with histological grade. Acta Radiol. 2014;55:1270–7. https://doi.org/10.1177/0284185113514967.
Wang WQ, Liu L, Xu HX, et al. Intratumoral α-SMA enhances the prognostic potency of CD34 associated with maintenance of microvessel integrity in hepatocellular carcinoma and pancreatic cancer. PLoS ONE. 2013;8(8):e71189. https://doi.org/10.1371/journal.pone.0071189.
Benzoubir N, Mussini C, Lejamtel C, et al. Gamma-smooth muscle actin expression is associated with epithelial-mesenchymal transition and stem-like properties in hepatocellular carcinoma. PLoS ONE. 2015;10(6):e0130559. https://doi.org/10.1371/journal.pone.0130559.
Zhang J, Gu C, Song Q, et al. Identifying cancer-associated fibroblasts as emerging targets for hepatocellular carcinoma. Cell Biosci. 2020;10(1):127. https://doi.org/10.1186/s13578-020-00488-y.
Gawlitza M, Purz S, Kubiessa K, et al. In vivo correlation of glucose metabolism, cell density and microcirculatory parameters in patients with head and neck cancer: initial results using simultaneous PET/MRI. PLoS ONE. 2015;10:e0134749. https://doi.org/10.1371/journal.pone.0134749.
Kim H. Variability in quantitative DCE-MRI: sources and solutions. J Nat Sci. 2018;4(1):e484.
Chartampilas E, Rafailidis V, Georgopoulou V, et al. Current imaging diagnosis of Hepatocellular Carcinoma. Cancers (Basel). 2022;14(16):3997. https://doi.org/10.3390/cancers14163997.
Taouli B, Johnson RS, Hajdu CH, et al. Hepatocellular carcinoma: perfusion quantification with dynamic contrast-enhanced MRI. AJR Am J Roentgenol. 2013;201:795–800. https://doi.org/10.2214/AJR.12.9798.
Acknowledgements
Not applicable.
Funding
This work was supported by the Regional Foundation of National Natural Science Foundation (81660283).
Author information
Authors and Affiliations
Contributions
R.G.: conception and design, acquisition of data, drafting the article, revising article critically. J.M.: design and supervise the study. Z.S. and P.Z.: research method design. J.A.: analyses of data. D.D.: animal MRI scanning. J.L. and Y.W.: validation. All authors contributed to the article and approved the submitted version.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the animal protection and ethics committee of The First Affiliated Hospital of Shihezi University School of Medicine. All experiments were performed in accordance with relevant guidelines and regulations.Additionally, Our manuscript reporting adheres to the ARRIVE guidelines (https://arriveguidelines.org) for the reporting of animal experiments, so all data should be submitted to the Ethics Committee of this institution for use.
Consent for publication
Not applicable.
Competing interests
The authors declare that the research was conducted in the absence of any commercial or fifinancial relationships that could be construed as a potential conflflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Guo, R., Song, Z., Zuo, P. et al. MRI quantitative hemodynamic parameter histogram assement of hepatocellular carcinoma development in a rabbit VX2 liver cancer model. Chin J Acad Radiol 7, 147–156 (2024). https://doi.org/10.1007/s42058-024-00146-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s42058-024-00146-z